
Abstract
Huntington’s disease (HD) is a progressive neurodegenerative disorder characterized by motor dysfunction, cognitive decline, and psychiatric disturbances. It is caused by the abnormal expansion of cytosine-adenine-guanine triplet repeats in the HTT gene, leading to the production of mutant huntingtin (mHTT) protein. This protein contributes to neuronal dysfunction and cell death, particularly in the striatum and cortex. The review examines recent research focused on identifying and assessing potential biomarkers of HD, emphasizing the use of peripheral fluids and tissues as sources of biomaterials. Among the reviewed biomarkers, neurofilament light chain and mHTT emerge as robust indicators of disease progression, while combined biofluid and imaging biomarkers show promise for improving prognostic accuracy. These biomarkers offer insights into key pathological features of HD, such as oxidative damage, mitochondrial impairments, and persistent inflammatory responses. The incorporation of diverse biomarkers, including those from peripheral fluids and tissues, holds great promise for improving the diagnosis and management of HD. A well-defined and validated biomarker panel could significantly enhance clinical outcomes by facilitating early detection, monitoring disease progression, and evaluating therapeutic efficacy. Ultimately, this progress could accelerate drug development and lead to more effective treatment strategies for HD.
Introduction
Huntington’s disease (HD) is a rare neurodegenerative disorder (ND) of the central nervous system (CNS) that is characterized by dementia, psychiatric impairments, and unintentional choreatic movements. 1 Exon 1 of the HD gene’s coding region contains a prolonged cytosine-adenine-guanine (CAG) repeat, which causes the hereditary autosomal dominant disorder. According to Willant et al., the number of CAG repeats instability affects the likelihood of developing HD: Fewer than 35 repeats instability indicates a very minor risk, 36–40 repeats indicate a moderate risk, and more than 40 repeats indicate a serious threat. 2
Roughly 1 in 10,000 people have this illness. The N-terminal region of mutant huntingtin (mHTT) contains a lengthy polyglutamine (PolyQ) stretch that interferes with interactions with HTT-binding proteins and encourages protein aggregation. 3 There is currently no active rehabilitation to stop the disease from starting or progressing, and many symptoms do not respond well to medication. The irreversible clusters of the abnormal mHTT protein brought on by its proteolytic cleavage, which appear as identifiable enclosures in the cytoplasm and nucleus of affected cells, are among the most obvious cytological alterations. However, the exact mechanism by which the accumulation of harmful mHTT proteins occurs is unknown. 4 HD typically manifests as a combination of behavioral, cognitive, and motor symptoms. 5
Cognitive impairment has been identified as a significant contributor to debility in earlier studies. While not as widespread as motor and cognitive symptoms, emotional disorders and personality deviations are also common, albeit they tend to manifest less consistently. Scientists are now working on creating biomarkers that could allow for the evaluation of a person’s disease progression. Despite ongoing efforts, biochemical, cognitive, neuroimaging, and clinical biomarkers have yet to demonstrate consistent success in HD. Current research continues to evaluate their clinical applicability and aims to identify novel therapeutic approaches for the effective management of disease. 6
Pathophysiology of HD
HD is principally defined neuropathologically by damage to the cerebral cortex and striatum. 7 While medium-sized spiny neurons (MSNs) represent 90%–95% of total neurons in the striatum and predominant neurotransmitter is Gamma-Aminobutyric Acid. 8 The striatum has also numerous modulatory subcomponents, including cholinergic or GABAergic involvements from striatal interneurons and dopamine (DA) projections from the substantia nigra pars compacta.9–11 In the cortex area, the pyramidal neurons in layers III, V, and VI ultimately degenerate. Yet, striatal neuronal death could account for numerous symptoms at the later stages of HD. 7 The development of neuroimaging techniques has greatly advanced our understanding of HD pathophysiology by enabling correlations between changes in the structure of the brain and the emergence of cognitive deficits in processes such as focus, active memory, and decision-making.12,13
Multiple pathological cascades are initiated by the dysfunctional and detrimental expansion of the mHTT protein’s function, leading to neuronal fatalities. As in previous studies, the first pathogenic mechanism examined was excitotoxicity. The development of HD has been linked to aberrant downstream signaling, which causes hypersensitive striatal postsynaptic glutamate receptors and excessive glutamate receptor activation through cortical inputs. 14 The main sources of glutamatergic input to the striatum are the cortex and, most significantly, the thalamus. To meet their robustness requirements, neurons primarily rely on mitochondrial oxidative phosphorylation (OXPHOS). The electron transport chain (ETC), which is embedded in the inner mitochondrial membrane (IMM), is a series of protein complexes that transport protons from the mitochondrial matrix into the intermembrane space. Compact forms of flavin adenine dinucleotide and nicotinamide adenine dinucleotide, which are produced during the Krebs cycle, supply electrons to these complexes. The potential gradient formed across the IMM facilitates the synthesis of ATP in the final stage of OXPHOS. 15
