
Abstract
Polyvictimization refers to multiple forms of victimization experienced by youths. The extent to which aggregated or cumulative early life victimization increases risk of victimization within juvenile correctional facilities is unclear. Furthermore, pathways from early polyvictimization to facility victimization may be partly explained by trauma symptomatology. Drawing upon the extant polyvictimization literature, this study explores both composite and cumulative effects of childhood victimization on later victimization within correctional facilities and the mediating role of trauma symptomatology among a nationally representative sample of incarcerated youth. Data were drawn from the Survey of Youth in Residential Placement. Incarcerated youths (N = 7,073) were surveyed on constructs including early victimization, trauma symptomatology, and experiences of victimization within correctional facilities. Using appropriate weights in analyses, structural equation models revealed the relationship between amassed early polyvictimization and composite facility victimization was partially explained by trauma symptoms; facility victimization also linked to trauma symptoms. Additional models revealed that as youths report more victimization experiences, there was a successive increased likelihood for trauma symptoms, facility robbery, and facility physical victimization. The relationships between cumulative early victimization and facility robbery, physical, and sexual victimization were partially or fully mediated by trauma symptoms. Research and practice implications are discussed.
Literature Review
Introduction
Early life victimization, which may involve sexual, physical, or emotional abuse; exposure to domestic violence; abandonment; or neglect, occurs all too often in the lives of youth (Costello, Erkanli, Fairbank, & Angold, 2002; Finkelhor, Ormrod, Turner, & Hamby, 2005; Ford, Chapman, Mack, & Pearson, 2006). Rates of victimization among delinquent youths, however, are about 2 times higher than those in the general population (Coleman, 2005; Coleman & Stewart, 2010). Approximately 40–60% of adjudicated delinquent youths have been victimized (Currie & Tekin, 2006; Ford, Chapman, Hawke, & Albert, 2007; Stahl, 2006). Victimization research has tended to focus narrowly on a single event occurring at one point in time (Turner, Finkelhor, & Ormrod, 2010), despite contrary findings that youths who endure one type of victimization are likely to experience other forms (Dong et al., 2004; Finkelhor, Ormrod, & Turner, 2007a; Saunders, 2003) in other contexts (Turner, Shattuck, Finkelhor, & Hamby, 2016). Consequently, research has also investigated the effects of multiple types or forms of abuse experienced by youth and children, a concept coined polyvictimization (Finkelhor, Ormrod, & Turner, 2009a).
Abuse or victimization experiences can lead to myriad adverse outcomes (Turner et al., 2010) including trauma symptomatology (Cuevas, Finkelhor, Clifford, Ormrod, & Turner, 2010; Finkelhor et al., 2007a) and repeated victimization (Cuevas et al., 2010; Tseloni & Pease, 2003; Turanovic & Pratt, 2012b). Given that revictimization is higher among youths who have endured polyvictimization (Finkelhor, Ormrod, & Turner, 2007b), juvenile justice–involved youths with cumulative victimization experiences may be at greater risk of victimization in confined settings. However, this has yet to be tested. Further, the relationship between polyvictimization and repeated victimization experiences may be partially explained by the trauma symptoms that often accompany early victimization experience(s) (Cuevas et al., 2010). Nevertheless, there is limited research on the extent to which early life amassed or cumulated forms of victimization increase risk of facility revictimization in juvenile justice settings, whether this relationship is partially explained by trauma symptomatology, or whether facility victimization also contributes to trauma symptoms. This study uses a nationally representative sample of incarcerated youths to (1) test the relative effects of composite and cumulated early life victimization on collective and independent experiences of physical and sexual victimization and robbery in juvenile correctional facilities, (2) determine the mediating effects of trauma symptomatology in these relationships, and (3) determine the independent relationship between facility victimization and trauma symptoms.
Guiding Framework
While there are many theoretical frameworks explaining the etiology of juvenile offending, the polyvictimization/revictimization literature can elucidate linkages between multiple forms of early life victimization and revictimization experiences among individuals in correctional facilities (Listwan, Daigle, Hartman, & Guastaferro, 2014). Specifically, robust research reveals successive effects of early victimization; one or more experience(s) creates cumulated risk of trauma symptomatology and subsequent revictimization relative to never experiencing victimization (Finkelhor et al., 2007b; Turner et al., 2010). This body of work symbolizes a victim–repeat victim hypothesis; it is a nexus of experiences in which multiple forms of early life victimization create vulnerabilities that then generate additional risk of victimization. Such a framework may be applied to juvenile justice involved youths, adding to the victim-offender hypothesis (see Widom, 1989) to further explicate why victimized offenders may be revictimized in incarceration settings. Nevertheless, there are very few studies examining the relationship between polyvictimization, revictimization, and the mediating role of trauma among incarcerated youths; the effects of facility victimization on trauma symptoms; and even fewer studies have methodologically calculated both a total and cumulative polyvictimization score to determine relative impacts.
Polyvictimization, Trauma Symptoms, and Revictimization
Polyvictimization, or experiencing multiple forms of abuse (Finkelhor et al., 2007a; Turner et al., 2010), occurs somewhat frequently among youths and children. Among a sample of nearly 2,000 recently detained, pretrial youths, aged 10–17 years, 5% of participants who reported histories of multiple forms of adversity met criteria for polyvictimization (Ford, Grasso, Hawke, & Chapman, 2013). These youths experienced an average of 5 of 11 different types of traumatic victimizations (Ford et al., 2013). Additionally, in a nationally representative sample of over 4,000 children and youths aged 2–17 years, approximately 66% experienced more than one type of victimization, 30% experienced five or more forms, and 10% experienced 11 or more forms (Turner et al., 2010). The risk factors for polyvictimization among older youths (12–17 years of age) include co-occurring unfavorable life experiences such as dangerous communities, unsafe families, and multiproblem family contexts (Finkelhor, Ormrod, Turner, & Holt, 2009b).
Abuse or victimization experiences can lead to negative psychological, emotional, physical, and physiological outcomes (Turner et al., 2010). There is a robust evidence base linking the experience of early life abuse to trauma symptoms (Ackerman, Newton, McPherson, Jonnes, & Dykman, 1998; Turner et al., 2010; Widom, 1999, 2000). Research suggests that trauma symptoms such as nightmares, bad thoughts, nervousness, or hypervigilance are common psychological responses to early life victimization (Cuevas et al., 2010) because of the way in which abuse experience(s) are physiologically and neurologically coded (Perry, Pollard, Blakley, Baker, & Vigilante, 1995). The human body is equipped to respond to abuse using fight or flight mechanisms (Perry, 2009). Therefore, differential response patterns to victimization events are possible and can range from hyperarousal (being defensive and displaying “fight or flight”) to dissociation (freezing and disengaging; Perry et al., 1995). Abuse experiences can activate physiological responses that serve a survival or protective function (Perry, 2009; Perry et al., 1995); these responses become health damaging when repeatedly stimulated or when a person continuously experiences victimization (Perry, 2009). Resultantly, trauma symptoms may be more severe with multiple forms of abuse (Turner et al., 2010). For example, trauma symptomatology has been found to be higher among polyvictimized youths relative to nonpolyvictimized youths (Finkelhor et al., 2007a) and polyvictimization experiences have been shown to predict more severe trauma symptoms (Finkelhor et al., 2006: Turner et al., 2010).
Polyvictimization experiences may also be a risk factor for later revictimization. In fact, longitudinal research has revealed that polyvictimized youths surveyed in Year 1 were at risk of recurring victimization in Year 2 (Finkelhor et al., 2007b). In a study examining the effects of revictimization patterns among polyvictimized youths, results suggest that one victimization experience creates risk of additional forms of victimization in different contexts (Finkelhor et al., 2006). Some scholars have referred to this as a “contagion” effect (see Mohr, 2006), whereby multiple forms of victimization in one situation can foster hyperarousal, fear, or dysregulation in other situations (Finkelhor et al., 2009b). So, the early polyvictimization experience can create psychological struggles that are carried into other contexts (Finkelhor et al., 2009b); youths can develop a victim profile characterized by social isolation or deficits in interpersonal and coping skills that may be markers for vulnerability to revictimization experiences (Finkelhor et al., 2006).
