
Abstract
Court-involved youth (CIY) comprise a significant portion of the U.S. population and have a high prevalence of psychiatric illness and substance use. Youth delinquency has also been associated with family variables and parenting practices. However, it is not known which family factors are most relevant to behavioral outcomes in CIY mandated to outpatient mental health treatment. Self-report measures from 163 CIY (M = 15.19 years; 58.3% male) starting psychiatric care in two U.S. cities were utilized in a cross-sectional analysis to examine the association of parental monitoring and family functioning with the severity and variety of delinquent acts. Results demonstrate that, even after controlling for psychiatric symptoms and substance use, parental monitoring is significantly associated with the delinquent behavior of CIY in mental health treatment. Improved understanding of influential family factors can enhance tailoring of existing interventions to ensure that they are relevant to the needs of CIY, especially those in psychiatric treatment.
Introduction
According to the National Center for Juvenile Justice, in 2019 approximately 700,000 youths under the age of 18 received dispositions through the juvenile court system in the United States (U.S.; Sickmund et al., 2020). Considering this vast number, it is important to recognize that court-involved youth (CIY) have a high prevalence of psychiatric illnesses, such as disorders of attention, anxiety, mood, substance use, and learning (Winkelman et al., 2017; Perry and Morris, 2014; Teplin et al., 2003; Shufelt and Cocozza, 2006). In addition, CIY have been shown to have an elevated risk of suicide (Coffey et al., 2003; Barnert et al., 2016; Morris et al., 1995; Kemp et al., 2016). Furthermore, in studies involving CIY, approximately 50% or more of participants endorsed engaging in substance use (Castrucci and Martin, 2002; Teplin et al., 2003; Teplin et al., 2005; Tolou-Shams et al., 2021) with cannabis being one of the most common (Morris et al., 1995; Tolou-Shams et al., 2021). Psychiatric symptoms, including difficulties with affect regulation (Brown et al., 2012), externalizing symptoms (Haney-Caron et al., 2019), and aggressive disorders (Barrett et al., 2014), have also been associated with risky and delinquent behaviors. Therefore, providing mental health treatment to CIY is a potential means by which to reduce and prevent recidivism or system re-entry, as well as reducing other morbidities associated with psychiatric disorders. Studies have demonstrated that receiving mental health treatment reduces time-to-re-offending and recidivism rates in CIY (Zeola et al., 2017; Kendall et al., 2017; Perry et al., 2019), emerging adults (Davis et al., 2015; Sheidow et al., 2016), and adults (Wallace and Wang, 2020).
Although providing mental health treatment to CIY is a critical component of recidivism prevention, these youths’ psychiatric symptoms, behaviors, and justice-involvement cannot be viewed in isolation from the larger family system. As CIY are minors, their caregivers are engaged in both their home lives and in their court-appointed dispositions. Furthermore, the relationship between youth behavior and the family unit appears to be bidirectional. Namely, youth delinquency and court-involvement cause stress and strain on the family system, and the family unit itself impacts youth behavior with notable potential for buffering and improvement in outcomes. Viewing delinquency in the context of both psychopathology and family factors is consistent with the Social-Personal Framework (SPF), which has been previously utilized in interventions targeting adolescent risk behaviors (Donnenberg et al., 2018; Brown et al., 2014; Snow-Hill et al., 2021;Kendall et al., 2017). The SPF highlights that adolescent risk-taking does not occur in isolation, but rather in the setting of personal attributes, family context, peer and partner relationships, and environmental circumstances (Donenberg & Pao, 2005).
