
Abstract
Purpose:
To examine the association between telehealth utilization and mammogram receipt by rurality, and to characterize geographic patterns of concurrent increases in telehealth and mammography use in urban and rural communities.
Methods:
The sample included women, aged 50 years or older, receiving services in primary care or gynecology/women’s health practices at MultiCare Health System from 2018 to 2023. For the difference-in-difference (DiD) analyses, women who had only in-person visits during the prepandemic period but had at least one telehealth visit in each year of the postpandemic period were defined as the treatment group. Women who had only in-person visits during both pre- and postpandemic periods were defined as the control group. For the spatial analyses, we analyzed ZIP Codes in which both telehealth and mammography utilization increased from 2018–2019 to 2020–2022.
Findings:
DiD analyses suggested that telehealth use was significantly associated with a greater probability of mammogram receipt among rural women; however, this association was not found in urban women. Spatial analyses indicated that concurrent increases in telehealth and mammogram use occurred in both rural and urban settings but exhibited greater spatial concentration in urban areas and comparatively more dispersed patterns across rural ZIP Code Tabulation Areas.
Conclusions:
The findings suggest that telehealth may be particularly beneficial for improving mammography screening among rural individuals, who typically experience greater structural barriers to accessing health care. While urban areas may exhibit clustered patterns driven by interconnected care systems, rural areas may experience more diffuse but meaningful gains as telehealth expands access across large geographic distances.
Introduction
Telehealth is defined by the Health Resources and Services Administration as “the use of electronic information and telecommunication technologies to support and promote long-distance clinical health care, patient and professional health-related education, public health and health administration.” 1 Telehealth has gained prominence in modern health care delivery, particularly following the onset of the pandemic, with around 5–10% of all ambulatory visits now occurring online. 2 Due to resumption of in-person care, telehealth utilization has declined following the initial postpandemic surge; however, current utilization is greater than the prepandemic levels of <1%. 3 Despite issues related to technology access and digital literacy, telehealth could hold potential in reducing health care disparities by improving convenience of obtaining care and patient-provider connectivity.
Breast cancer is the most commonly diagnosed cancer among women, with women in rural areas more likely to experience barriers in accessing specialty breast cancer care. 4 Mammography plays a central role in the early detection of breast cancer. The US Preventive Services Task Force guidelines recommend biennial screening among women aged 40–74 years, 5 whereas the American Cancer Society, the National Comprehensive Cancer Network, the American College of Radiology, the Society of Breast Imaging, and the American College of Surgeons support annual screenings. 6 There are significant disparities in mammography screening rates between rural and urban populations, such that individuals in rural areas undergo screening at lower rates than their urban counterparts. 7 Differences in access to health care facilities and socioeconomic conditions could explain the lower rates of breast cancer screening among rural women. 8 In 2022, 50.6% of rural women aged 45–84 years had limited geographic access to mammography, with this percentage exceeding 50% in 28 states, whereas only 3.0% of urban women experienced similar limitations. 9
The persistent gap in mammography utilization between rural and urban populations signals the need to understand whether telehealth could be utilized as a tool to bridge disparities in mammography screening. Transportation, inability to take time off work, and childcare needs have been associated with missed or deferred in-person health care appointments,10,11 with rural patients commonly experiencing greater transportation barriers than urban residents. 11 Telehealth could overcome these barriers by reducing travel and wait times for individuals seeking health care. For example, one study showed that telehealth saved an average of about 4 hours per encounter among cancer patients treated at a tertiary medical center in Utah. 12 This could result in a time-trade off, whereby telehealth frees up time 13 which could be used for other healthcare needs that require in-person visits, such as mammograms. By enabling remote patient-provider communication, 14 telehealth could improve receipt of breast cancer screening services especially among rural residents who report greater travel time for accessing health care. 15 A comparison of mammography receipt between telehealth and nontelehealth users by rurality could provide more understanding on the relationship between telehealth and mammography receipt.
In a previous study utilizing 2018–2022 encounter data from a large health care system in Washington State, we showed that women with at least one telehealth visit were more likely to undergo mammography compared with those with no visits. 16 While this prior study longitudinally assessed changes in patient-level mammogram receipt in relation to telehealth use, it did not explicitly examine the effect of telehealth on mammography receipt by comparing outcomes between groups. The goal of the current study was to examine the association between telehealth utilization (for primary care or gynecology/women’s health services) and mammogram receipt, stratified by rurality, via a quasi-experimental study design. In addition to the patient-level, quasi-experimental analyses, a ZIP Code–level spatial analysis of changes in telehealth and mammography utilization across Washington State and northern Idaho was conducted to characterize geographic patterns of concurrent increases in telehealth and mammography use in urban and rural communities.
Methods
Settings and population
This study drew its patient population from MultiCare Health System, the state’s premier nonprofit community health care network comprising more than 20,000 practitioners, staff, and volunteers. 17 In the state of Washington, MultiCare is the second-largest provider by market share, capturing ∼18% of the market. 18 The organization operates an integrated health care delivery system spanning Washington State’s metropolitan and rural communities, offering hospital-based care, primary medicine, telehealth, urgent treatment, pediatric care, specialty care, and cancer care services. The study protocol received approval from MultiCare’s institutional review board.