One important modulator of mitochondrial transport is the amount of calcium in the cytosol. The movement of mitochondria is slowed or stopped by an increase in cytosolic Ca2+.16,17 Furthermore, even in healthy conditions, 2% of electrons “leak” from the ETC to produce reactive oxygen species (ROS), making mitochondria a significant source of ROS. Mitophagy is a specialized type of autophagy that eliminates damaged mitochondria. 18 When phosphorylated at serine 133, the transcription factor CREB (cAMP response element-binding protein), which belongs to the leucine zipper family, binds to the coactivators p300 and CBP (CREB-binding protein) to activate transcription. The movement of CBP’s acetyltransferase is disrupted in HD; it becomes trapped in CAG aggregates and runs out of its typical nuclear location. Furthermore, mHTT inhibits CREB phosphorylation, which in turn reduces the number of transducers of regulated CREB activity seen in HD cellular models, postmortem HD striatal tissue, and the striatum of a transgenic mouse model. 19
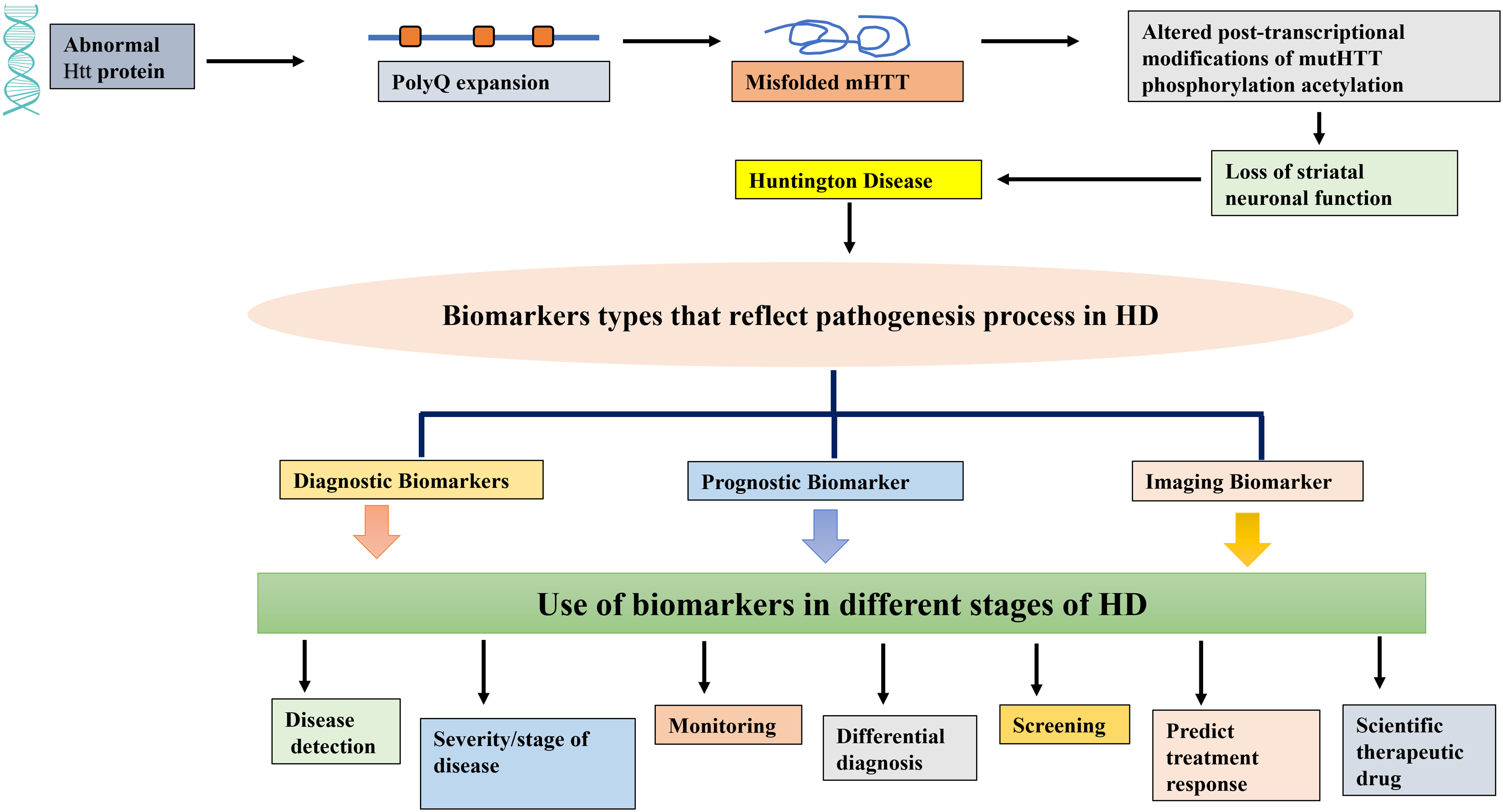
The development of brain-derived neurotropic factor (BDNF) may be hampered by the reduced CREB signaling activity and by the suppression of PGC 1-α.20,21 Cortical neurons produce BDNF, which is then transported via the cortico-striatal pathway to MSNs in the striatum.22–25 The figure depicts the interplay of transcriptional dysregulation, mitochondrial dysfunction, and synaptic failure, which results in HD. The disturbance of cellular pathways brought on by mHTT protein causes neurodegeneration in the striatum (Fig. 1).

Diagram showing the cellular pathophysiology of Huntington’s disease in presynaptic and postsynaptic neurons. The diagrammatic summary illustrates that mHTT perturbs multiple intracellular signaling pathways, culminating in neurodegeneration. HTT gene inside the nucleus undergoes transcription to form HTT RNA. Due to a cytosine-adenine-guanine (CAG) trinucleotide repeat expansion in the HTT gene, this RNA encodes an mHTT. Precisely, mHTT inhibits the activity of PGC 1-α, a critical regulator of mitochondrial biogenesis and cellular energy homeostasis. This suppression results in mitochondrial dysfunction, reduced ATP production, and elevated oxidative stress. Simultaneously, mHTT impairs the phosphorylation of CREB, thereby downregulating the expression of BDNF, which is essential for neuronal survival, synaptic plasticity, and differentiation. Additionally, mHTT inhibits histone acetyltransferase enzymes responsible for chromatin remodeling and transcriptional regulation, leading to epigenetic dysregulation and further transcriptional repression. These pathological mechanisms collectively contribute to the progressive loss of striatal neuronal function, with a particular impact on the medium spiny neurons of the basal ganglia, a hallmark of HD pathophysiology. BDNF, brain-derived neurotrophic factor; CREB, cAMP response element-binding protein; HD, Huntington’s disease; mHTT, mutant huntingtin protein; PGC-1α, peroxisome proliferator-activated receptor gamma coactivator 1-alpha.
Importance of Biomarkers in Neurodegenerative Diseases
Repetitive deprivation of nerve cells leads to structural damage and malfunction, resulting in NDs. Numerous NDs, including HD, Alzheimer’s disease, Parkinson’s disease, multiple sclerosis, and amyotrophic lateral sclerosis, have been found to be triggered by factors that range from molecular to systemic. 26
With the exception of HD, these conditions are becoming more common, mostly due to the aging population. Currently, imaging tools are used in conjunction with clinical evaluation to diagnose the majority of disorders. 27 In order to facilitate the quick, affordable, and precise detection, screening, and staging of NDs, significant efforts are being made to identify the biochemical markers present in biological fluids. Advancements in early detection are expected to improve existing treatment options and may ultimately lead to the discovery of a cure for these diseases. 28 Reliable biomarkers are essential for advancing new therapeutic strategies, selecting appropriate patients for clinical trials through enrichment or stratification methods, and demonstrating clinical efficacy by accurately measuring treatment effects. These biomarkers may include a wide range of molecules such as nucleic acids, lipids, proteins, peptides, and metabolites, which can be identified using established proteomic and genomic techniques. 29
In this study, we want to draw attention to the limitations and current status of HD diagnosis. This also provides details on the biomarkers’ sensitivity, specificity, and early diagnostic potential, which can be assessed using techniques based on their molecular characteristics, which include a variety of substances, such as proteins and nucleic acids. We will discuss the various classifications and applications of biomarkers, with a focus on their application in the creation of HD drugs.
