
Abstract
Although evidence exists that bully victimizations are related to a range of negative outcomes later in the life course, existing research has largely ignored the timing of the victimization experience. Using data from the National Longitudinal Survey of Youth 1997, the present study uses propensity score matching to investigate the adult consequences of victims experiencing repeated bullying in childhood, adolescence, or both developmental periods. Individuals victimized as children reported higher instances of arrests, convictions, violence, and substance use than child nonvictims. The results point to the importance of implementing effective prevention programs early in the life course.
Bullying remains a significant public concern among school-aged youth. Identified as repetitive abusive behaviors with specific intent to harm the victim and accompanied by an imbalance of power between the offender and the victim (Olweus, 1993), prevalence rates of bully victimization remain high and significantly vary across age (Juvonen, Graham, & Schuster, 2003; Nansel et al., 2001). As evidence, research has documented that bullying is most prevalent in younger school-aged children where data indicate that approximately 20% of students in elementary schools report being victimized by a bully (Dake, Price, & Telljohann, 2003; Kochenderfer & Ladd, 1996; Ma, Stewin, & Mah, 2001). Prevalence rates of bullying tend to decrease as students age into middle and high school, where national data have revealed that 8.5% of students were bullied “sometimes,” and 8.4% of students were bullied once a week or more (Nansel et al., 2001). A recent meta-analysis conducted by Modecki, Minchin, Harbaugh, Guerra, and Runions (2014) estimates victimization prevalence rates at 15.2% for cyberbullying and 36% for traditional bullying for adolescents (i.e., 12- to 18-year-olds).
The growth in public interest surrounding bullying has ushered in an area of research focused on the effects that victims of bullying experience later in the life course. Research has documented a variety of adverse consequences related to individuals experiencing bully victimization. Victims of bullies have reported experiencing maladjustment problems such as fighting and other violent behaviors, substance use, poor relationships with peers, increased loneliness, low self-esteem or self-concept, and lacking the ability to make friends (Juvonen et al., 2003; Kochenderfer & Ladd, 1996; Ma et al., 2001; Nansel et al., 2001; Valdebenito, Ttofi, & Eisner, 2015). Compared to nonvictims, victims were also more likely to report higher levels of anxiety, report a significantly greater number of physical health symptoms, engage in avoidance behaviors, suffer more significant depressive symptoms, and report severe suicidal ideations (Dake et al., 2003; Juvonen et al., 2003; Kochenderfer & Ladd, 1996; Lereya, Copeland, Costello, & Wolke, 2015; Ma et al., 2001; Nansel et al., 2001; Sigurdson, Undheim, Wallander, Lydersen, & Sund, 2015; Takizawa, Maughan, & Arseneault, 2014; Turner, Exum, Brame, & Holt, 2013).
Although important contributions to the knowledge base have been made regarding the consequences of bullying, significant gaps in the research have yet to be addressed. One question that research has yet to explore is whether the timing of the victimization experience (i.e., childhood vs. adolescence) has similar (or different) consequences of individuals once they reach adulthood. That is, are children who experience bully victimization more vulnerable to its effects and therefore experience greater levels of adverse consequences in adulthood compared to adolescents who experience bully victimization? Based on the tenets of life-course theory, it is expected that the timing of bullying victimization will play a role in its consequences. According to this perspective, events that occur during a person’s life have the capacity to influence the life trajectory (Elder, 1994)—these key turning points may be potent enough to shape a person’s life long term. Bullying victimization occurring during early childhood may be more impactful, given that this developmental time period is when children are developing key characteristics that will shape their future interactions (Clausen, 1991).
As such, understanding whether the consequences of bullying victimization are different for children and adolescents is important because if differences do occur, effective interventions focusing on the physical, emotional, and psychological trauma associated with the experience can be more efficiently targeted toward a particular age-group. Better understanding of the long-term consequences of bullying can also aid in deciding when and how to intervene in response to bullying victimization. The purpose of the present study is to fill this void in the literature and investigate whether adult consequences of bully victimization differ depending on whether the individual was victimized as a child or as an adolescent. To contextualize these questions, the literature investigating the effects of bully victimization is reviewed below.
Bully Victimization Over the Life Course
As identified above, prevalence rates of bully victimization vary over the life course. On the individual level, it follows that there exists variability in one’s probability of experiencing a bully victimization. Some individuals might be victimized in childhood, some individuals might be victimized in adolescence, and some may be victimized over both developmental periods. Since victimization may occur at different points during the life course, it is important to acknowledge that the consequences of victimization may vary depending on the age at which individuals are victimized.
The life-course perspective is rooted in the notion that events that occur during key developmental time points in the life course are capable of changing the trajectory of a person’s life (Elder, 1994). Experiences such as bullying may be salient enough to carry significant consequences and influence a person’s life-course trajectory. When during the life course the bullying occurs will likely determine the influence on the trajectory, given that experiencing this type of victimization during certain developmental time periods is likely to be more harmful than others. Childhood and adolescence are the developmental periods in which individuals develop personal and psychological resources that enable them to problem solve and make good decisions (Clausen, 1991). When considering the nature of victimization and what it does to a person, it is likely that after being bullied, a person has their perceptions of agency and self-efficacy affected (Macmillan, 2001). Further, beliefs and perceptions about others are also influenced as individuals are seen as sources of harm (Macmillan, 2001). When bullying happens earlier in the life course (i.e., childhood rather than adolescence), these perceptions and beliefs may be altered in ways that create other, and perhaps different, long-term negative consequences. If children or adolescents do not believe that they can trust others to provide support and care, that they are able to protect themselves, or that their future can be different than their past, their life-course trajectory may appear quite different from others (Macmillan, 2001).
Another consideration in how bullying behavior may shape a person’s trajectory is the type of bullying that a person experiences. Differential victimization experiences are likely to produce different (or more pronounced) consequences across the life course. Although relatively unexplored in the bullying literature, a few studies have examined the effects of different forms of bullying on a single outcome—depression (Turner et al., 2013; van der Wal, de Wit, & Hirasing, 2003). Turner, Exum, Brame, and Holt (2013) found that levels of depression varied across the type of bully victimization, and gender differences emerged among victims of cyberbullying where females were more adversely affected than males. Similarly, van der Wal, de Wit, and Hirasing (2003) found that levels of depression were higher for indirect rather than for direct forms of bullying, suggesting that indirect and covert forms of bullying, such as social isolation, may cause more psychological harm to the victim than direct, physical forms of bullying. It is possible, then, that bullying at different time periods may carry different consequences insomuch as the type of bullying experienced may be different across time (Craig et al., 2009).
Consequences of Bully Victimization
In addition to recognizing that the consequences of bullying may vary depending on the developmental time period in which it occurs, the different types of consequences that may occur for children and adolescent victims are also important to examine. The existing literature has determined that depression and suicidality (Copeland, Wolke, Angold, & Costello, 2013; Lereya et al., 2015; Lund et al., 2008; Sigurdson et al., 2015; Silberg et al., 2016; Takizawa et al., 2014), antisocial behaviors (Luk, Wang, & Simons-Morton, 2010; Mitchell, Ybarra, & Finkelhor, 2007; Sullivan, Farrell, & Kliewer, 2006; Valdebenito et al., 2015), academic competence (Cornell, Gregory, Huang, & Fan, 2013; Glew, Fan, Katon, Rivara, & Kernic, 2005; Juvonen, Wang, & Espinoza, 2011), and psychosomatic symptoms (Fekkes, Pijpers, & Verloove-Vanhorick, 2004; Natvig, Albrektsen, & Qvarnstrøm, 2001) are consequences of bully victimization. Each of these factors is discussed below.
Depression and Suicidality
Children who are victims of bullying experience more depressive symptoms and are at higher risk of suicide than children who are not bullied (Copeland et al., 2013; Klomek, Marrocco, Kleinman, Schonfeld, & Gould, 2007; Lund et al., 2008). Using a sample of 9th- through 12th-grade students in New York, Klomek, Marrocco, Kleinman, Schonfeld, and Gould (2007) found that students who were frequent victims of bullying were 7 times more likely to be depressed compared to students who had never been victimized, and students who were infrequently bullied were still approximately 2–3 times more likely to be depressed. Being a victim of bullying does not only lead to childhood depression, rather the elevated risk of suffering from depression extends into early adulthood and later in life as well (Copeland et al., 2013; Lereya et al., 2015; Lund et al., 2008; Takizawa et al., 2014). High intensity or high duration of bullying results in a significant increase in the odds of having, or having had, depression during the ages of 31–51 years (Lund et al., 2008).
