
Abstract
Salvia miltiorrhiza
(SM)–Dalbergia odorifera (DO) is a commonly used circulating blood and transforming stasis drug pair for the treatment of cardiovascular and cerebrovascular diseases, but systematic studies on the optimal ratio for the treatment of cerebrovascular diseases have not been reported. In this study, we determined the optimal ratio of SM–DO for the treatment of ischemic stroke (IS) through the mixture design.
Five different ratios of SM and DO were applied to middle cerebral artery occlusion (MCAO) mice using an enhanced simplex center-of-mass mixture design by Minitab 17 software. The experimental ratios of SM and DO as independent variables and dependent variables including modified neurological severity scores, corner test, sticker removal test, cylinder test, 2,3,5-triphenyltetrazolium chloride staining, lactate dehydrogenase (LDH) and neuron-specific enolase (NSE) levels, and the optimal ratio of the two herbs was obtained by fitting regression equations through mixture design and multi-objective synchronization optimization. The therapeutic effects of the optimal ratio of SM–DO on MCAO mice were verified and evaluated by the indicators of neurological function, brain swelling, cerebral infarction volume, brain histopathological morphology, and the levels of LDH and NSE. The optimal ratio of SM:DO = 0.61:0.39 was obtained by multi-objective synchronization optimization. The results of pharmacodynamic validation showed that the optimal ratio of SM–DO significantly improved the neurological function scores of MCAO mice, the motor functions of the left forelimb, the sensory functions of the left paw, the motor functions of the right steering, the cerebral infarct volume, and the release of LDH and NSE and exerted the therapeutic effect on IS. The optimal ratio of SM (0.61) and DO (0.39) was found to be effective in the treatment of IS mice based on mixture design.
Introduction
Stroke is a group of diseases caused by the blockage of blood vessels in the brain, which prevents blood from flowing into the corresponding areas of the brain, or by the sudden rupture of blood vessels leading to brain tissue damage. It mainly includes ischemic stroke (IS) and hemorrhagic stroke. 1 IS is the most critical type of stroke in China, the second-largest cause of death, as well as the third-largest cause of disability in the world. 2 With the continuous acceleration of China’s population aging, preventing and treating IS has become an essential task in current medical research. Currently, clinical treatment strategies for IS mainly include the administration of internal medicine treatments such as thrombolysis, improving brain microcirculation and neuroprotective drugs, and surgical treatments such as thrombectomy surgery. However, due to the narrow treatment time window and limited treating effect of existing drugs, the improvement is poor for neurological dysfunction in patients. 3 Therefore, it is urgent to find new strategies for treating IS.
Traditional Chinese medicine (TCM) treatment intervenes in the pathological mechanism of IS through multi-component, multi-path, and multi-target approaches, showing fewer adverse reactions, and can give full play to the advantages of comprehensive treatment in multiple pathological links of IS. The herb pair of Salvia miltiorrhiza (SM)–Dalbergia odorifera (DO) comes from traditional prescriptions and a wide range of contemporary drug preparations, such as Xiangdan injection, Guanxin II prescription, and Guanxin Danshen tablets, which play an important role in the treatment of cardiovascular diseases. 4 TCM believes that “stasis of qi and blood in the collateral channels with meridian obstruction” is the main pathogenesis of IS. SM, slightly cold in nature, exhibits heat-clearing and stasis-resolving properties; DO, warm in nature, promotes meridian-warming and collateral-dredging effects. When combined, these herbs achieve dual therapeutic actions: cooling the blood while activating circulation to dissipate stasis, harmonizing yin–yang dynamics, and ensuring the pungent-induced dispersion of cold does not deplete yin, while the bitter-mediated heat clearance avoids impairing yang. SM is bitter in flavor, possessing draining and drying properties; DO is pungent, with dispersing and moving