
Abstract
Introduction
Women in the United States have a life expectancy of 81 years, compared with 76 years for men. 1 Although women live longer than men, approximately 25% of their lifespan is also spent experiencing higher rates of morbidity and disability, impacting quality of life.2,3
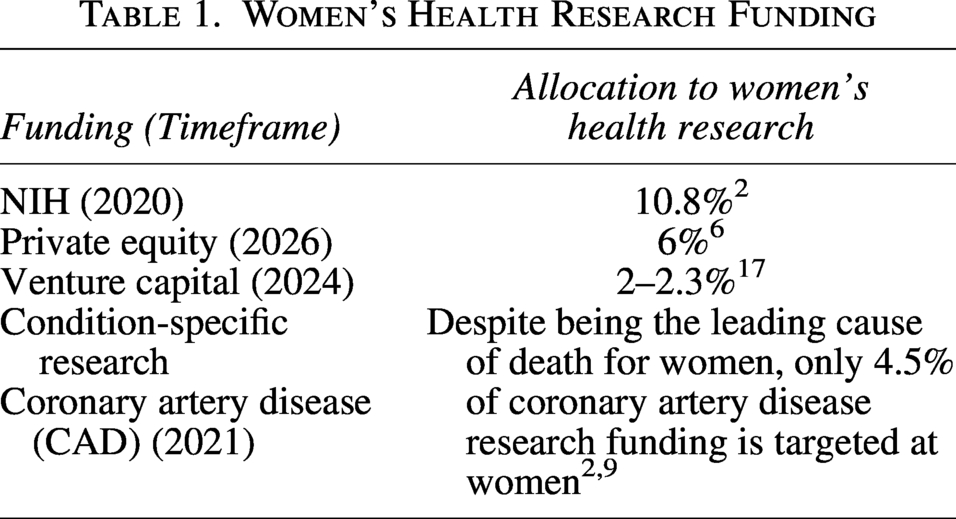
Despite representing half the population, women’s health received less than 11% of National Institutes of Health (NIH) research funding and only 6% of private health care investment.2–8 (Table 1) Funding disparity occurs across both the private and public research sectors, as women’s health is often viewed as a niche market by investors. 9 This funding gap persists even though women make 80% of health care purchasing decisions.7,8 Diseases affecting women exclusively (e.g., menopause), disproportionately (e.g., osteoporosis), or differently (e.g., heart disease, bleeding disorders, mental health conditions) remain understudied.10–12
Women’s Health Research Funding
In conditions that affect all, but affect women disproportionately or differently, women of varying ages, race and ethnicities, and socioeconomic status are not always well represented in clinical trials. In some cases, women are excluded during certain life stages (e.g., women of childbearing potential, pregnant or lactating women).13,14 In the United States, women were actively excluded from clinical research until the early 1990s, creating gaps in data and understanding of how to address potential sex differences during the development of medical products. Updated regulations and guidance from both the NIH and the U.S. Food and Drug Administration (FDA) have sought to encourage the participation of women in clinical research.15,16 These efforts have been successful in increasing the participation of women in clinical studies, although women remain underrepresented overall.
Gaps in women’s health research exist across the spectrum, from basic scientific discovery and preclinical studies through clinical trials to the clinical use of new therapies. These challenges impede the development, approval, and application of effective treatments for conditions that affect women. Diagnosis and treatment for medical conditions as they pertain to women are hindered by a variety of factors, including
Limited research prioritization Limited understanding of female physiology and pathophysiology Limited understanding of changing pharmacodynamics and pharmacokinetics in the context of hormonal changes during menarche, perimenopause, and menopause How the above contribute to an insufficient understanding and identification of health outcomes relevant to women and a lack of clear, well-defined women-centered endpoints Gaps in real-world data (RWD)/real-world evidence (RWE) relevant to health outcomes across women’s life stages Underrepresentation of women in research across biopharmaceutical research fields and in research sample populations A lack of clear regulatory and reimbursement pathways to spur innovation to address the various health needs of women across their lifespan
These gaps hinder progress throughout the drug development pathway, from discovery to clinical application, contributing to delayed diagnoses, limited treatment options, and poorer health outcomes for women.
On November 20, 2025, the Reagan-Udall Foundation for the FDA (the Foundation), in collaboration with the Milken Institute’s Women’s Health Network, hosted an invitation-only roundtable with thought leaders encompassing diverse stakeholder perspectives, including women’s health advocates, clinicians, drug developers, researchers, regulatory scientists and strategists, and investors. Participants discussed unmet needs in drug development to address women’s health, exploring lingering pain points and potential solutions along the drug development life cycle for conditions affecting women exclusively, differently, or disproportionately.