Antisocial behaviors
Childhood bullying can have long-term repercussions on behavior, including violence (Liang, Flisher, & Lombard, 2007; Sullivan et al., 2006), substance use (Luk et al., 2010; Mitchell et al., 2007; Sullivan et al., 2006; Valdebenito et al., 2015), and delinquency (Mitchell et al., 2007; Sullivan et al., 2006). Although the current literature shows that bully victims (those who have bullied and who have experienced bullying) have a higher likelihood of engaging in these behaviors (Kim, Catalano, Haggerty, & Abbott, 2011; Liang et al., 2007), victims of bullying remain at risk (Liang et al., 2007; Luk et al., 2010; Mitchell et al., 2007; Sullivan et al., 2006).
Compared to nonvictims, victims of bullying have been found to be more likely to be involved in violence, such as fighting (Liang et al., 2007). Youth who were victimized reported engaging in criminal offenses such as theft, vandalism, traffic violations, and other property crimes (Liang et al., 2007; Sourander et al., 2007). Involvement in illicit behavior has been shown to extend into early adulthood (Sourander et al., 2007). Bully victimization is also positively associated with substance use (Luk et al., 2010; Mitchell et al., 2007) including alcohol, cigarettes, marijuana, and inhalants (Tharp-Taylor, Haviland, & D’Amico, 2009). In one study that examined delinquency, violence, and other antisocial behaviors into adulthood, bullying was not found to be related to these outcomes (Bender & Losel, 2011). These relationships, however, were only examined at age 25 among a small sample of males.
Academic competence
Current research documents that there is a significant association between bully victimization and academic competence (Cornell et al., 2013; Glew et al., 2005; Juvonen et al., 2011; Ma, Phelps, Lerner, & Lerner, 2009; Schwartz, Gorman, Nakamoto, & Toblin, 2005). A victim’s academic achievement can be mediated by a variety of factors: depressive symptoms, difficulties with attention regulation and concentration, experiencing extreme stress in the school environment, and avoidance behaviors, such as skipping school to avoid being bullied (Ma et al., 2009). The association between bully victimization and poor academic functioning, as measured by grade point averages and achievement test scores, has been demonstrated in samples of elementary school children as well as the sixth graders (Glew et al., 2005; Juvoven et al., 2011; Schwartz et al., 2005). Furthermore, prevalence rates of bullying as perceived by the ninth graders and their teachers were found to be predictive of high school dropout rates for the same cohort of students (Cornell et al., 2013).
Psychosomatic symptoms
In addition to harm academically, bully victimization may be associated with negative health outcomes. Psychosomatic symptoms refer to physical health complaints including, but not limited to, headaches, abdominal pain, sleeping problems, dizziness, fatigue, bed-wetting, and loss of appetite (Fekkes et al., 2004; Gini, 2008; Natvig et al., 2001). These physical ailments are thought to arise due to the stress experienced by victims of bullying (Fekkes et al., 2004; Natvig et al., 2001). Studies have found that elementary-aged children who were bullied had a higher risk of experiencing a variety of psychosomatic complaints such as headaches, abdominal pain, sleeping problems, poor appetite, bed-wetting, dizziness, and feeling tense compared to children who were uninvolved in bullying behaviors (Fekkes et al., 2004; Gini, 2008). Additionally, Natvig, Albrektsen, and Qvarnstrøm (2001) explored this relationship using a sample of adolescents between the ages of 13 and 15. They found that compared to students who reported that they were never bullied, students who reported being bullied had significantly higher odds of experiencing every psychosomatic symptom measured (physical complaints included headache, stomachache, backache, and dizziness, while psychological complaints included feeling low, irritability, nervousness, and difficulty getting to sleep), except sleeplessness. Some studies have examined the link between childhood bullying and adult health. The existing evidence suggests that individuals who were bullied in childhood suffered from worse physical health or poorer perceived quality of life in adulthood than those who had not experienced childhood bullying (Allison, Roeger, & Reinfeld-Kirkman, 2009; Takizawa et al., 2014). Whether adolescent bullying victims also experience poor health outcomes into adulthood and whether these outcomes are the same as childhood bullying victims have yet to be investigated.
Current Focus
Despite the existing scholarly contributions, little, if any, research has focused on thoroughly understanding the similarities and differences in bully victimization that occur during different developmental periods. Although current research explores the causes and consequences of bully victimization in childhood and in adolescence separately, the research is relatively silent when it comes to systematic comparison of the effects of victimization experienced across these two developmental periods. We fill this void in the literature using data from the National Longitudinal Study of Youth 1997 (NLSY97) cohort. Specifically, we address three research questions: First, to what extent, do individuals experience bullying victimization as children only, as adolescents only, or during both childhood and adolescence? Second, do victim groups (childhood, adolescent, chronic) differ in characteristics such that the factors that correlate with membership in them vary? Third, are the consequences of victimization (measured in adulthood) similar or different for individuals victimized in childhood, in adolescence, and those who were chronically bullied during both developmental periods?
Method
Data
The data used for this study are extracted from the NLSY97. The NLSY97 is part of a series of surveys funded by the U.S. Department of Labor and the Bureau of Labor Statistics to investigate how youths transition into the labor force. The NLSY97 is comprised of a nationally representative sample of 8,984 individuals born between the years 1980 and 1984. More specifically, the NLSY97 cohort is comprised of two independent probability subsamples: (1) a cross-sectional sample of 6,748 individuals and (2) a supplemental sample of 2,236 individuals designed to oversample for African Americans and Hispanics.
The NLSY97 cohort was selected in two separate phases (Moore, Pedlow, Krishnamurty, & Wolter, 2000). In the first phase, 96,512 households were identified as eligible housing units from 147 nonoverlapping primary sampling units chosen from the National Opinion Research Center’s 1990 master probability sample of the United States. The second phase identified individuals within the 96,512 households who were eligible for inclusion in the NLSY97 cohort. Individuals who were NLSY97 eligible were, at the time of the first interview, between the ages of 12 and 16 as of December 31, 1996. A total of 9,907 individuals were selected for interview during the household screening phase, and a total of 8,984 (90.7%) individuals were ultimately interviewed in Wave 1. Participants were between the ages of 27 and 29 during the most recent wave (i.e., Wave 15) of data used in the analysis.
Sample
The current study utilizes the cross-sectional sample of 6,748 individuals. The supplemental sample is excluded from analysis to make the results of this study generalizable to the larger U.S. population, while avoiding the complexities related to sample weighting (see Brame, Bushway, Paternoster, & Turner, 2014; Brame, Turner, Paternoster, & Bushway, 2012). In the cross-sectional sample, there were 3,459 (51%) males and 3,289 (49%) females in the initial interview, with the following racial and ethnic breakdown: non-Black/non-Hispanic: 4,665 (69.1%), Black non-Hispanic: 1,081 (16%), Hispanic or Latino: 921 (13.6%), and mixed race/ethnicity: 81 (1.2%).
Due to age-specific covariates, the NLSY97 excluded a number of participants by only applying specific variables to certain ages. To maximize the number of valid cases, the sample was restricted to participants between the ages of 12 and 14 at Wave 1. These restrictions resulted in a final sample of 3,655 participants.
Measures
Bully victimization
Our first objective is to identify whether individuals experienced bully victimization during childhood, adolescence, or both developmental periods. To accomplish this task, we relied on two sets of survey questions. At Wave 1 in 1997, when individuals were between the ages of 12 and 14, each subject was asked, “Before you turned age 12, were you ever the victim of repeated bullying?” Response options were no (= 0) and yes (= 1). When subjects reached the age of 18, they were asked, “Between the ages of 12 and 18, were you ever the victim of repeated bullying?” This survey item was administered from Wave 3 to Wave 7 (1999–2003), but each participant was only asked this question one time upon reaching the age of 18. Response options were no (= 0) and yes (= 1). Respondents who answered “yes” to the first question only were coded as child victims. Respondents who answered yes to the second question only were coded as adolescent victims. Respondents reporting they were victimized in childhood and adolescence were coded as chronic victims. Finally, respondents who indicated that they were victimized neither in childhood nor in adolescence were coded as nonvictims.
Depression
Beginning in Wave 8 when individuals were between the ages of 20 and 22 and continuing until Wave 14 when individuals were between the ages of 26 and 28, the NLSY97 included a question to measure depression: “How much of the time during the last month have you felt so down in the dumps that nothing could cheer you up?” Respondents were able to answer with one of the following: all of the time (= 3), most of the time (= 2), some of the time (= 1), and none of the time (= 0). Our final measure of depression was created by summing the valid depression scores and dividing this value by the total number of valid waves.