Types of Biomarkers
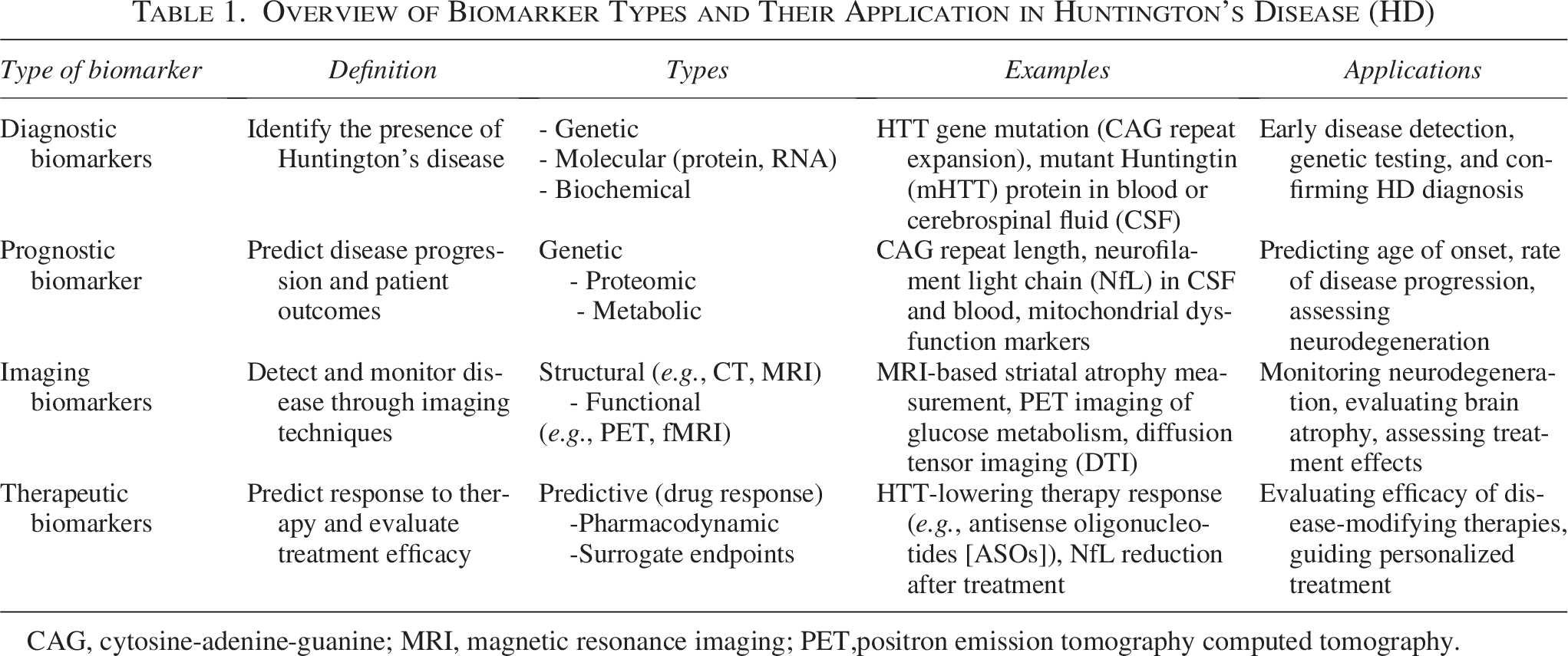
Once the physical symptoms that are typical of HD start to appear, a medical diagnosis can be made, as in Figure 2. Since HD has a genetic etiology, genetic testing can confirm it in situations where there is no family history of the condition. The majority of possible carriers of the familial mHTT gene decline to be tested for a variety of reasons, including career, family planning, psychology, and the lack of treatments that alter the disease. Genetic testing is therefore commonly carried out following the onset of clinical symptoms resembling chorea. 30
Schematic representation of biomarker types reflecting the pathogenesis of HD and their application across different disease stages.
To assess the different facets of the HD phenotype, a number of standardized clinical tests and rating scales have been developed. Four primary domains impacted by HD can be measured by the Unified Huntington Disease Rating Scale (UHDRS), possibly in conjunction with additional quantitative clinical, neuroimaging, and biochemical evaluations. 31 A biochemical marker could be considered the perfect biomarker since it combines the benefits of clinical testing and neuroimaging, including high sensitivity, low cost, and high throughput. 32 Table 1 gives a summary of the various types and uses of HD diagnostic, imaging, prognostic, and therapeutic biomarkers.
Overview of Biomarker Types and Their Application in Huntington’s Disease (HD)
CAG, cytosine-adenine-guanine; MRI, magnetic resonance imaging; PET,positron emission tomography computed tomography.
Diagnostic Biomarker
Blood-based biomarker
Biomarkers can be standard biological progressions, pharmacological comebacks to therapeutic involvement, or recurring indications of pathogenic processes. 33 It has been suggested that blood-based biomarkers can either partially replicate concurrent central neuropathogenic processes or instantly identify the peripheral pathophysiologic changes linked to HD. As previously stated, mHTT is crucial to the pathophysiology of HD and results in a number of harmful changes that harm and kill neurons.34,35 Furthermore, the precise measurement of mHTT concentration in cerebrospinal fluid (CSF) samples is permitted by ultrasensitive immunoassays, which have been authorized for use in clinical trials. 36 The severity and stage of HD are correlated with the amount of mHTT in the patient’s CSF, and the severity of the disease is assessed using several factors, including the patient’s age at onset, disease burden score, UHDRS scale, and motor score.37,38
Blood-based biomarkers are of particular interest in HD research because they offer a less invasive method for monitoring disease progression and evaluating treatment response. Several promising blood biomarkers have been identified in recent years, which may prove valuable in both clinical management and therapeutic trials. Notably, HD can potentially be detected through blood biomarkers even before the onset of clinical symptoms. 39 For instance, neurofilament light chain (NfL) has emerged as a key marker. Several studies have shown that NfL is increased in the CSF of patients undergoing HD and is associated with clinical severity.40–42 Our prior argument supports the notion that blood biomarkers such as mHTT, NfL, inflammatory biomarkers, and miRNAs offer a more holistic approach to understanding the etiology of the diseases. There are several biomarkers that can improve specificity in diagnosis and tailor treatment regimens to the patient. We go into great detail about the different kinds of blood-based biomarkers here.
mHTT levels and aggregation
The progressive and fatal combination of behavioral, cognitive, and motor symptoms that define HD is caused by an mHTT extended PolyQ tract, which causes neuronal dysfunction and death.6,43 In clinical trials of HTT-lowering treatments, measuring mHTT in the CSF would be useful as a pharmacodynamic biomarker. CSF mHTT may prove to be a useful marker in the future for tracking the course of HD and predicting its phenotype. 36
MicroRNAs in HD pathology
According to Tafrihi and Hasheminasab (2018), microRNAs (miRNAs) are a family of endogenic noncoding small RNAs that have been preserved through evolution. They regulate the expression of approximately 90% of the body’s genes and are essential for cell division, senescence, and propagation. 44 An increasing body of research has demonstrated that dysregulated miRNAs are linked to HD. 45 Additionally, studies have revealed that several key neuronal miRNAs, such as miR-9, miR-124, and miR-132, were less abundant in the brains of HD patients and mouse models. 46 This reduction could have an adverse effect on neuronal function and miRNA regulation. miRNA microarray analysis was used to display complete miRNA expression patterns in three HD mouse models (Lee et al. 2007).
