
Abstract
Adverse childhood experiences (ACEs) have long been recognized for negatively influencing individual outcomes such that each additional ACE exposure increases the risk for negative health and behavioral outcomes. Little is known, however, about how the more recent accumulation of ACEs occurring in follow-up periods influence global functioning considering the past accumulation of ACEs reported at baseline by justice-involved adolescents. Participants were 851 adolescents who completed the Northwestern Juvenile Project (NJP), a longitudinal survey. OLS regression models were used to examine the influence of follow-up and baseline ACEs on the functional impairment of youth. Results indicate that both follow-up and baseline ACEs were associated with worse functioning over time with baseline ACEs demonstrating a greater effect. This study highlights the importance of assessing accumulations of ACEs over time for adolescents in the juvenile justice system and considering how youth of different characteristics and experiences may differently encounter functional impairment. Implications for offering trauma-informed services to disrupt the effects of adversity on adolescents’ functioning are discussed.
Exposure to traumatic adversities among justice-involved youth is high (Abram et al., 2004; Charak et al., 2018; Ford et al., 2013). In a recent study of lifetime exposure to adversities, nearly 93% of justice-involved youth reported experiencing four or more types of adversity (Charak et al., 2018). Many of these adversities include personal experiences of maltreatment or family experiences of difficulty. The adverse childhood experiences (ACEs) study is well-known for establishing the measurement of childhood adversities that reflect an individual’s prior experience in 10 key areas; these areas include abuse (physical, sexual, and emotional), neglect (physical and emotional), and household dysfunction (mother who experienced domestic violence, parental abandonment, household member who experienced substance abuse, mental illness or incarceration) during the first 18 years of life (Anda et al., 1999). Conceptualized as a cumulative risk model, higher ACE scores denote higher levels of adversity with previous research indicating that greater exposure to ACEs early in life is associated with greater risk of mortality, many forms of morbidity, mental health difficulties, and behavioral health problems over the life course (Felitti et al., 1998; Gilbert et al., 2010; Kessler, et al., 2010; Timmermans et al., 2010). While it is widely recognized that each additional ACE increases personal risk (Flaherty et al., 2013; Grasso et al., 2016; Wolff et al., 2017), the influence of early and later accumulations of risk on overall functioning has not been well documented among justice-involved adolescents. This paper examines the cumulative effect of follow-up ACEs (ACEs accumulated during the course of the study and later in the adolescent’s life) and baseline ACEs (ACEs accumulated prior to the study and earlier in the adolescent’s life) among a sample of justice-involved youth to discover how more recent ACEs and past ACEs influence global functioning. Global functioning, related to functional impairment, is measured in this study by an overall assessment of the presence of symptoms that disturbs personal and social well-being.
Cumulative Adversities: A Strain on Development
Much of the ACEs research has considered how cumulative stressful or traumatic events in childhood are significant risk factors for unhealthy development from childhood to adulthood. Robust findings have indicated that multiple relative to single risk exposures have worse developmental consequences (Gutman & Flouri, 2017; Rutter, 1979, 1981; Sameroff, 2006; Sameroff et al., 2004). This is particularly concerning for justice-involved youth who experience greater rates of trauma exposures than youth in the community (Dierkhising et al., 2013). In a previous study of youth involved in the Northwestern Juvenile Project (NJP), youth reported an average of 14.6 traumas with 93% of detained youth reporting at least one trauma and 84% reporting more than one trauma (Abram et al., 2004). These high rates of adverse exposure are related to poor personal outcomes, including higher rates of post-traumatic stress disorder (PTSD) that exceed the lifetime estimates of PTSD in community samples (Abram et al., 2004). Justice involved youth with high trauma exposure experience brain and personality disruptions that interfere with self-regulation (Ford et al., 2007) and many internalizing (Finkelhor et al., 2011) and externalizing problems (Dierkhising et al., 2013). Furthermore, research indicates that childhood adversities are associated with an increased likelihood of offending behavior (Teague et al., 2008) and reoffending behavior (Wolff et al, 2017). The association of childhood adversities to delinquency and recidivism has implications for how juvenile justice systems engage with youth (Baglivio et al., 2015; Barrett et al., 2014).
Research has also found that risks for symptomatic outcomes may vary based on the age when traumas are experienced (Schoedl et al., 2010). Studies related to timing of adversities or sensitive periods of exposure have produced mixed results. A recent study focusing on accumulation, timing, and duration found that intermittent adversity had the strongest relationship to later childhood behavior problems (Schroeder et al., 2020). Contrarily, in a study examining DNA methylation—an epigenetic mechanism—adverse exposures before 3 years of age produced the most variability in altering gene expression (Dunn et al., 2019). Bosch et al. (2012) similarly found that pre and postnatal adversities had the strongest effects when considering timing from the prenatal period to middle adolescence. Overall, adversities during middle childhood throughout adolescence were associated with irregular cortisol levels indicating that adolescence is a sensitive time for stressful events (Bosch et al., 2012). Dierkhising et al. (2013) found that more than half of the justice-involved youth participants in their sample experienced initial traumas in the first 5 years of life with ongoing exposures occurring each year into adolescence. Collectively these findings suggest that impairments to global functioning may be different for youth at different ages of exposure. Further, because adolescence is a period of significant developments in cognitive, biological, and psychological abilities, it is possible that adversities experienced by youth at later ages are differently associated with functional impairments than earlier adversities.