Antisocial behaviors
The NLSY97 captured violent tendencies in participants through the following question administered during Waves 7–15 (2003–2011): “Since the last interview on [date of last interview], have you attacked someone with the idea of seriously hurting them or have had a situation end up in a serious fight or assault of some kind?” The response options were yes (= 1) or no (= 0). A violence measure was created by counting the waves that the participant answered yes. A higher score indicated more frequent annual involvement in violence. Only measures of violence after the age of 18 were included as outcomes in the analysis.
Substance use was measured by two survey questions that were administered from Waves 7 to 15. The first question asked respondents, “Since the date of last interview, have you used marijuana, even if only once, for example, grass or pot?,” and the second question was “Excluding marijuana and alcohol, since the date of last interview, have you used any drugs like cocaine, crack, heroin, or crystal meth, or any other substance not prescribed by a doctor, in order to get high or to achieve an altered state?” The response options for these 2 items were yes (= 1) or no (= 0). A substance use measure was created by summing the yes responses. A higher score indicated more frequent annual involvement in substance use. Only measures of substance use after the age of 18 were included as outcomes in the analysis.
Formal involvement in the criminal justice system was measured using 2 separate self-report items. The first item measuring arrest included the following: “Since the date of last interview on [date of last interview], have you been arrested by the police or taken into custody for an illegal or delinquent offense (do not include arrests for minor traffic violations)?” This question was administered during Waves 7 through 15, and response options were yes (= 1) or no (= 0). The arrest measure was created by summing the waves that the participant answered yes. Higher scores indicated more frequent involvement in the criminal justice system. The second item measuring conviction, also administered during Waves 7 through 15, included the following: “Since the date of last interview on [date of last interview], were you convicted of, or found delinquent (adjudicated delinquent) of any charges, or did you plead guilty to any charges?” Again, response options were yes (= 1) and no (= 0). A measure of self-reported convictions was created by summing the number of times a participant answered yes. Higher scores indicated more frequent involvement in the criminal justice system. Only measures of arrests and convictions after the age of 18 were included as outcomes in the analysis.
Academic competence
Academic competence was measured by a single question during the final wave: “What is the highest educational degree you have ever received?” Respondents were given the following response options: none, General Education Development (GED), high school diploma (regular 12-year program), associate/junior college (associates of arts), bachelor’s degree (bachelor of arts, bachelor of science), master’s degree (master of arts, master of science), doctor of philosophy, and professional degree (doctor of dental surgery, juris doctor, medical doctor). Individuals who did not receive any type of degree or obtained a GED were coded as not academically competent (= 1) and those who earned a high school diploma or higher were coded as academically competent (= 0).
Psychosomatic symptoms
The NLSY97 includes psychosomatic consequences related to sleep. In Waves 11 through 15 (2007–2011), participants were asked: “On a typical week night, how many hours of sleep do you usually get?” Answers ranged from 0 to 10+ hours. Research has documented the desired average sleep quota for an adult is 7.5 hours of sleep per night (Ferrara & De Gennaro, 2001). Therefore, responses were coded where participants with 0–7 hours of sleep had sleep difficulties (= 1) and those with 8–10+ hours of sleep did not have sleep difficulties (= 0). This procedure was repeated for all five waves of data. An aggregate sleep difficulty score was created by summing the valid sleep difficulty scores from Waves 11 through 15 and dividing this value by the total number of valid waves. Only measures of sleep deprivation after the age of 18 were included as outcomes in the analysis.
Control Variables
As discussed in more detail below, we use a propensity score matching (PSM) design to address our research questions. Therefore, we match participants as closely as possible on several variables, so that we can achieve balance among respondents receiving the treatment (bullying victims) and those not receiving the treatment (nonvictims). Specifically, individuals were matched on the following variables: age, race, sex, socioeconomic status (SES), parental monitoring, parenting style, family/home risk, exceptionalities, body mass index (BMI), height, school type, urbanity, and delinquency score. Age is a continuous variable measured in years. Measures for sex (male = 0 and female = 1) and race (White = 0 and non-White = 1) are also included. The SES variable was created by standardizing and then summing the following 3 items: (1) gross household income in 1997, (2) highest grade completed by biological father, and (3) highest grade completed by biological mother (Cronbach’s α = .56). Scores above 0 indicate the SES were higher than the sample mean (Powell, Wada, Krauss, & Wang, 2012).
Parental monitoring contained four questions answered by the residential mother that were measured on a 5-point scale. Youths were asked, (1) “How much does she know about your close friends, that is, who they are?” (2) “How much does he or she know about your close friends’ parents, that is, who they are?” (3) “How much does he or she know about who you are with when you are not at home?” and (4) “How much does she know about who your teachers are and what you are doing in school?” Response options included knows nothing (= 0), knows just a little (= 1), knows some things (= 2), knows most things (= 3), and knows everything (= 4). The parental monitoring index was scored by summing all of the questions and ranged from 0 to 16, where higher scores indicated a greater degree of parental monitoring (Cronbach’s α = .71).
Parenting style was measured in Wave 1 by the residential mother who was presented with the following two questions: (1) “When you think about how she acts toward you, in general, would you say that she is very supportive, somewhat supportive, or not very supportive?” and (2) “In general, would you say that she is permissive or strict about making sure you did what you were supposed to do?” The supportive responses were measured on a 3-point scale (very supportive = 1, somewhat supportive = 2, not very supportive = 3), and the strictness responses were measured on a 2-point scale (permissive = 1, strict = 2). These two variables were then combined to produce a parenting style variable with four categories: (1) uninvolved (permissive and not very or somewhat supportive), (2) authoritarian (strict and not very or somewhat supportive), (3) permissive (permissive and very supportive), and (4) authoritative (strict and very supportive), which served as the reference category.
Family home/risk was measured in Wave 1 by the family/home risk index. The family/home risk index is a 30-item measure that addressed potential areas of risk including home physical environment, neighborhood, enriching activities, religious behavior, school involvement, family routines, parent characteristics, and parenting. Each item (or set of items) was coded into risk categories (risk = 1 and no risk = 0). These items were then summed and resulted in a composite score on the family/home risk index, where higher scores indicated more risk in the family and home environment.
Exceptionalities were measured via questions capturing the existence of the following conditions: (1) learning disability (i.e., dyslexia) or attention disorder and (2) mental retardation. Our exceptionality measure was a dichotomous indicator, where absence of exceptionalities was coded as “0” and presence of exceptionalities was coded as “1.”
Weight and obesity were measured in Wave 1 by calculating the participant’s BMI. According to the Centers for Disease Control and Prevention, children and adolescents whose weights are less than the 5th percentile are underweight, children and adolescents whose weights are greater than the 5th but less than the 85th percentile are a healthy weight, children and adolescents whose weights are greater than the 85th percentile but less than the 95th percentile are overweight, and children and adolescents whose weights are equal to or greater than the 95th percentile are obese. In the present study, individuals scoring between the upper and lower deciles were coded as healthy weight (= 0), while those in the lower decile were underweight (= 1) and those in the upper decile were overweight (= 2). Healthy weight individuals were treated as the reference category in the multivariate analyses. The height variable is a continuous variable measured in inches. The school type variable in this study took the original school type measure in the NLSY97 and modified the 11 available values down to 3 (1 = public school, 2 = private school, 3 = other 1 ), with public schools acting as the reference category.
Urbanity is a nominal variable, where rural was coded as “0,” urban was coded as “1,” and unknown was coded as “2.” Urban environments were excluded as the referent. The NLSY97 provided a delinquency score index containing 10 dichotomous indicators of the respondent’s self-reported involvement in specific delinquent behaviors. The delinquency score measure for the present study was calculated using 7 of the original 10 variables. Participants were asked if they had ever carried a handgun, purposely destroyed or damaged property, stolen anything less than US$50, stolen anything greater than US$50 including a car, committed other property crimes, purposely attacked someone with the intent to hurt or fight, or helped sell illegal drugs (yes = 1, no = 0). Responses were summed for a total count ranging from 0 to 7, with higher scores indicative of greater incidents of delinquency.
Analytical Strategy
The primary goal of this research is to examine the effect of childhood, adolescent, and chronic bullying on seven outcomes (academic competence, arrests, convictions, depression, sleeping difficulties, substance abuse, and violence), whose measures are described above. In pursuit of this goal, we employ a PSM analysis. PSM is a quasiexperimental design that reduces the bias due to confounding variables by approximating the experimental conditions of random assignment to treatment. Drawing on the experimental logic of the estimation of a counterfactual, PSM pairs cases in the treatment condition to cases in the untreated condition to serve as the counterfactual comparison (Apel & Sweeten, 2010), where treatment can be defined as any intentional intervention. Here, we are defining treatment as one’s status as a childhood bullying victim, an adolescent bullying victim, or a chronic victim who was victimized in childhood and adolescence. A propensity score is defined as “the conditional probability of assignment to a particular treatment, given a vector of observed covariates” (Rosenbaum & Rubin, 1983, p. 41). In other words, one can use multiple observed variables to estimate the propensity of having received treatment, in this case one of the bullying conditions. Cases in the treated and untreated conditions can then be paired based on equivalent propensity for having received treatment in order to estimate the average treatment effect (ATE).