This report aims to capture the actionable solutions shared during the roundtable discussion to close these gaps and advance drug development that acknowledges and measures natural phenomena in women’s health and lifespan.
Roundtable Discussion
A Drug Development Journey Map (Supplementary Appendix SA1), displaying key pain points across the development continuum, provided the foundational framework for the discussion. For various therapeutic areas, participants considered how the general pain points manifest for drug products designed for use in conditions affecting women exclusively at different life stages (e.g., pre-menarche, reproductive years, pregnancy and postpartum, perimenopausal, post-menopausal) and in conditions affecting women disproportionately or differently. Participants also explored how benefit/risk considerations are weighed in drug development as it pertains to addressing the health needs of women. (see Supplementary Appendix SA4).
Proposed Solutions
To address the persistent challenges in women’s health drug development, the discussion culminated in a set of targeted solutions designed to mitigate pain points across the entire research and development continuum. These solutions focus on three primary areas:
Expanding opportunities for pre-competitive, multisector research collaboration, Modernizing study trial design while ensuring that women’s voices and lived experiences inform research priorities, and Enhancing benefit-risk assessment tailored to women’s health in both pre-market and post-market drug development.
Each solution was formulated to be both specific and scientifically grounded, aiming to drive meaningful progress and close critical gaps in women’s health innovation.
Opportunities for pre-competitive, multisector research collaboration
Women’s health research should not be viewed as a niche market; rather, it requires broad collaborative efforts to drive meaningful progress. Advancing women’s drug development depends on collaboration across the entire ecosystem, including patients, industry, academia, and government.
Roundtable participants identified key aspects of multi-sectoral partnerships to advance sharing of knowledge, data, research, and business strategies in pre-competitive spaces. These collaborations are essential to overcoming barriers in developing products that address women’s unique health needs throughout their lives. Priority pre-competitive areas include advancing the understanding of female physiology and pharmacokinetics across hormonal cycles, expanding ecosystem-wide data collection across subpopulations and conditions, developing appropriate artificial intelligence (AI) models to analyze clinical trial data, and supporting citizen science initiatives that gather women’s health data over time.
Collaboration and data-sharing can be supported through the establishment of consortia or centers of excellence. Multi-sectoral and multi-sponsored partnerships drive innovation and foster a culture of open, transparent sharing of scientific and business insights. This approach de-risks research initiatives and can provide governance and programmatic infrastructure to support scientific exchange and coordinate regulatory communication. It also prevents duplication of effort, reduces wasted resources, and builds trust among stakeholders, ultimately accelerating meaningful change in women’s health research and development.
Participants emphasized that it is essential to establish a comprehensive research repository for widespread use. The repository should contain completed basic research, pre-clinical work, and results from interventional and observational clinical trials. As outlined in 42 U.S.C. § 282(j), the results of interventional clinical trials should be posted publicly regardless of outcome. This principle should also be applied to basic and pre-clinical research. Insights from successful trials, as well as those with null or negative findings, should be shared to prevent unnecessary duplication of research.
In addition to research findings, documenting business strategies to launch research startups (including the barriers and stumbling blocks) within the repository will help users identify successful strategies relevant to their context and minimize repeating failed strategies. Complementing this, incubator and accelerator programs can facilitate the exchange of business strategies by enabling startups to engage directly with experienced biotech professionals and potential commercialization partners.
A comprehensive, standardized infrastructure to collect, report, store, and exchange data is urgently needed in women’s health research. Such a foundational framework could guide how data are stored within the research repository and shared among stakeholders. Rare disease research provides a framework for successful pre-competitive data sharing (i.e., Rare Disease Cures Accelerator-Data and Analytics Platform (RDCA-DAP®), Rare Disease COA Consortium).18,19 Areas for pre-competitive data sharing beneficial for women’s health research may include ecosystem-wide data collection in women at various life stages, leveraging AI to collectively mine existing trial data, and supporting citizen scientist initiatives where women share health data over their lifespan. Streamlined partnerships with digital health tool innovators offer opportunities to track outcomes and collaborate more effectively. There are also opportunities for drug developers to share the cost of funding clinical studies to meet FDA-mandated data requirements, as exemplified by the TRAVERSE study supporting the safe use of testosterone replacement therapy in men with low testosterone and high risk for or pre-existing cardiovascular disease (CVD). 20
Clear, proactive communication with regulatory agencies is essential for progress, including expanded opportunities for interaction with the FDA throughout the drug development process. For example, establishing a Women’s Health Center of Excellence at the FDA would centralize expertise. The CDER Center for Real World Evidence Innovation specifically supports the advancement of RWE, for instance, as does the Oncology Center of Excellence. Engaging regulatory bodies like the FDA in pre-competitive settings to agree on benchmarks, models, and pathways can streamline innovation. Early and frequent conversations with regulators enable discussions about risks associated with non-traditional women-centered endpoints. Efficiency can be improved by establishing expedited pathways to meet unmet needs in women’s health, such as priority vouchers for women-focused drug development.
