
Abstract
Regenerative medicine for stroke patients has been attracting attention. However, the effects of rehabilitation after the cell transplantation have not been fully elucidated. The purpose of the present study was to investigate whether intensive gait-focused rehabilitation using a robotic orthosis after regenerative medicine improved gait function and induced plastic changes in cortical networks. The present study was conducted in a retrospective cohort study. We selected seven chronic stroke patients, those who had undergone adipose-derived mesenchymal stem cells (MSC) transplantation therapy after the onset of stroke and had been receiving adequate subsequent gait rehabilitation with a robot for more than 2 months. During hospitalization, each patient received at least 2 h of rehabilitation, including robotic-assisted gait training more than five times per week. As the assessments, gait performance and M1 seed-based resting state-functional connectivity (rs-FC) obtained by a magnetoencephalography were compared before and after hospitalization. After rehabilitation, cadence and spatial gait symmetry ratio were significantly improved, and a significant negative correlation was found between the changes in the gait symmetry ratio and the time from transplant to rehabilitation. Seed-based rs-FC in the beta band between the lesioned M1 and multiple brain regions (e.g., both frontal areas, ipsilateral postcentral gyrus) was significantly decreased after the rehabilitation. Significant negative correlations were also observed between the changes in the gait symmetry ratio and the changes in lesioned M1 seed-based rs-FC in the paracentral gyrus and regions associated with the default mode network. It was revealed that intensive gait-focused rehabilitation using a robotic orthosis improved gait function and induced plastic changes in the cortical networks. The improvements were significantly correlated with the timing of the start of rehabilitation after MSC transplantation.
Introduction
After effects of stroke on motor and sensory functions are one of the major obstacles to patients’ activities of daily living and often require nursing care. Numerous rehabilitation approaches have been conducted to improve patients’ quality of life, but there are still many patients who do not recover satisfactorily.
In recent years, regenerative medicine has been attracting attention for stroke patients. The effects of regenerative medicine using mesenchymal stem cells (MSCs) have been investigated and are now in clinical trial stages for medical insurance coverage.1,2 On the contrary, some clinics have been transplanting autologous MSCs to stroke patients as a treatment. However, in these clinical studies and clinical situations, rehabilitation after transplantation has not been adequately considered; it has been performed as a conventional approach or left up to the patients in many cases, and the effects of rehabilitation after regenerative medicine have not been clarified. Consideration should be given as to when, what type, and how much rehabilitation should be provided after the cell transplantation.
It has been reported that treadmill exercise enhanced the effects of MSC transplantation and promoted recovery of motor function in a rat cerebral contusion model, 3 and the combined use of rehabilitation reduced infarct volume, promoted synapse formation, and enhanced neuroplasticity by thickening the corpus callosum. 4 The importance of applying rehabilitation after regenerative medicine was recently proposed toward the goal of optimizing functional recovery through tissue regeneration, remodeling, or repair. 5
Appropriate, repetitive, and reproductive movements are needed to rebuild lost neural circuits in rehabilitation after regenerative medicine. Robot-assisted gait rehabilitation is expected to be one of the most promising tools in postregenerative rehabilitation because it can repetitively provide appropriate stimulation and assistance. The benefits of using robots for gait rehabilitation are earlier initiation in severely dependent individuals, less effort for therapists, longer gait training, higher gait intensity, and more physiological and reproducible gait patterns.6,7 In gait rehabilitation after stroke, various walking-assistive robots have been developed and their clinical efficacies reported.8–10 In a meta-analysis of randomized controlled trials for stroke patients, it was reported that robot-assisted gait training significantly improved gait independence compared with conventional rehabilitation alone. 10
The purpose of the present study was to investigate whether intensive gait-focused rehabilitation using a robotic orthosis for stroke patients after regenerative medicine improved their gait function and had plastic changes in cortical networks, and whether the changes were influenced by the start and the duration of the rehabilitation.
