
Abstract
Genitourinary syndrome of menopause (GSM) is a chronic, progressive condition resulting from estrogen and androgen deficiency that affects 27–84% of postmenopausal individuals. Symptoms include vaginal dryness, dyspareunia, urinary urgency, dysuria, and recurrent urinary tract infections. Despite strong evidence supporting the safety and efficacy of local vaginal estrogen (VE) therapy, treatment remains underutilized due to clinician uncertainty, misconceptions regarding systemic risk, and regulatory warnings. Recent clinical guidelines emphasize vaginal hormones as first-line therapy for GSM. This review summarizes the pathophysiology of GSM, evidence supporting local hormone therapy, safety considerations, and practical prescribing strategies for clinicians. Pearls for clinical practice are discussed, including dosing regimens, formulation selection, patient counseling, and strategies to overcome barriers to treatment adherence.
Keywords
Introduction
Genitourinary syndrome of menopause (GSM) encompasses a constellation of vulvovaginal, sexual, and urinary symptoms caused by declining estrogen and androgen levels after menopause.1,2 These hormonal changes lead to thinning of the vaginal epithelium, loss of elasticity, reduced lubrication, and increased tissue fragility. 3 Clinical manifestations include vaginal dryness, dyspareunia, burning, irritation, urinary urgency, dysuria, and recurrent urinary tract infections (UTIs). 4 GSM affects approximately 27–84% of postmenopausal individuals, with vaginal dryness reported in up to 50–60% and dyspareunia in up to 40% of affected patients.1,5–7
GSM is also associated with significant reductions in quality of life and sexual function. 8 Despite the availability of highly effective treatments, the condition remains undertreated. Studies suggest fewer than 10–20% of symptomatic patients receive vaginal estrogen (VE) therapy. 9
Recent consensus guidelines from the American Urological Association (AUA), Society of Urodynamics Female Pelvic Medicine and Urogenital Reconstruction (SUFU), and American Urogynecologic Society (AUGS) recommend VE as a primary therapy for GSM symptoms. 3 This review summarizes the evidence supporting VE therapy and provides clinicians with practical prescribing guidance in a postmenopausal population.
Evidence for VE Therapy
Symptom relief
A substantial body of clinical evidence supports the efficacy of low-dose VE therapy for the treatment of GSM.10,11 Randomized controlled trials have consistently demonstrated that VE significantly improves vaginal dryness, dyspareunia, irritation, and discomfort compared with placebo.12,13 Furthermore, a systematic review of 53 studies found that VE is clinically effective for the treatment of GSM symptoms including vulvovaginal dryness and burning, dyspareunia, and urogenital symptoms such as urgency, dysuria, and recurrent UTI. 14 In addition to a reduction in patient-reported symptoms, objective physiologic improvements in vaginal tissue health have also been documented. Meta-analyses of clinical trials show that VE facilitates normalization of vaginal pH, increases the vaginal epithelial maturation index, improves lubrication, and meaningfully enhances sexual function.10,12 These therapeutic effects reflect the restoration of estrogen-dependent vaginal physiology, including increased epithelial thickness and greater glycogen production within epithelial cells. 15 Increased glycogen within estrogenized vaginal epithelium promotes Lactobacillus growth and lactic acid production, maintaining an acidic vaginal pH and a protective microbial environment associated with reduced urogenital infection risk. 16
Prevention of recurrent UTIs
