
Abstract
Background:
Unwanted or mistimed pregnancies are pregnancies that occur in women who do not intend to become pregnant or did not desire another child at the time of conception. Ensuring access to contraception is important for both preventing unwanted pregnancy among active duty service women (ADSW) and preserving their right to reproductive autonomy. Women’s Health Clinics (WHCs), available on some installations, bases, or duty stations owned and operated by the United States military, are intended to improve contraceptive access. This study aims to determine the association between availability of WHCs and unwanted pregnancy among ADSW.
Methods:
Using data from the 2020 Women’s Reproductive Health Survey of ADSW we examined unwanted pregnancy in 2,939 ADSW who reported pregnancy in the last 12 months. Bivariate analyses and weighted binary and multivariable logistic regressions were used to assess the relationship between women reporting an unwanted pregnancy and having a WHC at their installation.
Results:
We identified 354 unwanted pregnancies. Having a WHC at their current installation was significantly associated with a 39% decreased odds of unwanted pregnancy (aOR = 0.61; 95% CI: 0.42–0.88).
Conclusions:
Having a WHC at an ADSW’s installation is associated with significantly decreased odds of unwanted pregnancy. This suggests that access to specialty women’s health care at duty stations may promote reproductive autonomy among ADSW, contributing to the prevention of unwanted or mistimed pregnancies, ultimately enhancing mission readiness.
Keywords
Introduction
Unwanted pregnancies are those that occur in individuals who do not want to become pregnant or did not want another child at the time of conception. They occur when conception is not planned or expected as a result of sexual intercourse. Unwanted or mistimed pregnancies represent a critical public health issue in the United States, with an estimated 41.6% of pregnancies not being planned or expected in 2019. 1 Unwanted or mistimed pregnancies have significant associations with adverse maternal and infant outcomes, such as maternal depression, preterm birth, low birthweight, and interpersonal violence. Women who experience unwanted or mistimed pregnancies are also more likely to experience maternal complications and mental health consequences. 2 Unwanted or mistimed pregnancy may also have negative developmental and socioeconomic effects for other children in the household. 3 Women with an unplanned pregnancy have higher levels of depressive symptoms during the perinatal period compared with those with a planned pregnancy. 4
Use of contraceptives can help to prevent both unwanted and mistimed pregnancies. However, some sexually active individuals who do not desire pregnancy choose not to use contraception for various reasons, such as lack of awareness, misinformation, concerns about the safety of contraceptives, prior adverse drug reactions or unwanted side effects when taking contraceptives, or simply not wanting to use contraception.5,6 Educational interventions aid individuals in making informed decisions regarding contraceptive use to prevent unwanted or mistimed pregnancy.7,8
There are approximately 1.3 million female service members across five active duty branches, comprising 17.9% of the total active-duty force, of which 95% are of reproductive age.9,10 Estimates suggest approximately 4.5% of active duty service women (ADSW) will experience an unwanted or mistimed pregnancy each year, which indicates a higher rate of unintended pregnancy among ADSW compared with the U.S. general population, which has an unintended pregnancy rate of 4.5%. 11 Military service can lead to disrupted reproductive health care access; one-third of military service members experience a formal relocation each year. 12 Additionally, approximately half of the continental U.S. military locations are located within a health professional shortage area, also known as a health care desert. 12 This may limit the ability of ADSW to access reproductive care, which could lead to a lack of contraceptive education or access that can result in an unexpected or unwanted pregnancy and limit the ability of ADSW to practice reproductive autonomy, or the power to make decisions regarding contraceptive use, pregnancy and childbearing for oneself. Other identified barriers to contraceptive care for ADSW that have been highlighted in the literature include difficulty obtaining an appointment, provider reluctance to discuss contraception, inability to obtain their desired contraceptive option, and inability to get a full supply of contraception prior to deployment.13–15
For ADSW, the consequences of unwanted or mistimed pregnancy extend to their career. According to a 2021 scoping review on unintended pregnancy among ADSW in the U.S. military, unwanted or mistimed pregnancy is associated with negative interpersonal and career outcomes for ADSW, including punishment, early return from deployment, and expulsion from military service. 16 Unwanted or mistimed pregnancy also has the potential to contribute to a substantial amount of readiness days lost due to the physical limitations, temporary duty restrictions, and limited deployment eligibility that result from pregnancy, all of which can negatively impact mission readiness. 11 Because of the detrimental impacts to health, personal life, and career that can result from unwanted or mistimed pregnancy, encouraging reproductive autonomy and contraceptive use among ADSW is necessary.