Ongoing Risk for ACE Accumulation
Research has found that children who have endured any trauma exposure are at increased risk of additional or chronic trauma exposures (Dierkhising et al., 2013; Finkelhor et al., 2007a; Finkelhor et al., 2007b). This potential for ongoing risk to adversity over the life course suggests that a recency effect might influence well-being. The recency model suggests that current mental health functioning is most strongly associated with concurrent risks rather than antecedent risks (Shanahan et al., 2011). The exploration of the effects of distant and more recent adverse accumulations in relation to the overall functioning of youth interacting with justice systems has been largely absent from the literature. However, research relating to developmental timing and co-occurrence of multiple adversities signals that the examination of ACE exposures relative to timing may be an important area of study.
Research on current versus past poly-victimization and mental health has found that for younger children lifetime victimization prior to the most recent year influenced current trauma symptoms, while for older children prior victimizations did not influence current trauma symptoms, but present year victimizations did (Finkelhor et al., 2007a). Other research has found that the timing and chronicity of maltreatment influences outcomes such that maltreatment occurring in adolescence only and persistent maltreatment from childhood through adolescence was related to delinquency when childhood-only maltreatment was not (Stewart et al., 2008; Thornberry et al., 2002). Further, research examining the developmental timing of trauma from infancy through puberty and psychopathology outcomes among girls found that risk for depression was associated with trauma experienced during grade school, risk for anxiety was associated with trauma experienced during puberty, and risk for PTSD increased with the recency of exposure (Marshall, 2016). Such variations in the effects of trauma suggest that the timing of adversities encountered from childhood through adolescence influence particular personal outcomes (Marshall, 2016). Given the influence of adversity and trauma on psychopathology and overall functioning based on timing of exposures, research is needed to explore how more recent adversities occurring in follow-up periods of adolescence influence global functioning and how historical adversities occurring before baseline may affect this relationship.
ACEs and Functional Impairment
Numerous studies indicate that stressful and traumatic events, especially multiple exposures, are associated with lower levels of global functioning or functional impairment, with children and adolescents with histories of trauma and adversity susceptible to engaging in interpersonal violence and experiencing challenges in social, family, and academic functioning (D’Andrea et al., 2012; Duke et al., 2010; Kiesel et al., 2016). Notably, justice-involved youth are more likely than their peers to exhibit impaired functioning (Abram et al., 2008; Teplin et al., 2002). Measuring such functional impairment serves several key purposes. Combined with an evaluation of the presence of specific psychiatric symptoms, assessing functional impairment is important to the diagnosis of mental health disorders (Bird, 1999; Winters et al., 2005). A bidirectional relationship exists whereby symptoms can influence impairment and impairment can influence symptoms (McKnight & Kashdan, 2009), thereby requiring the assessment of both psychiatric diagnoses and functioning in order to completely assess mental health status. With this framework in mind, it is important to consider how an association between ACEs and impaired functioning may be experienced differently for those with a psychiatric diagnosis. Research indicates that justice-involved youth have high rates of mental health disorders, including substance abuse (Dierkhising et al., 2013; National Center on Addiction and Substance Abuse, 2004; Schufelt & Cocozza, 2006). In a previous study of youth in the NJP study, more than 1 in 6 detained youth had a major mental disorder (Teplin et al., 2005). Thus, the current study considers the potential moderating effect of psychiatric diagnosis on the relationship between ACEs and impaired functioning.
Furthermore, given the high number of ACEs experienced by this justice-involved sample, recognizing the relationship between baseline and follow-up ACEs and functional impairment has implications for the assessment and treatment of psychiatric disorders. Functional impairment scores have been used to measure mental health treatment effectiveness (Winters et al., 2005) by indicating changes in dysfunction particular to social and psychiatric functioning. Further, retrospective assessments of the cumulative ACEs experienced over an individual’s first 18 years do not consider how ongoing or new prospective accumulations of ACEs during these formative adolescent years affect current levels of functioning. This research seeks to address this gap by examining how accumulations of ACEs at two different times influences the global functioning among justice-involved adolescents.
Current Study
The current study examined the association between cumulative ACEs and global functional impairment, as measured by the Children’s Global Assessment Scale (CGAS) (Shaffer et al., 1983 to explore how baseline ACEs and follow-up ACEs influence level of functioning. Unlike multidimensional scales which consider functioning in specific areas, CGAS is a unidimensional scale through which raters synthesize a youth’s social, school, and family functioning into a single global functioning score (Bird, 1999; Bird et al., 1987; Shaffer et al., 1983). As a unidimensional measure, CGAS is more sensitive to change than multidimensional scales, and thus, well-suited to considering differences in levels of functioning after intervention and over time (Bird et al., 1987; Bird et al., 1990; Bird, 1999; Shaffer et al., 1983).
Method
Data
The sample for this study is drawn from the Northwest Juvenile Project (NJP), a longitudinal study of 1,829 adolescents who were arrested and detained in Cook County, IL between 1995 and 1998 (see Teplin et al., 2013 for a description of the study). The NJP examined long-term outcomes, particularly mental health needs and service use, after youth left detention. Given the longitudinal nature of this dataset and sampling strategy, this was an ideal source of data for examining the nature of cumulative trauma and functional impairment among a juvenile justice population. A stratified random sample of adolescents were recruited at baseline, ranging in age from 10-18 years old. The sample was stratified by key areas, including sex, race/ethnicity (Black, non-Latinx White, Latinx), age (10–13 years or 14 and older), and legal status (processed as a juvenile or as an adult), in order to ensure sufficient recruitment in these areas. Youth who were 10–13 years old and youth who were transferred to adult court were oversampled. In Waves 2 and 3 of the study, 3.5 and 4-year follow-ups, only a random subsample of participants was included (n = 996). The sample in the current study was further limited to youth who ranged in age from 12 to 17 years of age, had provided responses to ACE items across all waves, had functional impairment scores at baseline and follow-up 4, 4.5 years later, and had complete data for race/ethnicity, age, and psychiatric diagnosis (n = 851).