Analytic data and study sample
The analytic data for this study consisted of MultiCare Health System records from 2018 to 2023, documenting in-person and telehealth encounters for women aged 50 years or older receiving services in primary care or gynecology/women’s health practices. The study sample included only women who completed at least one eligible encounter from 2018 to 2023. More details on the analytic data and study sample are described elsewhere. 16
Mammogram receipt (outcome variable)
Procedure codes paired with their text descriptions were used to identify screening mammograms. The methodology, as previously described, 16 accounted for a 12-month window between the health care encounter and screening mammogram. For this purpose, for each encounter year, the number of mammograms in the respective encounter year and the next calendar year was calculated and dichotomized as: (1) absence of screening mammograms or (2) presence of one or more screening mammograms. Given that the study period included data up to December 2023, this methodology for computing mammogram receipt was applied to encounter years spanning from 2018 to 2022.
Telehealth use
For all study participants, the number of encounters was computed, and analyses were limited to women with fewer than four encounters per year. Those with four or more yearly visits were excluded because higher health care use could imply presence of chronic health conditions.19,20 Annual encounter data were summarized to indicate whether the participants had: (1) only in-person encounters, (2) at least one telehealth encounter, or (3) no encounters. For this study, those with no encounters at any time during the study period were excluded.
Treatment and control group (explanatory variable)
Telehealth use during the pre- (i.e., 2018 and 2019) and postpandemic (i.e., 2021 and 2022) periods was assessed to classify women into treatment or control groups. Women who had only in-person visits during the prepandemic period but had at least one telehealth visit in each year of the postpandemic period were defined as the treatment group. Women who had only in-person visits during both the pre- and postpandemic periods were defined as the control group.
Demographic characteristics
Participant demographic information included race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, other races, including multiracial) and age at the time of most recent encounter. Insurance coverage for each year was categorized based on payment type: (1) all encounters covered by commercial insurance; (2) at least one encounter paid by Medicaid (but not Medicare, other government programs, or self-pay); (3) at least one encounter paid by Medicare (but not other government programs or self-pay); (4) at least one encounter covered by other government insurance (but not self-paid); (5) at least one self-paid encounter; and (6) encounters paid by other nongovernment insurance.
Statistical analysis
The association between telehealth use and mammogram receipt was estimated using difference-in-difference (DiD) models. The parallel trends assumption of the DiD model states that mammogram receipt rates should be similar between the treatment and control groups in the absence of the treatment. While this scenario cannot be directly tested, pretreatment trends can be examined by interacting the type of group (i.e., treatment or control) with an indicator for year (i.e., 2018 and 2019). 21
Generalized linear mixed models were used for the DiD analyses to estimate the association between telehealth use and the probability of mammography receipt. Models included fixed effects for group assignment (treatment versus control), time period (preintervention [2018–2019] versus postintervention [2021–2022]), and a group-by-time interaction term. The coefficient of the interaction term represented the DiD estimate of the association between telehealth use and mammography receipt. Models were adjusted for age, race/ethnicity, and insurance coverage and included a random intercept to account for within-subject correlation. Sensitivity analyses were conducted by excluding women with breast cancer.
Spatial analyses included ZCTAs classified as urban or rural using Rural–Urban Commuting Area (RUCA) codes based on ZIP Code of residence.22,23 ZIP codes in urban areas (RUCA codes 1–3) were grouped as urban, whereas those in rural areas (RUCA codes 4–10) were grouped as rural. Geographic boundaries were defined using ZCTAs from the U.S. Census Bureau’s TIGER/Line files (2010 vintage), which were used as geographic approximations of postal ZIP Codes for spatial analysis. 24
Global Moran’s I and Local Indicators of Spatial Association (LISA) were calculated across the full study region among all included urban and rural ZCTAs rather than being estimated separately within urban and rural strata. Spatial autocorrelation was evaluated using a binary outcome indicating whether both telehealth and mammography utilization increased from the prepandemic to postpandemic period. Urban–rural classification was retained as a descriptive variable to compare mapped clustering patterns and interpret differences across metropolitan core and rural/noncore communities while preserving a single spatial weights structure.
Classification of telehealth and mammography utilization changes
For the spatial analyses, we analyzed ZIP Codes in which both telehealth and mammography utilization increased from 2018–2019 to 2020–2022. This category was selected to identify communities where improvements in remote care access coincided with improvements in preventive screening utilization.
For each ZIP Code, changes in telehealth and mammography utilization were independently classified as increases, decreases, or no change. These classifications were then combined to create mutually exclusive directional change categories representing all possible combinations of change across the two services.
Spatial autocorrelation analysis
Spatial autocorrelation analyses were conducted using R statistical software and reproducible spatial analysis workflows commonly employed in public health research. 25 Global spatial autocorrelation was assessed using Moran’s I with 999 Monte Carlo permutations, and local spatial clustering was evaluated using LISA. Spatial relationships were defined using a k-nearest neighbors spatial weights matrix (k = 6) to ensure consistent connectivity across urban and rural ZCTAs. Analyses were conducted using projected coordinates (NAD83/Conus Albers; EPSG:5070) to avoid geographic distortion and to ensure accurate distance-based spatial calculations. Statistical significance was assessed at α = 0.05.
Results
Demographic characteristics
Table 1 indicates the demographic characteristics of women, based on rurality and whether they were classified as treatment/control group. About 97% and 94% of rural women in the treatment and control groups were non-Hispanic White, respectively, whereas about 87% of urban women in the treatment and control groups were non-Hispanic White. Most of the women in the study sample had encounters paid via commercial insurance/at least one Medicare-paid encounter.