Therefore, the relationship between polyvictimization and revictimization may indeed be partly understood through trauma symptoms. Trauma symptoms have been found to increase the likelihood for revictimization; specifically, this has been demonstrated among sexual abuse victims, as risk of ongoing sexual abuse was explained by associated trauma symptomatology (Risser, Hetzel-Riggin, Thomsen, & McCanne, 2006). Furthermore, research has shown that polyvictimization experiences have a stronger link to trauma symptoms than the experiences of repeated victimization (Turner et al., 2010), suggesting that perhaps trauma symptoms may be an intermediary pathway explaining the direct relationship between polyvictimization and repeated victimization. It is possible that as a person experiences more forms of victimization, they experience more severe symptoms, and, in turn, they are at increased risk of revictimization. Nevertheless, there is minimal research altogether exploring the relationship between early polyvictimization and revictimization (Finkelhor et al., 2007b) and even less research on revictimization among juvenile offenders residing in juvenile justice settings. Consequently, it is important to test these relationships in varied ways and to determine whether they are partially explained by trauma symptoms or whether trauma symptoms are also influence by victimization within juvenile justice facilities.
Victimization in Juvenile Justice Settings
Multiple research studies have indicated associations between victimization and juvenile justice involvement (Ford et al., 2006; Lin, Cochran, & Mieczkowski, 2011; Widom, 1989). Scholarship has also revealed that polyvictimized youths, compared to those who have just witnessed violence, are more involved in delinquency (Ford, Elhai, Connor, & Frueh, 2010; Lin et al., 2011). Furthermore, polyvictimized youths with complex trauma symptoms residing in secure juvenile facilities have impaired impulse control, pro-aggression schemas, and relationships with delinquent peers (Ford, Chapman, Connor, & Cruise, 2012). Accordingly, youthful offending may be a function of protective coping mechanisms or a reaction to reminders of early victimization (Ford et al., 2006). Nevertheless, environments characterized by violence, abuse, or neglect (like correctional facilities) may also contribute to internalizations of violence, as exposure to or consistent renderings of violence can shape insights that reinforce and normalize violence in various contexts (Costello et al., 2002; Ford et al., 2006). As such, victimized youths who commit crimes and reside in juvenile justice facilities are prone to additional victimization exposure that may also contribute to trauma symptomatology.
There has been a growing concern for the welfare and safety of youths in correctional facilities (Dozier et al., 2014). There are reports of victimization experiences at the hands of peers or staff within the juvenile correctional facilities (Attar-Schwartz, 2014). In fact, research has revealed that juvenile justice youths reported approximately 12–20 traumatic stressors within correctional facilities including witnessing victimization, being threatened, fear of being physically hurt, physical assault or abuse, and sexual assault (Abram et al., 2004). Also, victimization can lead to behavioral disruptions, suicidality, aggression and violence, or other emotional dysregulation (Attar-Schwartz & Khoury-Kassabri, 2015; Hodge & Yoder, 2017). Recurring victimization can be especially prominent among individuals leading high-risk lifestyles including delinquent youths (Finkelhor et al., 2007b; Turanovic & Pratt, 2012a, 2012b).
Thus, victims and victimizers are not mutually exclusive categorizations for juveniles. In fact, involvement with delinquent peers and committing serious offenses puts juvenile offenders at elevated risk of being victimized by others (Loeber, Kalb, & Huizinga, 2001). Low self-control coupled with these associated risks can lead victim-victimizers to be revictimized by other offenders while incarcerated (Schreck, Wright, & Miller, 2002). When victims and offenders are contained in close proximity, like incarceration settings, and under the control of others, there is a high likelihood that some of the offenders will also become victims of new crimes while incarcerated (Finkelhor & Asdigian, 1996; Loeber et al., 2001; Schreck et al., 2002). For example, in a study of adult prisoners from the Ohio Department of Rehabilitation and Correction, inmate reports of a hostile environment coincided with victimization experiences while incarcerated (Listwan et al., 2014). As such, victimization experiences in juvenile correctional facilities may also lead to or potentially even exacerbate trauma symptomatology (Wasserman & McReynolds, 2011).
Gaps in Research
While the polyvictimization framework has been used to explain how early life forms of victimization contributes to revictimization in other contexts (Finkelhor et al., 2006, 2009b), there has been minimal research that applies it to juvenile justice systems by specifically testing how polyvictimization creates risk of facility victimization or how trauma symptoms may mediate this relationship. Further, correctional facilities may intensify or cause repeated victimization experiences that produce a persistent state of vigilance that, when triggered, can lead to trauma symptoms (Perry et al., 1995). There is evidence to suggest that more so than other individual-level factors, increased early life victimization is associated with greater total institutional misconduct by inmates (DeLisi et al., 2010); perhaps this unexplored vulnerability in behavioral disruptions can be explained by trauma symptoms. So, although we know that adverse experiences within juvenile correctional facilities can contribute to trauma symptomatology (Hodge & Yoder, 2017), more research is needed on the effects of facility victimization on trauma symptoms. Finally, as some have critically appraised contemporary scoring of adverse childhood experiences as perhaps a bit reductive (using a total score rather than identification of specific risks or amassing risk; Finkelhor, 2017), it is imperative to study both the aggregated and cumulative impacts of multiple forms of victimization given the profound effect that just one victimization experience can have in a person’s life (Finkelhor et al., 2007b; Turner et al., 2010).
Purpose of This Study
The level of victimization within juvenile correctional facilities is an area of grave concern (Hodge & Yoder, 2017). This study seeks to explore the composite and cumulative effects of childhood polyvictimization on later sexual and physical victimization and robbery within the correctional facility and the mediating role of trauma symptoms among a nationally representative sample of incarcerated youths. Drawing upon the polyvictimization literature, the analyses are organized around three primary research hypotheses: (1) The relationship between amassed early victimization and facility victimization is partially mediated by trauma symptoms, but facility victimization also contributes to trauma symptoms; (2) there is a cumulative risk effect of early life victimization on trauma symptoms and robbery, sexual, and physical facility victimization; more forms of early victimization sequentially increase the risk of respective facility victimization and trauma symptoms; and (3) the relationship between cumulative early victimization and robbery, sexual, and physical facility victimization is partially mediated by trauma symptoms.
Method
Sample and Procedures
This article uses data from the Survey of Youth in Residential Placement (SYRP; Sedlak, 2003), an Office of Juvenile Justice and Delinquency Prevention (OJJDP)-sponsored research priority. The SYRP was the third part in a series of surveys aimed at capturing facility and juvenile-specific information to inform national knowledge of custody statistics. The survey was combined with two other census surveys, the Census of Juveniles in Residential Placement (CJRP) and the Juvenile Residential Facility Census (JRFC), which collected data on juvenile facility administrators.
The SYRP was a nationally representative, anonymous, self-report survey taken by pre- and postadjudicated youths who were aged 10–20 years and housed in juvenile facilities. The SYRP used a stratified two-stage probability proportional-to-size sample design, in which they first sampled the facilities and then clusters of youths were drawn from each facility (Sedlack et al., 2012). A total of 290 facilities were randomly sampled across 36 states. Of those, 240 were eligible for data collection, and 204 participated. Nonparticipating facilities were unable to establish clearance through state or local personnel authorities (Sedlak, 2010). Of the 9,495 eligible youths, 7,073 youths (74.5%) completed the surveys. The nonparticipating youths failed to receive parental consent, refused, were unavailable, or the facility refused (Sedlak, 2010). The SYRP directly queried incarcerated youths and gathered perspectives and life experiences rarely sought in large surveys at the time of data collection (Sedlak, 2010)—a particularly unique feature. Surveys were carried out between March and June 2003. The survey was administered using an audio-assisted self-interview (ACASI) methodology, where youths listen to a prerecorded voice read questions aloud, while questions are simultaneously being displayed on the computer screen. To safeguard sensitive material, strict anonymity procedures were followed in which a unique identifier was assigned to youths (Sedlak, 2010).