Measures
Global functioning
Global functioning is measured through an assessment of functional impairment as defined in the clinical rating of an individual’s social (home, school, and peers) and psychiatric functioning that indicates severity of disturbance (Shaffer et al., 1983). The interviewer uses the CGAS to summarize their impression of the lowest level of functioning observed by the clinician based on information gathered about how things are going at home, in school, or other social environments (Shaffer et al., 1983). The CGAS is a widely-used measure of functional impairment demonstrating good reliability and validity (Schorre & Vandvik, 2004). Scores range from 1 to 100, with a score of 1 indicating the most severe level of impairment (Bird, 1999; Shaffer et al., 1983; Teplin et al., 2005; Winters et al., 2005). The scale is split into decile categories, with each decile containing a description of the levels of functioning corresponding with a rating in that range (Bird, 1999; Shaffer et al., 1983; Winters et al., 2005). CGAS scores were reverse-categorized from 1-10, such that 1 corresponded with scores ranging from 91-100 indicating superior functioning in all areas (less impairment) and 10 corresponded with scores ranging from 1-19 indicating a need for constant supervision (more impairment). For example, “needs constant supervision (24-hour care) - 10” refers to a level of impairment “due to severely aggressive or self-destructive behavior or gross impairment in reality testing, communication, cognition, affect, or personal hygiene” while a mid-range score of 5 or 6 indicates “moderate interference in most social areas/severe impairment of functioning in one area” (5) or “variable functioning with sporadic difficulties/symptoms in several but not all social areas” (6) (Shaffer et al., 1983). As measured in the NJP study, CGAS scores at baseline reflect the lowest level of functioning in the previous 6 months and scores at follow-up reflect the lowest level of functioning in the previous 3 months. CGAS scores at follow-up 4 were used as the dependent variable.
Adversities
Adversities are defined as adverse childhood experiences including child maltreatment and household dysfunction (Felitti et al., 1998). Composite scores were created based on the ACE study (Felitti et al., 1998) by summing dichotomized yes/no responses to NJP questions that asked about childhood maltreatment and household dysfunction. Of the 10 typical adversities assessed in the original ACEs study, 7 were included in the NJP questionnaires. These items were drawn from the Child Maltreatment Assessment Profile which was based on the Child Maltreatment Interview Schedule (Briere, 1992) and the Child and Family Assessment developed by the NJP study to assess risk and protective factors that included family functioning. An example of one item that was collected to reflect physical abuse includes the baseline question, “How many times in your whole life have you been hit very hard?” and the follow-up modified question, “How many times since the last interview have you been hit very hard?” The 7 ACEs included in this this study are emotional abuse, physical abuse, sexual abuse, intimate partner violence toward the child’s mother, household substance abuse, household mental illness, and household incarceration. The first composite score reflected ACEs reported at baseline, representing lifetime experiences of accumulated adversity, hereafter referred to as baseline ACEs. The second composite score reflected ACEs reported from follow-ups 1–4, representing new incidents or more recent experiences of accumulated adversity, hereafter referred to as follow-up ACEs. At each follow-up, participants were asked to report “since the last interview” any new incidents of particular experiences. These ACEs were counted as new reports of abuse or household dysfunction, with follow-up scores ranging from 0 to 7. These scores served as predictors and were treated as continuous measures where higher scores indicate a higher number of adversities.
Psychiatric diagnosis
Psychiatric diagnosis is defined as the presence of symptoms related to Diagnostic and Statistical Manual - IV (DSM-IV) diagnoses. Analyses considered the presence of a recent psychiatric diagnosis as a critical indicator of functional impairment that was initially controlled and then examined as a moderator. The Diagnostic Interview Schedule for Children, versions 2.3 and 4.0 (DISC 2.3 and DISC 4), were used to measure mental disorders (Shaffer et al., 2000) and the Diagnostic Interview Schedule, version 4.0., was used to measure substance disorders (DIS-IV; Robins et al., 2000). DISC 2.3 was administered at baseline. DISC 4 and DIS-IV were administered in follow-up assessments 1 through 4, reflecting the revised DSM-IV (American Psychiatric Association, 1994) and ICD-10 (World Health Organization, 1993). Both DISC and DIS-IV versions assess the presence of DSM disorders with acceptable reliability and validity (Compton & Cottler, 2004; Shaffer et al., 2004). DISC items examine the presence of symptoms up to a span of 12 months. Two categorical variables for psychiatric diagnosis, one for reports at baseline and one for reports at follow-up 4, were created to reflect a positive screening (dichotomous ratings, 0/1, that indicate absent/present or negative/positive) for any of the following disorders: affective (major depression, mania, hypomania), anxiety (generalized anxiety, panic, post-traumatic stress), behavior (conduct, attention-deficit/hyperactivity, oppositional), psychosis (schizophrenia), and substance use disorders (alcohol, marijuana, amphetamine, sedative, cocaine, opiate, PCP, hallucinogen, inhalant abuse/dependence).