In support of this theoretical framework, previous research has demonstrated relationships between family functioning, parental mental health, parenting practices, and youth behavior in CIY (Tolou-Shams et al., 2012; Tolou-Shams et al., 2018; Folk et al., 2020; Bouffard & Armstrong, 2021) and in non-court-involved populations (Barker et al., 2019; Donenberg et al., 2012, 2018). Findings to date have demonstrated that differences in family context, including communication, relationships, monitoring, and permissiveness, are associated with substance use, functional impairment, risky sexual behavior, psychiatric symptom burden, and response to psychosocial interventions (Barker et al., 2019). Furthermore, among CIY, impaired parent-child communication and family affective responsiveness have been shown to be related to engagement in unprotected sex and cannabis use (Tolou-Shams et al., 2012). Interventions for juvenile offenders that involve caregivers have shown promise in targeting unsafe behaviors, such as substance use and risky sex (Tolou-Shams et al., 2017) as well as re-offending (Davis et al., 2015; Sheidow et al., 2016; Perry et al., 2019; Celinska et al., 2019; Gottfredson et al., 2018). These interventions have utilized a variety of methodologies including Multisystemic Therapy (MST; Davis et al., 2015; Sheidow et al., 2016), affect management strategies (Tolou-Shams et al., 2017), and Functional Family Therapy (FFT; Celinska et al., 2019; Gottfredson et al., 2018). Therefore, CIY’s families and caregivers are an important biopsychosocial factor to consider in recidivism prevention.
While previous research has demonstrated general associations between CIY’s behavior and psychosocial family factors and parenting practices, it is not known how these familial attributes relate to delinquency outcomes in youth diverted by the court to mental health treatment, which can be brief and focus solely on individual treatment. Pursuing this understanding would allow for the creation of tailored, evidence-based services that could address these key and modifiable familial factors in this population and thus, effectively prevent continued involvement and later re-entry into the justice system. Therefore, our objective was to utilize this multifaceted approach, supported by the SPF, and explore the specific roles of family functioning and parental monitoring in the severity and variety of delinquent acts by CIY at the start of their court-mandated mental health treatment. Our examination of the literature, as described above, informed our decision to specifically choose these familial constructs due to their links to youth behavior. We hypothesized that family functioning and parental monitoring would be associated with recent delinquent behaviors in youth diverted by the court to outpatient psychiatric care.
Methods
Participants
Between November 2011 and April 2015, 598 adolescents were referred for study participation by court officials (i.e., intake worker, probation officer, magistrate, or judge) after diversion to mental health treatment. Youth were eligible if they were: 1) able to speak and read English; 2) between the ages of 11 and 17 years; 3) had an open petition with the partnering Family Court at the time of referral; and 4) residing with a legal guardian who was able to attend weekly therapy sessions. Referred adolescents were excluded if they: 1) were currently enrolled in mental health treatment; 2) had prior psychotic symptoms which necessitated intensive treatment at a higher level of care; or 3) required evidence-based care not included in the current intervention, including those charged with sexual offenses and/or carrying diagnoses of obsessive-compulsive disorder or pervasive developmental disorder. Approximately 53% (n = 317) of referred individuals were eligible to participate, among whom 54% (n = 170) provided consent. This paper utilizes data from 163 adolescents who provided valid baseline data.
Procedures
Adolescents and parents/caregivers were recruited from two eastern U.S. cities for a longitudinal randomized controlled trial (RCT) which compared standard community mental health counseling to a novel intervention that integrated mental health treatment with an HIV prevention program. Adolescent participants being diverted to the community in place of detention, were referred by the court when mental health services and evaluation were warranted. Consent was obtained prior to participation. The Institutional Review Boards of the two participating sites approved all study protocols. Adolescents completed measures on laptop computers utilizing an audio computer-assisted self-interview (ACASI) program. For the purposes of this study, only the youths’ baseline survey responses at study intake were analyzed. Study methods have been reported elsewhere and are summarized below (Tolou-Shams et al., 2018).
Measures
Independent Variables
Demographics
Demographic data for adolescent participants.

Dependent Variables
National Youth Survey of Self-Reported Delinquency (NYS).
The NYS is a 40 item self-report measure designed to assess the type of delinquent acts that adolescents commit, including stealing, carrying weapons, engaging in violence, using and selling drugs, and public misconduct (Elliott et al., 1985). It also assesses how often drugs and alcohol were involved in these delinquent acts. The NYS has been shown to have acceptable reliability and validity with correlations equaling r = .75 for frequency and r = .84 for variety of acts reported with a mean coefficient of r = .74 (Huizinga & Elliott, 1986). This measure was administered at study intake in order to assess for lifetime engagement in delinquent behaviors prior to adjudication to mental health treatment by the court.