In the assessment, we evaluated not only motor and gait performance but also brain function to know the functional brain recovery itself. It is known that resting state-functional connectivity (rs-FC), which is detected by the synchronization of neural activity between distant brain regions, has attracted attention as an indicator reflecting cortical function. In magnetoencephalographic (MEG) studies, it has been reported that the primary motor cortex (M1) formed a functional network with several motor areas, such as the premotor cortex, supplementary motor cortex, and parietal lobe, and that it was disrupted in stroke patients depending on the degree of functional impairment.11,12
Materials and Methods
Participants
The present study was conducted in a retrospective cohort study. We selected patients from hospitalized for rehabilitation purposes at the Innoshima Medical Associate Hospital, those who met the following inclusion criteria: (1) had gait disturbance due to the cerebrovascular diseases, (2) having underwent adipose-derived MSC transplantation therapy after the onset of stroke, and (3) having had adequate robotic gait rehabilitation during the hospitalization.
Twelve chronic stroke patients had received MSC therapy before the hospitalization; however, three patients were excluded from the study because of the types of MSCs, and two patients were excluded because they were unable to perform robotic gait rehabilitation during the hospitalization due to severe gait disturbance. The profiles of all seven patients who met the criteria are shown in Table 1. They were administered intravenously 1.0–1.2 × 108 autologous adipose-derived MSCs before the hospitalization. The present study was approved in advance by the Ethics Committee of Hiroshima University in accordance with the Declaration of Helsinki.
Patient Profiles
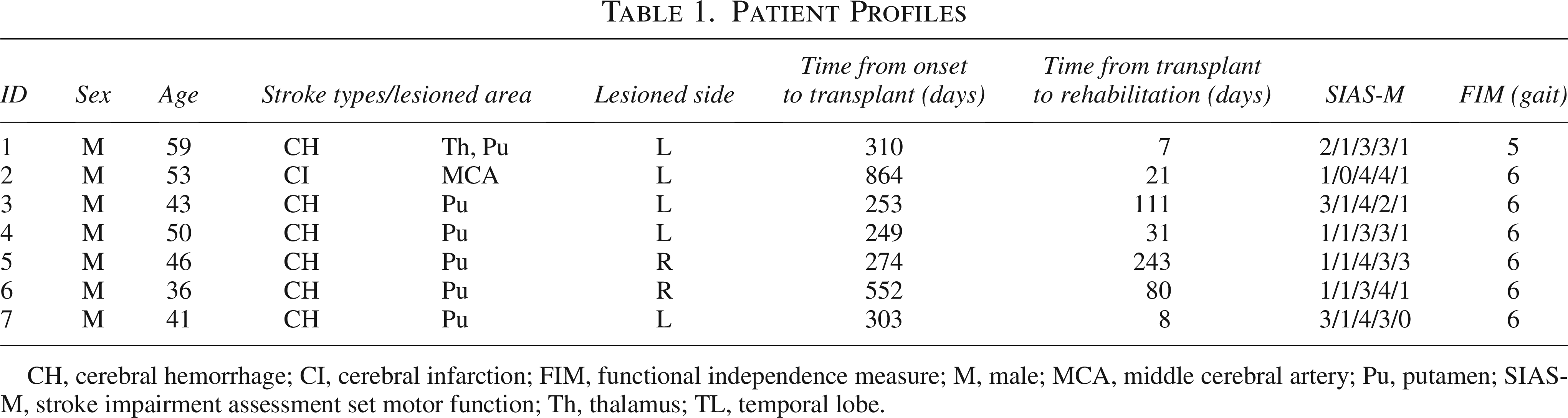
CH, cerebral hemorrhage; CI, cerebral infarction; FIM, functional independence measure; M, male; MCA, middle cerebral artery; Pu, putamen; SIAS-M, stroke impairment assessment set motor function; Th, thalamus; TL, temporal lobe.