Areas for Investment and Action Summarized:
Research Collaboration
Create and maintain a prioritized list of women’s health conditions with unmet needs. Develop proposals to address these conditions and maintain a dashboard to track progress. Analyze research data for sex differences using outcome measures that would capture potential differences. Research Repository and Comprehensive Data Infrastructure
Create and maintain a research repository of research methodologies and research results. Create and maintain a repository of business strategies. Invest in systems for data collection, sharing, and analysis, including digital health tools and AI. Regulatory Communications
Foster ongoing, transparent engagement with regulatory agencies and advocate for women-centered regulatory processes. In the spirit of partnership, transparently share fundamental testing requirements, protocol parameters, and other non-proprietary guidance received from FDA and other stringent health authorities. Align with FDA on registrational endpoints with a focus on disease-specific primary or surrogative endpoints.
Modernizing study trial design while ensuring that women’s voices and lived experiences inform research priorities
Modernizing study trial design is another important focus. It is necessary to understand whether treatments affect women differently from men and ensure that trial enrollment is proportional to prevalence of a condition in women. Patients should drive research questions, inform endpoints of relevance, and help shape study designs that facilitate engagement, recognizing that patients are not monoliths. 16 How clinical trials are conducted also needs revising to facilitate enrollment and trial completion.
Patient-reported outcomes (PROs) must be sensitive and relevant to women, not just company-specific. Not all PROs are validated in a context of use per FDA requirements for determining fit-for-purpose; therefore, validation should be a requirement. There is a need for PROs specific and relevant to women that accurately represent the construct being studied, are reliable, and meet regulatory and/or clinical requirements. The availability of core templates, such as semi-structured interview guides and psychometric analysis plans, can expedite the identification and validation of relevant well-defined women-centered endpoints for inclusion at the trial design stage. Again, having well-defined women-centered endpoints and PROs requires frequent conversations with regulators. Discussions need to address potential benefits and risks of using nontraditional endpoints, such as quality of life, that are more reflective of women’s health concerns and priorities.
One problem is not only underrepresentation of women in clinical trials but also a lack of data analysis by sex even when women are included. It is important to use appropriate clinical outcome assessments to detect meaningful sex differences in endpoints and to provide incentives for advancing research to determine whether sex differences exist (e.g., using depression scales that capture atypical depressive symptoms often seen in women). Researchers should be analyzing data for sex differences whether they expect them or not and using outcome measures that will capture differences. Incentives may be used to support powering studies accordingly or retrospectively analyzing collected data.
Clinical trial modernization efforts include decentralized visits and tele-visits, which help meet women where they are by recognizing time constraints and familial commitments. Such modifications should be implemented to alleviate additional burdens during trial participation. Trial modernization also requires updating ethics to reflect more equitable benefit-risk discussions, including women as research partners, and removing barriers known to dissuade women from participating in clinical trials (e.g., contraception requirements, heavier burden of informed consent considerations imposed on women of childbearing age). 21
Including payer perspectives and formalizing access strategies early in drug development ensures that relevant patient subgroups and well-defined women-centered endpoints are central to eventual access and reimbursement decisions.
Areas for Investment and Action Summarized:
Create forums to bring women’s voices to the table early in the drug development process. Inclusion across the drug development spectrum will meaningfully inform the patient experience, identify areas most relevant to address in clinical trials (including well-defined women-centered endpoints and barriers to enrollment), and to understand health outcome preferences. Collected information and patient preferences can then be communicated to and understood by FDA when assessing the benefit–risk profile of new therapies. Include women across all ages, races, ethnicities, ancestries, geographies, and socioeconomic status pertinent to the scientific questions and data being collected.