Incarceration
Incarceration is defined as confinement in the past 3 months related to violations of the law as assessed using the Child and Adolescent Functional Impairment Scale (Hodges, 1990). In order to control for the active consequences of ongoing justice-involvement that could influence functional impairment, incarceration at follow-up 4 was included as a categorical variable (yes/no).
Sociodemographic characteristics
Sex and race and ethnicity were controlled in the analyses. Race and ethnicity were dummy coded to reflect the categories of Black, non-Latinx White, and Latinx. Age was included as a continuous variable.
Analytic Strategy
Due to the oversampling strategy used for sample recruitment, sample weights were used based on the Cook County Juvenile Temporary Detention Center population to estimate descriptive statistics and model parameters (Korn & Gubbard, 1999; Teplin et al., 2013). Weighted analyses were conducted using Stata, version 14 (StataCorp. 2015). Bivariate correlations were conducted to determine the association between variables included in this study. Ordinal Least Square (OLS) regression was used to determine the relationship between risk and functional impairment. All assumptions were checked and found to be satisfactory. CGAS scores were used as a continuous variable, collapsed from the 1–100 point scores, with observation of normal distribution. Three OLS regressions were estimated. The first model included follow-up accumulation, ACE scores reported from follow-ups 1-4, along with controls for sociodemographic characteristics consisting of age, gender, and race and ethnicity. The second model included the addition of ACEs reported at baseline. The third model included the addition of controlled variables for functional impairment reported at baseline (CGAS), psychiatric diagnosis at baseline, psychiatric diagnosis at follow-up 4, and incarceration at follow-up 4. Interaction terms were also examined to determine if the effects of baseline ACEs on functional impairment was moderated by psychiatric diagnosis.
Results
Sample Description
Descriptive characteristics are presented in Table 1. The majority of the sample was male (90%), Black (75%), and was an average age of 14.83 years old (SD = 1.32) at entrance into the study. Accumulations of childhood adversity reported at baseline ranged from 0 to 7, with an average of 2.15 experiences (SD = 1.77). Follow-up accumulations of childhood adversities reported at follow-ups 1 through 4 ranged from 0 to 7 new ACEs over all follow-up waves with an average of 2.35 (SD = 1.44) experiences. Average ACEs reported from one assessment to the next reveal that justice-involved youth reported the highest number of follow-up accumulationx from baseline to follow-up 1, 3 years later (M = 1.67, SD = 1.30) and between follow-up 1 and follow-up 2, half a year after follow-up 1 and 3.5 years after baseline (M = 0.82, SD = 0.97). The ACEs most frequently reported at baseline included experiences of emotional and physical abuse, household mental health, and household substance abuse. The ACEs most frequently reported at follow-ups 1-4 included experiences of emotional and physical abuse, household substance abuse, and household incarceration.
Descriptive Statistics (n = 851).
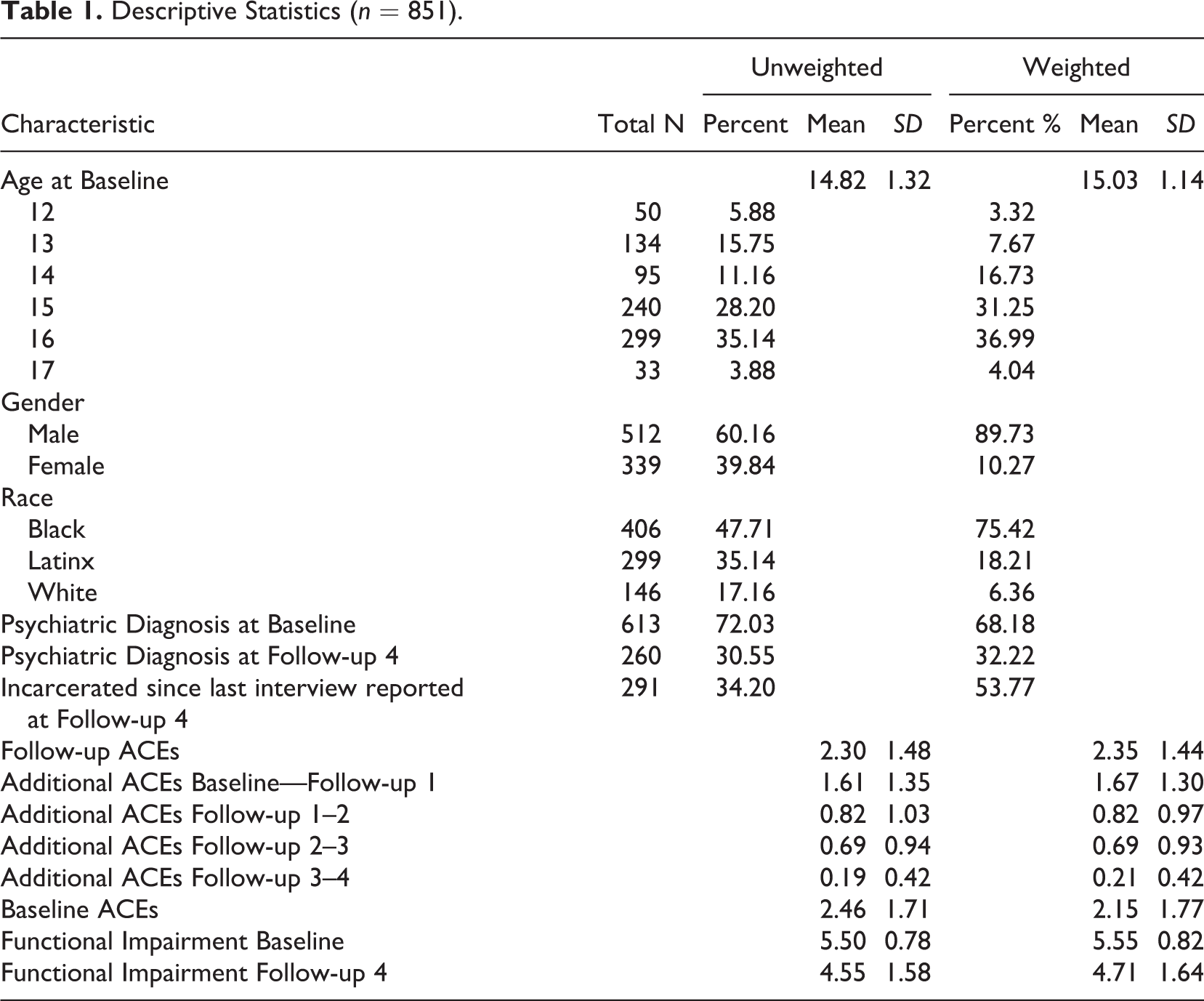
Baseline assessments of functional impairment averaged 5.55 (SD = 0.82), revealing that initial scores of global functioning were between the range of “variable functioning with sporadic difficulties/symptoms in several areas” and “moderate functioning in most social areas/severe impairment in one area.” Follow-up 4 assessments of functional impairment averaged 4.71 (SD = 1.64), revealing global functioning in the range of “some difficulty in a single area/generally functioning well” and “variable functioning with sporadic difficulty/symptoms in several areas.” Approximately one third of the sample reported a psychiatric disorder at follow-up 4 (32%). Additionally, at follow-up 4, 4.5 years after entering Cook County’s juvenile system, over half of the adolescents in the sample reported recent incarceration (54%).
Bivariate Results
Table 2 presents data for all bivariate correlations. Pearson’s bivariate correlations were significant between several variables and follow-up ACEs, including a negative association with age (r = −.10, p < .01) and positive associations with functional impairment scores at follow-up 4 (r = .19, p < .0001), baseline ACEs (r = .24, p < .001), incarceration at follow-up 4 (r = .12, p < .001), and psychiatric diagnosis at follow-up 4 (r = .13, p < .001). Baseline ACEs were also correlated with several variables, including a positive association with baseline functional impairment scores (r = .16, p < .001) and gender (r = .15, p < .001).
Bivariate Correlations Between Study Variables (n = 851, Weighted).