RE-Gait
RE-Gait® (Space Bio-Laboratories Co. Ltd., Japan) is a close-fitting assisted walking device shaped like an ankle foot orthosis (AFO). It weighs 1 kg and is easy to wear (Fig. 1). The device decodes the gait cycle using two pressure sensors located at the toe and heel, which control angular velocity in each gait cycle at the preferred timing using an attached tablet. The details were shown in our previous studies.13–15

RE-Gait®.
Robotic rehabilitation
During hospitalization, each patient received at least 2 h of rehabilitation more than five times per week. In addition to conventional rehabilitation, they walked on a flat floor for at least 20 min per day using a close-fitting robotic-controlled AFO, RE-Gait®. Before the robotic gait rehabilitation, conditioning electricity was applied to the lower leg muscles to control spasticity and enhance sensory inputs. 16 The robotic control was set to increase anterior propulsion force during the stance phase and sufficient push-off motion during the preswing phase.
Assessments
The clinical information was obtained by reviewing medical records, including information of MSC transplantation. Results of the 10-m walking test and foot pressure data during the gait were used to assess their gait performance before and after hospitalization. In addition, data on background brain magnetic activities measured by MEG were used for evaluating changes in the cortical functional connectivity.
Gait assessment
Gait performance was assessed by the 10-m walking test. Each patient walked distance of 10 meters at a comfortable speed with their usual walking aid or AFO (or without aids if they did not use them).
Foot pressure was assessed by the pressure-instrumented platform, FDM 1.5 Pressure Walkway (Noraxon USA Inc., Arizona, USA) with a sampling frequency of 100 Hz. Patients were asked to walk on the sheet for five round trips at a comfortable speed. The footprinted area was recorded automatically by the software module, MyoPressure P150 (Noraxon USA Inc., Arizona, USA). Based on the data obtained, we analyzed the spatial characteristics by calculating the step length of each stance phase.
MEG measurements
MEG measurements were recorded using a 306-channel whole-head MEG system (Vector-view, ELEKTA Neuromag, Helsinki, FIN) under eye-closed resting conditions in the supine position in a magnetically shielded room. The measurement time was 5 min. MEG signals were digitally recorded at a sampling rate of 1,000 Hz.
Analysis
Gait analysis
Gait performance was assessed before and after hospitalization based on the four indicators: gait speed, stride length, cadence, and spatial symmetry ratio. Spatial symmetry ratio was calculated by dividing the step length of the paretic limb by that of the nonparetic limb. The changes in gait performance were calculated using the following formula, where improvement is described as positive:


Furthermore, to investigate whether the timing of the MSC transplantation and subsequent rehabilitation affected functional recovery, the correlation between the changes in gait performance and the number of days to the MSC transplantation and rehabilitation onset was examined.
MEG analysis
MEG analysis was carried out with a seed-based rs-FC design using MATLAB R2022a (Mathworks, Natick, USA) and the Brainstorm software. 17 Recorded data were segmented into 30 nonoverlapping 10-s epochs, and artifact-contaminated epochs were manually detected and excluded from the analysis. 18 The obtained data were projected on the default 3D brain model. Seed location was defined around the primary motor areas (M1) of lower limbs in both hemispheres, and M1 seed-based rs-FC was estimated using amplitude envelop correlation (AEC) analysis. AEC was calculated by correlating the amplitude envelopes of two oscillatory brain activities, defined as the absolute value of the Hilbert transform of a cortical oscillation, and can detect synchronization between functional brain networks within frequency bands.19–21 In the present study, the Hilbert transformation was applied to the filtered signals of alpha (8–13 Hz) and beta (13–25 Hz) bands. High AEC values indicate synchronous amplitude envelope fluctuations between oscillations.