Due to the complex design, the data were assigned weights that are required for usage in analysis to yield accurate estimations (Sedlak et al., 2012). To adjust for the nested structure of the data (clusters of youths nested in facilities), over- and undersampling of facilities and youths, and youths and facility nonresponse rates, the principal investigators of the study employed design effects (see Sedlak, 2012). These methods included weight trimming, final weighting adjustments, and jackknife replication as an unbiased technique to calculate the sampling variance from complex survey data (Sedlak, 2012). When running the statistical analyses, it is required that researchers use these weights for precise parameter estimations (Sedlak, 2012); this will be discussed further in the analysis section. Access to the data was granted through approvals from the university institutional review board and the National Archive of Criminal Justice Data (NACJD) through the Inter-University Consortium for Political and Social Research (ICPSR) Data Access Request System (IDARS).
Participants
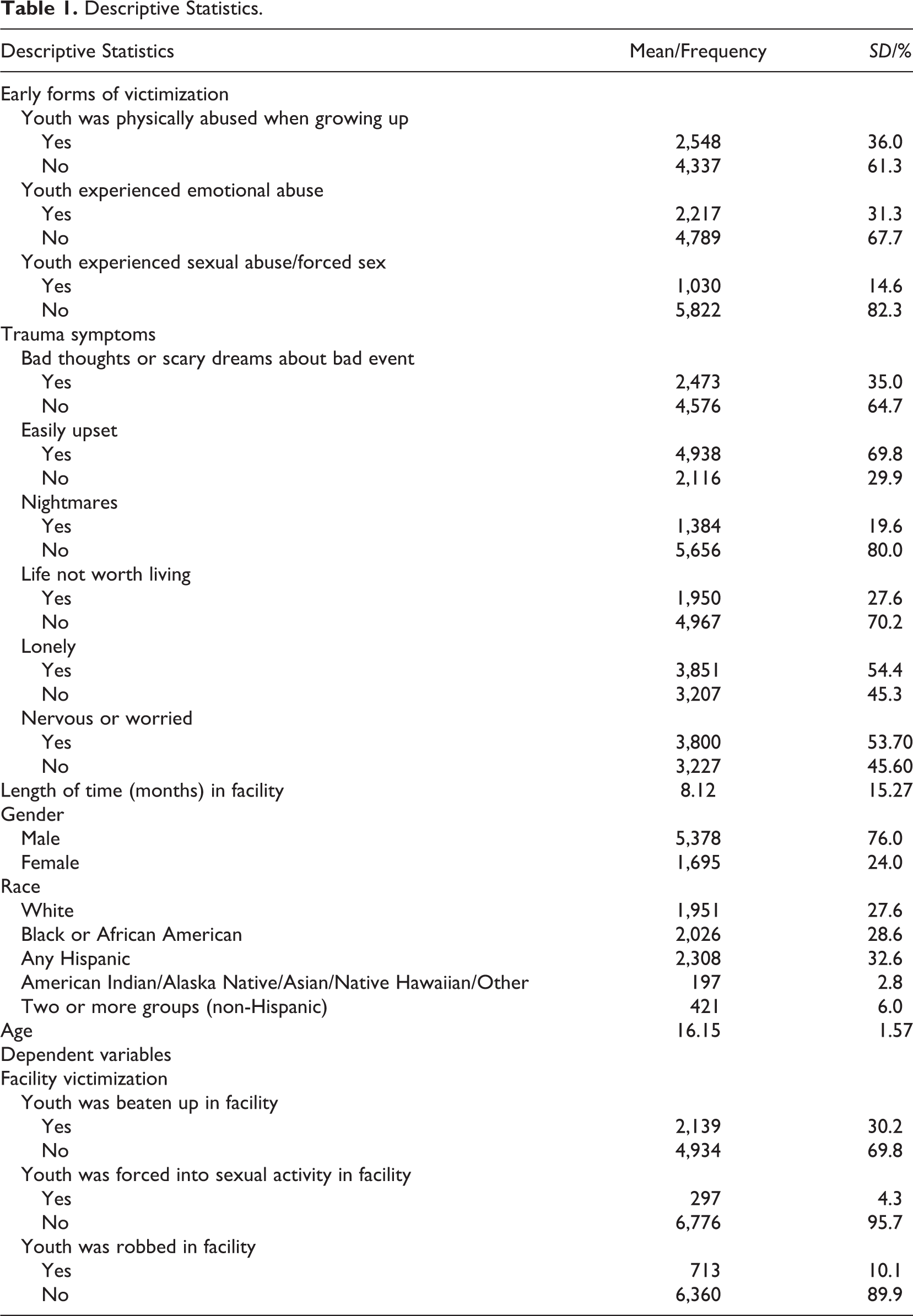
The sample participants (N = 7,073) averaged 16.5 years of age (SD = 1.5) were primarily males (n = 5,378; 76.0%), with slightly more White youths (n = 2,527; 35.7%) than Black youths (n = 2,403; 34.0%). The length of time is in months that the youths have been in their current facility (M = 8.12; SD = 15.27). The sample characteristics and additional descriptive statistics for all variables are provided in Table 1.
Descriptive Statistics.
Measures
Independent variables of interest included early polyvictimization and trauma symptoms. Demographics included age, gender, and race (individual dummy coded variable). There were three dependent variables that represent facility victimization and included robbery, sexual abuse, and physical abuse.
Independent Variables
Early polyvictimization
Early polyvictimization was an overarching term used to describe three forms of victimization (sexual, physical, and emotional). The variable was created using four dichotomous variables (0 = No; 1 = Yes) related to youths’ victimization experiences while growing up (see Finkelhor et al., 2007a). These variables included physical abuse, emotional abuse, sexual abuse, and forced sex. Example items included, “Were you physically abused while growing up?” or “Were you were emotionally abused while growing up?” Because of the overlap between sexual abuse and forced sex, with 52.5% of the reporting sample endorsing both forms of sexual victimization, the variables were collapsed to create a single sexual abuse variable. The final variables were sexual abuse, physical abuse, and emotional abuse. The variables’ values were cumulated to create one 3-level polyvictimization ordered variable (0 = none; 1 = 1 form; 2 = 2 forms; 3 = 3 forms). This variable yielded acceptable reliability (α = .748).
Trauma symptoms
The trauma symptoms variable was created from six dichotomous variables (0 = No; 1 = Yes) that pertained to traumatic symptoms youths experienced over the past few months. Example items include, “Over the past few months, have you had nightmares that are bad enough to make you afraid to go to sleep?” and “Over the past few months, have you had a lot of bad thoughts or dreams about a bad or scary event that happened to you?” and “Over the past few months, have you had nervous or worried feelings?” The variables were cumulated to create a scale that yielded acceptable reliability (α = .720).
Demographics and controls
Demographic and control variables were included in the models. Age was the number of years old at the time the survey was administered. Gender was dummy coded to indicate (0 = male; 1 = female). Youth’s race was measured as (1) Black, (2) any Hispanic, (3) American Indian/Alaska Native/Asian/Native Hawaiian/Other, and (4) Two or More Groups (non-Hispanic). A separate dummy coded race variable was created to indicate White = 1; Else = 0. The length of time, in months, residing in the facility was also assessed.
Dependent Variables
Facility physical victimization
Youths were asked to report on their physical abuse experiences while living in the correctional facility. The question was posed, “Since you have been here, have you been beaten up or threatened with being beaten up?” The item was dichotomously measured (0 = No; 1 = Yes). Approximately 2,139 (30.2%) youths reported they had been physically victimized while in the facility.
Facility sexual victimization
Youths were asked to report on their sexual victimization experiences while living in the correctional facility. The question was posed, “Since you have been here, has anyone forced you to engage in sexual activity?” The item was dichotomously measured (0 = No; 1 = Yes). Approximately 297 (4.2%) youths reported having experienced sexual victimization.
Facility robbery
Youths were asked to report on their experiences being robbed while living in the correctional facility. The question was posed, “Since you have been here, have you had personal property stolen directly by force or threat?” The item was dichotomously measured (0 = No; 1 = Yes). Approximately 686 (9.7%) youths reported having experienced robbery.