Using the NLSY97 sample described above, we use PSM to estimate the ATE of childhood, adolescent, and chronic bullying on seven outcomes. We therefore perform a total of 21 PSM analyses. Analyses were performed in R Version 3.2.2 using the matching package created by Sekhon (2011). For robustness, we use a one-to-one, three-to-one, and five-to-one nearest neighbor matching protocol where one, three, and five nonvictims were matched to each victim, such that participants who were victimized in childhood were matched with participants who were not victimized in childhood. Similarly, PSM was also utilized to match participants who were victimized in adolescence with participants who were not victimized in adolescence, and chronic victims were matched to nonchronic victims. The ATEs of childhood, adolescent, and chronic bully victimization were then estimated. Missing cases were most often the result of noninterview and were, therefore, excluded from the analysis. To maximize the number of valid cases, PSM models for each dependent variable were run separately.
For both childhood and adolescent bullying, we estimated the propensity score, P(xi ), using the logistic distribution function. 2 The crucial output from this model of treatment status, P(xi ), is the predicted probability of experiencing childhood, adolescent, or chronic bullying. This predicted probability is used as the propensity score in the subsequent matching procedures.
Results
Table 1 presents the descriptive statistics for the subsamples used in predicting the consequences of childhood, adolescent, and chronic bully victimization, while Tables 2–4 depict the propensity score models and balance diagnostics of the subsamples. Because of missing data, separate subsamples were required for estimating the treatment effect of bullying on sleep difficulty and depression, and these subsamples are shown in Tables 3 and 4, respectively. For the main subsample in Table 2, results from the logistic regression equations predicting childhood, adolescent, and chronic bullying are shown. The model predicting the probability of experiencing childhood bullying indicates that childhood bullying victims are likely to be younger, are more likely to be male, have a higher family/home risk index, are more likely to be overweight, and have higher scores on the delinquency scale than those who do not experience childhood bullying. The models predicting adolescent and chronic bullying are less robust, only indicating that adolescent bullying victims are likely to be older and less likely to be White, while chronic victims are likely to be older, attend schools that are neither public nor private, and have higher scores on the delinquency scale than nonvictims.
Descriptive Statistics for Subsample 1 (Used in Predicting Academic Competence, Arrests, Convictions, Substance Use, and Violence), Subsample 2 (Used in Predicting Depression Score), and Subsample 3 (Used in Predicting Sleep Difficulties Score).
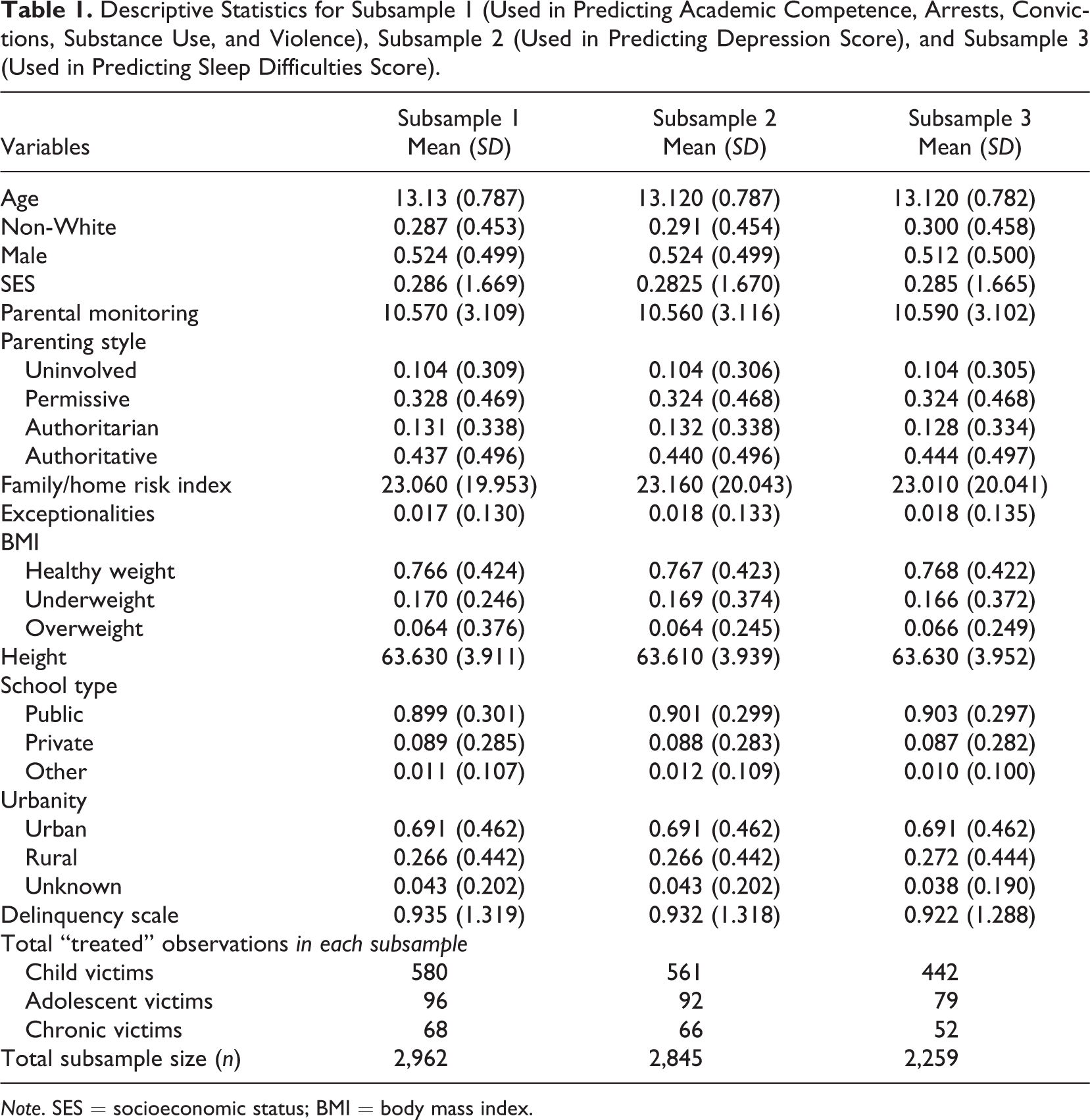
Note. SES = socioeconomic status; BMI = body mass index.
Propensity Score Models for Subsample Used in Predicting Academic Competence, Arrests, Convictions, Substance Use, and Violence.