To compare connectivity in each brain region, the brain region was divided into 68 regions (34 regions for each hemisphere) using the Desikan–Killiany atlas. 22 The mean connectivity between bilateral M1 and each brain region was calculated and compared before and after hospitalization. In addition, the correlation analysis between the amount of changes in gait performance and neurological data was conducted to examine whether the changes in rs-FC contributed to behavioral improvement.
Statistical analysis
SPSS Statistics software version 28 for Windows (IBM Corp., Armonk, NY, USA) was used for statistical analyses. Data are presented as the mean ± SD, and the significance level (P value) was set as less than 5%. The distribution of data for normality was examined using the Shapiro–Wilk test. Depending on the normality of data, the paired t-test or Wilcoxon signed-rank test was applied to compare indices related to gait performance and rs-FC before and after hospitalization. For the correlation analysis, Spearman’s rank correlation coefficient was applied to the association between changes in gait performance and the number of days to MSC transplantation and rehabilitation onset, and Pearson’s correlation to the association between the changes in gait performance and rs-FC.
Results
After hospitalization, cadence and spatial gait symmetry ratio were significantly improved (Fig. 2). However, individual differences were observed in the size of changes. The correlation analysis was conducted using the time from onset to regenerative medicine and the time from transplant to rehabilitation as factors. Significant negative correlation was found between the time from transplant to rehabilitation and the changes in the symmetry ratio (r = −0.79, P < 0.05) (Fig. 3).

Changes in gait parameters before (pre) and after (post) the session. n = 7, *P < 0.05, **P < 0.01.

Scatter diagrams showing between the gait parameters and timing of the transplantation
Figure 4 shows a representative data of M1 seed-based rs-FC in the beta band (ID 07). Spatial distribution from the nonlesioned M1 was centered on the sensorimotor area, while the distribution from the lesioned M1 tended to spread widely to the parietal and occipital regions in the presession. However, in the presession, the distribution from the lesioned M1 tended to converge around the sensorimotor area.

A representative data of rs-FC analysis comparing presession to postsession (ID07). Spatial distribution of lesioned (left) and non-lesioned (right) M1 seed-based rs-FC correlations in the beta band.
Grand averaged changes in rs-FC between both M1 and each of 68 brain regions are shown in Figure 5 (alpha band) and Figure 6 (beta band). The connectivity from the lesioned M1 in the alpha band tended to be higher than those from nonlesioned M1. Though no significant differences were found due to high variability, the connectivity in the frontal, parietal, and temporal was tended to decrease after the hospitalization (Fig. 5). On the contrary, significant decrements were observed in the beta band between the lesioned M1 and multiple brain regions (e.g., both frontal areas, ipsilateral postcentral gyrus, contralateral temporal areas, and both rostral anterior cingulate gyrus), and few significant decrements were observed decrement between the nonlesioned M1 and other regions (Fig. 6).

Connectivity between M1 and each brain region in the alpha band. The brain regions were divided into 68 areas by using Desikan–Killeny atlas. The black circle indicates the presession, and the red circle indicates the postsession.

Connectivity between M1 and each brain region in the beta band. The black circle indicates the presession, and the red circle indicates the postsession.
To examine the relationship between the improvement in the gait function and cortical functional connectivity, we examined the correlation between the amounts of changes in the symmetry ratio of bilateral step length and rs-FC from the lesioned M1 and found significant negative correlations in the five brain regions (ipsilateral para central lobule [PCL], r = −0.88, P < 0.01; contralateral PCL, r = −0.79, P < 0.05; ipsilateral inferior parietal gyrus, r = −0.91, P < 0.02; ipsilateral isthmus cingulate gyrus, r = −0.77, P < 0.05; ipsilateral pars orbitalis gyrus, r = −0.92, P < 0.01) (Fig. 7).

Scatter diagrams showing significant negative correlation between the changes of symmetry ratio and rs-FC in the beta band between lesioned M1 and each brain region. rs-FC, resting state-functional connectivity.