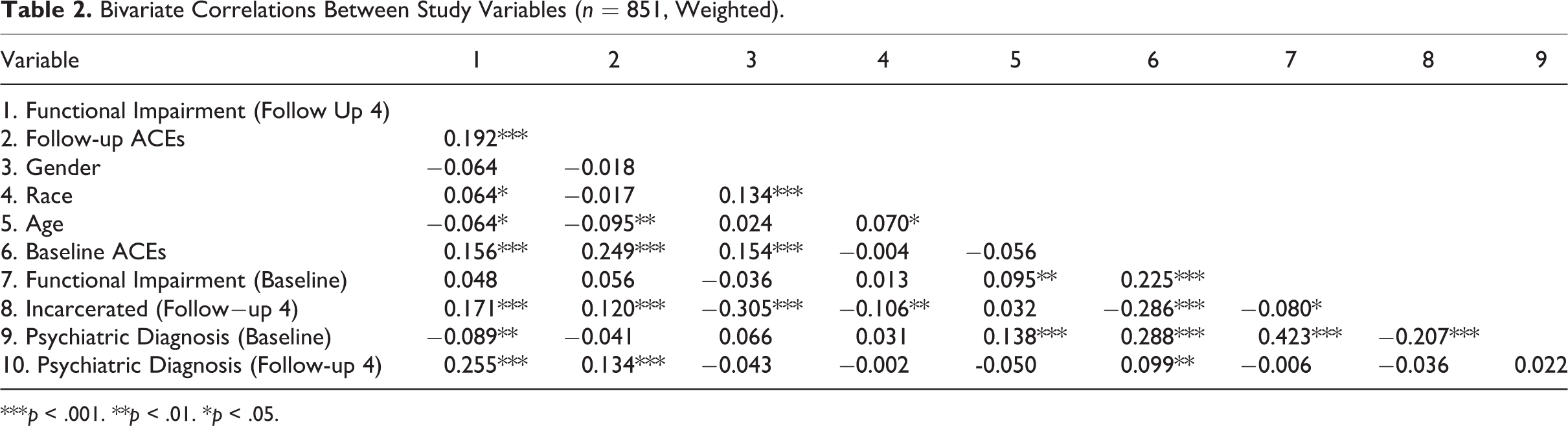
***p < .001. **p < .01. *p < .05.
OLS Results
Table 3 presents results from all three OLS regression models. In the first model, a greater number of follow-up ACEs were related to worse functional impairment at follow-up 4 (β = 0.21, p < .001), controlling for socio-demographics. Every additional follow-up ACE exposure was associated with a 0.21 scale change in functional impairment on the 1 to 10 scale, indicating lower functioning. Latinx youth compared to Black youth also had greater functional impairment at follow-up 4 (β = 0.35, p < .05). Female youth had lower levels of functional impairment compared to males (β = −0.37, p < .05). In the second model, including the addition of baseline ACEs, follow-up ACEs (β = 0.18, p < .001) and identifying as Latinx (β = 0.37, p < .0) remained significantly related to functional impairment at follow-up 4. Gender was also significant (β = −0.47, p < .05) indicating that males had greater functional impairment at follow-up 4 than females. The addition of baseline ACEs was significant in the model (β = 0.12, p < .001) and slightly changed the predictive power of follow-up ACEs and race and ethnicity. In the third model, including the addition of baseline functional impairment, baseline psychiatric diagnosis, and follow-up psychiatric diagnosis, the association of follow-up ACEs to impaired functioning at follow-up 4 and baseline ACEs to impaired functioning at follow-up 4 continued to have a positive effect. While controlling social demographics, baseline functional impairment, psychiatric diagnosis, and incarceration, every additional follow-up ACE exposure was associated with a 0.08 (p < .05) scale change in functional impairment, revealing lower functioning. Every additional baseline ACE exposure was associated with a 0.18 (p < .001) scale change in functional impairment. Latinx adolescents compared to