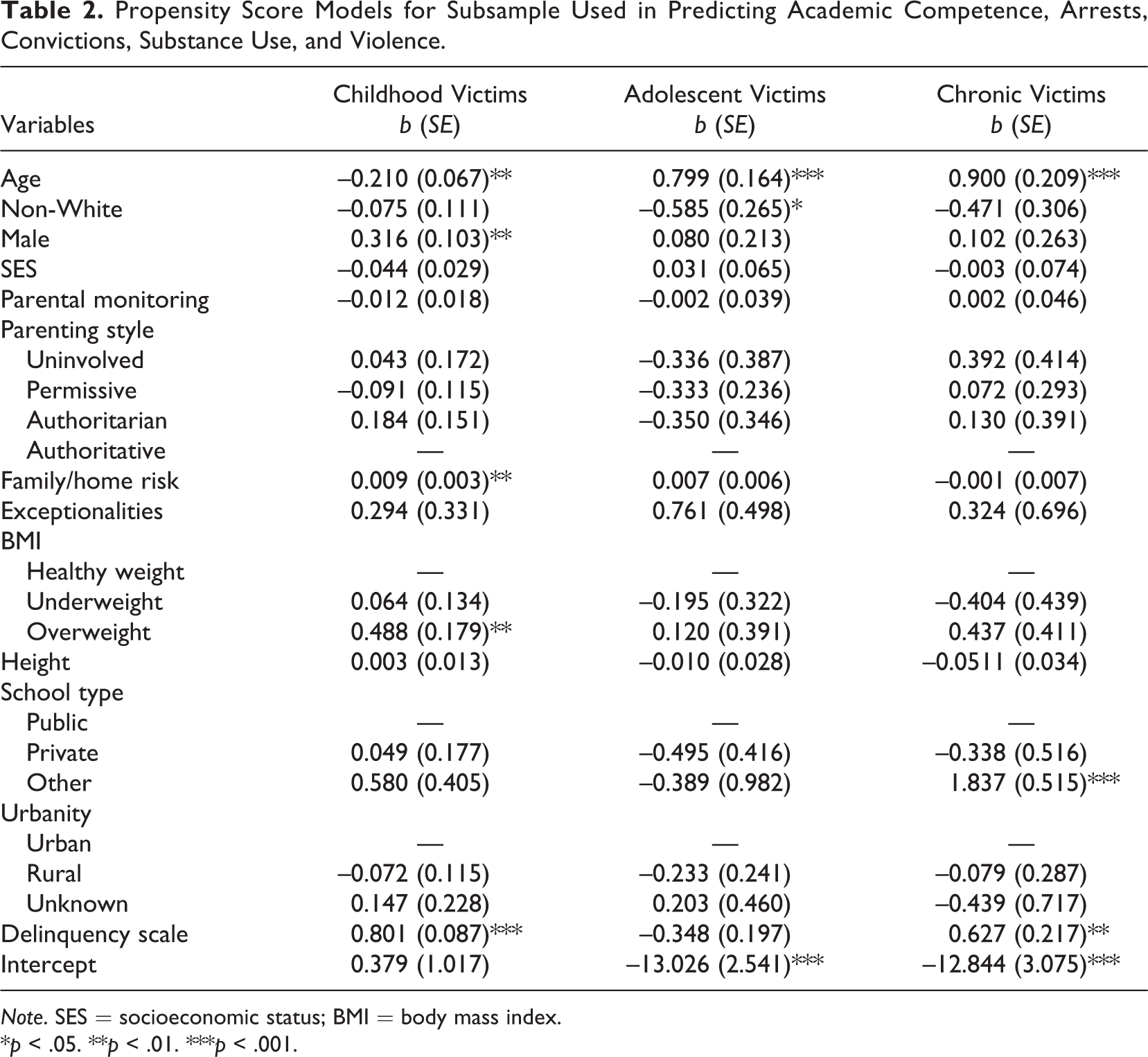
Note. SES = socioeconomic status; BMI = body mass index.
*p < .05. **p < .01. ***p < .001.
Propensity Score Models for Subsample Used in Predicting Depression Score.

Note. SES = socioeconomic status; BMI = body mass index.
*p < .05. **p < .01. ***p < .001.
Propensity Score Models for Subsample Used in Predicting Sleeping Difficulties Score.
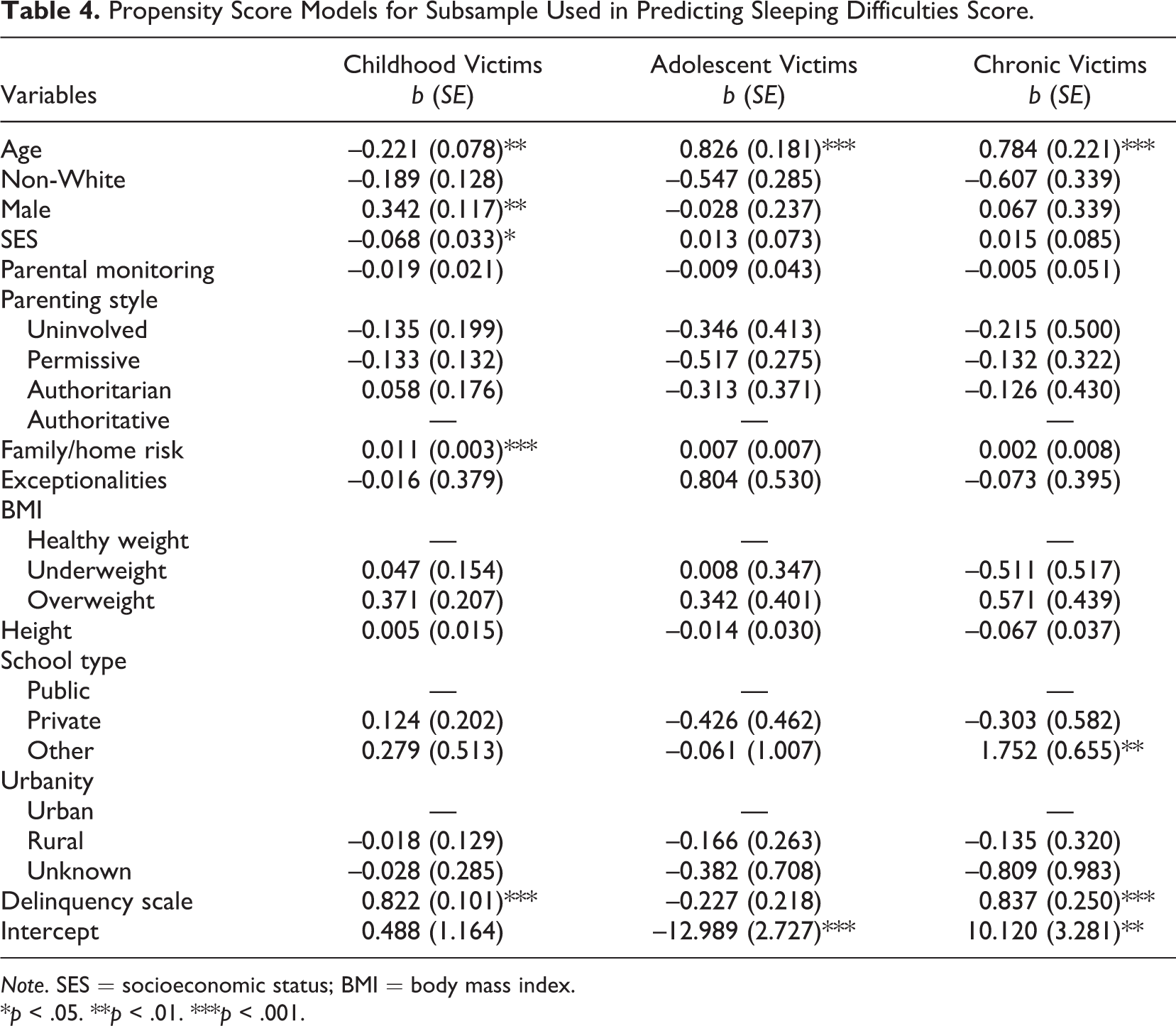
Note. SES = socioeconomic status; BMI = body mass index.
*p < .05. **p < .01. ***p < .001.
The logistic regression predicting probability of childhood bullying for the depression subsample (Table 3) indicated that childhood bullying victims are likely to be younger, are more likely to be male, are more likely to be overweight, and have higher scores on the delinquency scale. The adolescent bullying model for the depression subsample indicated that victims were likely to be older and less likely to be non-White than nonvictims. Finally, the chronic bullying model for the depression subsample indicated that victims were likely to be older, attend schools of other types, and have higher delinquency scores. The pattern of low sample size for adolescent and chronic bullying victims continued in these models. Only 92 respondents were adolescent bullying victims, and only 66 were chronic bullying victims.
The logistic regression predicting childhood bullying for the sleep difficulties subsample (Table 4) is quite similar to the model for the larger subsample. Here, childhood bullying victims are likely to be younger, are more likely to be male, come from lower SES, and have a higher family/home risk index and higher delinquency scores than nonvictims. As with the larger subsample, the model predicting the probability of adolescent bullying suffered from low sample size; of the 2,259 included respondents, only 79 were adolescent bullying victims. The model indicated these individuals were likely to be older than nonvictims. The chronic victim model also suffered from low sample size; only 52 respondents were chronic bullying victims. This model duplicated the results from the main sample, suggesting victims were likely to be older, are more likely to attend schools of other types, and have higher delinquency scores.
To assess the balance on included covariates between the treated and untreated cases, we have included the standardized bias (SB) measures before and after matching for each treatment condition for each of the three subsamples in Tables 5–7. Conventionally, covariates with |SB| > 20 are considered imbalanced. For the childhood bullying models in all three subsamples, four variables were imbalanced prior to matching. These four variables were consistently found to be sex, parental monitoring, family/home risk, and delinquency. After matching, there were no longer any SBs greater than 20, indicating that the matching procedure achieved balance. In the PSM models for adolescent bullying victimization prior to matching, treated and untreated cases were imbalanced on age and race. 3 The matching procedure greatly improved balance on age but failed to achieve balance, while achieving balance on race. This was likely due to the weak model fit stemming from low variation on the dependent variable but nonetheless presents a limitation. In the chronic bullying models, age, parental monitoring, underweight BMI, schools of other types, and delinquency were imbalanced prior to matching, and the matching procedure was able to achieve balance on most but not all of these covariates. Some measures additionally became imbalanced after matching, highlighting the problems resulting from low variation on the dependent variable.