Within the Military Health System (MHS), women’s health clinics (WHCs) provide preventive education, measures, and resources for family planning, including contraceptive services that may help to reduce unwanted pregnancies, assisting individual service members in preventing pregnancy and/or spacing pregnancies in a manner that accommodates both personal and professional goals. In addition to family planning and contraceptive services, WHCs also provide a range of other specialized women’s health services, including pregnancy care, urogynecology, and complex gynecology.17,18 Evidence suggests that specialized reproductive health clinics are more likely to provide services that make contraceptive use more accessible for patients, resulting in a higher probability of continuously using highly effective contraception. 19 The first comprehensive WHC in the MHS was opened in 2018 at Naval Medical Center San Diego.20,21 While access to WHCs and contraceptive services have expanded, they are not currently available on all military installations (bases or duty stations owned and operated by the U.S. military). 21 Failure to ensure access to contraceptive care can lead to readiness and cost consequences for the Department of Defense (DoD) and the MHS.11,22 An unexpected pregnancy may require early return from a deployment or result in career limitations or voluntary separation, decreasing the number of operationally ready personnel. 16 While more research is needed on WHCs in the military, in civilian literature WHCs have been associated with higher patient satisfaction and higher rates of preventive and gender-specific screening. 23
This study aims to assess the impact of the availability of WHCs at military installations on unwanted pregnancy among ADSW who were pregnant at any time in the past 12 months. We hypothesize that the presence of a WHC will be associated with a reduction in the prevalence of unwanted pregnancies. Results from this study will inform future interventions to expand access to reproductive care for ADSW, ensuring a fit and ready female force, regardless of career demographics and location.
Methods
Data source
Data were analyzed from the 2020 Women’s Reproductive Health Survey (WRHS) of Active-Duty Service Members. 21 This survey, commissioned by the DoD and conducted by the RAND Corporation, assessed how servicewomen experienced family planning services and counseling. It was conducted from August to November of 2020 among ADSW in the U.S. Air Force, Army, Coast Guard, Marine Corps, and Navy. The survey was administered electronically. Those who were trainees or at military academies were excluded from sampling. The WRHS used a stratified random sample, based on service branch and pay grade, of 249,128 eligible ADSW, resulting in 131,113 ADSW selected to be contacted for participation. The final analytic sample included responses from 23,950 ADSW. The overall weighted response rate was 17.8%. Complete information about the survey and sampling frame can be found in the WRHS research report. 21
Study sample
The initial study sample included participants who reported that they had been pregnant at any time in the past 12 months (n = 3,566). 21 Those who reported they were not sure if their current installation/duty station had a WHC were excluded as this was the primary study exposure (n = 627). The final study sample included 2,939 participants (Table 1). 21
Unwanted pregnancy
Information regarding unwanted pregnancy was self-reported. To understand the woman’s intentions and desires regarding pregnancy, women were asked the question (Q63) “Just before you became pregnant, did you yourself want to have a/another baby at any time in the future?” 21 The response options were “Q63 = 1: wanted a/another baby in the future,” “Q63 = 2: did not want to have a/another baby at any time in the future,” and “Q63 = 3: not sure, Q63.” 21 For this analysis, unwanted pregnancy was defined as a dichotomous outcome (yes/no): yes, “Q63 = 2: did not want to have a/another baby at any time in the future,” or “Q63 = 3: not sure if wanted a/another baby at any time in the future,” versus no, “Q63 = 1 wanted a/another baby in the future.” 21 For a sensitivity analysis (N = 2,809), we excluded the “Q63 = 3: not sure if wanted a/another baby at any time in the future,” group and classified unwanted pregnancy as yes, “Q63 = 2 did not want to have a/another baby at any time in the future,” versus no, “Q63 = 1 wanted a/another baby in the future (Table 1).” 21
Exposures
The primary study exposure was the presence of a WHC at the respondent’s current installation.
The presence of a WHC at the respondent’s current installation was assessed by asking respondents, “Q17: Does your current installation or duty station have a WHC?” 8 Responses were categorized as “Yes,” “No,” or “Not sure.” 21
Sociodemographic and military characteristics
Sociodemographic characteristics included age (18–24, 25–34, ≥35), non-White minority race/ethnicity (yes/no), education (high school or less, some college, Bachelor’s degree or greater), marital status (not married nor cohabiting, married or cohabiting), service branch (Air Force, Army, Coast Guard, Marine Corps, Navy), and pay grade (officer, enlisted). Pay grade, or rank, is often used in research of military personnel as a proxy for socioeconomic status, as it organizes service members by socioeconomic rewards and job characteristics, with enlisted personnel generally having lower socioeconomic status compared with officers. 24 Race/ethnicity was condensed from four racial and ethnic categories (White, non-Hispanic Black, Hispanic, and other) into a binary variable to ensure respondent anonymity.