Enhancing benefit-risk assessment tailored to women’s health in both pre-market and post-market drug development
A significant barrier in women’s health research is the way benefit and risk are evaluated during drug development and whether these evaluations truly address women’s unique health needs. In the short term, clinical trials should focus on endpoints that can be measured within the pre-market phase, such as immediate therapeutic effects and safety signals. For long-term outcomes, post-market monitoring should track effects that take longer to manifest, ensuring that both immediate and delayed responses are captured. Defining clear, women-centered endpoints for both phases is essential to accurately assess benefit and risk for women.
Women are not a homogeneous group, and responses to interventions may vary widely due to factors such as age, ethnicity, and life stage. Menopause, for example, illustrates the diversity of experiences among women. Women’s physical and emotional experiences during perimenopause and menopause are influenced by sociocultural contexts, concurrent health conditions, and the quality of support they receive from the health care system.22,23 Without inclusive studies that represent women across different backgrounds, research risks making inaccurate assumptions and overlooking important differences.
Engaging women early and consistently in the drug development process is critical. Understanding their health priorities, definitions of therapeutic benefit, care preferences, and access barriers informs the generation of PRO data and validated and meaningful endpoints for clinical studies. 24 This approach helps address clinical trial challenges, such as recruitment, and guides the selection and measurement of meaningful endpoints. Additionally, incorporating women’s preferences enhances the accuracy of benefit-risk assessments throughout their lifespan.
Insurance coverage and economic analysis are also critical throughout the drug development process. Evaluating the cost-effectiveness and broader benefits of interventions can assist in determining the viability and usability of a product post-market.
Areas for Investment and Action Summarized:
Utilize clinical assessments that address women’s specific health needs, incorporating PROs, patient and public involvement (PPI), and real-world experiences. Engage women as partners throughout the drug development cycle to understand what matters most to them, how they define therapeutic benefit, and what barriers they face. This approach can improve clinical trial recruitment and ensure that measured outcomes are meaningful. Consider accepting greater uncertainty or risk when it aligns with women’s preferences and priorities, while still prioritizing patient safety. Women may be willing to take greater risk from a therapeutic because they value the benefit more. This is especially important when defining acceptable risk in women of childbearing potential and pregnant women.
Next Steps
The robust conversation among roundtable participants identified persistent challenges and potential solutions throughout the drug development life cycle. This collaborative effort culminated in a call for immediate, actionable steps in three critical areas:
Engaging, recruiting, and retaining women in clinical trials. Prioritizing sex-specific endpoints in pre- vs. post-market assessment of safety, efficacy, and/or effectiveness. Exploring the opportunity for RWD to identify and characterize women during different hormonal cycles and stages and to support and extend clinical trials.
As a next step, we propose a series of workshops, each addressing a specific challenge through the lens of discrete therapeutic areas. The workshops will generate context-specific solutions.
Workshop 1: Develop strategies to improve female engagement in clinical trials
While female representation in clinical trials has improved overall, gaps remain. Overall, women are underrepresented in certain therapeutic areas and acutely under-represented by specific age categories, pregnancy status, and ethnicities, compared with disease burden. One example of underrepresentation is in CVD research, where an assumption of similar disease presentation of women to men led to decades of misidentification of symptoms, delayed diagnosis, or misdiagnosis of CVD in women. 9
The objective of this workshop is to improve the enrollment of all women who would benefit from a therapeutic into clinical trials, remain engaged, and benefit from those trials.
The workshop will:
Explore specific information and design challenges in discrete therapeutic areas. Discuss the need for modernization of ethics and institutional review board processes in an age of increasing patient partnership in trials and novel technologies for data visualization and sharing.
To ground these discussions, focus groups are proposed to understand perspectives on factors that might affect female inclusion in, retention in, and benefit (both real and perceived) of clinical trials in the three identified therapeutic areas.
Workshop 2: Discuss the role of benefit-risk assessment with consideration for the preferences and unmet needs of women in the selection of pre- vs. post-market data requirements and endpoints
For many conditions that affect women exclusively or differentially, as well as for those conditions where women have been routinely excluded from clinical trials, there is a need to accelerate access to safe and effective therapies. Requirements and provisions of accelerated review programs, like FDA’s Expedited Programs, can provide insight on how to structure and prioritize endpoints for evaluation in pre- vs. post-approval trials.
The goal of this discussion would be to explore benefit-risk assessment with consideration for the preferences and unmet needs of women across all sub-groups and life stages. Discussion will explicitly examine considerations for identification of appropriate pre- vs. post-market trial endpoints.