Balance Diagnostics for Subsample Used in Predicting Academic Competence, Arrests, Convictions, Substance Use, and Violence.
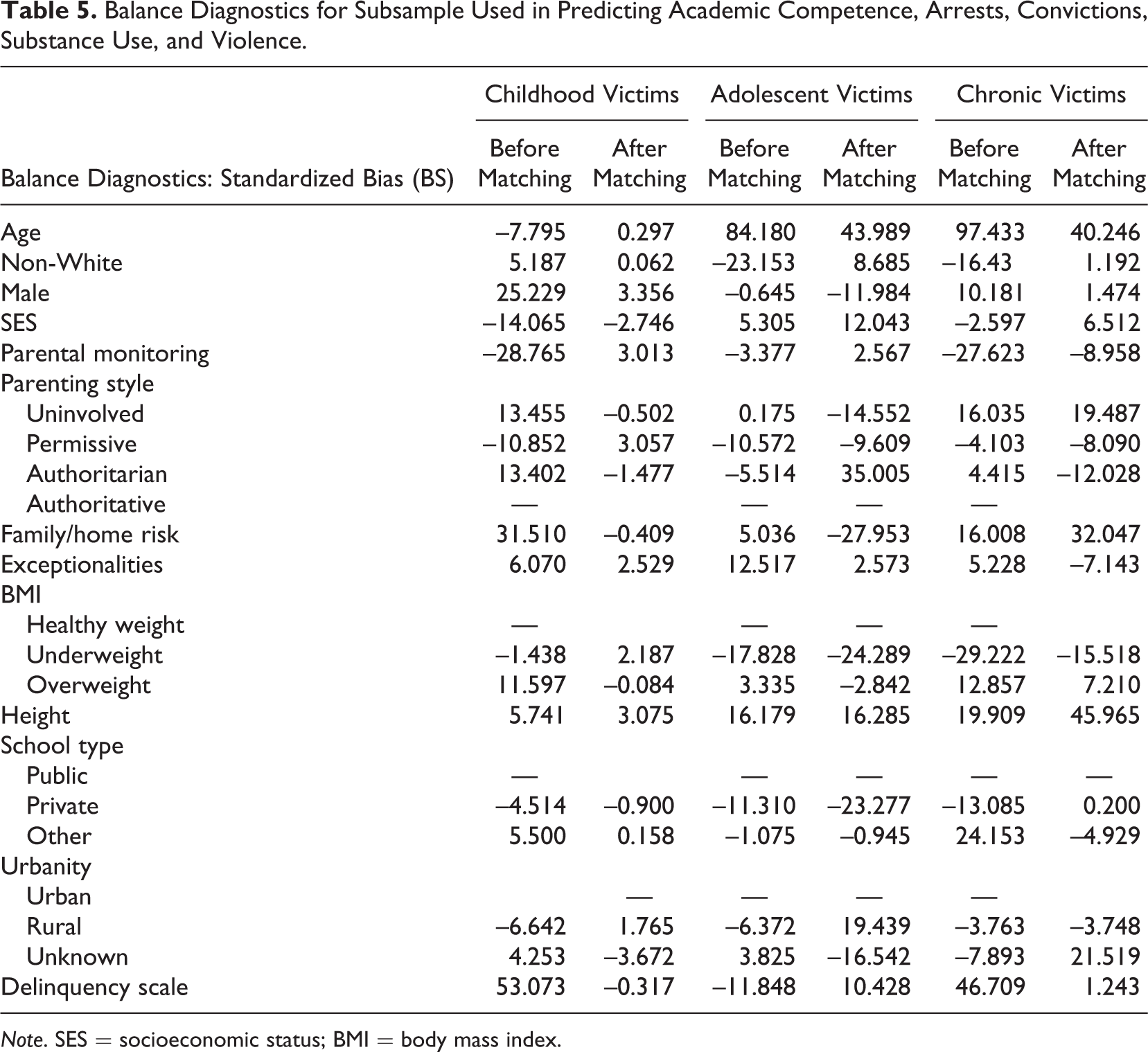
Note. SES = socioeconomic status; BMI = body mass index.
Balance Diagnostics for Subsample Used in Predicting Depression Score.
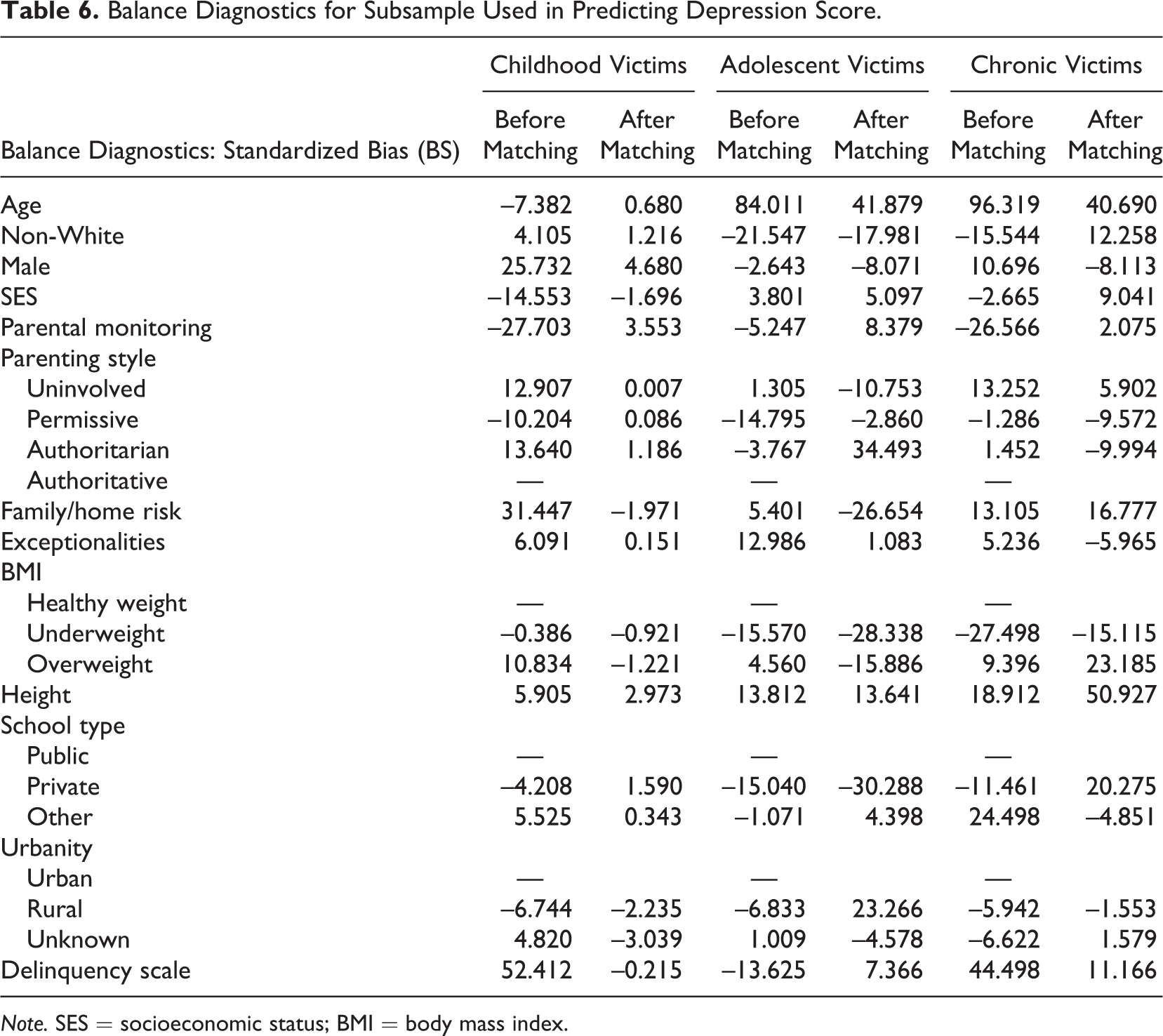
Note. SES = socioeconomic status; BMI = body mass index.
Balance Diagnostics for Subsample Used in Predicting Sleeping Difficulties Score.

Note. SES = socioeconomic status; BMI = body mass index.
We assessed the distributions of the propensity scores for treated and untreated cases. Considering the three treatment conditions separately, we plotted the proportion of treated and untreated cases in each of 20 equally sized bins. There was substantial overlap between treated and untreated cases for all three bullying conditions, demonstrating common support (results shown in Figure 1). These distributions are based on the largest subsample seen in Table 2, but results from the two smaller subsamples mirror these and have not been included in the interest of space. Lastly, the diagnostics for balance on covariates presented here have all been based on a three-to-one nearest neighbor matching protocol with no caliper. Balance diagnostics for one-to-one and five-to-one nearest neighbor matching protocols replicate the conclusions detailed above.