In addition, the R6/2 HD transgenic mice expressed the N-terminal exon 1 of a human mHTT, and the YAC128 transgenic mice expressed a full-length mHTT as seen in patients with HD. 47 Langfelder et al. conducted a review that the striatum had the utmost differentially expressed miRNAs, followed by the cerebellum, hippocampus, and cerebral cortex, when looking at different brain regions of HD model mice with endogenous HTT that had increased CAG length. They also showed that the expansion of the HTT CAG repeat is potentially correlated with mir-212, mir-132, and mir-128, suggesting that these miRNAs may be involved in modulating the different susceptibilities of CAG length expansion. 48
Prior studies have found that small vesicles or direct delivery of miRNAs into body fluids such as peripheral blood, serum, plasma, saliva, and urine have been observed to either bind to proteins or other molecules. To elaborate, miRNAs can bind to plasma and high-density lipoprotein to form stable structures in the peripheral circulation. As miRNAs can survive extracellularly, they may serve as useful biomarkers to detect HD in the peripheral circulation. 49
Biomarkers of oxidative stress
Different studies suggest that there are abnormal connections between the mitochondria in the neurons that are developing defects and producing excessive amounts of free radicals and mHTT.50,51 When free radicals are produced in excess, they can react with macromolecules like proteins or unsaturated lipids, disrupt multiple neural targets, and reduce ATP synthesis. Thus, mitochondrial metabolic dysfunction and interactions between ROS and neuronal components such as DNA may be the cause of the oxidative byproduct accumulation caused by changes in neuronal loss in HD patients, particularly in the neostriatum and to a lesser extent in the cortex. Prior research found that the peripheral blood of HD patients had increased levels of lipid peroxidation byproducts, high concentrations of substances that damage proteins and DNA due to oxidative stress, and changed levels or activity of a number of endogenous enzyme antioxidants.52–55 In particular, the degree of oxidative stress caused by ROSs oxidizing guanine may be correlated with the amount of 8-hydroxy-2′-deoxyguanosine in blood and urine. DNA damage has been proposed as a robust and dependable peripheral clinical HD biomarker.56,57
Neuroinflammatory biomarkers
The postmortem examinations that show a strong correlation between inflammation and HD progression, including the stimulation of inflammatory cytokines, chemokines, and the activation of the accompanying system, are the source of neuroinflammation in HD. Björkqvist et al. found that HD patients’ plasma had higher concentrations of a number of cytokines, such as IL-1β, IL-4, IL-6, IL-8, TNF-α, and IL-10, and that their striatum had higher levels of IL-6, IL-8, and TNF-α. 58
Patients with HD had significantly lower plasma levels of IL-4, a gauge of T-helper-2 cell responses, than healthy controls. However, there were no discernible differences in the plasma levels of IFN-g, IL-1b, IL-2, IL-6, IL-8, IL-10, IL-12p70, IL-13, or TNF-α in HD patients. Particularly, C-C motif chemokines such as CCL2, CCL4, CCL11, CCL13, and CCL26 are markedly elevated in plasma from HD patients. CCL11 and similar chemokines could potentially have a direct impact on the neurodegenerative process of the CNS. 59 According to Wild et al., the HD group from an initial cohort of 65 HD patients had higher levels of CCL11 and CCL26 after comparing the plasma levels of cytokines in two distinct groups of HD patients. 60
Imaging Biomarkers
Neuroimaging technologies such as magnetic resonance imaging (MRI) and functional MRI (fMRI) have been greatly important at the stage of disease (asymptomatic and symptomatic) for detecting structural and functional differences in the brain. These techniques offer better sensitivity, high temporal and spatial accuracy, and the capacity to record both dynamic and structural information when compared to other tomography methods. 61 When used in clinical studies that collect adequate samples, these biomarkers produce good results, and they play significant roles in the early stages of diagnosis and in measuring the progression of the disease. 62
Phosphodiesterase (PDE) is prominently involved in the pathophysiology of HD, and damage to postsynaptic dopaminergic neurons results in the loss of MSNs. The promotion of neuronal existence and the facilitation of cell signal transduction depend on this intracellular enzyme. PDE10A is essential for controlling dopaminergic signaling and is mostly expressed in the striatum. In HD animal models, studies have demonstrated that mHTT reduces striatal PDE10A expression, with this decrease seen even prior to the onset of symptoms.63,64
There are various methods for analyzing a brain scan. For example, whole-brain analysis looks at areas that are known to be pathologically affected, while region-of-interest (ROI) analysis is more objective, exploratory, and independent of prior assumptions. ROI studies are especially helpful for research because they also usually show a high degree of sensitivity in identifying assembly modifications and monitoring changes over time. 65
All parts of the brain can be exploratorily examined through whole-brain analysis. It is widely used in HD research to measure brain size, and the most widely used technique is voxel-based morphometry (VBM). White matter, gray matter, and CSF volumetric differences between groups can be measured thanks to VBM. It has also been used to correlate other biomarkers with brain volume. 66
Structural MRI: Brain atrophy and volume changes
Significant and progressive striatal volume loss is the most reliable result in HD. Research has shown that in patients with mild to moderate HD, the average putamen volume decreases by nearly 50%–54%, and the caudate volume decreases by roughly 28%–29%. 67 Early-stage HD patients with total functional capacity scores of I and II have also been found to exhibit striatal atrophy. 68 According to Fox and Raichle (2007), striatal atrophy has also been found in premanifest HD gene carriers, even those thought to be 15–20 years away from the anticipated onset of symptoms. 69
The length of the CAG repeat expansion, the severity of the disease, and the age at onset are all associated with the degree of striatal volume loss. 70 While Mini-Mental Status Examination) scores and other cognitive evaluations show an inverse relationship with the notch of caudate volume reduction, greater putamen atrophy is linked to more severe motor impairment.67,71
The goal of the multicentre longitudinal study TRACK-HD is to identify sensitive and trustworthy biomarkers in patients in the early stages of the disease, as well as in people with the HD gene before symptoms appear. 72
fMRI: Connectivity and brain activity
There is mounting evidence that the severity of clinical symptoms may also be influenced by neuronal dysfunction and brain circuit remodeling, which may start early in HD and even before obvious neurodegeneration. By identifying blood flow changes associated with neural activation, functional neuroimaging techniques—like fMRI—provide a dynamic perspective on brain activity and shed light on patterns of neuronal function.73,74
Using fMRI and assemblage autonomous constituent analysis, Unschuld and colleagues examined functional connectivity networks in both premanifest HD gene carriers and healthy controls during a Stroop color-naming task. They found a connection between these networks and symptoms of depression. Abridged activity in the ventromedial prefrontal cortex was more strongly associated with depressive symptoms in premanifest HD gene carriers than in healthy controls. 75