Black adolescents experienced a 0.42 (p < .001) increase in functional impairment scores, also indicative of lower functioning. Recent incarceration was associated with lower functioning (increased impairment), an increase of 0.75 (p < .001). Lower functioning at baseline was related to lower functioning at follow-up (β = 0.14, p < .05). Having a psychiatric diagnosis at baseline was related to higher functioning at follow-up (β = −0.46, p < .001). Lastly, a recent psychiatric diagnosis reported at follow-up 4 was associated with an increase in functional impairment, an increase of 0.69 (p < .001). Interactions were examined for the possible moderation of psychiatric diagnosis on the association between follow-up ACEs and impaired functioning at follow-up 4, but no significant relationships were found.
OLS Regression of Baseline and Follow-Up ACEs Predicting Functional Impairment at Follow-Up 4 (n = 851, Weighted).
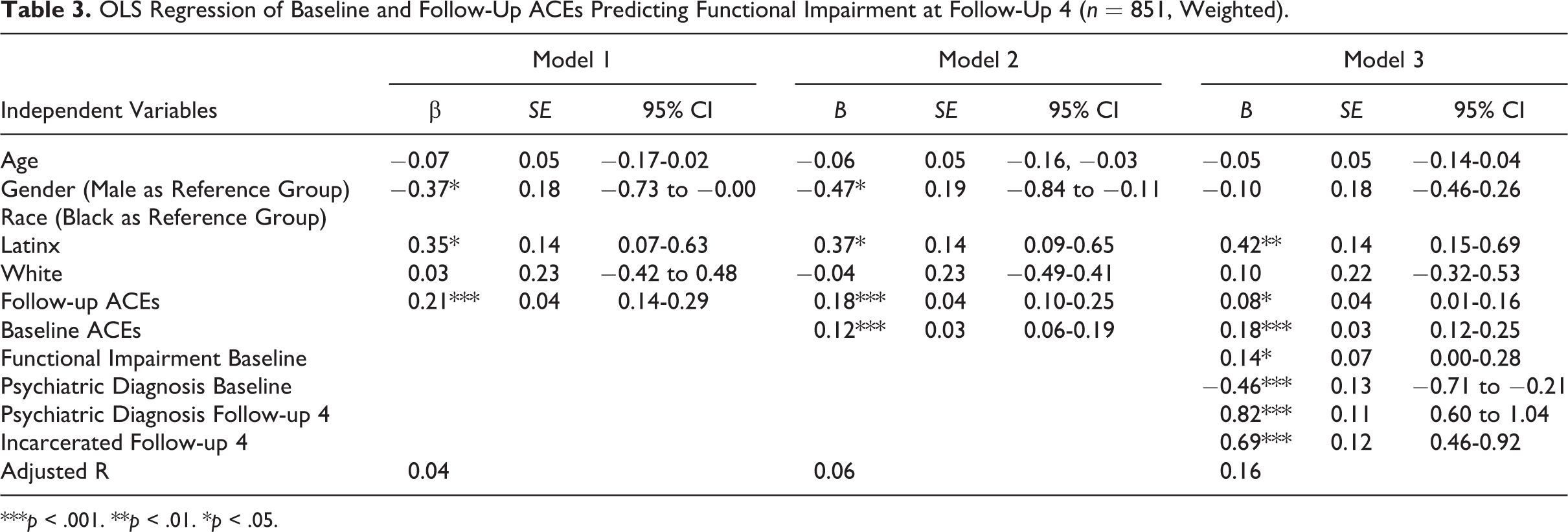
***p < .001. **p < .01. *p < .05.
Discussion
The purpose of this study was to investigate the association between follow-up and baseline accumulations of ACEs and impaired functioning among justice-involved adolescents. Specifically, we explored whether ACEs accumulated during the course of the study (follow-up) and ACEs accumulated prior to the study (baseline) predicted greater functional impairment. Both baseline and follow-up ACEs significantly predicted difficulties in social and psychiatric functioning among the sample. Baseline ACEs demonstrated a greater influence than follow-up ACEs, suggesting that early adversities continue to have long lasting and consequential negative effects. Not only do childhood traumas immediately diminish child well-being and functioning, but traumas in childhood and adolescence demonstrate toxic consequences on several domains of functioning well into adulthood (Cloitre et al., 2009; Ogle et al., 2013).