Analyses
Two forms of analytic techniques and statistical software were used to analyze the data. To address the first hypothesis, two structural equational models were conducted using Mplus v. 7.4 (Muthén & Muthén, 2015). To address the second hypothesis, a series of regression models were run using Stata 13.1 (StataCorp, 2013). Complex survey methods were used to analyze the data, as two types of sampling weights were employed in all analyses. The final youth weight (FYWT) was used due to the complex sampling design in the SYRP survey, while the 74 replicate weights (R_FYWT1 to R_FYWT74) generated in the SYRP database were used in the variance estimation methods. Specifically, a balanced repeated replicate (BRR) variance estimator was used to generate standard errors used in the development of p values and confidence intervals. The BRR is variance estimation technique used with designs like the SYRP with two primary sampling units (facility and youth; McCarthy, 1966). It provides reasonable variance and standard error estimations that would otherwise be artificially inflated. In fact, the authors of the study (see Sedlack et al., 2012) require the use of survey weights for all analyses to account for nesting of youths within facilities and oversampling of females and Hispanic youths.
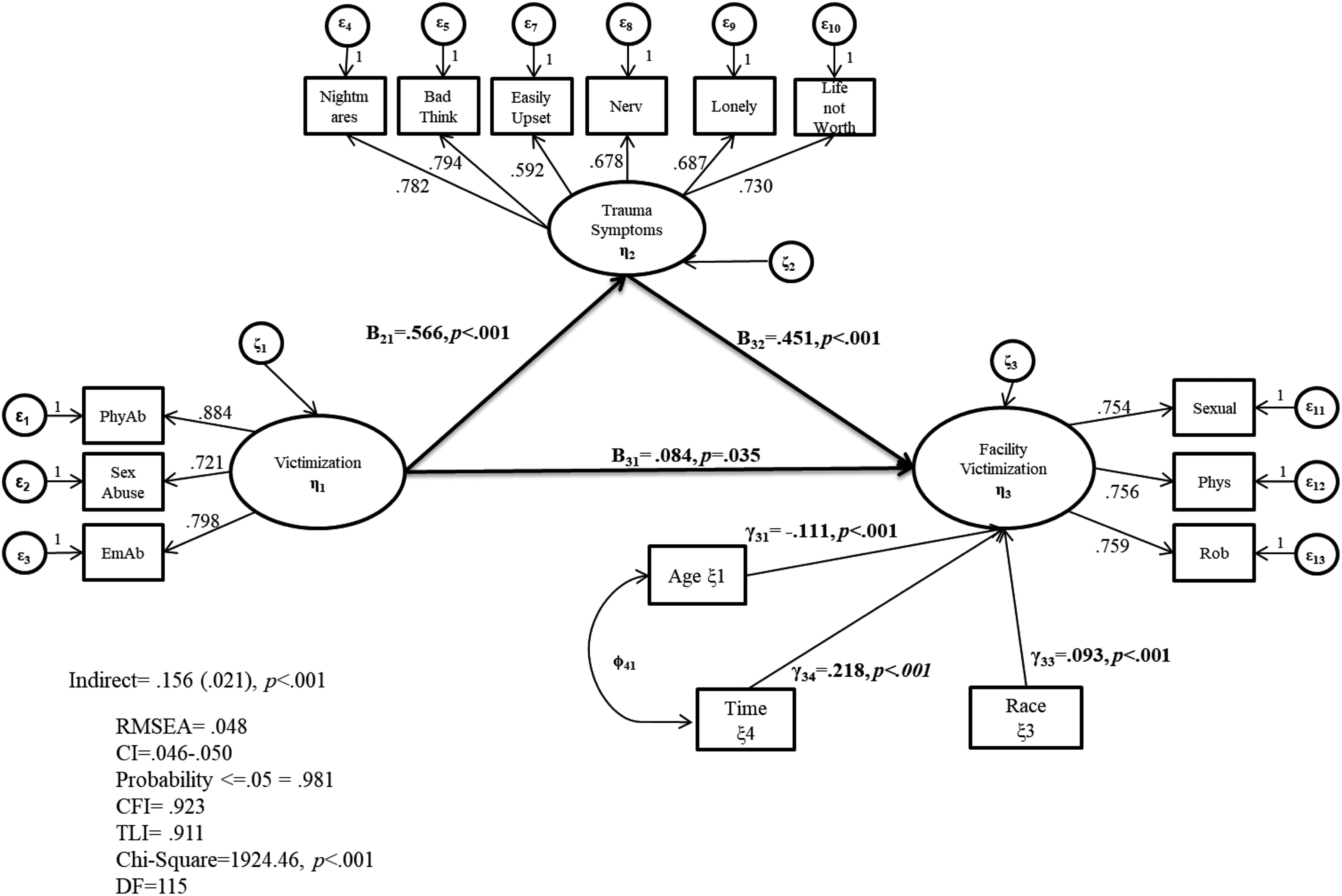
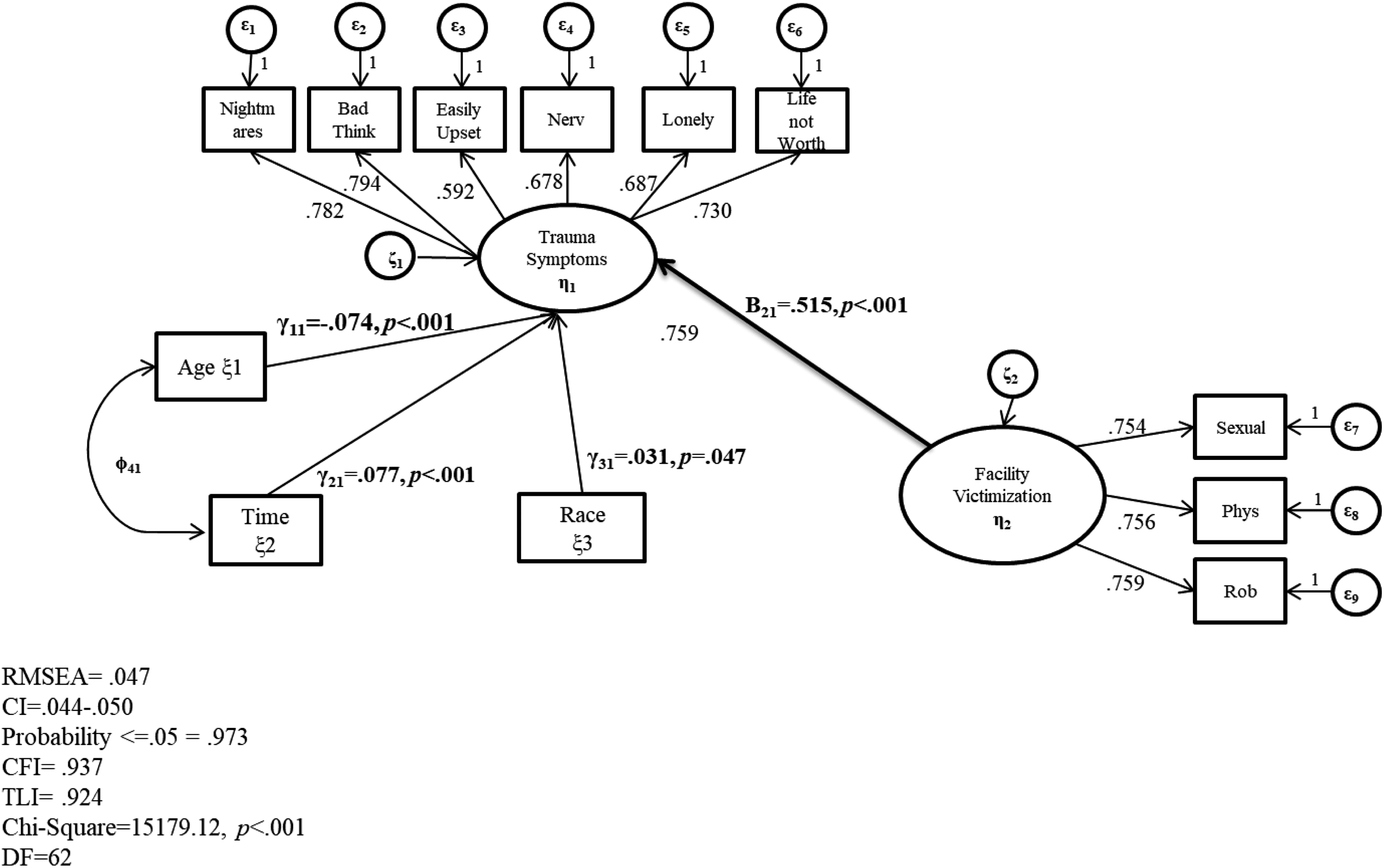
Structural equational modeling was used to address the first research hypothesis. This is a particularly informative approach to testing theoretically or literature-driven hypotheses (Bowen & Guo, 2012). Confirmatory factor analyses determined a good model fit by referencing the Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), root mean square error of approximation (RMSEA), and χ2 statistic (Bowen & Guo, 2012). The RMSEA (<.06) is typically the metric used to determine model fit (Hu & Bentler, 1999; Iacobucci, 2010), although the CFI and TLI are also used (<.95; Brown, 2006; Hu & Bentler, 1999; Iacobbuci, 2010). Given the weighted nature of the data, tests of model fit were run without weights, and then, the structural models were run with weights to report coefficients. This was done because the models will not report fit statistics with weights (Asparouhov & Muthen, 2010). The components of the fully specified model composed of latent factors and analogous observed variables with factor loadings are provided in Figures 1 and 2. In running the SEM models, a weighted least square estimation procedure (WLSMV) was used as it does not assume a normal distribution like the ML estimator; the variables included in the analyses are ordinal and dichotomous (Bollen, 1989). Mplus also uses a pairwise present strategy to retain all cases with at least one data point.