Delinquency Severity: Youth were divided into three delinquency severity categories based on their responses to the NYS: serious, moderate, and minor. These categories have been previously utilized and validated in the literature regarding CIY population (Haney-Caron et al., 2019). Youth were placed into the
Delinquency variety: The variety of delinquent acts was a variable generated from the well-validated (α = .93) general delinquency subscale of the NYS, which is a summary measure consisting of the 24 items that examine a full range of delinquent acts (Elliott et al., 1985). For the purposes of this study, the item “Have you had sexual intercourse with a person who was not your serious partner when involved in a relationship?” was excluded from this subscale. This 23-item version of the general delinquency subscale has also been utilized and published in the literature (Feaster et al., 2010; Tolou-Shams et al., 2019; National Institute on Drug Abuse, 2016). Higher scores on this subscale indicate a greater number of types of delinquent acts endorsed.
Statistical Analysis
For the purposes of this investigation, only self-reported baseline responses were analyzed. The primary outcomes were severity and variety of delinquent acts. Means and standard deviations were calculated for scale scores and categorical variables. Initial analyses, including t tests, chi-square tests of independence, and analyses of variance (ANOVAs/ANCOVAs) were conducted to compare demographic and baseline variables across the delinquency severity groups and frequencies of delinquency. Correlations were used to assess the relationship between baseline measures (i.e., FAD, PMQ, GSI, CDDR), delinquency outcomes, and demographic variables. Variables that were significantly associated (p < .05) in the bivariate analyses were entered into regressions in order to examine the extent to which they were associated with delinquency severity (ordinal multiple logistic regression) and variety (negative binomial multiple linear regression). We specifically included psychiatric symptoms and substance use, in addition to demographic variables, in our statistical analyses and models as above in order to account for the fact that these participants were all mandated to mental health treatment. Furthermore, we also wanted to recognize for the high prevalence of psychiatric symptoms and substance use in CIY populations and the potential impacts of these factors on youth behavior (Winkelman et al., 2017; Perry and Morris, 2014; Teplin et al., 2003; Shufelt and Cocozza, 2006; Castrucci and Martin, 2002; Teplin et al., 2005; Tolou-Shams et al., 2021; Brown et al., 2012; Haney-Caron et al., 2019; Barrett et al., 2014). All analyses were done with IBM SPSS Statistics for Windows, version 26 (IBM Corp., 2019).
Results
Demographics
The adolescent participants ranged in age from 12 to 17 years old with an average age of 15.19 years (SD = 1.36). The majority were White (60.7%) and male (58.3%). Full demographic data is presented in Table 1.
Utilizing the NYS, 36.2% of the sample were determined to have severe delinquency, 31.3% moderate delinquency, and 32.5% minor delinquency. Regarding substance use, cannabis and alcohol were the primary substances used with only 11.7% reporting use of other drugs. Among the participants, 38.7% reported using cannabis and 32.5% reported consuming alcohol in the past 3 months. Of those who drank alcohol, 73.6% (23.9% of all participants) reported engaging in binge drinking of five or more drinks at least once during the past 3 months.
Primary Analyses
Initial associations between psychosocial variables and prior delinquency severity.