The urinary benefits of VE are becoming increasingly recognized, particularly in the prevention of recurrent UTIs in peri- and postmenopausal individuals. Estrogen deficiency leads to significant alterations in the genitourinary tract, including thinning of the urethral epithelium, decreased vascularity, and disruption of the vaginal microbiome.5,6,17 These alterations promote colonization by uropathogenic bacteria and increase susceptibility to infection.18,19 Restoration of local estrogen signaling with VE reverses many of these changes by enhancing epithelial maturation, lowering vaginal pH, and promoting recolonization with Lactobacillus species that inhibit the growth of pathogenic organisms. 20 By restoring the vaginal epithelium and promoting recolonization with protective lactobacillus species, VE therapy reduces the frequency of recurrent infections and therefore decreases the need for repeated antibiotic treatment and health care encounters.21,22 Clinical guidelines from the AUA recommend VE therapy for peri- and postmenopausal individuals with recurrent UTIs when no contraindication to estrogen exists. 23 Randomized clinical trials have demonstrated that VE therapy significantly reduces UTI recurrence rates in postmenopausal women compared with placebo. In a landmark randomized controlled trial, women treated with intravaginal estriol experienced a marked reduction in recurrent infections, an effect attributed to restoration of normal vaginal flora. 21 Subsequent systematic reviews and meta-analyses have confirmed these findings, with recurrence rates decreasing from approximately five infections per year to fewer than two annually when VE is used.10,22 More recently, a large retrospective review of 5,638 hypoestrogenic women prescribed VE for UTI prevention found a >50% reduction in UTI frequency in the year following initiation of therapy. 24 Together, these findings support VE as both an effective treatment for genitourinary symptoms and an effective nonantibiotic strategy for preventing recurrent UTIs in hypoestrogenic populations.
Cost-effectiveness
VE may also provide substantial economic benefits by reducing the incidence of recurrent UTIs and associated health care utilization. UTIs are among the most common bacterial infections among women and account for millions of outpatient visits, emergency department encounters, and antibiotic prescriptions annually in the United States.25,26 They comprise an estimated 1 − 6% of healthcare encounters, corresponding to about 7 million visits annually, and generate at least $1.6 billion in health care costs each year.27,28 Among older adults, UTIs account for approximately 25% of all infections annually. 29
In a retrospective Medicare analysis, UTI-related care comprised roughly one-third of total annual spending among affected patients. 30 As such, UTIs are associated with substantially increased per-patient costs and represent a meaningful contributor to overall Medicare expenditures. 28 Hospitalizations for UTIs further contribute to this burden, with median costs of approximately $10,000 per admission. 31 Notably, VE use in postmenopausal women was associated with a 22% reduction in risk of hospitalization, which may translate into meaningful reductions in UTI-related health care expenditures. 32
Economic modeling studies suggest that broader implementation of VE therapy in eligible postmenopausal patients could yield substantial cost savings. One cost-effectiveness analysis estimated that widespread adoption may reduce UTI-related healthcare expenditures by approximately $6–22 billion annually in the United States, largely through reductions in physician visits, diagnostic testing, and antibiotic prescriptions.18,23 Another cost-saving model estimated that, at a per-UTI cost of $1,222, reductions in UTI frequency with topical estrogen could translate to $3,000–$6,000 in annual savings per beneficiary. 30 These findings suggest that VE therapy is not only clinically effective but may also represent a cost-saving preventive strategy for recurrent UTIs in hypoestrogenic populations.