Adversity and Delinquency
Overall, the accumulation of ACEs experienced by justice-involved adolescents support previous empirical literature establishing a graded relationship between personal adversities and several harmful outcomes (Bielas et al., 2016; Flaherty et al., 2013; Hunt et al., 2017). In fact, the connection between childhood trauma and delinquent behaviors is well documented (Finkelhor, et al., 2011; Wilkinson et al., 2018; Wood et al., 2002). This association between childhood trauma and delinquent behaviors is of particular concern given the high exposure to adversities reported by participants in this study over the four and half years examined. Furthermore, the repeated measurement of ACEs at distinct times demonstrates that youth are often exposed to new incidents of adversity, whether of the same type as previously documented or new types. Taken together, the persistence of accumulations of adverse encounters suggests that children and adolescents who are justice-involved are challenged by multiple relational and environmental constraints that increase the likelihood of ongoing exposure.
Ongoing Risk for Adversity
Consistent with previous research, we found that many adolescents who experienced traumas in earlier years reported ongoing experiences of abuse in later years (Finkelhor et al., 2007b). Previous research has indicated that a continuity of stress exposure exists such that early adversities are associated with continuous structural environments that increase the likelihood of further risk exposure (Finkelhor et al., 2007b; Raposa et al., 2014). Childhood adversities are accumulated across life-course development revealing a linkage of more distal adversities to more proximal ones, what can be considered an interrelation of risks with the possibility of experiencing more than one type of trauma increasing as children age (Dierkhising et al., 2013; Turner & Butler, 2003). The continuity in pernicious exposures accumulated over time has many cataclysmic results for youth. Heterogeneity in findings from previous research concerning recency, accumulation, and timing of exposures suggest that declines in youths’ well-being may result in different symptoms depending on personal characteristics and experiences. In recent research, Dunn et al. (2019) found that timing of adversity rather than accumulation or recency of events better explained the variability of DNA methylation which controls gene expression. Further, Dunn et al. (2018) concluded that the relationship between adversity and mental health symptoms demonstrated different pathways depending on sex and type of exposure. Beyond quests to single out the most consequential attributes of ACEs, we recognize that such toxic exposures have strong effects on health and well-being. Our focus on impaired functioning scores in relation to ACE exposure over time adds to the literature examining mental health outcomes by considering levels of functioning separately from psychiatric diagnosis. For systems interacting with youth at high risk for new or ongoing adversities, this study supports treatment approaches, particularly trauma-informed modalities, that consider youths’ functional impairment as an important indicator of rehabilitation.
Adversity and Functional Impairment
As changes in functioning often lag symptom changes, functional outcomes can help with monitoring treatment success (McKnight & Kashdan, 2009). Further, although severity of symptoms and level of functioning may be confounded, functional impairment is an interaction of the individual with the environment, such that certain individuals with severe symptoms of a disorder may show little impairment while individuals with mild to moderate symptoms may demonstrate more impairment (ÜStÜN, & Kennedy, 2009). In a longitudinal study of youth receiving mental health services in Australia, Iorfino et al. (2018) found that chronic functional impairment was experienced by youth suggesting that functioning as well as symptomatic relief be the focus of interventions. Using NJP data, Teplin et al. (2002) found that just under 67% of males and more than 70% of females had both a diagnosis and impairment in functioning relating to that diagnosis at baseline.
Along with clinical interviews to assess and qualify functioning, impaired functioning scores have been used to understand problematic behaviors in the domains of family life, peer relationships, and school life, reflecting the lowest level of functioning in a designated short-term duration preceding the assessment (Shaffer et al., 1983). Researchers have found that CGAS scores under 61 (a 4.9 on the 1-10 scale), combined with mental health symptoms, are indicative of clinical cases of mental health disorders, and that cut-off has become commonly used (Bird, 1999; Bird et al., 1987; Bird et al., 1990; Shelton, 2004; Teplin et al., 2005). The lack of moderation of psychiatric diagnosis on the relationship between baseline ACEs and impaired functioning demonstrates that lower levels of functioning among youth enduring adversities were not associated with the presence of a psychiatric diagnosis. Although many justice-involved adolescents are inflicted by mental health service needs and there may be overlap between symptoms and impairment, recognizing and addressing experiences of adversity may be paramount to improving low levels of functioning.
Results of the current study indicate that on average, adolescents involved in the justice system were assessed as having clinically impaired functioning 4.5 years after their first assessment. Related to this functioning was the consistently significant relationship of both groups of ACE accumulations. Each additional follow-up ACE reported was associated with a 10% reduction in reported functional impairment and each baseline ACE reported was associated with a 119% reduction. Assessing mental health service needs through youth experiences of adversities or traumas may provide for more robust juvenile outcomes and an opportunity for juvenile justice systems to offer targeted services that could mitigate the factors associated with new or ongoing adversity. As some research has found that abuse at different developmental stages may be associated with distinct psychiatric symptoms, it may also be helpful for juvenile justice organizations to ask about when such adversities occurred (Schoedl et al., 2010).
Considering Cultural Experiences of Adversity and Functional Impairment
While juvenile justice populations are overwhelmingly represented by youth of color, considering differences by race and ethnicity may be helpful to establishing targeted and culturally sensitive intervention practices. In this study, Latinx adolescents compared to Black adolescents experienced a 39% increase in functional impairment over 4.5 years. For these youth, functioning in several domains worsened over time. Considering that those who identified as Lantinx are the fastest growing ethnic group in the criminal justice system (Schuck et al., 2004) and that these individuals tend to have low levels of mental health treatment use (Dalton et al., 2009), understanding the factors that may be influencing low functioning is a critical next step for supporting this population in the juvenile justice system. Research focused on Latinx youth and their families has found that immigration status and acculturation can influence well-being (Lorenzo-Blance et al, 2016). Parent acculturation stress can interrupt positive family functioning and negatively impact the mental health and substance use of adolescent children (Lorenzo-Blanco et al., 2016). Health inequities related to discrimination, social isolation, communication barriers, and racial/ethnic competition for work, housing, and educational and social resources may be more salient for this group, also influencing low levels of functioning (Barrington et al., 2012). Juvenile justice systems can use this finding along with other research related to race and ethnicity to explore culturally relevant experiences of family life and daily living that may be interfering with positive development and successful use of services particularly for Latinx youth.