Demographic Characteristics Of Women Seeking Healthcare, By Type Of Visit And Rurality, Within A Large Healthcare System In Washington State
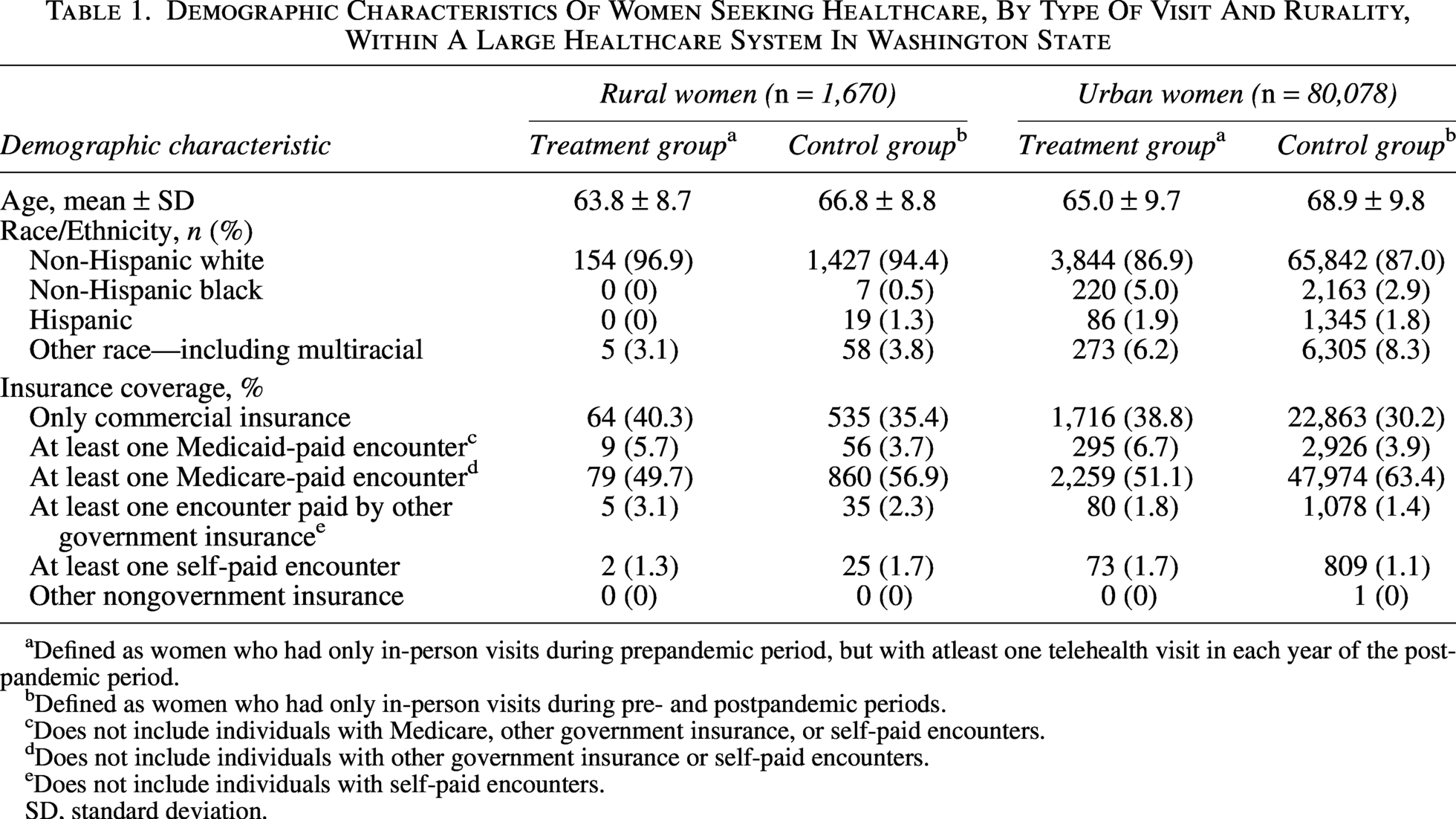
Defined as women who had only in-person visits during prepandemic period, but with atleast one telehealth visit in each year of the postpandemic period.
Defined as women who had only in-person visits during pre- and postpandemic periods.
Does not include individuals with Medicare, other government insurance, or self-paid encounters.
Does not include individuals with other government insurance or self-paid encounters.
Does not include individuals with self-paid encounters.
SD, standard deviation.
Telehealth use and mammogram receipt
In the prepandemic period, the test for the parallel trends assumption suggested similar trends in mammogram receipt between the treatment and control groups (i.e., the interaction between the type of group [i.e., treatment or control] and an indicator for year [i.e., 2018 and 2019] was not found to be statistically significant). Table 2 indicates the associations between telehealth use and mammogram receipt among rural and urban women, as estimated via DiD models. As shown in Table 2, the DiD analyses suggested that telehealth use (as indicated by whether the woman was classified into the treatment or control group) was significantly associated with a greater probability of mammogram receipt in rural women (estimate = 0.18; 95% confidence interval [CI] = 0.06, 0.29; p value = 0.002). However, this association was not observed among urban women.