Safety of VE
Systemic absorption
One of the most common concerns among clinicians and patients regarding VE is the potential for systemic estrogen exposure. However, low-dose VE results in minimal systemic absorption and maintains circulating estradiol levels within the normal range. 33 Pharmacokinetic studies evaluating modern low-dose formulations, including estradiol tablets, softgel capsules, and vaginal rings, consistently show only transient or negligible increases in serum estradiol concentrations following administration. 34 In most cases, serum estradiol levels remain below or within the typical postmenopausal range of approximately 3–10 pg/mL, indicating limited systemic hormonal exposure. A secondary analysis of data from a randomized clinical trial demonstrated that low-dose vaginal estradiol results in transient, low-level increases in serum estradiol concentrations that generally remain within the postmenopausal range. 35
Clinical trials evaluating estradiol vaginal tablets (10 µg) have similarly demonstrated no clinically meaningful elevation in systemic estradiol levels with standard dosing regimens, even during the initial daily induction phase.36,37 These findings reflect the primarily local mechanism of action of VE therapy, which targets estrogen receptors within the vulvovaginal tissues while minimizing systemic distribution. As a result, professional societies including the North American Menopause Society and the American College of Obstetricians and Gynecologists recognize low-dose VE as a safe and effective treatment for GSM, particularly when systemic hormone therapy is not indicated.34,38 Understanding the minimal systemic absorption associated with these therapies is critical for addressing patient concerns and improving clinician confidence in prescribing VE for the management of GSM. Any vaginal bleeding in a postmenopausal patient should undergo evaluation, regardless of whether the individual is using VE. 3
Breast cancer risk
Safety concerns regarding breast cancer have historically contributed to clinician and patient hesitancy surrounding VE use. The AUA/SUFU/AUGS Guidelines on GSM advises clinicians to counsel patients that there is no evidence linking local low-dose VE to the development of breast cancer, and notes that available data do not demonstrate increased recurrence or breast cancer-specific mortality among survivors when used within a shared decision-making framework.3,39 A Danish cohort of postmenopausal women with early-stage ER-positive breast cancer found no overall increase in recurrence or mortality among users of VE therapy. 40 Similarly, population-based cohort studies using national registry data from Scotland and Wales have demonstrated no increase in breast cancer-specific mortality among women who used VE after diagnosis, with some analyses suggesting a small reduction in mortality among users. 41 Additional retrospective and cohort studies have also found no increased risk of recurrence among postmenopausal women with a history of breast cancer treated with VE for GSM.42,43
A recent large systematic review and meta-analysis including over 24,000 breast cancer survivors found no increased risk of recurrence, breast cancer-specific mortality, or overall mortality associated with VE use. 44 Similarly, large population-based studies demonstrate no association between VE use and breast cancer incidence. A nationwide Danish registry-based case-control study nested in a cohort of women aged 50–60 years showed that use of vaginal estradiol tablets was not associated with increased breast cancer incidence. 45 Likewise, long-term observational data from the Women’s Health Initiative and Nurses’ Health Study found no increased risk of breast cancer or other major chronic disease among VE users.46,47 Notably, large-scale epidemiologic analyses of menopausal hormone therapy have consistently shown that, VE is not associated with increased breast cancer risk. 48 These data support guideline-driven counseling that low-dose VE is not associated with increased breast cancer incidence and does not appear to increase recurrence or mortality in most breast cancer survivor populations. These findings reinforce the safety of VE as a local therapy.3,40
Cardiovascular risk
Concerns regarding potential cardiovascular risks associated with estrogen therapy have historically influenced prescribing practices, largely due to data from the Women’s Health Initiative. However, evidence indicates that low-dose VE therapy does not confer cardiovascular risks because systemic absorption is minimal. 46 Large observational cohort studies have demonstrated no increased risk of cardiovascular disease, venous thromboembolism (VTE), stroke, or all-cause mortality among users of VE therapy. In a large prospective analysis from the Nurses’ Health Study, VE use was not associated with increased risks of coronary heart disease, stroke, pulmonary embolism, or cancer compared with nonusers. 47 Similarly, analyses from the Women’s Health Initiative Study reported no increase in cardiovascular events or mortality among women using VE preparations. 46
A large Finnish cohort study found that vaginal estradiol use was associated with a decreased risk of cardiovascular mortality, although this finding may reflect healthy-user bias rather than a direct cardioprotective effect. 49 Importantly, emerging data also support safety in higher-risk populations. In a large, nested case-control study of over 44,000 women with a prior history of VTE, use of vaginal estradiol was not associated with an increased risk of recurrent VTE, suggesting that VE therapy is unlikely to meaningfully increase thrombotic risk even among women with prior events. 50 Taken together, these data support current clinical guidelines indicating that low-dose VE therapy does not increase cardiovascular or thrombotic risk and can be safely prescribed for the treatment of GSM.