effects, particularly for promoting qi and blood circulation. When combined, their pungent-opening and bitter-descending actions create mutual enhancement and restraint-activating qi without depleting it and moving blood without causing damage. This synergy regulates qi dynamics effectively, ensuring smooth qi-driven blood flow. The SM–DO combination exemplifies “mutual enhancement” among the seven herbal interaction principles in TCM. SM, as the sovereign herb, exerts primary effects on IS by activating qi, promoting blood circulation, and resolving stasis. DO, the courier herb, manifests “‘aromatic mobility” properties to guide drug effects upward, clearing pathogenic stasis from the brain and restoring mental tranquility. Their synergistic interaction achieves triple therapeutic actions: qi activation and blood circulation enhancement, stasis removal and meridian unblocking, and hemostasis with adverse qi downward directing. 5
TCM posits that the heart governs mental activities, which rely on proper brain function for manifestation. The brain, regarded as the residence of the primordial spirit, operates under the heart’s regulation and control. Together, they maintain normal mental states. The heart dominates blood circulation, propelling blood flow to nourish the entire body. The brain, as the sea of marrow, depends on heart–blood nourishment. Insufficient blood flow to the heart impairs brain function. The heart and brain are intrinsically interconnected through the meridian system and pathologically influence each other. Ma et al. 6 demonstrated that the SM–DO herb pair exerted therapeutic effects on middle cerebral artery occlusion (MCAO) rats, with significantly superior efficacy compared to either herb alone. Li et al.7–9 further reported that Xiangdan injection, a representative formulation of SM–DO, attenuated cerebral ischemic damage in MCAO rats by reducing surgery-induced brain tissue destruction. Jiale 10 demonstrated that the SM–DO herb pair exhibited therapeutic effects on MCAO rats and identified the active components responsible for ameliorating cerebral ischemic injury. The above research suggests that SM–DO has a brain protection effect, but the compatibility ratios for SM–DO in treating IS are uneven, and the optimal compatibility ratio has not yet been determined, making it difficult to guide clinically. Current studies have mostly focused on the validation of the neuroprotective efficacy of the SM–DO combinations, with only a preliminary exploration of their ratio relationship and no systematic or scientific optimization. In contrast, the present study is the first to apply a mixture design to the ratio screening of the SM–DO combinations. Through a multifactorial and multilevel experimental design, we have precisely determined the optimal ratio.
The mixture design is a scientific methodology that mathematically characterizes the relationship between component ratios and biological effects. This approach determines optimal formulations by analyzing individual component contributions within mixtures and is widely applied in product development and optimization.11,12 Li et al. 13 employed a mixture design to identify an optimal ratio of 80% salvianolic acid A, 10% salvianolic acid B, and 10% danshensu for treating oxygen-glucose deprivation-injured H9c2 cardiomyocytes. Similarly, Ouedrhiri et al. 14 applied a mixture design approach to determine the most effective antibacterial ratio against Bacillus subtilis: 17.1% myrtle oil, 39.7% artemisia oil, and 43.2% creeping thyme oil. Marrelli et al. 15 employed a mixture design and found that a ratio of 87.7% fennel, 0.0% oregano, and 12.3% lavender exhibited the strongest inhibitory effect on nitric oxide (NO) production in lipopolysaccharide-stimulated RAW264.7 macrophages. These studies demonstrate that the mixture design exhibits distinctive advantages, including reduced experimental trials, high predictive accuracy, methodological robustness, and capacity for multi-objective simultaneous optimization, making it particularly suitable for investigating compound formulation ratios.
Therefore, this study aims to employ the mixture design to identify the optimal SM–DO ratio for IS treatment, providing novel insights and methodological foundations for clinical formulation research.