Statistical analyses
All statistical analyses were performed using SAS 9.4 software (SAS Institute Inc., Cary, NC). To account for the complex sampling design and ensure that estimates are representative of U.S. ADSW, survey weights were applied to all analyses. Baseline characteristics were summarized using weighted frequencies and percentages for categorical variables (Table 2). Bivariate associations between each characteristic and unwanted pregnancy were assessed using weighted chi-square tests (Table 3). We employed a binary logistic regression model to examine the binary outcome, undesired pregnancy (yes/no). Unadjusted weighted estimates were calculated for each demographic characteristic and exposure variable to assess their individual associations with unwanted pregnancy. Subsequently, multivariable weighted binary logistic regression models were performed to assess the association of WHCs with unwanted pregnancy, controlling for demographic characteristics. Odds ratios (ORs) and adjusted odds ratios (aORs), along with their 95% confidence intervals (CIs), were used to assess the strength of the association. ORs indicate the odds of an outcome (i.e., unwanted pregnancy) in one group (i.e., those at a duty station with a WHC) divided by the odds of that outcome in another group (i.e., those at a duty station without a WHC). Table 4 presents both the unadjusted and adjusted regression models. For sensitivity analyses (Table 5), we excluded 130 respondents who reported “not sure if wanted a/another baby at any time in the future” to assess the robustness of our results. Statistical significance was defined as a two-sided p-value <0.05.
Definition of Unwanted Pregnancy: Yes/No
Weighted Prevalence of Characteristics in the Analytic Sample (n = 2,939)

LCL, lower confidence limit; UCL, upper confidence limit; WHC, women’s health clinic.
Sample Characteristics of Those with and without a WHC on Installation (n = 2,939)
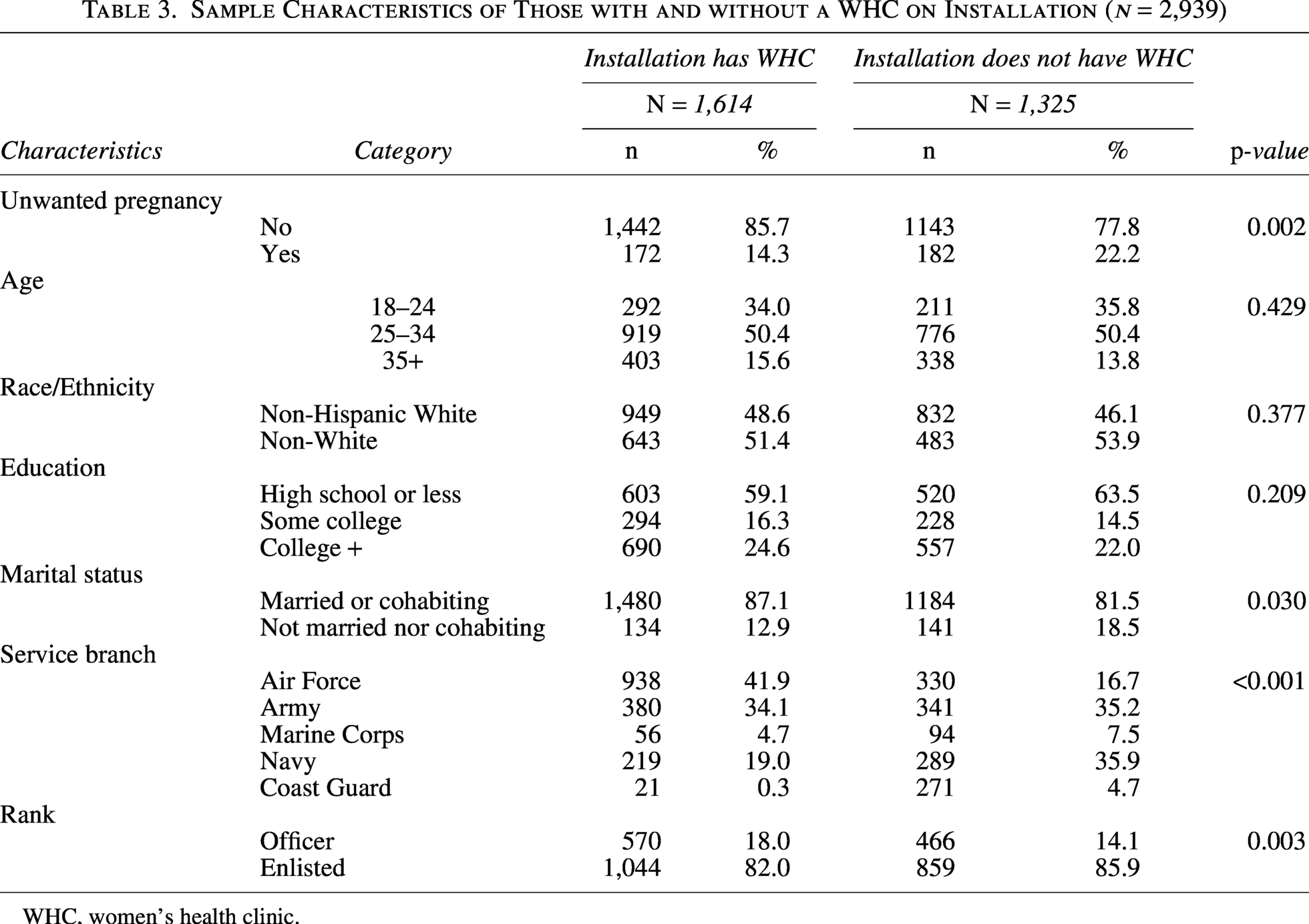
WHC, women’s health clinic.
Unadjusted and Adjusted Odds Ratios of Unwanted Pregnancy (n = 2,939)
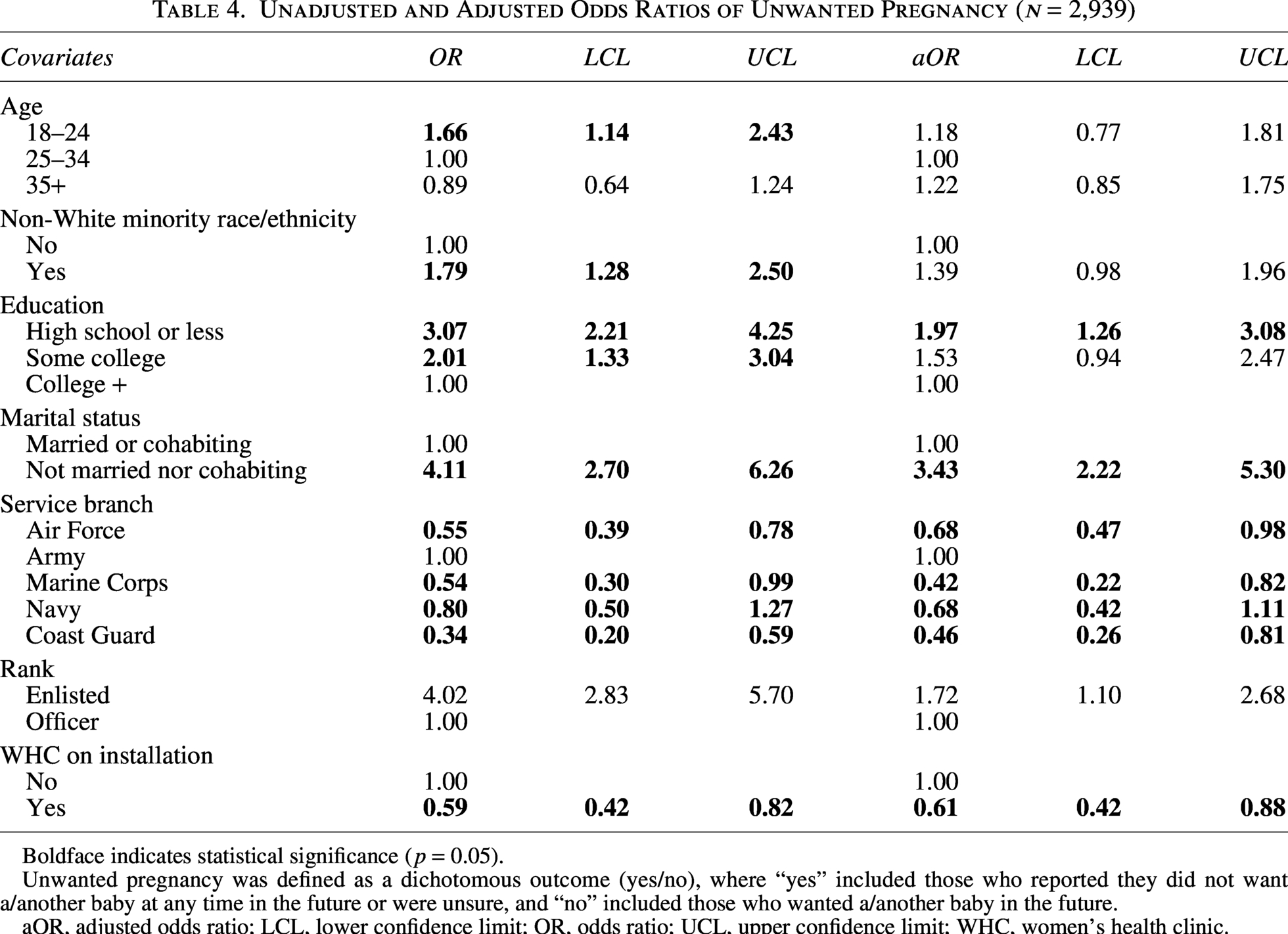
Boldface indicates statistical significance (p = 0.05).