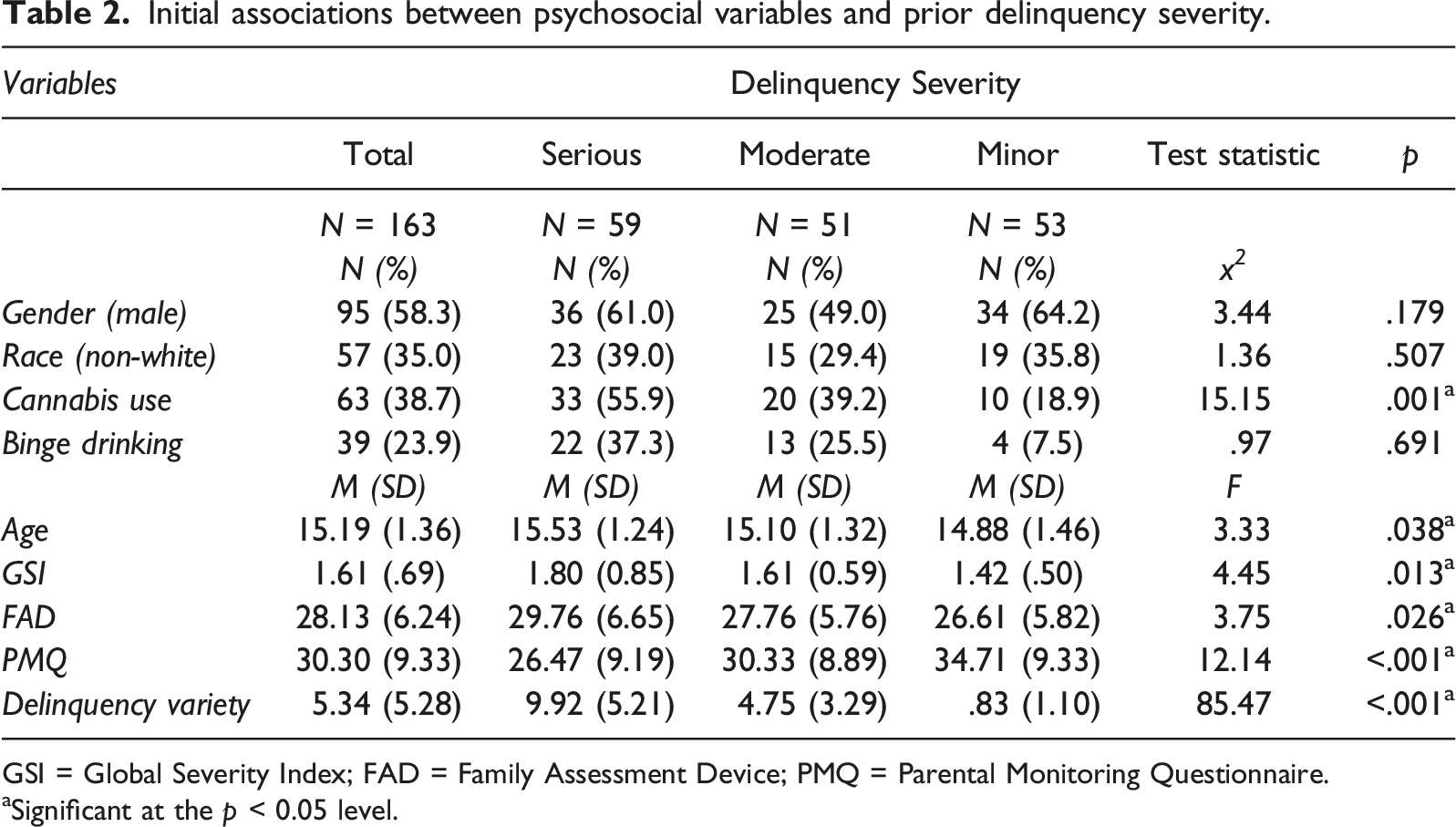
GSI = Global Severity Index; FAD = Family Assessment Device; PMQ = Parental Monitoring Questionnaire.
aSignificant at the p < 0.05 level.
Initial analyses between variables and prior delinquency variety.

GSI = Global Severity Index; FAD = Family Assessment Device; PMQ = Parental Monitoring Questionnaire.
aSignificant at the p < 0.05 level.
Ordinal multiple logistic regression analysis of psychosocial variables and prior delinquency severity.