Victimization predicts facility victimization mediated by trauma symptoms.
Facility victimization associated with trauma.
In addition to running structural equation models to determine mediational and direct pathways, a series of regression models were also conducted in effort to parcel out the single and cumulative effects of early polyvictimization. The .i option was applied to the early forms of victimization variable in Stata. This restricts one category to report only the factor-variable settings for variables with an indicated base. For these analyses, the default or 0 was used; the default for factor variables without a declared base level is first. The models were run this way in effort to distinguish the predictive effect of each value relative to the base, to identify the overall pattern or distribution of each factor, and to classify the predictive effects as values increased. Such nuanced analyses can illuminate the cumulative properties of the respective factor values to distinguish the cumulative effects of more than one form of victimization.
To address the first hypothesis suggesting the relationship between amassed early victimization and facility victimization is partially mediated by trauma symptoms, but facility victimization also contributes to trauma symptoms, two separate structural equation models were employed. Using polyvictimization/victimization literature, we first determined the overall mediational effect of trauma symptoms on the relationship between early and facility victimization variables that are represented by latent factors. The second part of the hypothesis was tested in a separate model to isolate the impacts of facility victimization on trauma symptoms while controlling for demographic vulnerabilities contributing to trauma. Further, more nuanced analyses, tested the cumulative effect of early victimization on each facility victimization experience. To test the second hypothesis suggesting there is a cumulative risk effect of multiple forms of victimization during early life on robbery, sexual, and physical facility victimization, and trauma symptoms, three bivariate logistic regression models and one bivariate linear regression model were run, respectively. The third hypothesis that conjectures the relationship between cumulative early victimization and robbery, sexual, and physical facility victimization is partially mediated by trauma symptoms was answered in two steps: (1) three bivariate logistic regression models regressed facility robbery, physical, and sexual victimization on trauma symptoms and (2) three final multivariate logistic regression models regressed facility physical and sexual victimization on trauma symptoms, polyvictimization, and all other control variables. The coefficients were compared in each model to determine the relative effect of including trauma symptoms in the models. The results are organized around the hypotheses.
Results
Hypothesis 1: Mediational Model of Composite Victimization and Facility Victimization
Results from the first SEM model revealed a good fitting model, χ2(115) = 1,924.46, p < .001, CFI = .923, TLI = .911; RMSEA = .048; 95% CI [0.04, 0.05]. There was a statistically significant direct effect of the latent factor of early victimization experiences on the latent factor of facility victimization, β31 = .084 (.04), p = .035, and this relationship was partially mediated by trauma symptoms, as early victimization was associated with trauma symptoms, β21 = .566 (.02), p < .001, and trauma symptoms was associated with facility victimization, β32 = .451 (.03), p < .001. The results yielded a statistically significant indirect effect, β = .156 (.02), p < .001. Furthermore, there was a statistically significant (p < .001) amount of variance in the two endogenous variables explained by the model; polyvictimization explained 32.1% of the variance in trauma, and polyvictimization and trauma explained 30.9% of the variance in facility victimization. The full results of the SEM model are presented in Figure 1.
Results from the second SEM model revealed a good fitting model, χ2(62) = 15,179.12, p < .001, CFI = .937, TLI = .924; RMSEA = .047; 95% CI [0.04, 0.05]. There was a statistically significant direct effect between facility victimization and trauma, β21 = .515 (.02), p < .001. A statistically significant (p < .001) amount of variance in trauma was explained by facility victimization and the controls (27.4%). Younger youths (γ11 = −.074 (.02), p < .001), more time in the facility (γ21 = .077 (.02), p < .001), and having a White ethnicity, γ31 = .031 (.02), p = .047, were also vulnerabilities associated with trauma symptoms.
Hypothesis 2: Cumulative Polyvictimization and Facility Victimization and Trauma Symptoms
Physical victimization in the facility
Results revealed a statistically significant regression model, F(3, 71) = 4,930, p < .001. There was a statistically significant cumulative risk effect between one or more early victimization experiences and physical victimization in the facility. For example, youths who reported one form of early victimization (relative to no reports) were 1.76 times (p < .001) more likely to experience facility physical victimization; youths who reported two forms of early victimization were 2.08 times (p < .001) more likely to experience facility physical victimization; and youths who reported three forms of early victimization were 2.92 times (p < .001) more likely to experience facility physical victimization.
Sexual victimization in the facility
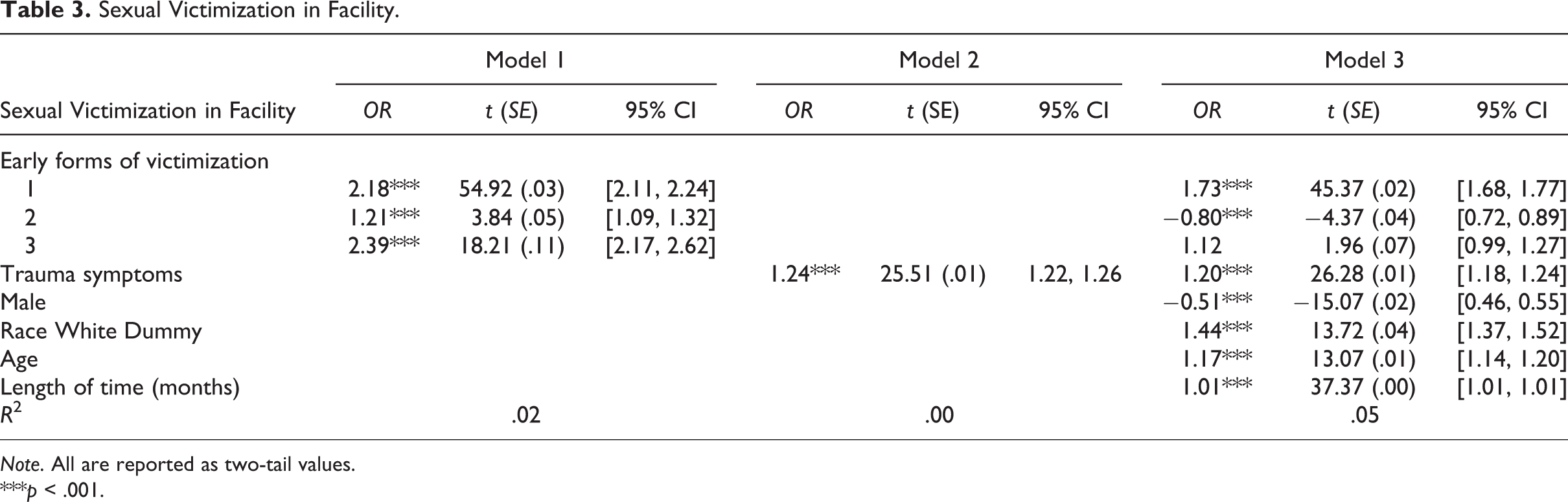
Results revealed a statistically significant regression model, F(3, 71) = 1,885, p < .001. There was a statistically significant direct effect between one or more early victimization experiences and sexual victimization in the facility, but the effect was not cumulative. For example, youths who reported one form (relative to no reports) of early victimization were 2.17 times (p < .001) more likely to experience facility sexual victimization; youths who reported two forms of early victimization were 1.21 times (p < .001) more likely to experience facility sexual victimization; and youths who reported three forms of early victimization were 2.28 times (p < .001) more likely to experience facility sexual victimization. So, the second early victimization experience had a smaller effect than one experience, but smaller than three experiences.