Unwanted pregnancy was defined as a dichotomous outcome (yes/no), where “yes” included those who reported they did not want a/another baby at any time in the future or were unsure, and “no” included those who wanted a/another baby in the future.
aOR, adjusted odds ratio; LCL, lower confidence limit; OR, odds ratio; UCL, upper confidence limit; WHC, women’s health clinic.
Unadjusted and Adjusted Odds Ratios of Unwanted Pregnancy (n = 2,809)
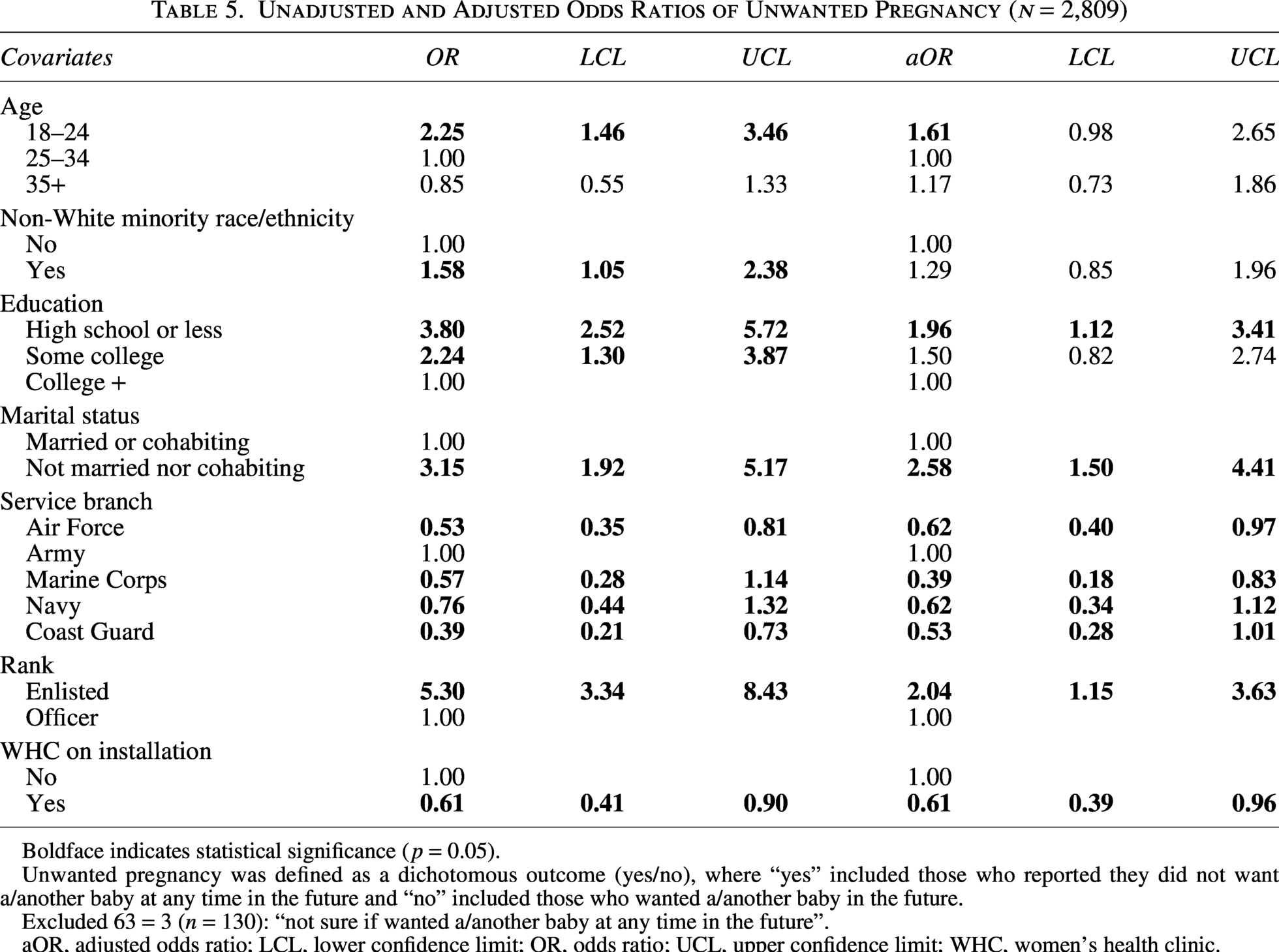
Boldface indicates statistical significance (p = 0.05).