Associationa Of Telehealth Use With Mammogram Receipt In Rural and Urban Women
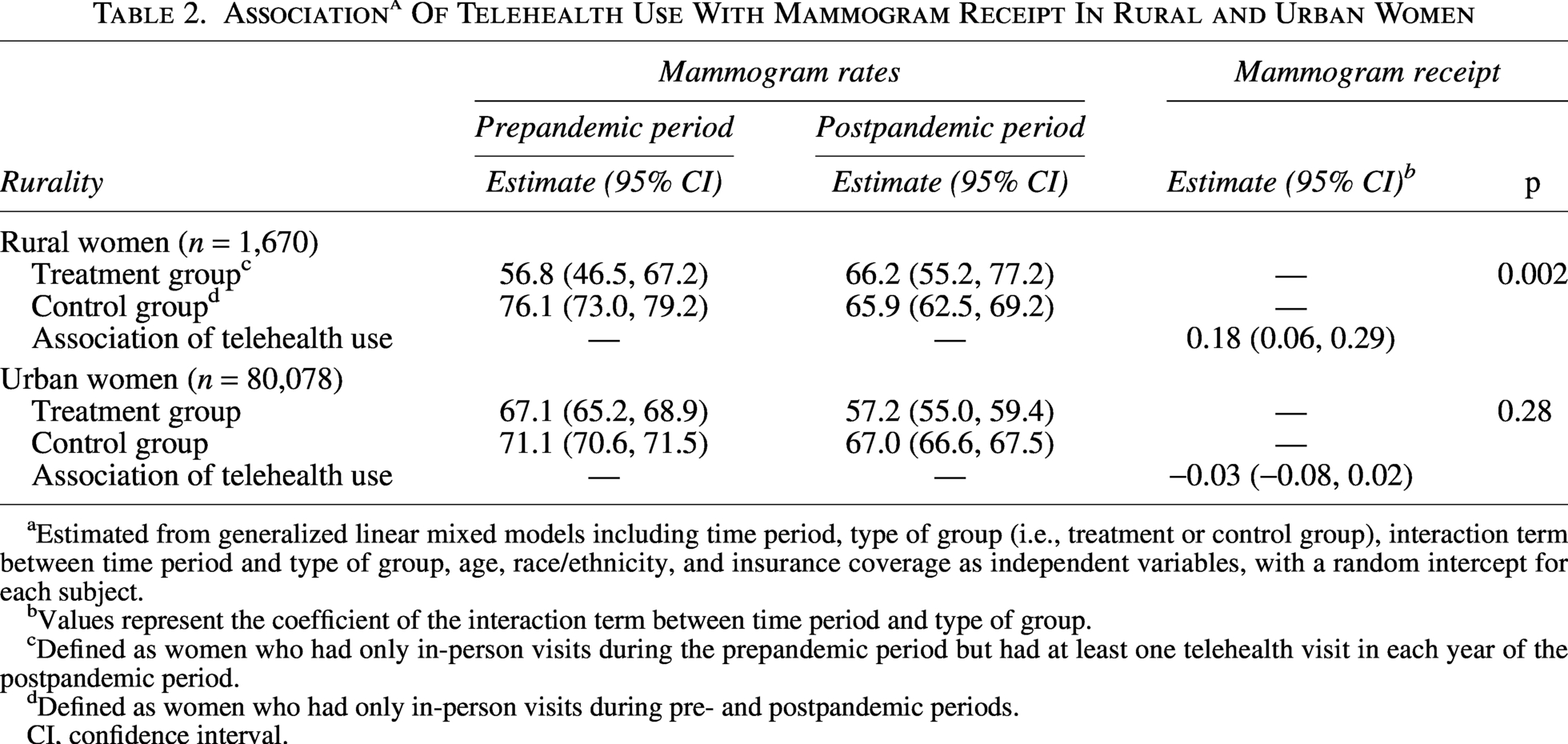
aEstimated from generalized linear mixed models including time period, type of group (i.e., treatment or control group), interaction term between time period and type of group, age, race/ethnicity, and insurance coverage as independent variables, with a random intercept for each subject.
bValues represent the coefficient of the interaction term between time period and type of group.
cDefined as women who had only in-person visits during the prepandemic period but had at least one telehealth visit in each year of the postpandemic period.
dDefined as women who had only in-person visits during pre- and postpandemic periods.
CI, confidence interval.
Sensitivity analyses
Sensitivity analyses excluding women with breast cancer did not change the overall findings (data not shown in Table). Excluding women with breast cancer resulted in sample sizes of 1,666 and 79,836 for rural and urban women, respectively. Telehealth use was significantly associated with a greater probability of mammogram receipt among rural women (estimate = 0.18; 95% CI = 0.06, 0.29; p value = 0.002). However, this association was not observed among urban women.
Directional changes in telehealth and mammography utilization
Across all ZCTAs included in the spatial analysis, 61.2% experienced concurrent increases in telehealth and mammography utilization between the pre- and postintervention periods (data not shown). Among these ZCTAs, the average increase in telehealth utilization was 22.9% points, accompanied by an average increase in mammography utilization of 10.2% points. This category represented the most common directional pattern observed.
Spatial patterning of telehealth and mammography changes
Global spatial autocorrelation analyses demonstrated strong and statistically significant clustering among ZCTAs experiencing concurrent increases in telehealth utilization and mammography receipt (Moran’s I = 0.41, p = 0.001), indicating that areas with concurrent improvement were geographically concentrated rather than randomly distributed within the service regions represented in the data.