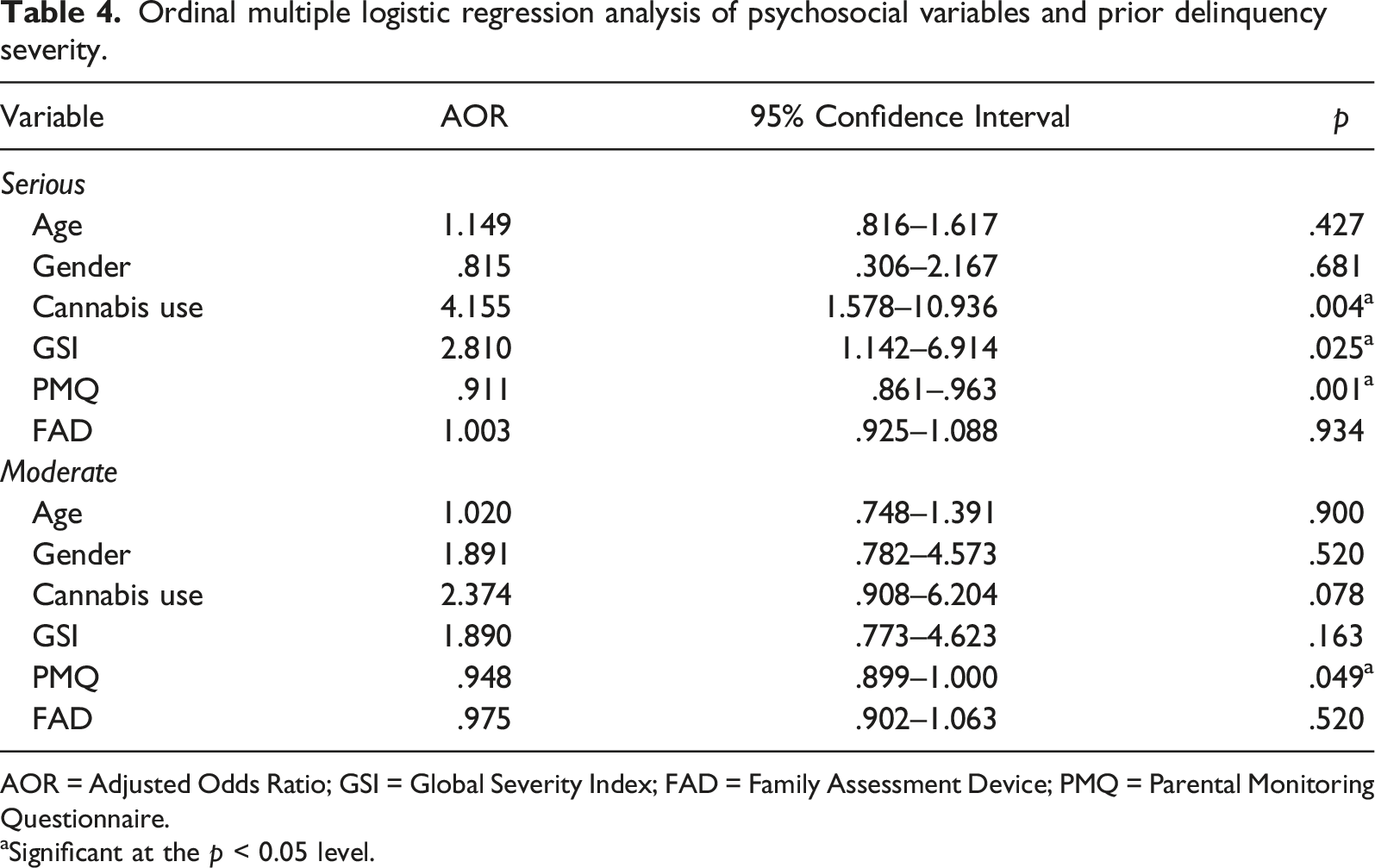
AOR = Adjusted Odds Ratio; GSI = Global Severity Index; FAD = Family Assessment Device; PMQ = Parental Monitoring Questionnaire.
aSignificant at the p < 0.05 level.
Negative binomial multiple linear regression of psychosocial variables and prior delinquency variety.