Using a Tower of London fMRI task, a similar research group discovered a significantly weaker efficient connection between the left premotor cortex and the medial prefrontal cortex in a cluster of premanifest HD gene transporters and early-stage HD participants. These results imply that reduced brain network connectivity reflects cognitive and emotional impairments even in the early stages of HD. Using resting-state fMRI, a technique that may provide insights into functional changes without compromising cognitive abilities necessary for task performance, recent studies have concentrated on functional brain connectivity resting-state patterns.69,76
Positron emission tomography imaging: Glucose metabolism and dopaminergic function
A useful imaging technique in nuclear medicine, positron emission tomography computed tomography (PET) has several claims in the field of neurology. PET has been widely used in neuroscience research in recent years to examine the pathophysiology of a variety of neurological conditions, including HD, AD, and PD. The only technique that allows for three-dimensional visualization of the human brain is PET. PET-CT scanners, which are sensitive to radioactivity, and PET radioligands, which are metabolically active molecules classified with radioactive isotopes and required for PET imaging, are used to accomplish this. 77
It can be used to assess the dopaminergic role and, in turn, the degree of basal ganglia dysfunction in HD by targeting both postsynaptic and presynaptic terminals. PET radioligands such as 11C-raclopride and 11C-SCH23390 are used for a postsynaptic terminal approach and are selective for visualizing the dispersal of D2 and D3 receptors, as well as D1 and D2 dopamine receptors, respectively. Both evident and premanifest HD patients have shown decreased availability of striatal postsynaptic D1, D2, and D3 receptors, according to human PET studies. HD patients were the first to show that the D1 and D2 receptors required in the caudate and putamen to the standard assortment had decreased by more than 30%. 78 Additionally, a decrease in 11C-raclopride binding in these areas causes changes in atrophy, as determined by volumetric MR imaging. 79
Furthermore, the membrane-spanning protein known as the dopamine transporter (DAT) is widely expressed in the presynaptic dopaminergic terminals. The DAT absorbs dopamine, which is then reabsorbed from the synapse into the cytosol. The DAT is selectively bound by 11C-β-CIT in PET imaging, which results in a 50% decrease in DAT availability when compared to normal levels. 80 In another study, cerebral blood flow and glucose metabolism were used with PET using 18F-fludeoxyglucose (FDG). Research involving pre-symptomatic and symptomatic HD cohorts, assessed using standardized PET imaging with 18F-FDG (glucose metabolism) and H2-15O (cerebral blood flow), has shown a measurable annual decay rate in metabolic and perfusion markers. These findings suggest that brain hypometabolism emerges before overt clinical manifestations of HD.81,82
Diffusion tensor imaging (DTI), another promising biomarker, used through MRI, can quantify changes in tissue composition. Two quantitative DTI metrics that can capture the architecture of the gray matter as well as a measure of sufficiency for the white matter in the brain are axial diffusivity and fractional anisotropy. 83 The correlation among white matter neuronal loss, striatal atrophy, and cognitive function we speculate that a combination of structural image measures would be a worthwhile biomarker for HD. Furthermore, a more recent analysis documented a correlation between white matter abnormalities in the sensorimotor cortex and phenotypic decline in HD. As such image quantification difference could be helpful in forecasting precursor symptoms in asymptomatic individuals carrying the mHTT. 84
Prognostic Biomarker
CSF biomarkers
Blood, saliva, urine, and CSF are among the bodily fluids that produce peripheral biomarkers; of these, CSF has the highest chemical content and provides the best source of biomarkers from NDs. Furthermore, a great deal of research has been done on measuring the levels of CSF in blood and peripheral blood, specifically mHHT and NfL. 85 The presence of molecular biomarkers in HD patients’ CSF may improve prognoses, give a better picture of how the disease progresses, and facilitate treatment. CSF is a readily available biofluid whose molecular makeup reflects both structural and functional changes in the brain. This makes it a useful biofluid for evaluating biomarkers in neurodegenerative diseases, particularly HD. 86
The prolonged PolyQ tract that mHTT carries in HD causes neuronal dysfunction and cell death, which causes gradual degeneration and the advanced loss of motor, cognitive, and behavioral symptoms. 6 Therefore, measuring disease-related proteins in CSF is increasingly useful for diagnosing, tracking the progression of the disease, and directing treatment for a variety of neurodegenerative diseases, including AD, PD, and ALS.87–89
The caudate nucleus and putamen are the main areas affected by mHTT-induced toxicity in the CNS, which over time led to neuronal cell loss and significant regional atrophy in the basal ganglia cortex and the striatum. 90 Although it has clear limits, mHTT is a significant potential biomarker of interest. Because of its low concentration in biofluids, it can be difficult to distinguish between mHTT derived from the CNS and that derived from the peripheral nervous system. 91 However, complementary results have been obtained from clinical trials on soluble mHTT in blood. When mutant and total huntingtin proteins in leukocytes were measured using a time-resolved Förster resonance energy transfer (TR-FRET) immunoassay in 2012, it was found that patients with HD had only slight variations in their overall HTT levels. 38
Similarly, a 2013 study that used a homogeneous time-resolved fluorescence (HTRF) assay discovered a slow, inverse relationship between the progression of the disease and declining levels of mHTT, which may indicate HD phonoconversion. However, the test was not taken into consideration for broader practice due to technical issues. 92 Finally, in 2015, a different study demonstrated that mHTT in CSF could be measured using a femtomolar-sensitive single molecule counting (SMC) immunoassay. 93
The closure of mHTT in CSF has been used as a biomarker to evaluate treatment success in pilot studies based on Huntington-reducing drugs. Even though mHTT is clearly a contributing factor to HD, it might not be the most accurate single biomarker for assessing clinical status or monitoring the progression of the disease. Measuring the levels of mHTT, the main pathogenic agent, should be combined with other biomarkers, like NfLs, which show axonal impairment, in order to screen for disease progression and assess treatment options. The challenges of measuring peripheral mHTT and its hazy correlation with clinical signs and symptoms necessitate this. 36
Neurofilament light
There have been reports of potential biofluid markers in HD patients, and it has been shown that elevated plasma NfL concentrations reflect cortical degeneration and may be associated with symptoms of motor, cognitive, and neuropsychiatric disorders. 94 Byrne et al. 39 indicate that HD patients have higher baseline NfL levels in plasma and CSF prior to the onset of the disease, and that these levels have the ability to independently predict the onset, course, and eventual brain atrophy of the disease.