Robbery in the facility
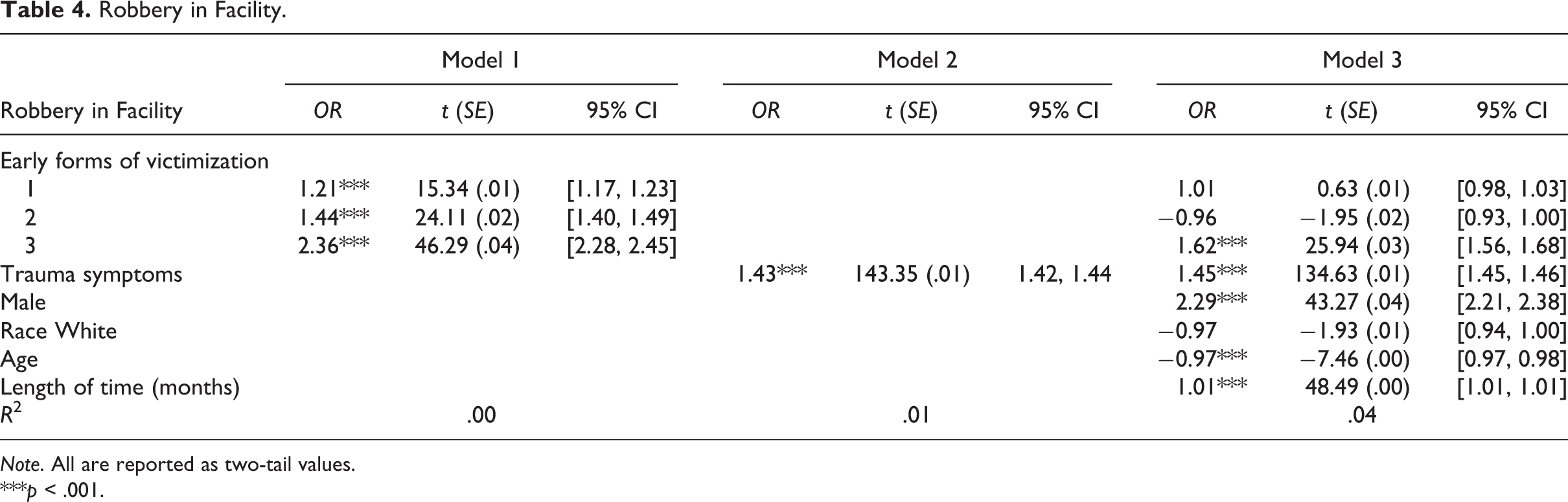
Results revealed a statistically significant regression model, F(3, 71) = 733.86, p < .001. There was a statistically significant cumulative direct effect between one or more early victimization experiences and experiencing robbery in the facility. For example, youths who reported one form of early victimization (relative to no reports) were 1.20 times (p < .001) more likely to experience facility robbery; youths who reported two forms of early victimization were 1.44 times (p < .001) more likely to experience facility robbery; and youths who reported three forms of early victimization were 2.36 times (p < .001) more likely to experience facility robbery.
Trauma symptoms
Results revealed a statistically significant regression model, F(3, 71) = 11,632, p < .001 with 13.33% of the variance explained. There was a statistically significant cumulative risk effect between one or more early victimization experiences and trauma symptoms. For example, youths who reported one form (relative to no reports) of early victimization were .72 times (p < .001) more likely to experience trauma; youths who reported two forms of early victimization were 1.34 times (p < .001) more likely to experience trauma symptoms; and youths who reported three forms of early victimization were 1.99 times (p < .001) more likely to experience trauma symptoms.
Hypothesis 3: Trauma as Mediator
Trauma and facility victimization
The results from the physical victimization model revealed a good model fit regressing facility physical victimization on trauma symptoms, F(1, 73) = 10,576.19, p < .001. Youths with trauma symptoms were 1.31 times (p < .001) more likely to be victimized physically in the correctional facility. The results from the sexual victimization model revealed a good model fit, F(1, 73) = 650.93, p < .001; youths with trauma symptoms were 1.24 times (p < .001) more likely to be victimized sexually in the correctional facility. The results from the robbery model revealed a good model fit F(1, 73) = 20,549, p < .001; youths with trauma symptoms were 1.43 times (p < .001) more likely to be robbed in the correctional facility.
Full multivariate model: physical victimization in facility
The results from the multivariate model, which regressed trauma, polyvictimization, and controls on physical victimization in the facility revealed a good model fit, F(8, 66) = 4,582.03, p < .001. Trauma symptoms were statistically significantly associated with physical victimization (odds ratio [OR] = 1.28, p < .001). There was a marginal cumulative polyvictimization effect, whereby one early victimization experience was linked to 1.50 times (p < .001) greater likelihood; two early victimization experiences were linked to a 1.50 times (p < .001) greater likelihood; and three early victimization experiences were linked to a 2.02 times (p < .001) greater likelihood for facility physical victimization. The results from all models revealed a partial mediating effect of trauma symptoms on the relationship between cumulative early victimization and facility physical victimization experiences. The results from the bivariate and full multivariate analyses with facility physical victimization as a dependent variable are presented in Table 2.
Physical Victimization in Facility.
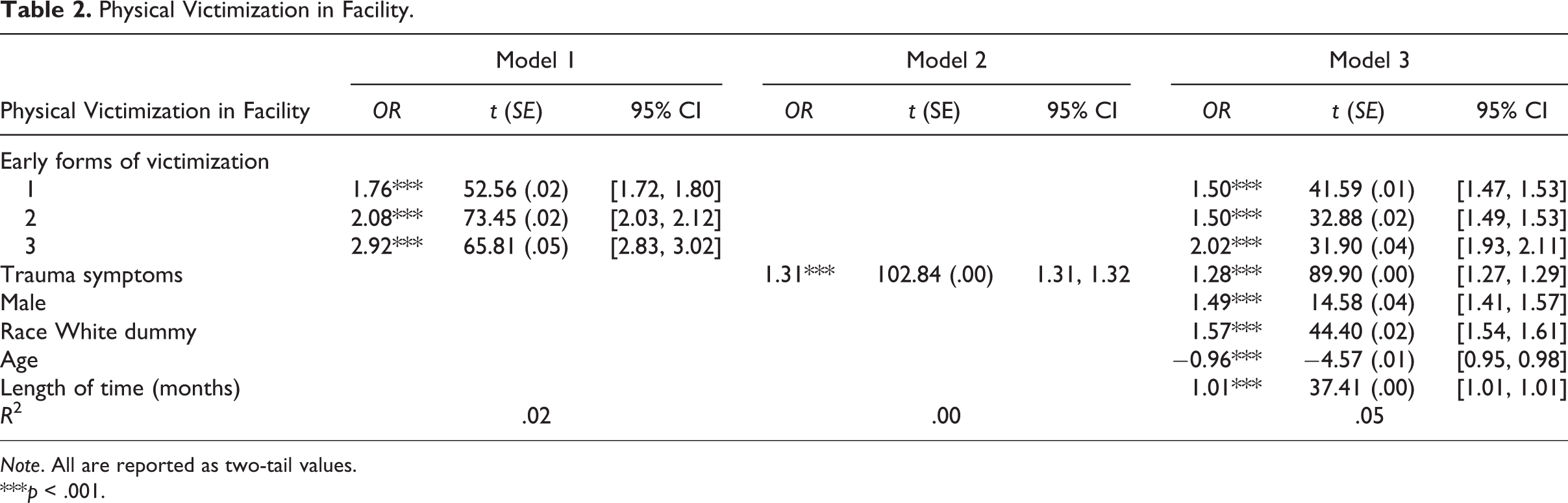
Note. All are reported as two-tail values.