VE Formulations
Multiple vaginal hormone formulations are FDA-approved for the treatment of GSM, enabling individualized therapy based on patient preference, symptom distribution, ease of use, and cost (Fig. 1). Current evidence demonstrates that several low-dose VE preparations have comparable efficacy in improving vulvovaginal symptoms and reversing physiologic changes associated with estrogen deficiency. 10 Accordingly, the selection of local hormone formulation should be guided by factors that prioritize patient adherence (such as comfort with the delivery system), rather than differences in clinical effectiveness.
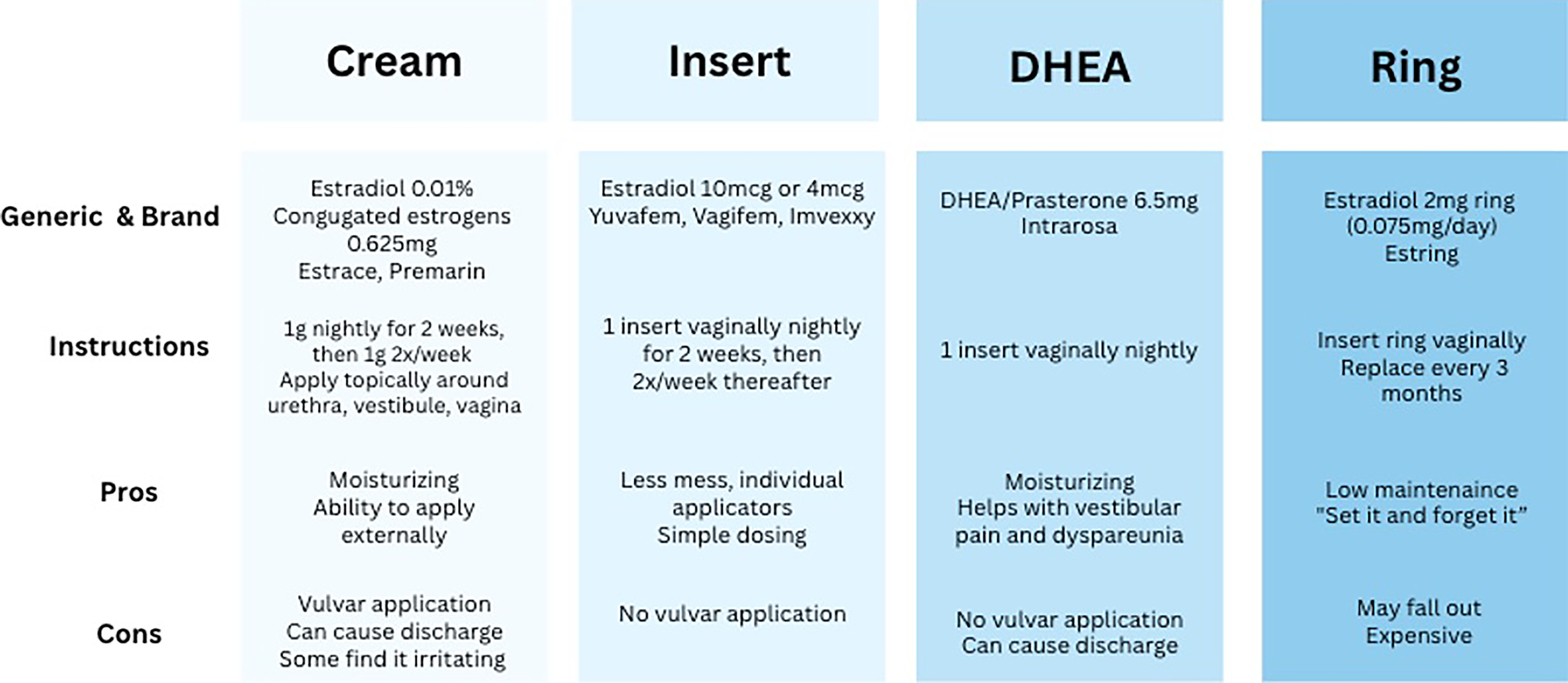
Vaginal hormone formulations.