One of the primary structural elements of neuronal cells, neurofilament is crucial for preserving the size, shape, and form of neurons as well as the axonal caliber, which is necessary for preserving the morphological integrity of neurons and the appropriate transmission of nerve impulses along the axons. 95 It has been suggested that cytoskeleton destabilization may contribute to neuronal death and damage. 96
Additionally, the earlier study implies that white matter involvement with axonal degradation is the cause of an early event in HD pathogenesis. Early neuropil deprivation in the substantia nigra and external globus pallidus is seen in patients with presymptomatic disease. In a recent study, selective white matter development in the early stages of HD was observed using the DTI technique. 84
Thus, CSF studies have shown that HD has higher levels of NfL and tau, which may be biomarkers for the stage of the disease. The previous study concluded that because HD’s neurodegenerative process is too slow, neurofilament proteins that are not confined to plasma may break down before they have an opportunity to accumulate in a detectable manner. 97
Electrophysiological biomarkers
An extension of the brain’s electrical activity is electroencephalography (EEG). It is a noninvasive technique that could yield biomarkers at a fair price. Event-related potentials (ERPs) and EEGs are the most effective instruments for examining HD biomarkers. The data was obtained by recording billions of distinct excitatory and inhibitory postsynaptic possibilities using a surface electrode EEG attached to the scalp. These possibilities are influenced by the coordinated activity of the brain’s cortical and subcortical regions. ERP)signals are used to calculate the average number of EEG segments that are synchronized to a particular class of events. ERPs are thus brain voltage changes associated with specific progressions. Potentials produced by olfactory, tactile, auditory, and visual inputs are referred to as sensory ERPs in a variety of ERP categories. Additionally, voluntary movements are preceded and followed by the motor ERPs. 98
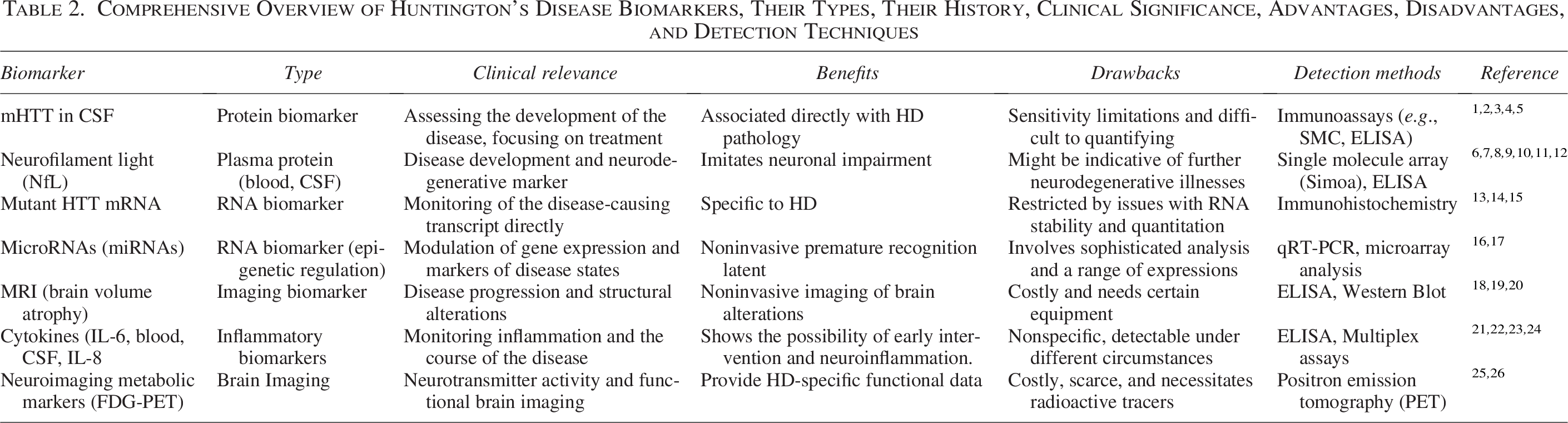
According to Bylsma et al., HD patients’ EEGs revealed a marked decrease in fresh and percent theta power as well as raw and percent alpha supremacy in the medial frontal region of the brain. 99 It is a quick, low cost, and easy way to assess subcortical disease. Quantitative electroencephalography (qEEG) is used to assess the severity of HD when motor dysfunction and subcortical dysfunction coexist. 100 The thalamocorticostriatal systems, which exhibit changes in the preclinical and early stages of HD, define brain oscillatory bustle, suggesting a plausible physiological link between qEEG biomarkers and the properties of mHTT reduction. 101 Table 2 provides a comprehensive summary of the various biomarkers and their types that have been investigated in HD research, along with details on their history, clinical significance, advantages, disadvantages, and detection techniques. Offering a more complete picture of the diverse biomarker landscape in HD, this in-depth review strengthens the emerging biomarker subsections and supports the potential applications of biomarkers in diagnosis, progression tracking, and therapy assessment (Fig. 3).
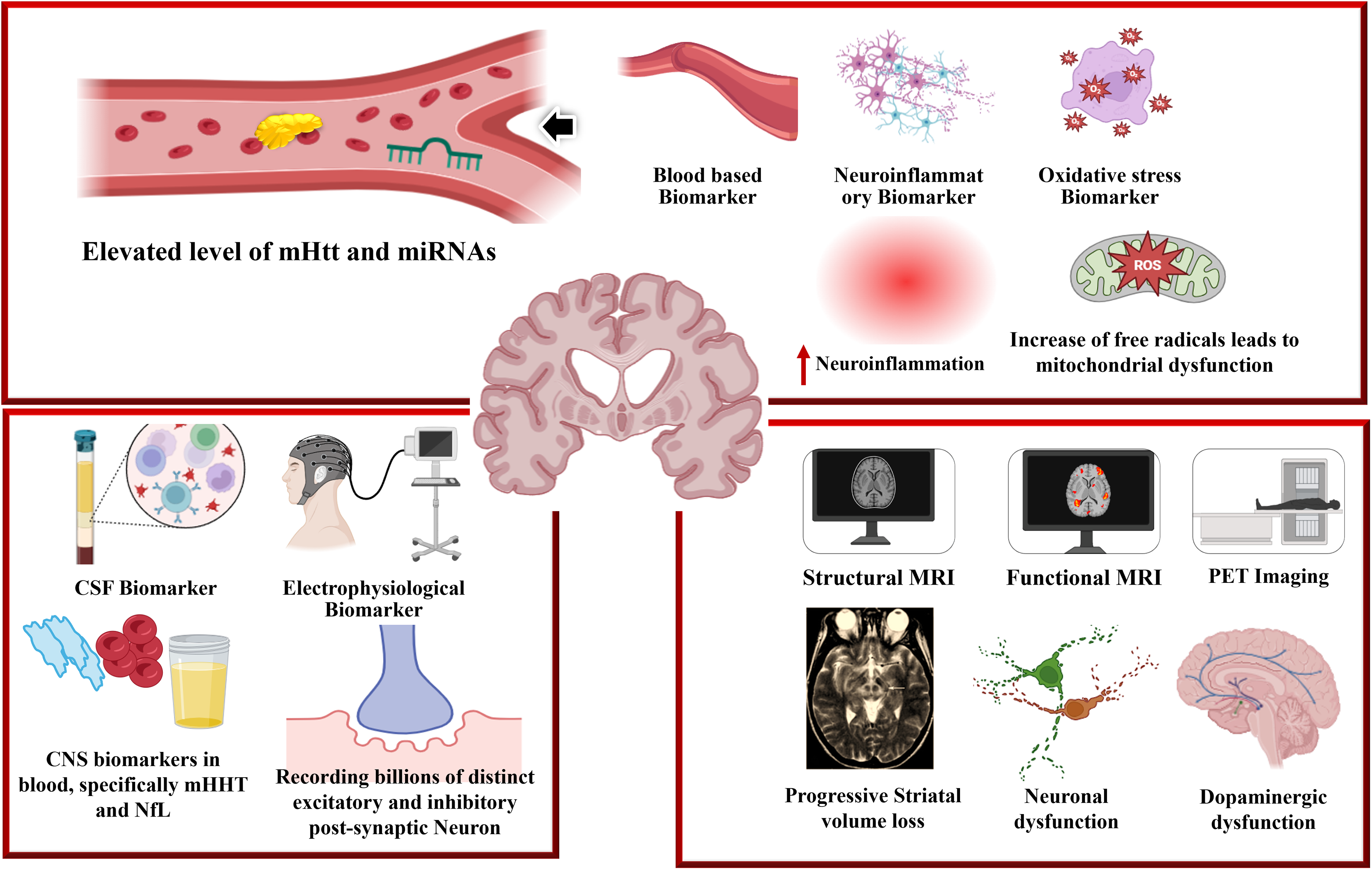
This diagram illustrates integrated peripheral and central biomarkers linked to HD pathophysiology. While neuroinflammatory and oxidative stress indicators indicate increased inflammation, increased ROS, and concomitant mitochondrial dysfunction, blood-based biomarkers reveal changed amounts of circulating miRNAs and mHTT. NfL and mHTT are two CSF biomarkers that show continued neurodegeneration. Excitatory and inhibitory neural signaling abnormalities are captured by electrophysiological biomarkers. Dopaminergic deficiencies, neuronal dysfunction, and increasing striatal volume loss are shown by neuroimaging modalities such as structural MRI, functional MRI, and PET. When taken as a whole, these multimodal indicators offer a thorough framework for tracking the course of the disease and assessing the effectiveness of treatments for HD.