Unwanted pregnancy was defined as a dichotomous outcome (yes/no), where “yes” included those who reported they did not want a/another baby at any time in the future and “no” included those who wanted a/another baby in the future.
Excluded 63 = 3 (n = 130): “not sure if wanted a/another baby at any time in the future”.
aOR, adjusted odds ratio; LCL, lower confidence limit; OR, odds ratio; UCL, upper confidence limit; WHC, women’s health clinic.
Results
Of the 2,939 ADSW included in the analytic sample, the weighted prevalence of unwanted pregnancy was 17.9% (n = 354) (95% CI: 15.5–20.4%) with 144 (40.7%) live births and 67 (15.0%) miscarriages resulted from the unwanted pregnancies. Table 2 presents the weighted demographic characteristics of study respondents. However, when we excluded 130 respondents who reported “not sure if wanted a/another baby at any time in the future,” the weighted prevalence was lower (12.7%; 95% CI: 10.5–14.9%). When we included ADSW, who did not know if their installation had a WHC, the prevalence of unwanted pregnancy showed an increasing trend across groups: 14.3% in ADSW with a WHC, 17.6% in ADSW who did not know if their installation had a WHC, and 22.2% in ADSW without a WHC (p-value = 0.0092). The prevalence remains highest in the group without a WHC.
Table 4 presents the results of the weighted unadjusted binary logistic regression model. In this model, having a WHC at an ADSW’s current installation was significantly associated with a 41% decrease in the odds of unwanted pregnancy (OR = 0.59; 95% CI: 0.42–0.82). Significant increases in odds of unwanted pregnancy were associated with those who were aged 18–24 (OR = 1.66; 95% CI: 1.14–2.43), non-White (OR = 1.79; 95% CI: 1.28–2.50), had an education level of some college (OR = 2.01; 95% CI: 1.33–3.04) or high school or less (OR = 3.07; 95% CI: 2.21–4.25), not married or cohabiting (OR = 4.11; 95% CI: 2.70–6.26), and enlisted rank (OR = 4.02; 95% CI: 2.83–5.70). Significant decreases in unwanted pregnancy were associated with those who were in the Air Force (OR = 0.55; 95% CI: 0.39–0.78), Marine Corps (OR = 0.54; 95% CI: 0.30–0.99), or Coast Guard (OR = 0.34; 95% CI: 0.20–0.59) compared with those in the Army.
In the adjusted binary logistic regression model, the decrease in odds of unwanted pregnancy associated with having a WHC at their current installation/duty station persisted (aOR = 0.61; 95% CI: 0.42–0.88). Table 4 also presents the results of the weighted adjusted binary logistic regression model. Significant increases in odds of unwanted pregnancy remained associated with those who had an education of high school or less (aOR = 1.97; 95% CI: 1.26–3.08), those who were not married nor cohabiting (aOR = 3.43; 95% CI: 2.22–5.30), and those who were enlisted rank (aOR = 1.72; 95% CI: 1.10–2.68). Significant decreases in odds of unwanted pregnancy remained associated with those in the Air Force (aOR = 0.68; 95% CI: 0.47–0.98), Marine Corps (aOR = 0.42; 95% CI: 0.22–0.82), and Coast Guard (aOR = 0.46; 95% CI: 0.26–0.81).