GSI = Global Severity Index; FAD = Family Assessment Device; PMQ = Parental Monitoring Questionnaire.
aSignificant at the p < 0.05 level.
Discussion
In this study, parental monitoring was significantly associated with the severity and variety of delinquent acts by youth at the start of their court-mandated mental health treatment, even after controlling for other significant factors, including psychiatric symptom burden and cannabis use. This study, which utilized a sample of CIY who met criteria for mental health treatment and were adjudicated to this level of care, demonstrates that psychiatric care focusing solely on the youth may not be enough to promote optimal behavioral outcomes. In fact, this study suggests that clinical interventions which target parenting practices, namely parental monitoring, may provide additional benefit to this high-risk population. This is in keeping with previous literature that shows parental factors should be addressed in treatment provided to CIY in order to reduce and prevent delinquency as well as further justice system involvement (Celinska et al., 2019; Gottfredson et al., 2018; Davis et al., 2015; Sheidow et al., 2016). It is also consistent with the SPF which highlights the importance of addressing personal context, including family factors, when considering youth risk behaviors (Donenberg & Pao, 2005). Family-based interventions, including MST and FFT, have been shown to be effective at improving delinquency outcomes in CIY (Sawyer & Borduin, 2011; Davis et al., 2015; Sheidow et al., 2016; Celinska et al., 2019; Gottfredson et al., 2018). However, these programs can be intensive both in terms of time commitments, staff support, and resources. They also may not always be feasible for family systems already under significant stress and strain as well as in a post-pandemic reality where staff shortages are commonplace. Furthermore, difficulties with insurance coverage may impact a family’s ability to participate, with one study demonstrating that approximately 20% of a large sample of system-involved youth could not participate in MST due to funding issues (Vidal et al., 2017). Therefore, establishing which unique and specific familial factors and parenting practices have the most impact on youth behaviors will be useful for future intervention development to create programs that are brief and tailored, including for those in psychiatric care.
Interestingly, in this current study, parental monitoring was the only significant family factor associated with youth delinquent behavior. Family functioning, while showing some association with delinquency severity and variety at the bivariate level, was no longer significantly associated when tested in a multivariable model. While previous research involving non-justice involved youth has shown that parental monitoring can influence youth behavior (Rusby et al., 2018; Holmgren et al., 2019; Odukoya et al., 2018; Lopez-Tamayo et al., 2016; Pollak et al., 2020), studies examining CIY have shown inconsistent results. Namely, Tolou-Shams et al. (2012) demonstrated that poorer parental communication, not parental monitoring, was associated with cannabis use and unprotected sex. Furthermore, Folk et al. (2020) found that parental monitoring did not predict youth delinquency and substance use nor did it mediate the relationship between baseline parental and youth psychiatric symptoms, whereas family functioning did. However, these above studies did not directly examine outcomes of delinquency severity and variety. Moreover, Folk et al. (2020) examined prospective data and not all youth in that sample had identified mental health needs, whereas this current study utilized baseline data of youth who were referred to mental health treatment. It is possible that the importance of specific family factors, such as family functioning and parental monitoring, may depend on the needs and stage of these youths’ psychiatric treatment. Therefore, it is possible that good family functioning is a necessary background upon which improved parental monitoring skills can take place or vice versa depending on the specific population of CIY being examined and/or on the stage in treatment the youth and their families are in. Furthermore, parental monitoring may have a more direct effect on our specific outcome variables than family functioning as enhanced parental supervision may reduce opportunities for delinquency.
Another family factor to consider is parental mental health. Previous research indicates that in order to target parenting practices, parental mental health must also be considered in clinical interventions. A sizeable number of parents of CIY have been shown to have their own clinically significant psychiatric symptoms (Brown et al., 2018). Parental psychiatric symptom burden has been associated with familial factors and, in turn, youth behavior. For example, parental psychiatric symptoms have been associated with worse family functioning (Folk et al., 2020), which may subsequently contribute to poorer parental monitoring (Tolou-Shams et al., 2018). Therefore, effective interventions should also refer parents for their own treatment and assist them with improving their relationship with their adolescents, general family functioning, monitoring and family climate.