***p < .001.
Full multivariate model: sexual victimization in facility
The results from the multivariate model, which regressed trauma, polyvictimization, and controls on sexual victimization in the facility revealed a good model fit, F(8, 66) = 2,745.68, p < .001. Trauma symptoms were statistically significantly associated with sexual victimization (OR = 1.20, p < .001). There was not a cumulative polyvictimization effect. In fact, one early victimization experience was linked to 1.73 times (p < .001) greater likelihood of sexual victimization, but two early victimization experiences were linked to a reduced likelihood for sexual victimization (OR = −.80, p < .001), and three early victimization experiences were not statistically significant associated with facility sexual victimization (OR = 1.12, p = .053). These findings, when compared with the earlier models, suggest that trauma symptoms fully mediate the relationship between two or more early victimization experiences and facility sexual victimization. The results from the bivariate and full multivariate analyses with facility sexual victimization as a dependent variable are presented in Table 3.
Sexual Victimization in Facility.
Note. All are reported as two-tail values.
***p < .001.
Full multivariate model: robbery in facility
The results from the final multivariate model, which regressed trauma, cumulative polyvictimization, and controls on robbery in the facility revealed a good model fit, F(8, 66) = 2,502.74, p < .001. Trauma symptoms were statistically significantly associated with robbery (OR = 1.45, p < .001). There was not a cumulative polyvictimization effect. In fact, one (OR = 1.00, p = .531) or two (OR = .96, p = .055) early victimization experience(s) was not statistically significantly associated with facility robbery; but youths with three early victimization experiences were 1.62 times more likely to experience facility robbery (p < .001). These findings when compared with the earlier models suggest that trauma symptoms fully mediate the relationship between one and two victimization experiences and robbery. The results from the bivariate and full multivariate analyses with facility robbery as a dependent variable are presented in Table 4.
Robbery in Facility.
Note. All are reported as two-tail values.
***p < .001.
Discussion
Effects of Early Composite and Cumulative Victimization
The findings revealed that overall, amassed and cumulative early victimization experiences were predictive of later facility victimization and trauma, alike. The structural equation model revealed direct effects between the collective early victimization experiences and combined facility victimization and trauma symptoms. As these results show how victimization experiences, in total, create amplified risk, it is becoming increasingly crucial to assess victimization through a fluid, multidimensional, and transformational lens. Victimization studies rarely profile victimization incidents in an exhaustive way and often explore a one-time only or single act (Finkelhor et al., 2007a). Further, there are complex effects resulting from polyvictimization (and often single victimization) experiences (Ford, 2011). Polyvictimization is undoubtedly multifaceted, as the reasons, motivations, and severity of the abuse can change during each event (Finkelhor et al., 2007a; Turner et al., 2010). Certainly, these experiences can cause elevated distress and pervasive functional difficulties that ebb and flow through the life course (Briere, Kaltman, & Green, 2008; Cloitre et al., 2009; Cyr, Marie-Eve, & Chamberland, 2014; Dong et al., 2004; Ford et al., 2009). Therefore, studying the impact of multiple victimization experiences can lead to greater specificity in discerning youths’ developmental pathways.
Analytical results in greater detail revealed a critical bivariate pattern, whereby each form of early victimization successively increased the likelihood for institutional physical victimization, robbery, and trauma symptoms. Although a similar pattern was not evident for facility sexual victimization, youths who reported three early victimization experiences, relative to no experiences, had almost a 2½ times greater likelihood for facility sexual victimization. These findings suggest that polyvictimization can unequivocally impact youths development (Finkelhor et al., 2007a). Multiple forms of victimization may not only create propensities toward delinquency, but also generate vulnerabilities to experience repeat victimization in the juvenile justice system. In fact, research has pointed to this phenomenon of revictimization among polyvictimized youths (Finkelhor et al., 2007b); polyvictims have also been found to experience victimization in multiple settings by multiple perpetrators (Turner et al., 2016), and research on juvenile justice polyvictimized youths reports similar findings (Butcher, Holmes, Kretschmar, & Flannery, 2016).
Overall, the bivariate models showed that three forms of victimization had the strongest effects. Violent forms of early victimization can be argued to be more severe in nature, as one’s body and mind endure greater stress rather than manipulation of one’s safety or boundaries commonplace in nonviolent forms of victimization (Card, Stucky, Sawalani, & Little, 2008). Findings regarding differential associations between early forms of victimization and trauma symptoms have been supported by longitudinal research that tested the psychological distress of disparate forms of violence (Norris & Kaniasty, 1994). Findings from Norris and Kaniasty (1994) showed that victims of violent crimes (relative to nonviolent crimes) maintained the highest level of distress 15 months later (Norris & Kaniasty, 1994). However, some scholars have argued for weighing forms of victimization to determine the comparative impact of each victimization form due to the heterogeneous and relative nature of the experiences (Scott-Storey, 2011). Nevertheless, in an environment where individuals are prone to various forms of revictimization, effects of severe early polyvictimization and trauma symptoms may appear to persist due to lengthened recovery times (Burgess & Holmstron, 1978; Norris & Kaniasty, 1994). In other words, youths may not have fully recovered from a prior victimization experience before they are incarcerated, likely compounding their distress and hyperarousal during more severe experiences of victimization.
Trauma as a Mediator
The results from this study revealed that trauma symptoms were particularly important in understanding how youths experience repeat victimization. Trauma either partially or fully mediated the relationships between early forms of composite or cumulative victimization and later facility victimization. Polyvictimization experiences can indeed influence trauma symptomatology as significant neurological impairments have been identified among youths with multiple victimizations (Perry et al., 1995). Abuses, particularly those experienced in greater doses, are associated with neural response deficiencies (Perry et al., 1995). Extreme or frequent abuse during “critical periods” of development can disrupt the central nervous system, resulting in neuronal activity abnormalities (Perry et al., 1995, p. 276). Such impairments greatly influence the degree to which individuals, particularly young individuals undergoing neurological development (occurring sequentially from back to front), can adaptively function. Experiences that transpire at a young age can delay or discontinue neurological development all together (Perry et al., 1995). Consequently, multiple forms victimization can “sensitize” youths (Perry et al., 1995, p. 278). Repetitive abuse triggers certain physiological, psychological, and behavioral responses. The young person subsequently adapts similar reactions when reminded of the event or in contexts (some benign) they perceive as fearful (Perry et al., 1995). This can be referred to as a “persisting fear state” (Perry et al., 1995, p. 278). These are conditions that are reflective of trauma symptoms.
The findings from this study support earlier research that reveals how polyvictimized youths have significant trauma symptoms (Finkelhor, Ormrod, & Turner, 2007c; Turner et al., 2016) but also reveals that trauma symptoms can help explain the impact of early polyvictimization on revictimization (Cuevas et al., 2010; Finkelhor et al., 2007a). Individuals who are victimized multiple times can have psychological states that fluctuate between hyperarousal and dissociation (Perry et al., 1995). So, while fear states become internal working models, trauma symptoms can manifest quite distinctively. Research reveals how only 70% of youths with severe trauma histories and marked hyperarousal symptoms meet criteria for post-traumatic stress disorder (Perry, 1995). As such, formal trauma symptoms may be only manifest under certain conditions. Undoubtedly, trauma symptoms can become discernable in the incarceration setting and can generate additional vulnerabilities toward facility victimization.
This article yielded findings that suggested that facility victimization also contributes to trauma symptoms. This is consistent with other studies that explored the relationship between harsh staff responses to youths and trauma symptomatology (Hodge & Yoder, 2017), suggesting that correctional facilities, in part, contribute to or exacerbate trauma symptoms. Additional research ought to explore exactly how early life trauma symptoms are intensified by facility experiences or what specific facility-level variables account for this association (e.g., punitive nature of facility culture), particularly as this study revealed significant reciprocal relationships between trauma symptoms and facility victimization. Furthermore, there may be other contextual or individual vulnerabilities that contribute to original victimization or repeated victimization. We partially accounted for this by testing age, race, and time in facility. However, extant research indicates that there are inherent or external vulnerabilities such as poverty, race, age, parental/caregiver stability, and surrounding neighborhood and community that put children and youths at risk of initial victimization (Dong et al., 2004; Odgers & Jaffee, 2013). These factors should be studied in greater detail among juvenile justice populations to glean greater specificity in developmental pathways to youth victimization and violence.