The workshop will explore:
Considerations for accepting greater uncertainty or risk when it aligns with women’s preferences and priorities, while still prioritizing drug safety. Clinical assessments that address women’s specific health needs, incorporating PROs, PPIs, and real-world experiences. How unmet need and registrational (i.e., specific, pre-specified primary outcomes in a clinical trial used to determine if a new therapy provides enough clinical benefit to warrant regulatory approval) and surrogate endpoints might be considered in benefit-risk calculations and inform selection of endpoints in pre- vs. post-market trials (e.g., what aspects of safety and/or efficacy might be explored in post-market study).
Workshop 3: Explore real-world data opportunities to better characterize women during different hormonal stages and support and extend clinical trials
A key benefit of RWD in drug development is the ability to contextualize, on a large scale, treatment use and outcomes. The objective of this third invitation-only discussion will be to explore data that are available in electronic health records or administrative claims to identify and characterize women at different hormonal cycles and stages; outcome trends observed in RWD for specific therapeutic areas and whether they may reflect associations with varying hormonal stages; and how RWD might be leveraged to reduce the burdens on and support clinical trials throughout the drug development pathway. Discussions will surface therapeutic areas where RWD opportunities may be applied in the near vs. longer term and in accordance with regulatory guidance.
The workshop will identify strategies to
Document what is known (and unknown) about treatment effectiveness in the context of hormonal cycles throughout women’s life course. Categorize data, including RWD, needed to define such endpoints throughout the life course and in the context of hormonal changes. Build a matrix to categorize conditions that affect women exclusively, disproportionately, or differently to guide drug development and ensure that sex differences are systematically considered. Guide study design and methodologies using RWD/RWE.
Finally, the three workshops will inform the development of an essential problem list and potential solutions, captured in a dashboard pairing specific pain points in a drug development pathway with potential solutions, by therapeutic area. Therapeutic areas will include only conditions that affect women exclusively, differently, and/or disproportionately
Whether in health care or business, the “essential opportunity list” will illustrate challenges requiring resolution. By mapping challenges within specific therapeutic areas to potential solutions, the dashboard will enable patient advocates, product developers, and regulators to identify pain points that resonate with them and to envision viable solutions to advance.
Conclusion
This roundtable was part of a broad wave of initiatives informing innovation in drug development and regulatory assessment in women’s health. This report offers potential actions to mitigate priority pain points hindering drug development in in women’s health.
Supplemental Material
sj-docx-1-jwh-10.1177_15409996261463009 — Supplemental material for Advancing Women-Centered Product Development: Understanding the Health Needs of Women Roundtable Proceedings
Supplemental material, sj-docx-1-jwh-10.1177_15409996261463009 for Advancing Women-Centered Product Development: Understanding the Health Needs of Women Roundtable Proceedings by Angela B. Hoth, Carla V. Rodriguez, Susan C. Winckler, Smita Abbi, Ayodola Anise, Beth Battaglino, Tiana Golding, Shefali Goyal, Nada Hanafi, Abigail Humphreys, Molly Hyer, Sabrina Johnson, Esther Krofah, Vanessa Perez Patel, Barrett Pignone, Ailie Reasons, and Susan Kornstein
Footnotes
Acknowledgments
Roundtable participants for their contributions: Abel, Ashley; Barletta, Katie; Broecker, Katherine; Brooks, Michelle; Chang, Christina; Cohen, Laura; Fretzen, Angelika; Garner, Elizabeth; Gross, Marielle; Hendricks-Sturrup, Rachele; Krockover, Mitzi; Kweder, Sandy; Neal-Perry, Genevieve; Park, Alexandra; Patterson, Jenica; Powell, Liz; Rock, Charlotte; Rubin, Joshua C.; Shapiro, Molly; Sokolowska, Marta; Wegrzyn, Renee; Yao, Lynne. Participation of FDA employees at the discussion does not represent the official views of, nor an endorsement by, FDA/HHS, or the U.S. Government. Georgia Peeples and Eynat Amir for their help with article preparation and submission.
Author Disclosure Statement
A.B.H. is a consultant for Merck & Co. C.V.R. holds stock in Gilead. S.C.W. is a Board Director and shareholder in Purgo Scientific. S.A., T.G., S.G., V.P.P. are employees of Organon and S.A. holds stock in Organon. S.J. is Founder & Chief Executive Officer of Daré Bioscience. B.P. and A.R. are employees of
Funding Declaration
The Reagan-Udall Foundation for the FDA receives funding from FDA, FDA-regulated industry, and others in the FDA ecosystem. Funding for this project was received from Daré Bioscience,
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.