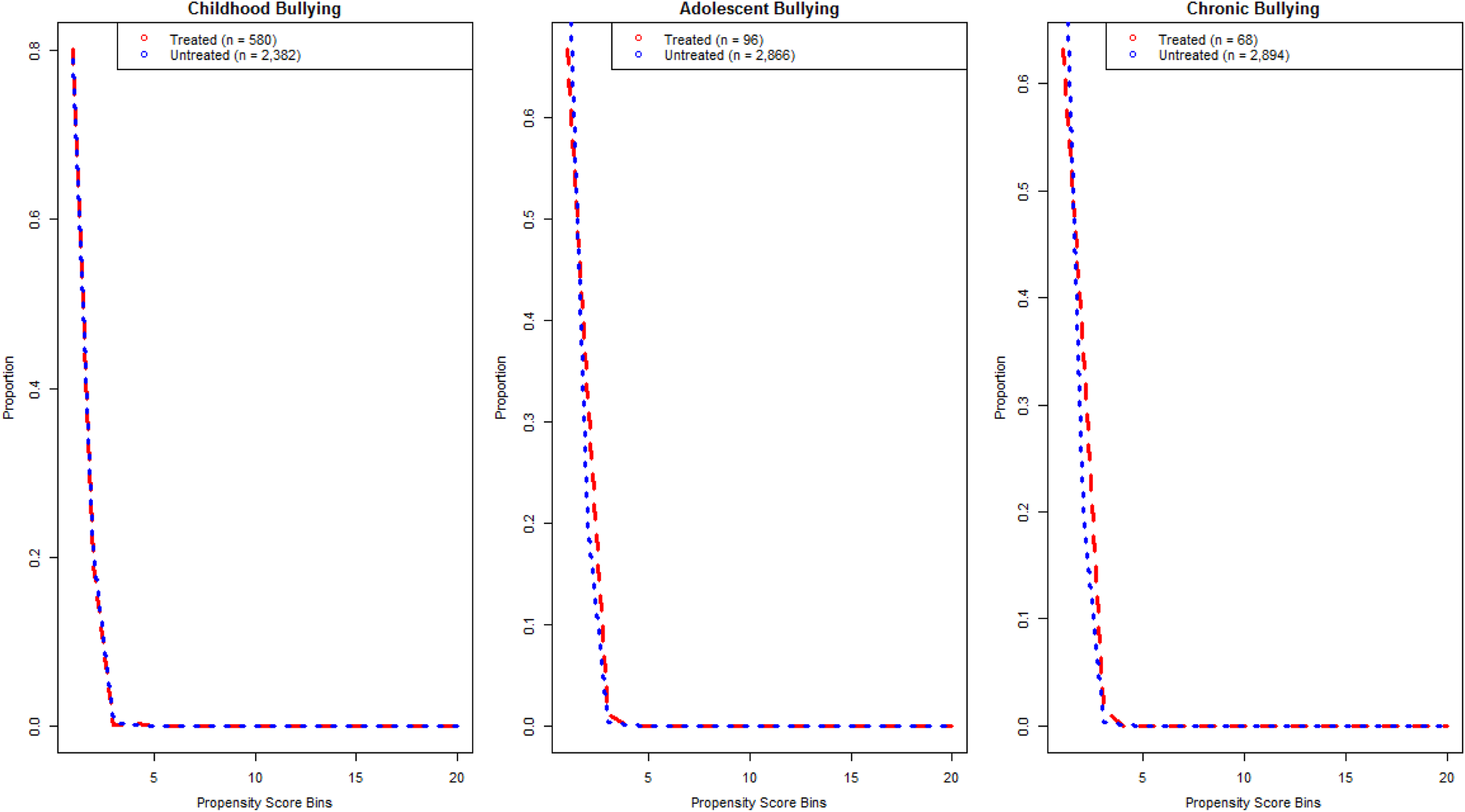
Propensity score distributions by treatment conditions.
Table 8 reports the ATEs of childhood, adolescent, and chronic bully victimization on each of the dependent variables. For robustness, we estimated the ATEs of each bullying condition on each of the seven outcomes using three model specifications. We estimated the ATE using a one-to-one nearest neighbor match with no caliper, a three-to-one nearest neighbor match with no caliper, and a five-to-one nearest neighbor match with no caliper. Results from these models are consistent across model specification, supporting the contention that results are not contingent on the choice of matching strategy. The results show that child victims are consistently shown to experience negative residual effects as a result of their bully victimization experience. Child victims had higher instances of arrests, depression, substance abuse, and violence compared to childhood bullying nonvictims. These findings are consistent with the current literature: Individuals who are victims of bullying engage in problem behaviors such as violence, substance use, and criminal offending (Liang et al., 2007; Luk et al., 2010; Mitchell et al., 2007; Sourander et al., 2007). It is worthwhile to note that no significant differences emerged when investigating the impact of bully victimization on sleep difficulty. The consequences of childhood bully victimization seem to appear primarily in the form of externalizing behaviors, not internalizing behaviors.
Average Treatment Effect (ATE) of Bullying Conditions on Included Outcomes.
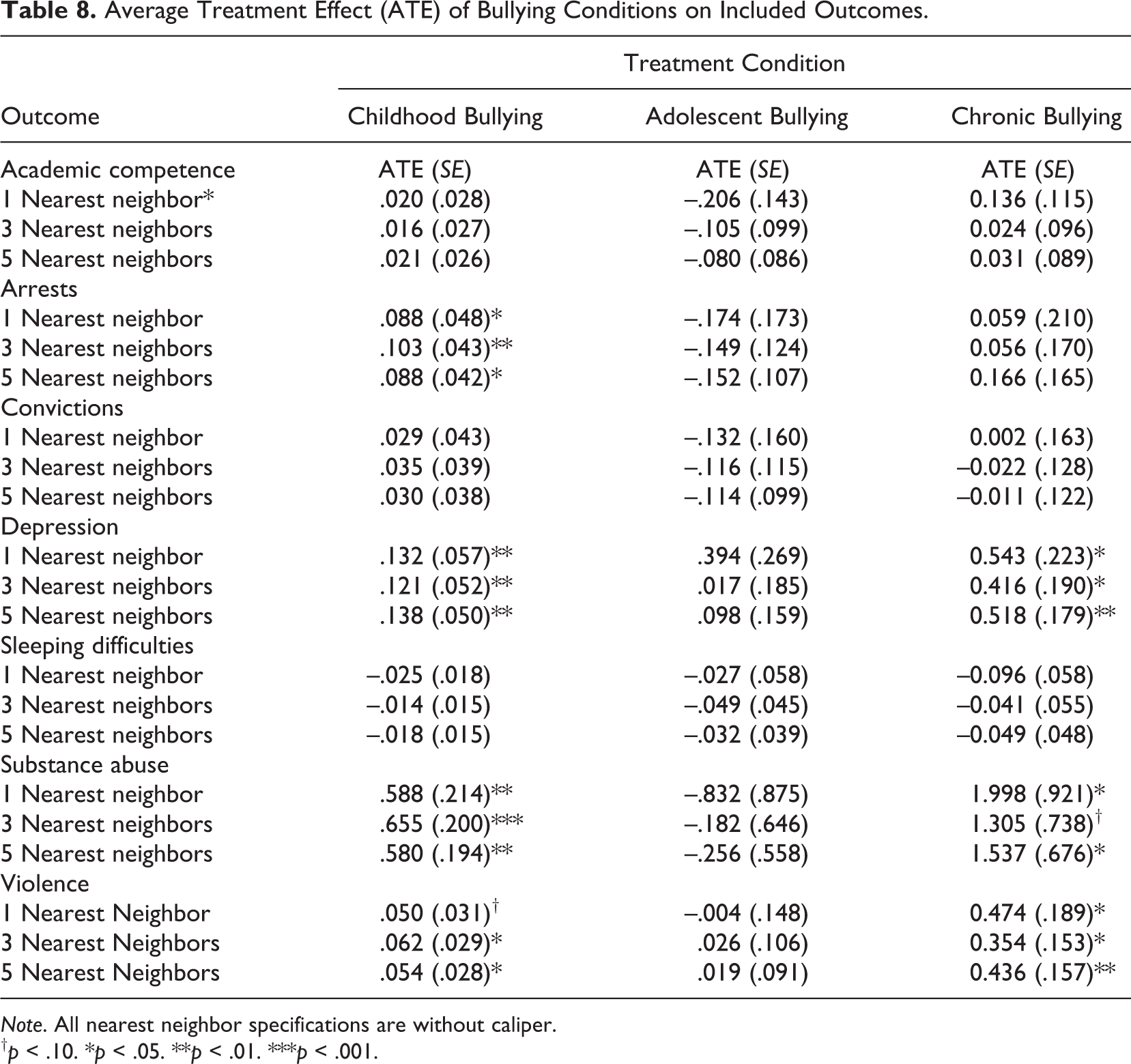
Note. All nearest neighbor specifications are without caliper.