Methods
Chemicals and reagents
SM formula granules (Lot: 2401006C) and DO formula granules (Lot: 2106001S) were purchased from China Resources Sanjiu Pharmaceutical Co., Ltd. MCAO nylon bolus wire (Cat. No.: 907-03063-00) was purchased from Shenzhen Reward Life Science and Technology, China. Suture material (Cat. No.: SA82G) was purchased from Shanghai Ethicon Medical Technology Co., Ltd. 2,3,5-triphenyltetrazolium chloride (TTC) staining solution (Cat. No.: SL7140) was purchased from Coolaber Technology, China. BCA protein quantitative kit (Cat. No.: PQ003) and RIPA lysis buffer (Cat. No.: PL001) were purchased from Zhonghui Hecai Biomedical Technology, China. Lactate dehydrogenase (LDH) kit (Cat. No.: A020-2-1) was purchased from Nanjing Jiancheng Bioengineering Institute, China. Neuron-specific enolase (NSE) kit (Cat. No.: YJ063810A) was purchased from Shanghai Enzyme-linked Biotechnology, China. Protocatechualdehyde (≥98%; Cat. No.: HP019896), rosmarinic acid (≥98%; Cat. No.: HR222655), lithospermic acid (≥98%; Cat. No.: HA061502), salvianolic acid B (≥98%; Cat. No.: HS034208), salvianolic acid A (≥98%; Cat. No.: HS034206), liquiritigenin (≥98%; Cat. No.: HL042236), butein (≥98%; Cat. No.: HB062613), naringenin (≥98%; Cat. No.: HN206559), formononetin (≥98%; Cat. No.: HF012465), and biochanin A (≥98%; Cat. No.: HB144451) were purchased from Baoji Chenguang Biotechnology Co., Ltd.
Potential pharmacodynamic substance analysis of SM–DO
Experimental design diagram for potential pharmacodynamic substance analysis of SM–DO
Here is the experimental design diagram for potential pharmacodynamic substance analysis of SM–DO, illustrating all procedures and assessments (Fig. 1).
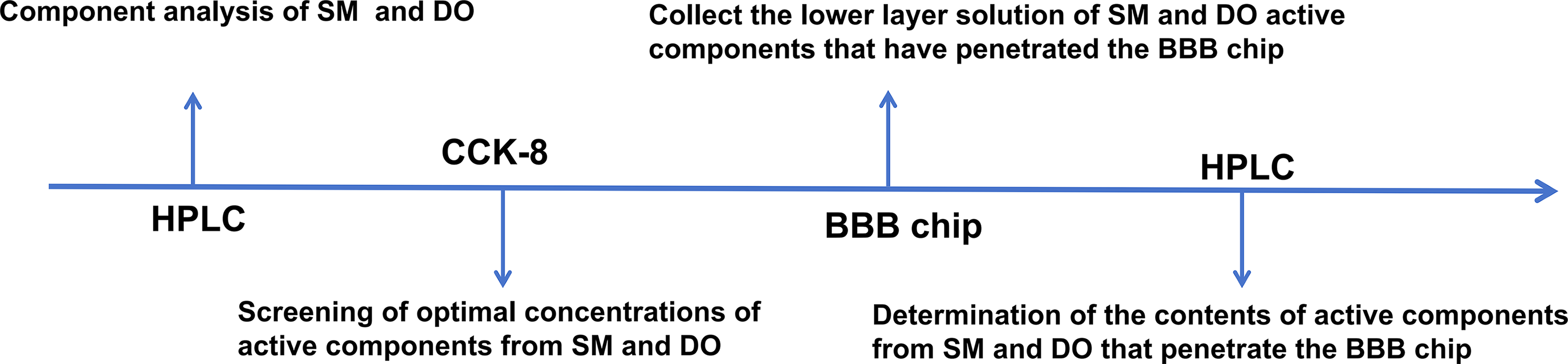
Experimental design diagram for potential pharmacodynamic substance analysis of Salvia miltiorrhiza (SM)–Dalbergia odorifera (DO). BBB, blood–brain barrier; HPLC, high-performance liquid chromatography.
Composition analysis of SM formula granules and DO formula granules
The SM formula granules were analyzed by a high-performance liquid chromatography (HPLC) instrument (Waters 2695-PDA996, USA), which was equipped with a C18 chromatographic column (4.6 × 150 mm, 3 μm). The column temperature was 30°C, and the mobile phase consisted of acetonitrile (solvent A) and 0.1% phosphoric acid aqueous solution (v/v) (solvent B). The gradient elution was as follows: 0–20 minutes, the phase A increased linearly from 20% to 50% at a flow rate of 0.8 mL/min. The detection wavelength was set in the range of 190–460 nm, and the injection volume was 5 μL.