LISA further characterized these patterns, revealing distinct urban–rural clustering among ZCTAs within MultiCare’s primary service areas, which are concentrated in western Washington and selected regions of central and eastern Washington. Among urban ZCTAs (RUCA 1), 104 areas were classified as statistically significant high–high clusters and 48 as low–low clusters (p ≤ 0.05), with 11 high–low spatial outliers and 112 ZCTAs classified as not statistically significant (Fig. 1). Among rural ZCTAs (RUCA 2), 10 areas were classified as high–high clusters and 15 as low–low clusters, with 4 high–low outliers and 103 classified as not statistically significant (Fig. 2). Low–high clusters were not observed among either urban or rural ZCTAs. Together, these findings indicate that concurrent increases occurred in both settings but exhibited greater spatial concentration in urban areas and comparatively more dispersed patterns across rural ZCTA (Fig. 3).
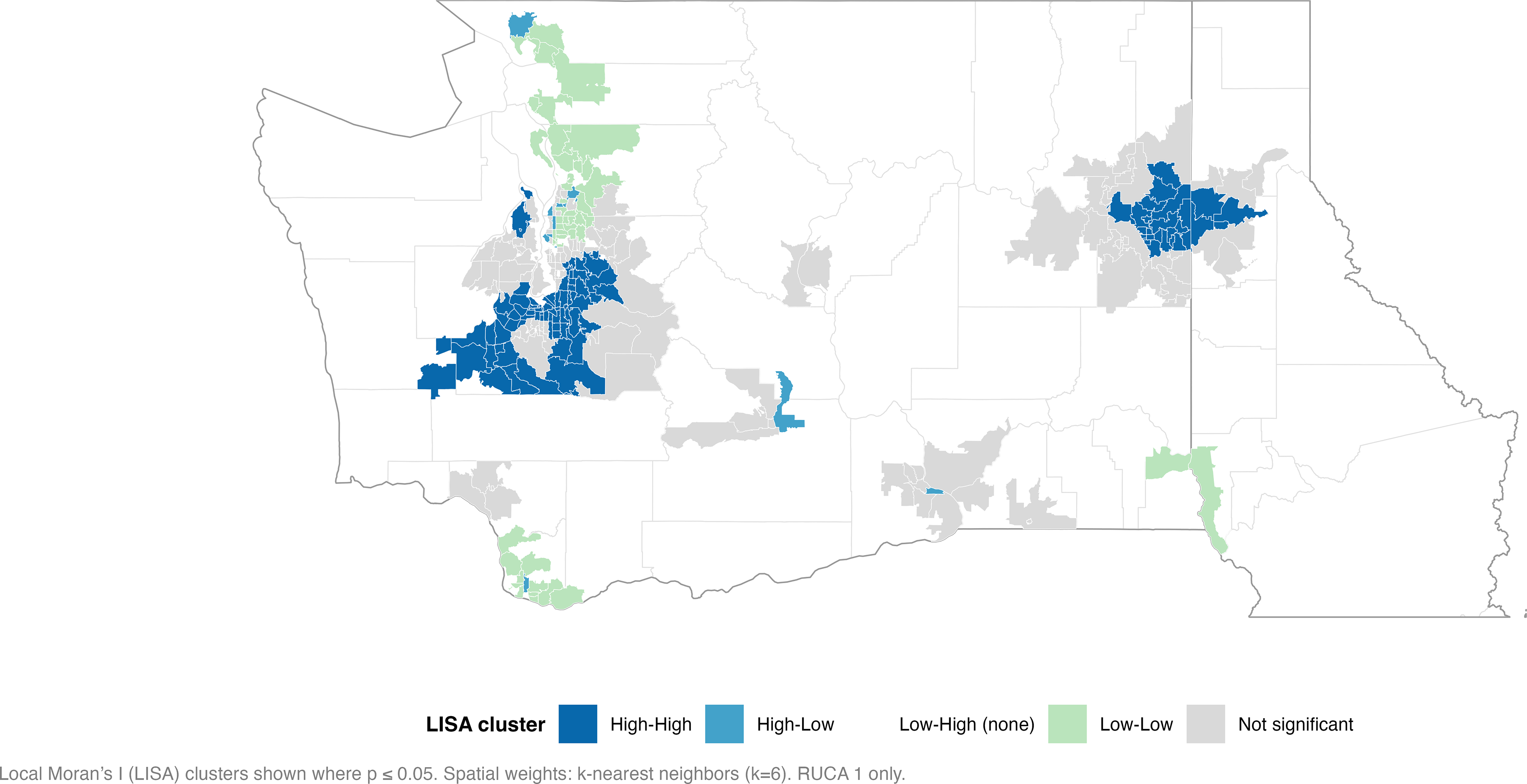
Urban ZIP Code Tabulation Areas (ZCTAs) with concurrent increases in telehealth and Mammography utilization. Local Indicators of Spatial Association (LISA) clusters identifying ZCTAs classified as urban (RUCA 1) that experienced concurrent increases in telehealth and mammography utilization during the study period. Statistically significant high–high and low–low clusters are shown (p ≤ 0.05) based on a k-nearest neighbors spatial weights matrix (k = 6). Urban classification was defined using Rural–Urban Commuting Area (RUCA) codes. ZCTAs not meeting the significance threshold are shown as not significant.