Vaginal cream
VE cream remains one of the most widely used topical hormone therapies. It is available in multiple formulations, including estradiol 0.01% cream (estrace) and conjugated equine estrogens (premarin 0.625 mg/gm). Both creams are commonly prescribed using an initial loading phase consisting of nightly application of 1 g for approximately 2 weeks, followed by a maintenance regimen of 1 g twice-weekly application. Cream formulations provide flexibility in dosing and allow direct application to both vaginal and external vulvar tissues, which may be particularly beneficial in patients with prominent vulvar symptoms such as dryness, fissures, or irritation. 38 Some patients report that creams can feel messy or inconvenient, which may affect adherence. Patients occasionally report irritation secondary to the cream itself, which can often be mitigated by switching brands or manufacturers (i.e., changing from an alcohol-based cream to an oil-based cream). Finally, initiation of VE may slightly increase the risk of yeast infections, but there is not sufficient data to describe the quantity of increased risk. However, it is thought that the vaginal microbiome will recalibrate as the body adjusts to the lower vaginal pH associated with VE, thus the risk of yeast infections is only elevated at initiation, not long term. 51
Vaginal tablets
Vaginal estradiol tablets are another commonly used formulation. The 10 µg estradiol vaginal tablet (Vagifem) is typically administered nightly for 2 weeks during the induction phase and then continued twice weekly for long-term maintenance therapy. Compared with estradiol cream, estradiol tablets deliver a lower standardized dose and are often preferred by patients who desire a “less messy” and more discreet administration method. 36
Vaginal capsules
More recently, estradiol softgel capsules (Imvexxy) have been introduced as an ultra-low-dose option available in 4 µg and 10 µg. These capsules are inserted digitally without the need for an applicator and have been shown to effectively improve symptoms of GSM while maintaining minimal systemic estrogen exposure. 37 Their small size and ease of insertion may improve adherence among patients who prefer a simplified dosing method. Of note, Imvexxy is pink in color, and patients have reported pink discharge and concern for postmenopausal bleeding (PMB). It is important for the clinician to distinguish true PMB from discharge tinted by the capsule.
Vaginal ring
Long-acting VE delivery is also available in the form of the estradiol-releasing vaginal ring (Estring), which provides continuous low-dose estradiol release over a 90-day period. The vaginal ring sits in the upper one-third of the vagina and offers several advantages, including convenience, reduced need for frequent dosing, and improved adherence in patients of different abilities, including those with decreased manual dexterity or dementia. 10 The VE ring can be inserted and removed either by the provider or the patient themselves; however, most patients report that they are comfortable doing insertion and removal after brief coaching from their physician. 52 Additionally, the VE ring can stay in place during intercourse; however, if the patient desires, it is acceptable to remove it and replace it shortly after. The ring can cause minor discomfort if it sits too low in the vaginal canal, which can occur due to changes in intra-abdominal pressure (i.e., associated with straining or constipation). If this happens, the patient can simply use a clean finger to readjust the position of the ring into a more comfortable spot (Estring® Package Insert).