For incarcerated youths, polyvictimization can contribute to or explain delinquency through an internalization process; polyvictimized youths may experience a survival mode temperament when they are exposed to reminders of the event (e.g., in similar conditions or contexts). For example, youths with early polyvictimization, compared to youths witnessing violence, have been shown to be more delinquent (Ford, Connor, & Hawke, 2009) and present a host of other problematic profiles including family disconnectedness, trauma symptoms, community violence, or chaos (Turner et al., 2016). Nevertheless, we may need to look beyond the reflexive capacities of polyvictimization experiences as they explain offending and instead consider how polyvictimization fundamentally alters psychological, emotional, and physical responses. Perhaps such early adverse experiences shape youths as both “offenders” and recurring victims. While the theoretical cycle of violence is a well-established framework underlying the development of delinquent behaviors (Widom, 1989), conceivably this study contributes to a larger emergent phenomenon reflecting a “cycle of violence and recurring victimization.” A locked confinement setting certainly encompasses omnipresent reminders of early victimization experiences and may lead to expression of trauma symptoms. These reminders may trigger early victimization cues and similar neurological response strategies that put the youths at greater risk of analogous victimization.
Implications
The results from this study suggest universally adopting a new juvenile justice response model. The established link between trauma and offending necessitates early response to trauma and victimization to circumvent involvement with the juvenile justice system. Prevention efforts, in this regard, include system integration, particularly within child welfare, health and mental health, and substance use agencies. For example, child welfare primary prevention programs like “Triple P” or “Positive Parenting Program” uncover and target parental and environmental risk and protective factors and tailor service provision to assist parents with child-rearing (Daro & Dodget, 2009; Sanders, 2008). Services are delivered according to the level of need identified by caregivers, and it has been shown to be effective in improving parenting (Sanders, 2008).
As many states are moving away from incarceration as a “catch-all” approach, partially in effort to be more fiscally responsible (Cooley, 2011; Welsh, Loeber, Stevens, Cohen, & Farrington, 2008), community-based care alternatives are taking shape (Cooley, 2011; Lipsey, 2006). As part of a strategy to substantively decrease juvenile incarceration rates, juvenile justice leaders are drawing from the risk principle embedded in the risk need responsivity (RNR) model (see Andrews, Bonta, & Hoge, 1990) that advises matching level of care to level of risk. This approach can be helpful in minimizing low risk offenders’ exposure to overly punitive or harsh responses (Lowenkamp & Latessa, 2005; Lowenkamp, Latessa, & Holsinger, 2006), subsequently lessening probability for iatrogenic effects (Gatti, Tremblay, & Vitaro, 2009; Lipsey, 2006).
This shift has transformed the juvenile justice culture in many states, but numerous residual concerns remain. For one, enhanced risk assessment tools can be helpful in screening risk levels and developing suitable responses (Hanson, 2005). National and statewide risk assessment tools have been designed and validated to capture evidenced based criminogenic needs or dynamic risks linked to the commission of crimes (see Latessa, Lovins, & Ostrowski, 2009). Nevertheless, the tools do not comprehensively address all domains (Taxman & Caudy, 2015) and certainly are not entirely inclusive of early life victimization or associated symptoms. Although victimization is not listed as a top eight criminogenic need in the RNR model (Andrews & Bonta, 2010), with more research emerging regarding the relative effect of victimization on initial and re-offense (Ford et al., 2006, 2007; Kerig, 2012), risk assessments can be reconceptualized to comprise aspects of victimization (static) and associated symptoms (dynamic) in assessing risk of victimization or offending.
Community-based care should be used in all relevant, appropriate, and applicable circumstances, while upholding the highest public safety and security standards (Coates, 1981; Cooley, 2011; Fagan, 2013). Also, increased dosage is being introduced as a treatment response to high-risk offenders (Makarios, Sperber, & Latessa, 2014). Like health sectors, proper dosage of treatment may guide for the future of incarceration programming (Makarios et al., 2014). Finally, this movement will only be effective if community-based and facility-based rehabilitative programs are developed, tested, and implemented with thoughtful consideration of risk factors, specifically trauma.
Programs can begin adapting a care-based model in and around trauma and victimization. This study reveals several disconcerting findings that suggest perhaps services for juvenile justice involved youths can be altered. First and foremost, incarceration settings for juveniles may always be necessary, particularly for those with the highest risk (Mulvey, Schubert, & Odgers, 2010). In effort to move away from punitive models of care, staff and facility-level transformations are necessary. Intervention components and organizational development can be two strategies to achieve change (Mulvey et al., 2010). Specifically, ongoing staff trainings are needed that attend to the precarious trauma-based risk factors of youths. It may be useful to augment facility climates by drawing upon the constructive capacities and entirely overhauling policies supporting environments that are overly restrictive, controlling, or abusive (Mulvey et al., 2010).
Moreover, alongside risk assessment tools, trauma, and polyvictimization screening is necessary. Such screening ought to identify risk of, symptoms of, and exposure to any and all trauma and victimization experiences. Screening tools can effectively classify youths who are at risk of ongoing psychological, behavioral, or other functional difficulties associated with these experiences. Trauma-screening tools ought to provide direct links to services addressing enduring external or internal struggles.
Finally, for identified youths, whether they are housed in incarceration settings or positioned in the community, all programs ought to implement evidence-based—or at the very least evidenced-informed—trauma services. The importance of trauma services was emphasized in a recent peer-reviewed OJJDP-sponsored journal focusing on the criticality of trauma-informed care. In one article, Olafson, Goldman, and Gonzalez (2016) discuss the importance of collaborative treatment efforts across various child and family services organizations for youths who have experienced traumatic events. The authors further highlight tools to support these collaborations that have shown positive outcomes in the rehabilitation of traumatized youths, such as cross-system specialized trauma training and early identification assessments. A subsequent article by Ford, Kerig, Desai, and Feierman (2016) provides a review of trauma-focused psychosocial interventions for youths involved with the juvenile justice system and the growing evidence base that supports the effectiveness of these services. There are also evidence-based trauma-informed models that unambiguously target brain plasticity or malleable zones susceptible to change (Perry, 2009). Other evidence-based practices attend to the ongoing behavioral disruptions associated with trauma or victimization experiences (Lawson & Quinn, 2013). No matter the model, programs ought to be educated on trauma and victimization as a significant risk factor, and develop and implement appropriate services.
Limitations
The variables in these models are derived from cross-sectional survey data. The data set is observed from a subset of a population. An experimental design was not used, and the data are cross-sectional. As such, findings from this study do not imply causation; rather, they reflect an association between the items and the dependent variables. Experiences in the facility could also contribute to youths reports. Further, the authors of this manuscript did not have direct responsibility or a personal investment in the collection or organization of this data set. Similar to limitations of prior work (Finkelhor et al., 2007a; Ford et al., 2013; Turner et al., 2010), indicators for early life victimization, trauma, and overall incarceration experience were derived from self-report information that may be biased or flawed in reporting or substantiation, particularly due to the responses that offered boundless time options (e.g., anytime growing up or any time since being in the facility) within the questions. Assumptions, including the need for independent and identically distributed observations, are easily violated by survey data. Through specification of sampling weights and a BRR variance estimator used to estimate standard errors, this study accounted for such limitations. Further, there may be additional factors not accounted for in these models. Despite attempts to be robust in assessing independent and dependent variables of victimization, the researchers were bound to the variables available in the data set. The operationalization of the variables may have some limitations and was reconciled using model fit testing. Nevertheless, it should be noted that this study may have operationalized polyvictimization incompletely. Additional measures ought to refine this concept and include other forms of victimization including, but not limited to exposure to domestic violence, gun violence or threats, sexual exploitation or prostitution, or emotional or physical neglect.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.