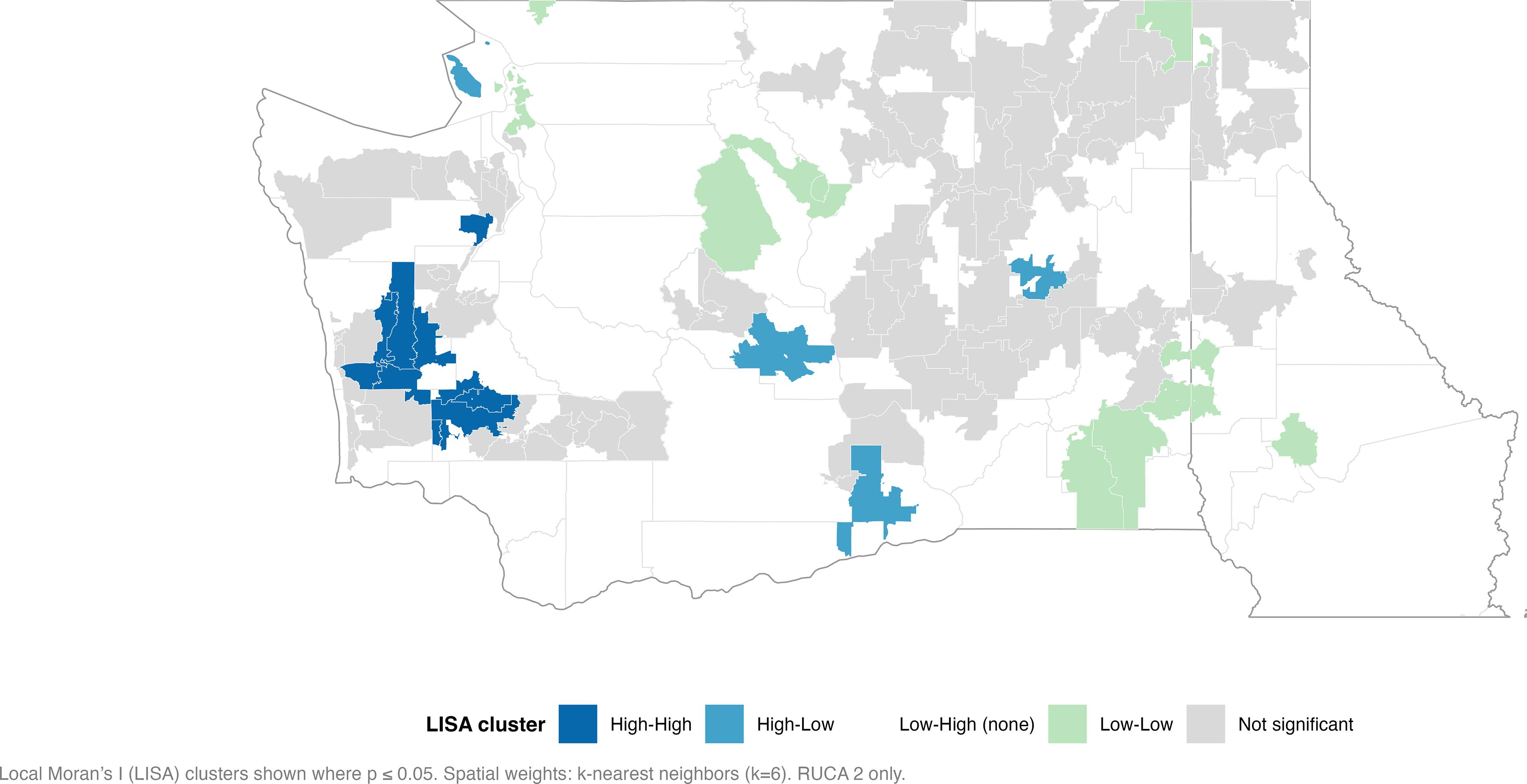
Rural ZCTAs with concurrent increases in telehealth and mammography utilization. LISA clusters identifying ZCTAs classified as rural (RUCA 2) that experienced concurrent increases in telehealth and mammography utilization during the study period. Statistically significant high–high and low–low clusters are shown (p ≤ 0.05) based on a k-nearest neighbors spatial weights matrix (k = 6). Rural classification was defined using RUCA codes. ZCTAs not meeting the significance threshold are shown as not significant.