Comprehensive Overview of Huntington’s Disease Biomarkers, Their Types, Their History, Clinical Significance, Advantages, Disadvantages, and Detection Techniques
Therapeutic Targeting Against Biomarkers in Preclinical Trial
Transgenic mouse models for HD, specifically R6/2 and zQ175, are frequently used in preclinical research.102,103 These models allow for the relatively rapid analysis of biomarkers from soon after birth until the onset of symptoms and replicate the characteristics of the disease seen in humans. 104
The R6/2 mouse, which has an enlarged CAG repeat sequence that starts in exon 1 of the human mHTT gene, shows extremely early onset of rapidly worsening symptoms. 105 The mHTT gene is present in the mouse genome of the zQ175 knock-in (KI) mouse model, which allows for a more gentle disease development that more closely resembles the progression of human disease,106,107 and qEEG makes it possible to identify disruptions in the brain network. QEEG in R6/2 and zQ175 mice, as well as tgHD and BACHD rats, has been covered in articles. Previous studies compared the data recorded from cortical or dural electrodes with the data recorded in wild-type (WT) mice during the sleep-wake cycle in order to analyze the qEEG results in R6/2 animals. 108
Kantor et al. performed an extension study and found behavioral changes and changes in qEG following administration of a hypnotic drug to a model of R6/2 mice. In addition, when comparing R6/2 mice with WT mice, the discrepancy between the two species was significantly higher in the former. 109 Fisher et al. analyzed sleep qEEG data from dural screw electrodes following sleep deprivation periods and found that sleep was fragmented and gradually decreased in duration. 108 Callahan and Abercrombie examined the oscillatory signals coming from the cortex and the subthalamic nucleus (STN) in anesthetized R6/2 mice using local field potentials (LFPs) and cortical recordings. In line with previous findings, they saw a decrease in absolute delta power and an increase in absolute beta and gamma power. Moreover, these researchers found reduced coherence between the STN and cortex in the delta frequency region during synchronized, but not desynchronized, cortical activity. 110 Additionally, there is a dose-dependent reduction in aberrant gamma oscillations with both zolpidem and amitriptyline. Additionally, they found that rapid eye movement (REM) sleep was abnormally high. 109
Since zolpidem increased absolute delta power in WT mice and did not disrupt the R6/2 model, it had no effect on WT mice for 6 hours, but it reduced REM sleep in R6/2 mice for at least 2 or 3 hours. In contrast, amitriptyline reduced the amount of REM sleep in the R6/2 and WT mouse models, respectively. During NREM sleep, it reduced the low incidence oscillatory power in both models. 108 Miller et al. performed extracellular recordings from transgenic mice and rats, focusing on neural spike activity in KI mice, rats with transgenic (TGHD) status, and rats with R6(1) and R6(2) status. The striatum of all models was recorded, as was the prefrontal cortex and primary motor cortex of R6 and KI mice. Moreover, LFP in the striatum of R6 + 2 mice were analyzed and revealed significant changes in spike activity. Significant variations in spiking activity occurred between the different models and their WT littermates. The changes included a decrease in firing rate, a decrease in the interspatial variance coefficient, a decrease in delta and theta relative superiority, and an increase in the intensity of the comparative gamma power LFP recordings from the R6 and 2 striatum at break. 111
Furthermore, several research groups are investigating the use of CRISPR/Cas9 technologies in preclinical studies for HD in order to eliminate prolonged CAG repeats, specific mutated HD alleles, incapacitate HD-associated alleles, or directly target the HTT gene, which will lower HTT levels generally. 112
Therapeutic Targeting Against Biomarkers in Clinical Trials
There is a lot of potential for new treatment modalities to be used as disease modifiers for HD. The pathways that generate mHTT, the primary cause of HD pathogenesis, are the focus of most of these strategies. RNA-targeted therapies that halt the production of mHTT at the posttranscriptional level include RNA interference (RNAi) and antisense oligonucleotides. These techniques work by cleaving, degrading, or inhibiting the transcription of mHTT. Targeting the underlying cause of HD, with a focus on lowering mHTT as a potential treatment strategy, has replaced the focus on identifying broad-spectrum and downstream progressions in recent years. 113
According to Rinaldi and Wood, 114 antisense oligonucleotides are short, single-stranded molecules made of chemically modified nucleotides that are designed to bind balancing to target mRNA sequences. Antisense oligonucleotides (ASOs) can either promote deprivation by endogenous enzymes like RNase H1 or inhibit the target RNA’s functions, which can lead to translation inhibition or changed RNA processing when they bind to their target mRNA. ASOs cannot penetrate the blood-brain barrier (BBB) and enter the CNS through administration. Clinical biomarkers are standardized clinical tests and rating scales that monitor the progression of different HD phenotypes, such as cognitive and motor decline. These tests rarely require sophisticated testing apparatus and are frequently inexpensive and simple to conduct. They can also provide neurobiological insights into HD and more accurately describe its phenotypic diversity. 115 ASOs have demonstrated the capacity to result in a long-lasting decrease in both HTT mRNA and its protein throughout the CNS in a variety of HD models. Even small reductions (more than 35%) have been associated with improvements in phenotype and survival, and reductions of more than 75% are achievable.116–118
Ionis Pharmaceuticals developed the allele-nonspecific ASO HTTrx, which targets both mutant and WT huntingtin. It is occasionally referred to as RG6042 or ISIS 443139. The first of its kind, the phase 1-2a, multiple-ascending-dose, randomized, double-blind clinical trial included participants with early-stage HD. Patients were assigned to receive either HTTrx or a placebo after being split up into five dose sets (10, 30, 60, 90, or 120 mg). The two highest dosages, 90 and 120 mg, did cause an unkind deterioration of 40%, but the experiment did not achieve the maximal steady-state drop in CSF mHTT. Preclinical pharmacokinetics and pharmacodynamics modeling indicate that a 40% reduction in CSF mHTT is linked to a 55%–70% decrease in cortical mHTT and a 20%–35% decrease in striatal mHTT. On the other hand, there is a 70%–85% decrease in cortical mHTT and a 35%–50% decrease in striatal mHTT for every 60% decrease in CSF mHTT.119,120