Limitations
This study had several limitations. Firstly, all measures utilized were self-report measures, which may have introduced recall bias, especially for measures assessing multiple months in the past, and social desirability bias, which could have contributed to underreporting regarding substance use and delinquent acts. Additionally, for the purposes of this study, only the adolescent versions of the measures were utilized and, thus, any potential discrepancies between parent and child reports of parental practices were not addressed. However, a recent study demonstrated that while parent reports, as well as discrepancies between youth and parent reports, are important predictors of youth delinquency, youth reports of parenting behaviors alone are highly predictive of delinquent behaviors (Bouffard & Armstrong, 2021). Furthermore, this study recruited a specific subset of justice-involved youth, namely CIY referred to mental health treatment in two cities in the Eastern United States, of which only 54% of those eligible to participate provided consent. Therefore, these results may not be generalizable to the CIY population at large. Additionally, this study was cross-sectional. Therefore, causal conclusions cannot be drawn from the findings and further study is warranted to assess the effects of parental monitoring on youth delinquent behavior over time. Moreover
Strengths
This study did have a number of strengths, including adequate sample size and use of scales that have been validated in psychiatric populations and/or justice-involved youths. Additionally, the sample addressed in this study represents a unique group of CIY: those who have been court-mandated to mental health treatment. Examination of the factors that influence delinquent behaviors in this group is valuable because it can be utilized to inform more tailored, family-based interventions that could potentially be administered during their mental health treatment. Furthermore, this study specifically assesses adolescents’ perspective of their family’s functioning and parent practices, which is important to consider as we are seeking to understand the drivers of youth delinquent behaviors. We also employed categorizations of delinquency severity and variety that have previously been used in the literature (Haney-Caron et al., 2019; Feaster et al., 2010; Tolou-Shams et al., 2019). In addition, as outlined above, our results are consistent with previous findings which highlight the importance of parental practices in youth behavioral outcomes.
Future Directions
Future research directions include examining the changes in parental monitoring and family functioning over the course of mental health treatment and how these factors predict delinquency as treatment progresses. In addition, the mechanisms that may underlie changes in parental behavior, such as emotional management and parental stress, should be examined in order to better inform clinical interventions to address these factors. Concurrently, considering the significant rates of mental health symptoms and parenting stress in the parents of CIY, (Brown et al., 2018) there is also great need for interventions that include parental mental health treatment in addition to parenting skills. Furthermore, examination of the role of addressing substance use in mental health treatment for CIY is needed when considering delinquency outcomes. In general, improved understanding of the biopsychosocial barriers and disparities faced by these youth and their families can allow for better tailoring of existing interventions to ensure that they are relevant to the needs of this population, especially those referred to psychiatric treatment.
Conclusions
This study provides evidence that mental health treatment alone is not enough to promote optimal behavioral outcomes for CIY mandated to mental health treatment. Furthermore, it demonstrates that a specific parenting practice, parental monitoring, is significantly associated with the delinquent behavior of CIY seeking mental health treatment, even when taking into account the role of psychiatric symptoms and problematic substance use. Therefore, to reduce delinquency, clinical interventions need to specifically target parental behavior and skills. Future directions for this research should include improving our understanding of the biopsychosocial barriers and disparities faced by these youth and their families and utilizing this information for better tailoring of existing family-based interventions to address the needs of CIY in psychiatric care.
Nomenclature
Audio Computer-Assisted Self-Interview
Customary Drinking and Drug Use Record
Court-Involved Youth
Family Assessment Device
Functional Family Therapy
Global Severity Index
Multisystemic Therapy
National Youth Survey of Self-Reported Delinquency
Parental Monitoring Questionnaire
Symptom Checklist-90-Revised
Social-Personal Framework
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Providence/Boston Center for AIDS Research (P30AI042853), National Institute on Drug Abuse (Grant: K24DA046569), and National Institute of Mental Health (Grants: 1R01MH087520-01A2, R25 MH125769, and R25 MH087520).