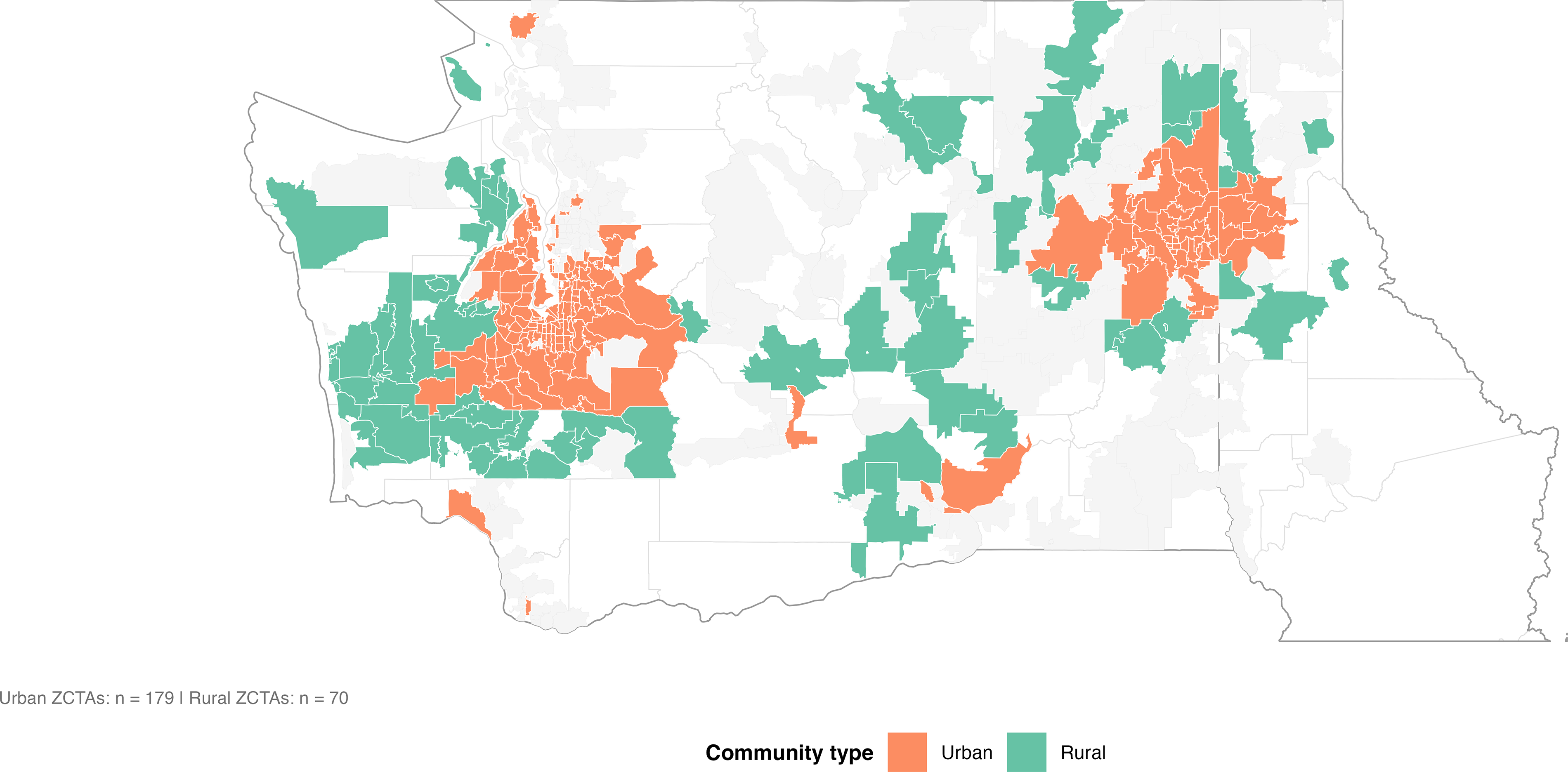
Choropleth map of ZCTAs in Washington State and Northern Idaho showing ZIP Codes that experienced concurrent increases in telehealth and mammography utilization in 2018. ZIP Codes meeting the focus criterion are shaded by community type (urban or rural), whereas remaining urban and rural ZIP Codes in the study region are shown in light gray for geographic context. County and state boundaries are included for orientation. Counts of urban and rural ZIP Codes meeting the criterion are annotated on the map.
Discussion
In this study, we observed distinct patterns in the association between telehealth use and mammogram receipt among rural and urban women. Findings from the DiD analyses suggest that telehealth use was significantly associated with mammogram receipt among rural women. Compared with the control group (i.e., those women who had only in-person visits during pre- and postpandemic periods), women utilizing at least one telehealth visit in each year of the postpandemic period had higher mammogram rates. In contrast, among urban women, telehealth use was not significantly associated with mammogram receipt. These findings suggest that telehealth may have encouraged utilization of breast cancer screening in rural populations during and following periods of healthcare disruption, whereas having a more limited impact on screening behaviors in urban settings. These findings have important implications for telehealth expansion efforts, given evidence suggesting that lack of access to virtual care offered by providers is a common barrier to telehealth use. 26
The current study findings are somewhat comparable to those of a meta-analysis of randomized controlled trials demonstrating that telehealth interventions could improve cancer screening uptake, with particularly strong effects observed for breast and cervical cancer screening. 27 The meta-analysis also found that these benefits extended to rural populations. 27 Notably, the randomized controlled trials included in the meta-analysis utilized different telehealth modalities, such as telephone, video, and text messages, for outreach or reminders. 27 The current study contributes to the literature by assessing the impact of telehealth visits with health care providers on mammogram receipt. The findings of this study differ from those of a previous longitudinal analysis we conducted using MultiCare encounter data. 16 That previous analysis found that engagement with health care services, whether in person or via telehealth, was strongly associated with higher mammogram receipt compared with no clinical encounters. However, women with exclusively in-person visits had the highest likelihood of screening, whereas those using telehealth had lower odds than in-person users but higher odds than women with no visits in both rural and urban areas. 16 The discrepancy in findings may be attributed to differences in study design between the current and previous analyses. Nevertheless, the findings collectively suggest that telehealth represents a valuable complementary strategy for facilitating mammogram receipt, especially in rural populations.
The spatial analyses provide complementary context for these findings by demonstrating that areas experiencing concurrent increases in telehealth and mammography utilization were not randomly distributed but instead followed geographically structured patterns. In urban areas, ZCTAs with concurrent increases tended to form geographically contiguous clusters, reflecting spatial cohesion consistent with dense health care networks and shared service environments. This clustering suggests that changes in utilization within urban settings may be influenced by regional health system characteristics and overlapping access pathways rather than isolated ZIP Code–level dynamics.