Discussion
Recently, the utility of applying rehabilitation protocols and principles together with regenerative medicine has been proposed toward the goal of optimizing functional recovery through tissue regeneration, remodeling, or repair. 5 The effective combination of regenerative medicine and rehabilitation is suggested to promote the activation and preservation of transplanted cells; activate and preserve recipient cells; and promote tissue regeneration. 23 Numerous studies have been conducted to verify the combined effects of regenerative medicine and rehabilitation using animal models of central nervous system diseases, such as cerebrovascular disorders and spinal cord injuries (SCI), and it has been reported that the combination of the two therapies has a synergistic effect on functional recovery.3,4,24,25 Their translation to human treatment is eagerly anticipated, but only a few clinical results have been reported.26–28
This is the first study to summarize the effects of rehabilitation in terms of motor and brain function on patients who received adipose-derived MSC transplantation in the chronic phase following cerebrovascular disease. After more than 2 months of gait-focused rehabilitation using an ankle-assistive robot, improvements in gait function and plastic changes in the cortical functional connectivity were observed.
Tashiro et al. suggested that the main roles of rehabilitation following regenerative medicine for SCI patients were categorized as conditioning/reconditioning, functional training, and physical exercise, all of which are indispensable for enhancing functional recovery.29,30 Conditioning/reconditioning is especially important in the chronic phase because of the long deconditioning period. Then, functional training is a core element of rehabilitation after regenerative medicine, and physical exercise is thought to act to upregulate neurotropic factors. 30 It was reported that the quality and quantity of rehabilitation influenced the long-term outcome in patients with SCI who underwent olfactory ensheathing cells transplantation. 26 Although these studies refer to patients with SCI, we believe it is also applicable to cerebrovascular disease, a central nervous system disorder.
During hospitalization, each patient received conditioning approaches to control spasticity in their lower leg muscles, followed by daily robot-assisted gait training as one of the functional training and physical exercise approaches to improve their gait function. The ankle assistive robotic AFO used in the present study has been reported to be useful in facilitating appropriate gait strategies for each patient, particularly in increasing anterior propulsion force and weight bearing of the paretic limb.13–15 The robotic control in the present study was set to increase anterior propulsion force during the stance phase, and sufficient push-off motion during the preswing phase because strategies that increase propulsion force on the paretic limb were considered important to improve their gait function. 31 As a result, the cadence and the spatial symmetry ratio of the step length were significantly improved after the hospitalization, which were affected by the propulsion force 32 and the weight bearing on the paretic limb. 33
Several studies have reported the effects of MSC therapy on chronic stroke animal models, although these are far less common than those reported in the acute phase. The primary therapeutic mechanism of MSC injection in the acute phase is thought to be neuroprotection, 34 whereas in the chronic phase, it has been considered to induce vascular stabilization and neural plastic change involving the elevation of the neurotrophic factors.35,36 In other words, transplantation of MSCs in the chronic phase is expected to lead to functional improvement. Thus, it is important to implement appropriate rehabilitation as soon as possible after MSC transplantation. Interestingly, the improvement of the symmetric ratio in both step lengths was significantly correlated with the start of rehabilitation following MSC transplantation in the present study. On the contrary, no significant correlation was found between the timing of MSC transplantation and each gait parameter. Previous studies have reported that the earlier the timing of cell transplantation, the better the transplantation effect. 37 However, since the present study was conducted on patients in the chronic phase more than 6 months after the onset of the disease, there would be no significant difference in the subsequent rehabilitation effects.