Vaginal dehydroepiandrosterone
In addition to estrogen-based therapies, intravaginal dehydroepiandrosterone (DHEA), marketed as prasterone (Intrarosa), represents an alternative local hormonal treatment for GSM. DHEA is converted intracellularly within vaginal tissues into both estrogens and androgens, allowing local restoration of sex steroid signaling without significant systemic hormone exposure. Clinical trials have demonstrated that vaginal DHEA improves dyspareunia and vaginal tissue health, making it particularly useful in patients with persistent vestibular pain or painful intercourse. 53 A recent randomized control trial directly compared vaginal DHEA with vaginal estradiol and concluded that DHEA is superior to estradiol in relieving severe dyspareunia; however, estradiol was better at improving signs of vulvovaginal atrophy. 54
Together, these formulations provide clinicians with multiple options to individualize treatment. Despite the range of available therapies, important limitations remain, including non-specific drug delivery, challenges with adherence, and a lack of well-tolerated alternatives for those who cannot or prefer not to use estrogen. These gaps highlight the need for more targeted, patient-centered innovations in treatment design. Shared decision-making remains pivotal in formulation selection and should be guided by patient preferences, symptom distribution, cost, and anticipated adherence. Notably, all approved vaginal hormonal therapies demonstrate similar efficacy in improving vulvovaginal symptoms and restoring vulvar anatomy and physiology in the setting of estrogen deficiency.
Clinical Pearls for Prescribing VE
Use an induction phase
Most VE therapies require an initial induction phase to restore vaginal epithelial health followed by long-term maintenance dosing. Standard regimens typically involve daily application for approximately two weeks, followed by twice-weekly maintenance therapy. This loading phase allows rapid restoration of estrogen-dependent vaginal physiology, including epithelial thickening, increased vascularization, and improved lubrication, often contributing to early symptomatic relief. 10
Treat indefinitely
Since VE is primarily used to treat GSM, it is important to note that GSM is a chronic and progressive condition. Discontinuation of therapy frequently leads to recurrence of symptoms. The physiologic changes associated with estrogen deficiency, including decreased lubrication, epithelial thinning, and increased vaginal pH, re-emerge when therapy is stopped. Patients should therefore be counseled that VE is generally intended as long-term maintenance therapy to sustain tissue health and maintain symptom relief. 1 In addition to treating GSM, VE is also indicated in other settings such as urethral prolapse, before or after vaginal surgery, genitourinary syndrome of lactation, recurrent UTIs, and more. In these cases, it can be trialed for a period of time until resolution of symptoms.
Let adherence guide formulation
Adherence to therapy is strongly influenced by patient preference and practical considerations. Although available VE formulations demonstrate similar efficacy, factors such as cost, perceived messiness of creams, fear of hormone exposure, skin irritation from a specific formula, and confusing medication labeling may influence patient adherence. Clinicians should therefore engage in shared decision-making when selecting a formulation and remain open to switching products if adherence issues arise. 38 Additionally, clinicians should monitor adherence and encourage changing formulations if a patient would benefit from trying a different therapy.
Barriers to VE prescribing
Despite robust evidence supporting the safety and effectiveness of low-dose VE for the treatment of GSM, it remains substantially underutilized in clinical practice. 55 GSM affects an estimated 50–70% of postmenopausal individuals, yet only a minority of symptomatic patients receive treatment with local estrogen therapy.1,56 Population-based studies demonstrate a marked gap between symptom prevalence and treatment. Analyses of U.S. Medicare claims data including more than 1 million women with GSM-related diagnoses found that only 9.0% filled a prescription for VE, despite guideline recommendations identifying local therapy as first-line treatment. 9 Similarly, a large TriNetX database study reported that more than 70% of women with documented GSM received no prescription therapy, highlighting substantial undertreatment even among patients already engaged in health care systems. 57 Survey-based studies reveal that many women experiencing GSM symptoms never seek medical care or remain untreated after evaluation, often because clinicians fail to initiate discussion about vulvovaginal symptoms.55,58 The under-prescribing of VE is multifactorial. Clinician misconceptions regarding systemic risks, particularly breast cancer, cardiovascular disease, and thromboembolism, persist despite evidence demonstrating minimal systemic absorption with low-dose vaginal preparations. 