In contrast, rural ZCTAs experiencing concurrent increases were more spatially dispersed across the study region, with fewer large contiguous clusters and greater geographic separation between areas exhibiting improvement. This dispersed pattern suggests that telehealth may have facilitated mammography receipt among rural women by reducing individual-level access barriers rather than through regionally concentrated system-level changes. In rural contexts, improvements in cancer screening may therefore occur across geographically isolated communities, even in the absence of strong local spatial clustering. However, several alternate mechanisms may also contribute to these patterns, particularly in isolated rural communities where both telehealth and mammography utilization increased. Localized outreach efforts,28–31 including mobile mammography services, federally qualified health centers, community health partnerships, and targeted screening initiatives, may have improved access independent of baseline geographic barriers. Travel behavior and care-seeking norms may also play an important role, as rural residents often travel longer distances for preventive care 32 and may consolidate multiple health care services into fewer visits. Telehealth may reduce travel burden for follow-up or primary care while preserving in-person mammography use, resulting in localized increases in both outcomes. Because clinic-level intervention data, mobile screening availability, outreach intensity, and travel behavior were not directly measured, these findings likely reflect a combination of health care access, transportation patterns, provider availability, and local health system characteristics rather than geographic proximity alone.
Together, these findings suggest that the relationship between telehealth use and breast cancer screening utilization operates through different spatial patterns in urban and rural settings. While urban areas may exhibit clustered patterns driven by dense and interconnected care systems, rural areas may experience more diffuse but meaningful gains as telehealth expands access across large geographic distances.33,34 This distinction underscores the importance of considering both patient-level and place-based dynamics when evaluating the impact of telehealth on health behaviors.
Findings from this study have important public health implications in light of persistent disparities in telehealth use and mammogram rates between rural and urban populations. In a Medicare population, breast cancer screening uptake was found to be lower in rural counties compared with larger urban counties. 35 These differences in uptake are likely multifactorial and may reflect geographic barriers to care, transportation challenges, and socioeconomic factors that limit engagement with screening services. Similarly, telehealth use in rural areas has been found to be lower compared with urban settings, potentially due to factors such as limited broadband access. 36 During the COVID-19 pandemic, telemedicine visits increased significantly across all populations, but rural patients experienced only a 27.2% increase in telemedicine use compared with a 52.3% increase among urban patients. 37 The current study findings imply the importance of reducing disparities in telehealth adoption in rural settings. Future research incorporating multilevel spatial–temporal approaches may further clarify how individual behaviors interact with geographically structured health system factors to influence breast cancer screening utilization in rural communities.
Results of this study must be interpreted in view of its limitations. First, the study sample predominantly consisted of non-Hispanic White individuals. Additionally, because the data were limited to patient interactions within MultiCare, interactions with providers and clinics outside this health care system were not recorded. Furthermore, only two time points during the prepandemic period were available to test the parallel trends assumption for the DiD analyses. It is also possible that the increase in mammogram rates in the treatment group, relative to the control group, during the postpandemic period could be attributed to other reasons, such as proactive health behaviors.
Several limitations related to the spatial analyses should be considered. Spatial analyses were conducted at the ZCTA level, which represents an administrative geographic approximation of postal ZIP Codes and may not fully capture the true spatial scale at which health care access and utilization decisions occur. Additionally, because the data were drawn from MultiCare’s service regions, spatial clustering reflects patterns within areas of provider coverage and may not generalize beyond those regions. As with all area-level analyses, these findings are subject to the modifiable areal unit problem, whereby observed spatial patterns may vary depending on the geographic unit of analysis. 38 Spatial relationships were defined using a fixed k-nearest neighbors spatial weights matrix, which ensures consistent connectivity across urban and rural areas but may not fully represent real-world care-seeking pathways or referral networks. Although this approach is commonly used in spatial analyses, alternative spatial weight specifications could yield different local clustering patterns. Finally, the spatial analyses were descriptive in nature and were intended to contextualize patient-level findings rather than establish causal relationships at the area level. Outreach intensity, mobile mammography services, local referral patterns, and travel behavior were not directly measured and may partially explain the observed clustering patterns, particularly in geographically isolated rural communities.
Conclusions
In the quasi-experimental analysis, telehealth use was significantly associated with higher mammogram receipt among rural women; however, this association was not observed among urban women. These findings suggest that telehealth may be particularly beneficial in improving mammography screening among rural individuals who typically experience greater structural barriers to accessing health care. The findings also imply the potential of telehealth to bridge geographic disparities in mammogram receipt by creating new opportunities for engagement outside of traditional in-person care. Spatial analyses indicated that rural areas experiencing concurrent increases in telehealth and mammography utilization were more spatially dispersed than urban areas.
Authors’ Contributions
O.A., P.M., C.M.P., and J.R. obtained funding; N.S. and O.A. conceptualized the research question; N.S. conducted the quasi-experimental analyses; P.M. conducted the spatial analyses; N.S., P.M., and S.C.M. wrote the first draft of paper; N.S. edited the paper; C.M.P. provided the data; and O.A., C.M.P., J.R., and P.M. reviewed and provided critical feedback for the paper.
Ethical Considerations
The study protocol was approved by the MultiCare Health System Institutional Review Board. The approval number is 2023/10/2.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the