Severity of Need Reflected through Severity of Justice Involvement
It is also important to note than adolescents in the study who had experienced incarceration sometime in the 3 months preceding the last follow-up assessment had over 70% greater impairment than adolescents who had not been incarcerated during this time. The Mendel report (2011) documents how state-funded institutions have failed to protect youth from abuse while in correctional confinement or reduce recidivism. Aside from adversities related to legal inequities or institutional practices, justice facilities often cannot meet the mental health needs of adolescents under their care (Mendel, 2011). Those youth receiving more restrictive adjudications may be those who demonstrate more complex behaviors that reflect high levels of need. This finding further supports policies and practices that expand community-based services for justice-involved youth and screening for adverse exposures within juvenile justice systems.
Limitations and Future Directions
There are a few limitations of this study that should be considered when interpreting these results. First, caregiver interviews were not included in the study and data relied on youth self-report which may be subject to underreporting. To facilitate youth participation, hard copy questionnaires were supplemented with electronic data collection using the audio computer assisted self-interview (ACASI) for some measures, providing privacy to participants when answering some questions. Second, the exact date associated with each reported ACE was not available. For baseline specifically, this means that it is unknown how early or late in childhood an adversity was experienced. Similarly, the exact age of incident is unknown for the follow-up ACEs reported. Because older youth could be in their 20s at the time of follow-up, potentially living away from home, these adversities may not present the same level of risk as when youth are under 18 years old. Given our expanded understanding of adolescent development as one occurring into ones 20s (Johnson et al., 2009), although the adversities experienced at follow-up may not constitute traditional ACEs they remain potential sources of trauma. Additionally, information on the severity, duration, or co-occurrence of adversities experienced was not available in this dataset. Therefore, it was not possible to analyze ACEs beyond the presence or absence of at least one experience of each ACE in the study. Finally, these data were taken from a large metropolitan city and may not be generalizable to youth in other settings such as rural environments.
Future directions of this study include replicating this study with contemporary data, and examining the severity, duration, or co-occurrence of ACEs and their impact on functional impairment for youth. Further, exploration of ACEs over a longer period of time would be important to assess approximate timing of ACE experiences to better understand if recency most strongly influences youth during adolescence or young adulthood and if developmental timing (early, middle, late childhood) is associated with greater psychopathology and impaired functioning. Additionally, the pathway through which ACEs influences functional impairment requires further investigation. Factors mitigating functional impairment, such as the identification of promotive factors to increase the likelihood of positive outcomes, may also be important in reducing risk among justice-involved youth. Promotive factors may include positive parental and family relationships, adaptive coping skills, social supports, and the use of mental health services. These factors are important to consider in future studies. Finally, the accumulation of ACEs are critical risk factors, but they are not the only risk factors. Consistent with cumulative risk models, it would be helpful to explore accumulations of ACEs along with other risk factors such as neighborhood conditions, family structure, and financial stability.
Conclusions
Justice-involved adolescents experience persistent exposures to adverse experiences which reduce global functioning. As juvenile justice systems interact with youth entering supervision with a high number of early ACEs and a high likelihood of experiencing adversity through new or persistent exposures, an opportunity exists to intervene to reduce the negative conditions associated with ongoing risk. Services at all levels of the juvenile justice system, from incarceration to re-entry, or immediate community supervising, can be strengthened through screening for ACEs and assessing impaired functioning. Such screening and assessment recognize that ACEs can influence impaired functioning, requiring trauma-informed interventions that contextualize delinquent behaviors through the lens of adversity risk. Overall functioning will be better improved by targeting the source of youths’ problematic behaviors as well as the problematic behaviors themselves.
Identifying ACEs may be a first step to determining an appropriate course of action that allows services to target critical areas of need. As many adversities included in an ACE screening pertain to maltreatment or household dysfunction, services should involve caregivers as appropriate, particularly when a youth is a minor. Other types of support may also benefit youth who report ACEs in order to limit further exposure and mitigate consequences of earlier historical ACEs. Positive social networks that include peer engagement and a caring adult role model, promotion of self-regulation strategies, asset building in academics or extracurricular activities, economic development, and family relationship building may work as promotive factors to reduce risk.
Furthermore, a measure of functional impairment may serve as an important indicator of program success and youth improvement that juvenile justice systems could incorporate in evaluating service outcomes. Juvenile justice systems have an opportunity to intervene with rehabilitative efforts that consider the environmental factors that may perpetuate risk. In particular, the persistent risk of childhood adversity found among justice-involved youth suggests that trauma-informed evaluations and services are needed to promote success in behavioral modification and personal well-being.
Footnotes
Acknowledgments
The authors would like to acknowledge the support of several research assistants who helped to organize the data, complete literature searches, and prepare references, including Amanda Costellano, Larissa Dinatale, Hima Sathian, and Alicia Pichalski.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.