Rs-FC has attracted attention as an indicator reflecting cortical function. It has been reported that patients with damage to the corticospinal tract might be able to perform upper limb movements compensatively by increasing rs-FC in the alpha band between bilateral motor cortices. 12 Another study has reported that rs-FC in the alpha band between bilateral M1 was correlated with their motor function in stroke patients. 11 Therefore, rs-FC in the alpha band might play a complementary role due to plastic changes in the brain, which may lead to improvement of movement. On the contrary, several studies have indicated that the rs-FC in the beta band between M1 and other brain regions reflected motor learning ability.18,38,39 Sugata et al. assessed the connectivity between the contralateral M1 of upper limb and other brain regions before motor learning in 53 healthy subjects and showed that the subjects with strong beta-band connectivity to the left superior temporal gyrus, bilateral sensorimotor regions, inferior frontal gyrus, and parietal areas had poor motor learning index. 18 These brain regions are involved in the theory of mind and default mode network (DMN), which might have inhibited motor learning because of the strong self-related and internal processes. Mary et al. also found that decreased coupling between the sensorimotor network, the cortico-striato-cerebellar network, and DMN was associated with better motor learning in both young and elderly subjects. 39
The present study evaluated rs-FC from both M1 of the lower limb in stroke patients before and after hospitalization. Though the alpha-band connectivity was not changed significantly, the beta-band connectivity from the lesioned-M1 was significantly decreased in both frontal, ipsilateral postcentral, contralateral temporal, and both rostral anterior cingulate regions. Since these brain regions are part of the DMN,40,41 we speculated that the improvement in motor function due to rehabilitation might have attenuated the cortical functional connectivity associated with the internal processes.
Furthermore, the relationship between the improvement in motor function and changes in brain connectivity was examined, and significant negative correlations were found between the improvement in changes in the symmetry ratio and the lesioned M1-based rs-FC to the ipsilateral brain regions associated with DMN (inferior parietal lobule, isthmus cingulate gyrus, and pars orbitalis) and both PCL. PCL controls motor and sensory innervations of the contralateral lower extremity. 42 The finding of a negative correlation in both PCL appears to be contradictory, but this phenomenon may be explained by the degree of contribution of brain activity to the process of gait recovery. Asymmetrical activity in the sensorimotor, premotor, and prefrontal cortices was observed depending on the severity of gait disturbance, but these activities were decreased as gait ability was improved. 43 Another study showed significant reductions in the sensorimotor cortex activity under body weight support treadmill training conditions. 44 The significant negative correlation in the present study could be explained by a hierarchical control including central pattern generators and supraspinal multiple motor centers, such as the subthalamic and brainstem locomotor regions. The reduction in effort for the gait associated with functional improvement may have decreased the rs-FC between M1 and PCL.
The present study revealed positive effects on gait function and cortical functional connectivity of the intensive gait-focused robotic rehabilitation for chronic stroke patients after transplantation of adipose-derived MSCs. The shorter the time between transplantation and the start of rehabilitation, the greater the degree of improvement in gait symmetry, indicating that rehabilitation should be received immediately after transplantation. In addition, changes in the cortical functional connectivity were also observed, suggesting that rehabilitation after the regenerative medicine might induce plastic changes correlated with DMN and sensorimotor network. However, the present study has several limitations. First, the small number of patients undoubtedly restricts the strength of our conclusions. Second, rehabilitation approaches other than robot-assisted walking were not standardized across the patients. Third, no significant changes were found in the M1 seed-based rs-FC in the alpha band. Finally, since we focused on only the patients who had received MSC transplantation in the present study, future group comparisons should clarify whether this rehabilitation approach after regenerative medicine is more effective than the controlled patients.
Footnotes
Acknowledgments
The authors thank all of the subjects for their voluntary participation in the present study. The authors thank Innoshima Medical Associate Hospital “RE-Gait Center” for their cooperation and patient recruitment.
Author Disclosure Statement
L.Y. is a director of Space Bio-Laboratories Co., Ltd (SBL), and Y.K. is the president of SBL, but they did not contribute to the measurement and analysis of the data. The potential conflicts of interest associated with this study have been approved by the Conflict of Interest Management Committee of Hiroshima University. By regularly reporting research progress to the Conflicts of Interest Management Committee, we will maintain fairness regarding the interests of this study.
Funding Information
No funding was received for this article.