† p < .10. *p < .05. **p < .01. ***p < .001.
Unlike childhood victims, adolescent victims did not significantly differ from adolescent nonvictims in terms of adverse consequences. No ATE for adolescent bullying on any of the considered outcomes reached the conventional level of statistical significance. The lack of significant findings for adolescent victims may be due, in part, to the extremely low instances of adolescent victimization. Furthermore, the total treated observations for adolescent victims were consistently smaller than the total treated observations for child victims. As noted above, chronic victims also had consistently smaller number of total treated observations. Despite this limitation, chronic victims showed a significant ATE for higher levels of depression and violence compared to nonvictims. Two of the three model specifications also showed a significant ATE for substance abuse, suggesting that chronic bullying victims may be more prone to using illegal substances. Due to low sample size, further research into this possibility is warranted.
Discussion
Exploring the long-term consequences of individuals who had experienced being victimized by a bully has captured the attention of scholars. Research has documented that adverse consequences occur not only proximate to the victimization incident, but also they emerge several years later in adulthood (Kim et al., 2011; Turner et al., 2013). The goal of the current study was to identify whether the long-term consequences of bully victimization were similar (or different) depending on the developmental period (i.e., childhood, adolescence, or chronic victimization) in which the bullying incidents occurred. Three important findings in alignment with our research questions emerge from our efforts.
First, we were able to identify the extent to which individuals experience bully victimizations during childhood and adolescence. Despite the concerns with using a retrospective, single-item repeat bully victimization measure, a significant proportion of individuals reported experiencing victimization incidents during childhood and adolescence. To be sure, one in five children below the age of 12 reported that they had experienced bully victimization; about 1 in 30 adolescents between the ages of 12 and 18 reported bully victimization, and 1 in 50 reported chronic bullying across childhood and adolescence. Although a significant majority of individuals reported they never experienced bully victimizations, it is worth noting that the measures used in this study are documenting repeated bully victimizations. These victims are not reporting an isolated incident that occurred on a playground or bus ride to school. Rather, these individuals are reporting they were repeatedly victimized over a period of time. Second, significant differences emerged in the characteristics across the victim and nonvictim groupings. These differences included age at Wave 1, sex, SES, parental monitoring, parenting style, family/home risk, and presence of exceptionalities. These results not only suggest that nonvictims differ from victims but that individuals who are victimized at different ages differ from one another. Particularly of note was that childhood victims were more likely than the other victim groups to be male. This finding suggests that gender plays a role in early childhood victimization.
Finally, we identified that there were differences in the consequences experienced by the different victim groups. Compared to adolescent or chronic victims, childhood victims were significantly more likely to endure negative residual consequences in adulthood as a result of their bullying experience. Individuals victimized as children reported higher instances of arrests, convictions, depression, violence, and substance use than child nonvictims. Alternatively, adolescent victims did not significantly differ from adolescent nonvictims in terms of residual consequences, and chronic victims differed only with respect to substance abuse and violence.
In line with the life-course perspective, these results seem to convey an important point. That is, repeated bully victimization experienced in childhood appears to have more impactful adverse effects in adulthood than bully victimization occurring in adolescence. The enhanced vulnerability in childhood may be due to it being a sensitive developmental period in the life course. Indeed, research suggests that childhood is a developmental period during which vulnerability and susceptibility to risk are enhanced (Turner, Hartman, Exum, & Cullen, 2007). Therefore, those who are victimized in childhood, compared to those who are victimized in adolescence, may not be able to adequately cope with their bullying experience (see Garmezy, 1985; Werner, 1989). Developmental psychologists refer to the variability in the influence of risks as “sensitive periods” in development where vulnerabilities to the causal influences of a risk are heightened compared with other periods in the life course (Bateson & Hinde, 1987). As such, individuals possess a greater susceptibility to the risk if it were to occur during the sensitive period, such as childhood, as opposed to some other point in time. This finding is especially poignant in light of the more varied negative consequences of bullying in childhood only compared to chronic victimization. The lack of significant findings for chronic victims may have been a result of low base rates of victimization (discussed below), or it may be that a confirmation that childhood bullying victimization indeed creates a severe vulnerability, compared to other time periods.
Policy Implications
Because those who experience repeated bully victimization during childhood are likely to experience negative consequences, and these consequences are relatively serious in nature, prevention and intervention are particularly important for this age-group. That is, prevention programs should be implemented early to target individuals in elementary and secondary school to intervene before bullying occurs. Many early intervention programs have been shown to be effective at reducing the occurrence of bullying (see Espelage & Swearer, 2004; Olweus & Limber, 2010)—promising programs should be expanded to target the types of bullying younger children are likely to experience and should be targeted especially at younger children. Our findings from the PSM analysis also indicate that the correlates of being a childhood bullying victim, an adolescent bullying victim, and a chronic victim differ somewhat. Insomuch as these factors are different, they should be targets for change for individuals during those specific developmental time periods. In this way, prevention programs should be age-specific. Not only should they be age-specific, but our findings indicate the childhood victims are more likely to be male than be female. This finding shows that prevention programs may be specially designed for young males. Future research should explore if risk factors operate the same for male and female childhood victims. In addition, programs should be designed to address bullying after it occurs, so that victims can receive resources to hopefully assuage the negative consequences of their victimization experience. For example, research on coping after bullying suggests that youth who use problem-solving styles of coping experience lower psychological distress than those with an avoidant coping style (Hunter, Nora-Merchan, & Ortega, 2004). Teaching such coping strategies can be incorporated into intervention programs. In addition, teachers, parents, and other children need to be taught to effectively intervene when they see bullying behaviors. Such bullying prevention programs that incorporate bystander intervention have been shown to increase responses by individuals witnessing the victimization, but the effects are larger for high school students compared with kindergarten through eighth-grade students (Polanin, Espelage, & Pigott, 2012). Future research should consider the different types of bullying victimization that younger children may experience, as research suggests that coping strategies are differentially effective for different types of bullying (Hunter et al., 2004).
Limitations and Future Directions
Notwithstanding these findings, it is important to identify the limitations of our research. First, the findings of this project are based entirely on secondary data. The NLSY97 was funded with the intent to examine youths entering the workforce and their transition into and out of the workforce. Although using secondary data is often beneficial in terms of time and finances, the use of the NLSY97 constrains the scope of the current study because the measures are limited. For example, age-specific predictor variables caused the sample to be restricted to participants between the ages of 12 and 14 during Wave 1, which reduced the sample size. Future research with larger samples should be conducted. In addition, we were unable to explore whether differences existed among bullies and/or bully victims (i.e., individuals who both bullied and were victimized). Consistent with past research, it is possible that the negative consequences are more severe for those both who are bullied and who bully—this avenue of research should be explored in the future (see Nansel et al., 2001). Second, repeat bully victimization was measured with a single item, which only asked if the participant was ever the victim of repeated bullying (either before the age of 12 or between the ages of 12–18). It is unfortunate that the method by which the individual was victimized (i.e., physical, verbal, relational, and cyber) was not included in the measure. Future research should focus on capturing different types of bullying to investigate whether different types of bullying have different consequences later in the life course (see Turner et al., 2013). Third, the base rates of adolescent-only and chronic victimization in the sample were extremely low. This also suggests that victimization during adolescence virtually requires victimization during childhood—a modification of Robins’ paradox as it pertains to delinquency and crime. As previously discussed, research with larger samples may allow for the identification of a greater number of adolescence-only and chronic bullying victimization. Finally, some scholars might believe that the NLSY97 data are old and perhaps might not apply to the adolescents of today. We should point out, however, that the nature of our research question demanded that we assess individuals over an extended period of time that includes three developmental periods (i.e., childhood, adolescence, and adulthood). Because of this, we could not investigate our questions with individuals who are currently being victimized. We encourage future scholars to explore these issues using more contemporary data.
Conclusion
In closing, bullying is a complex social problem that affects a large proportion of youths. Bully victimization is an important behavior to examine, especially due to the long-term negative consequences that arise from childhood victimization. It is of great concern that child victims have higher instances of arrests, convictions, violence, and substance use as a result of being bullied. It is important for future researchers to contribute to the victimization literature, in general, and specifically to contribute to furthering knowledge on the consequences of bully victimization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.