Our findings were robust when we excluded 130 respondents who reported “not sure if wanted a/another baby at any time in the future.” The association remains significant, having a WHC at an ADSW’s current installation was significantly associated with a 39% decrease in odds of unwanted pregnancy (aOR = 0.61; 95% CI: 0.39–0.96).
Discussion
This study explored the association between WHCs and unwanted pregnancy among ADSW. Our analysis indicated that the presence of a WHC was associated with a 39% decrease in odds of unwanted or mistimed pregnancy, which suggests WHCs may promote reproductive autonomy among ADSW and contribute to the prevention of unwanted or mistimed pregnancy. The decision to have a child is deeply personal and implies lifetime consequences that reach far beyond a single pregnant individual. A pregnancy that is both unwanted and mistimed has a biopsychosocial impact that can affect generations.2,3 For ADSW, unwanted or mistimed pregnancies result in additional significant challenges for individual and unit readiness, as pregnant individuals are entitled to light duty, which limits the kinds of tasks that they can perform while pregnant and are ineligible for deployment and, if already deployed, may require medical evacuation. WHCs can offer resources, education, and support to help women make informed reproductive choices, thereby potentially reducing the occurrence of unwanted or mistimed pregnancies. 25
Of the 2,939 ADSW included in the analytic sample, the weighted prevalence of unwanted pregnancy was 17.9% (95% CI: 15.5–20.4%). Much of the literature focuses on unintended pregnancies, which encompasses both unwanted and mistimed pregnancies, rather than solely on unwanted pregnancies. Despite this, we identified one study of U.S. pregnancies in 2009–2015 found that 18.0% (95% CI: 16.1–20.4%) of pregnancies in 2009 and 17.1% (95% CI: 15.4–19.0%) of pregnancies in 2015 were unwanted, which aligns with our findings. 26 However, when we excluded 130 respondents who reported “not sure if wanted a/another baby at any time in the future,” the prevalence in our findings was lower (12.7%; 95% CI: 10.5–14.9%).
Having a WHC at an ADSW’s current installation was significantly associated with decreased odds of unwanted pregnancy. This indicates that WHCs could serve as a potential protective factor in preventing unwanted pregnancies; however, as this is a cross-sectional study and cannot assess causality, additional research is needed into this association. In 2016, a pilot walk-in, full-service contraceptive clinic within a Military Treatment Facility (MTF) was launched with the aim of improving access to contraceptives and reducing unwanted or mistimed pregnancy within the MHS.16,21,27 The success of this clinic led to the expansion of the walk-in contraception services model within the MHS.25,28 Though not all WHCs within the MHS provide walk-in contraception services, these findings indicate that increased access to contraceptives is associated with decreased odds of unwanted pregnancy. 21 The U.S. Department of Veterans Affairs (VA) successfully implemented a WHC model decades prior to the MHS and found substantial increases in patient satisfaction. 23 Evaluating patient satisfaction at MHS WHCs would help to understand if ADSW perceive the same improvements in care quality observed within the VA WHCs. Additionally, there is evidence that patients seen at WHCs were more likely to have gender-specific screenings, such as breast examinations and pap smears, which should be explored in MHS WHCs. 23 However, the literature on WHCs is largely outdated and more research focused on their benefits, such as improved care quality and expanded reproductive services, should be conducted both within the MHS and in other care settings. 23
We also found significant associations with unwanted pregnancy among enlisted service members. This is consistent with the literature, which suggests that the lowest rates of contraceptive use and highest rates of unintended pregnancy are among those of enlisted rank. 29 This indicates that interventions to reduce barriers to contraceptive care and promote family planning should be targeted at enlisted service members. Additionally, we found that ADSW in the Air Force, Marine Corps, and Coast Guard were significantly associated with reductions in unwanted pregnancy when compared with ADSW in the Army. While previous literature has found that the Air Force and Coast Guard had lower odds of unintended pregnancy, the Marine Corps was found to have higher odds, in contrast to our findings. 30 Additional research is needed to understand if there are any service branch-specific barriers to contraceptives that may lead to the increased odds of unintended or unwanted pregnancy.