Another clinical study using RNAi techniques promotes specific mRNA degradation by utilizing innate, evolutionarily conserved cytosolic mechanisms. However, gene therapy methods must use viral vectors, such as the adeno-associated virus (AAV), to introduce RNAi because double-stranded RNA has slow diffusion and poor brain absorption. A phase 1/2 trial has been initiated by the biotechnology company UniQure to evaluate the safety, acceptability, and efficacy of a single AMT-130 dose administered once to HD patients.121–124 Voyager Therapeutics’ RNAi-based gene treatment VY-HTT01 uses a miRNA produced and delivered by an adeno-associated virus vector serotype 1 (AAV1) to target HTT mRNA for degradation. 125 YAC128 transgenic HD mice, which exhibit full-length human HTT with 128 CAG recurrences, showed strong striatal dispersal, reduced HTT masses, and improved motor and behavioral signs after receiving an intracranial injection of VY-HTT01, compact striatal HTT protein levels by 40%.126,127 Claims from clinical trials were rejected in late 2020, but they are still being examined because of problems with the chemicals, manufacturing, and control. 128
Furthermore, a different study tested the effectiveness of CRISPR/Cas9 in cell lines. In this study, three distinct fibroblast lines from HD patients had their expanded CAG duplications in exon 1 of the HTT gene targeted for effective deletion using a paired Cas9 Nickase method, which resulted in HTT inactivation. Nickases cause single-strand breaks, which increase selectivity and lessen off-target effects. Each treated cell line had a different length of CAG repeats, but they all displayed an approximate 70% reduction in HTT protein levels. 129 A technique that combined CRISPR–Cas9 with piggyBac transposon technology was able to successfully repair the mHTT allele in human-induced pluripotent stem cells derived from HD individuals, thereby curing phenotypic abnormalities associated with HD. 130
Novel Approaches
Few studies have been conducted on the use of genomic profiling in the search for disease biomarkers. A total of 322 transcripts were found to be altered in HD patients after mRNA expression analysis in peripheral blood samples. Consequently, 12 transcripts that could distinguish between controls, presymptomatic individuals, and patients were found.131,132 Additionally, the amount of soluble brain, plasma, and CSF samples using mutant HTT can be measured using the highly sensitive technique known as FRET. 133 Though much human research is needed to fully realize this assay’s potential in a clinical development, this method holds great promise for tracking the progression of the disease and specific HTT-lowering treatment strategies.
Challenges and Future Directions in Biomarker Research
Despite a number of obstacles, biomarker research in HD has enormous promise for the future. The absence of trustworthy early-stage biomarkers that can identify the illness before clinical symptoms manifest is one of the main challenges, which is made more difficult by patient variability in disease progression. 134 Furthermore, the identification of particular HD biomarkers is hampered by the intricacy of CNS functions and the challenge of obtaining CNS tissues, such as brain tissue or CSF. Many fluid biomarkers are still in the exploratory stage and lack standard validation, despite the fact that some, such as NfL, are exhibiting promise. Extensive research is essential for confirming biomarkers. 135 Despite these obstacles, the future of HD biomarker research appears bright, with smaller sample sizes resulting in lower statistical power. 136
While fluid biomarkers, genomic, transcriptomic, proteomic, and metabolomic studies are identifying new targets, advancements in imaging techniques such as PET and MRI are aiding in the detection of early brain changes. 115 Noninvasive biomarkers, such as those in saliva or blood, as well as digital biomarkers based on cognitive and motor function, are becoming more and more popular. Artificial intelligence in biomarker discovery and models derived from stem cells are also becoming important resources for comprehending HD. 101 Combining genetic information, fluid biomarkers, and neuroimaging provides a more thorough method of monitoring the course of a disease. By establishing standardized protocols and validating biomarkers, collaborative projects such as TRACK-HD and PREDICT-HD are eventually advancing toward earlier diagnosis and more individualized treatments for HD patients. 115
Conclusion
It takes years for HD, a genetic autosomal dominant condition, to show any clinical symptoms. enhanced understanding of the molecular mechanisms underlying the early changes in brain, neuronal, and nonneuronal cell functioning that result in the creation of therapeutic or preventative measures. With a focus on specific functions or disease-relevant pathogenic pathways, an analysis of the key proteins and their relationships in HD may provide crucial information regarding possible therapeutic targets. Promising potential biomarkers have been found using proteomic techniques; however, additional screening, expression analysis, and evaluation of sensitivity, specificity, and dynamic range are required before they can be used in practice. Given that a number of therapeutic modalities rely on gene therapy to identify the faulty allele or RNA, the HD protein is one such option.
However, measurements of huntingtin of the WT must also be examined in tandem to understand its endogenous actions. Additionally, examining the connections between the HD protein and other proteins may increase the likelihood that it will function as a molecular biomarker. This review covers a variety of biomarkers that could be useful in assessing the onset of a disease in its premanifest phase. Within this population, NfL and mHTT represent robust markers of disease progression, with integrated biofluid and imaging approaches offering improved prognostic potential. To ascertain their possible application in clinical practice and to aid in the development of innovative rehabilitations for patients with HD, researchers are examining biochemical, cognitive, neuroimaging, and clinical biomarkers. The discovery of new HD biomarkers may facilitate early diagnosis and prompt treatment to halt the disease’s progression and enhance patient outcomes.
Authors’ Contributions
A.S. supervised and conceptualized the work and critically reviewed the article; C.S. critically reviewed the article; G.S. wrote the article and drew the figures and tables. The authors confirm that no paper mill or artificial intelligence was used in this work.
Footnotes
Acknowledgments
The authors are thankful to the Institute for providing the facility to complete the review work.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
The authors gratefully acknowledge the University of Petroleum and Energy Studies for providing financial support, laboratory facilities, and internet resources that enabled the successful completion of this article.