34 Regulatory boxed warnings on VE products, originally derived from data on systemic hormone therapy, have further amplified patient and clinician concerns and may discourage treatment initiation. 38 In November 2025, the U.S. Food and Drug Administration announced the initiation of labeling changes to remove broad boxed-warning language from menopausal hormone therapy products, including warnings that had been applied to low-dose VE despite its distinct pharmacokinetic and safety profile. 59 This regulatory shift reflects growing recognition that boxed warnings extrapolated from systemic hormone therapy data may have overstated risks for local vaginal preparations, which demonstrate minimal systemic absorption and have not been associated with increased breast cancer, cardiovascular disease, VTE, or mortality in large observational studies and systematic reviews.34,44,46,47,59 Removal of misleading boxed-warning language may therefore reduce clinician hesitation, improve patient confidence, and help align prescribing practices with contemporary evidence and guideline recommendations. However, updated labeling alone is unlikely to eliminate underuse without parallel clinician education, patient counseling, and normalization of discussions about genitourinary and sexual symptoms. Patient-level barriers exist and include fear of hormone exposure, embarrassment discussing sexual symptoms, cost and access limitations, and limited awareness that GSM is treatable. 58 Many clinicians, including OB/GYN and primary care physicians, report insufficient training in sexual medicine and menopause care, contributing to low screening rates and inconsistent prescribing. 38 There is also a misconception that a pelvic exam is needed to diagnose GSM and prescribe VE; however, it is reasonable to initiate treatment based on patient-reported symptoms alone per the 2025 AUA Guidelines. 3 Addressing these barriers through clinician education, regulatory reform, and increased patient awareness is essential to closing the treatment gap and improving quality of life for individuals with GSM.
Future directions
Future research in VE therapy is evolving beyond traditional treatment paradigms and is increasingly focused on optimizing hormonal targeting, expanding therapeutic options, and addressing understudied physiologic states. An emerging area of interest involves the role of androgens in vulvovaginal health. Androgen receptors are widely distributed throughout vulvovaginal tissues, and endogenous testosterone levels decline with menopause, contributing to symptoms such as vaginal dryness, decreased elasticity, and sexual dysfunction. Therapies such as intravaginal DHEA have shown efficacy in improving dyspareunia and sexual function by locally converting to both estrogens and androgens within genital tissues.11,53 A recent RCT directly comparing vaginal DHEA with VE demonstrated that DHEA is superior in relieving severe dyspareunia. 54 More studies are needed to evaluate safety and efficacy of formulations combining estrogens and androgens.
Expanding research is also examining the impact of hormonal changes across a broader range of clinical contexts beyond menopause. Fluctuations in sex steroid levels, regardless of etiology, can significantly affect genitourinary health. Hypoestrogenic states associated with lactation, use of hormonal contraceptives, certain medications, and gender-affirming therapies may all contribute to symptoms similar to GSM, including vaginal dryness, irritation, and dyspareunia. 60 Recognizing these diverse clinical scenarios is critical to ensuring appropriate identification and treatment of patients who may benefit from local hormone therapy.
In parallel, growing interest in the vaginal microbiome has highlighted its essential role in maintaining urogenital health. Estrogen supports a lactobacillus-dominant environment, which helps maintain an acidic vaginal pH and protects against pathogenic overgrowth.16,61 Research suggests that the onset, severity, and type of GSM symptoms experienced may be associated with changes in vaginal microbiota. 62 These findings suggest a potential adjunctive role for microbiome-directed therapies alongside VE, although further research is needed to define their long-term efficacy and clinical integration.
Conclusion
VE therapy is an FDA-approved, highly effective, and well-established treatment for genitourinary symptoms associated with estrogen deficiency, yet it remains underutilized in clinical practice. Robust evidence supports its efficacy and safety across multiple formulations, with contemporary guidelines recommending local estrogen therapy as first-line treatment for symptom management of GSM and prevention of recurrent UTIs. Clinicians should be familiar with available formulations, dosing strategies, and patient counseling techniques to optimize adherence and improve patient outcomes.
Footnotes
Acknowledgments
The authors are grateful to the Sexual Medicine Research Team for their support and guidance in pursuing this research.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.