Women who do not desire pregnancy may seek pregnancy termination services. However, the ability to obtain these services is dependent on several factors, including individual and personal factors, access and availability, and interpersonal factors. 31 Cultural factors within the U.S. also influence pregnancy termination decision making; women in the United States are less likely to terminate an unwanted pregnancy compared with women in other industrialized countries. 27 Within the military, ADSW experience additional barriers. Abortion is only available at MTFs in cases of rape, incest, or to save the life of the pregnant woman, though ADSW may seek care outside of the MHS out-of-pocket.32,33 However, this has become more challenging in light of state-level bans on abortion services following the Supreme Court decision Dobbs versus Jackson Women’s Health Organization and reversal of a policy that had allowed ADSW to be reimbursed for travel expenses incurred to receive abortion services out-of-state.34,35 This policy reversal was part of a larger effort to eliminate programs and policies aimed at fostering diversity, equity, and inclusion within the Department of War, which may further impact women’s health care delivery within the MHS. 36 Findings from the literature suggest that policies impacting reproductive autonomy are associated with reductions in effective contraception use. 19 Because of these policy and cultural barriers to reproductive autonomy, unwanted pregnancies are more likely to result in delivery. 27
In a 2023 study examining rates of unintended pregnancy among service women and the factors that influence unintended pregnancy, Defense Health Horizons made four recommendations to improve the health and readiness of military women; these included the development of reliable data sources, access to their desired contraceptive options, identification and removal of existing barriers to contraceptive care, and establishment of service delivery targets for women’s preventive health services. 29 Based on our findings, we recommend expansion of WHCs within the MHS, which may help to address these recommendations by providing access to comprehensive contraceptive care to reduce unwanted or mistimed pregnancies.
Limitations
This study has some limitations. First, all data used in this study are both cross-sectional, limiting the ability to make causal inferences, and self-reported and therefore subject to recall bias and social desirability bias. Women might also not feel comfortable using the terms such as “unwanted” to describe their pregnancy. 37 Additionally, data regarding the timing within the pregnancy or post-partum period participants completed the survey was not collected, only that they had been pregnant at some point within the previous 12 months from when they completed the survey. This is a significant limitation, as the literature indicates that retrospective reports of pregnancy intention are likely to underestimate the frequency of unwanted pregnancy, and that retrospective intention can be impacted by pregnancy outcome. Presence of a WHC was also self-reported and unable to be confirmed as no location data was collected. In addition, ADSW may be relocated at some point during their pregnancy, thus their current installation may not be the installation that they were stationed at prior to becoming pregnant, which could lead to misclassification of our primary exposure. Additionally, the methods used in the survey to estimate unwanted pregnancies are not identical to the methods used in national estimates, which combine survey data with national birth records and surveys of providers and patients who administer or receive abortion services. National estimates also do not include an “unsure” response. 21 These differences may have contributed to the lower estimates of unwanted pregnancies in our analytic sample. 21 The weighted response rate for this survey was 17.8%, which is relatively low and may suggest selection bias; however, survey weights were used to minimize any selection bias and increase the representativeness of the analytic sample. 21 Another limitation of this study was the broad categories used for race, not allowing for analysis of all racial subcategories.
Conclusion
This study assessed the impact of the availability of WHCs at an ADSW’s current installation on unwanted pregnancy among ADSW to reduce the high rate of unwanted pregnancy. Having a WHC at an ADSW’s current installation was associated with lower odds of unwanted pregnancy by 39%, after adjusting for sociodemographic factors. Unwanted pregnancy can have long-lasting negative effects on both ADSW and their career, as well as mission readiness. Access to specialty care at duty stations may promote reproductive autonomy among ADSW and may play a role in preventing unwanted pregnancies and positively impacting force health protection and military readiness.
Authors’ Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, acquisition of data, execution, analysis and interpretation, took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Ethics Approval and Consent to Participate
All experimental protocols related to this study were approved by the Uniformed Services University of the Health Sciences Institutional Review Board. All methods were carried out in accordance with the relevant guidelines and regulations. Informed consent was waived for this study by the Uniformed Services University of the Health Sciences Institutional Review Board.
Availability of Data and Materials
The data that support the findings of this study are available from RAND and DoD but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Patient Consent Statement
Informed consent was waived for this study by the Uniformed Services University of the Health Sciences Institutional Review Board.
Disclaimer
The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views, opinions, or policies of Uniformed Services University of the Health Sciences (USU), the Department of Defense, the
Footnotes
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
This work was conducted with the Center for Health Services Research and funded by the Department of Defense, Defense Health Agency, grant no. HU00012520012. The funding agency played no role in the design, analysis, or interpretation of findings.