The gradient elution for DO formula was as follows: 0–15 minutes, the phase A increased from 30% to 70%; 15–20 minutes, the ratio of phase A to phase B was maintained at 70:30 (v/v). The other conditions remained the same.
bEnd.3 cell culture
bEnd.3 cells were cultured in Dulbecco’s modified Eagle medium (DMEM) in a carbon dioxide (CO2) incubator (37°C, 5% CO2). When the cells reached 90% confluence, the culture medium was discarded, the cells were washed with phosphate-buffered saline (PBS) twice, 2 mL trypsin (0.25%) was added, and the culture was incubated for approximately 2 minutes. When the cells became round and fell off, 2 mL DMEM was immediately added to terminate the incubation. The adherent cells were detached into a suspension with a pipette and transferred to a 15 mL centrifuge tube. After centrifugation at 1000 × g for 5 minutes, the cells that were resuspended in cell culture medium were transferred to a new cell culture bottle at a 1:2 proportion and placed in a CO2 incubator. DMEM was changed every 48 hours.
CCK-8 method for screening optimal drug concentrations
When the cells reached 90% confluence, they were inoculated into 96-well plates at a density of 5 × 104 cells/mL and incubated overnight. DMEM was replaced with a drug-containing glucose DMEM. After 24 hours, 10 μL of Cell Counting Kit-8 solution was added to each well, and the absorbance was measured at 450 nm after 2 hours of incubation. Experimental groups included: liquiritigenin (200, 100, 50, 25, 12.5, and 0 µmol/L), naringenin (160, 80, 40, 20, 10, and 0 µmol/L), formononetin (160, 80, 40, 20, 10, and 0 μmol/L), salvianolic acid A (40, 20, 10, 5, 2.5, and 0 μmol/L), salvianolic acid B (80, 40, 20, 10, 5, and 0 μmol/L), and lithospermic acid (80, 40, 20, 10, 5, and 0 μmol/L).
Construction of the blood–brain barrier chip model
bEnd.3 cells were diluted to a concentration of 6 × 106 cells/mL, and the cell suspension was loaded into the upper channel of the chip. Then the chip was cultured in a CO2 incubator with the medium changed every 24 hours. On the third day, a microfluidic injection pump was connected to the upper channel of the chip, and dynamic culture was performed at a flow rate of 2 μL/min.
Barrier selectivity evaluation of the blood–brain barrier chip model
A working solution of Fluorescein Isothiocyanate-labeled dextran (FITC-Dextran, 10 kDa) at a concentration of 50 µg/mL was injected into the upper channel of the blood–brain barrier (BBB) chip using a microfluidic injection pump. After incubation in a CO2 incubator for 4 hours, the fluorescence intensity of the culture medium in the lower channel was measured to calculate the permeability of FITC-Dextran. The permeability calculation formula is as follows: Papp = (Val × Cal)/(A × C × t), where Papp is the apparent permeability coefficient, Val (mL) is the volume of culture medium in the chip channel; Cal (mol/mL) is the concentration of the analyte that has crossed the BBB and entered the lower layer of the chip; A (cm2) is the area of the semipermeable membrane between the upper and lower layers of the chip; C (mol/mL) is the concentration of the analyte in the upper layer of the chip; and t is the perfusion time of the analyte.
Drug permeability experiment on the BBB chip model
The optimal drug concentration was selected via cytotoxicity assays for permeability testing. About 3 mL of each drug solution was separately infused into the upper channel at a flow rate of 2 μL/min. The solution from the lower channel was collected after 24 hours. The collected solutions were subjected to HPLC quantitative analysis. For liquiritigenin, isocratic elution was performed with a mobile phase of A–B (35:65, v/v) using isocratic elution. For naringenin and formononetin, gradient elution was applied: 0–15 minutes, the proportion of phase A increased linearly from 30% to 70%; 15–20 minutes, the phase A–B ratio (70:30, v/v) was maintained. For lithospermic acid, salvianolic acid A, and salvianolic acid B, gradient elution was used: 0–15 minutes, the proportion of phase A increased linearly from 20% to 50%; 15–20 minutes, the phase A–B ratio (50:50, v/v) was maintained. The injection volume for all components was 10 μL. For other procedures, refer to Method 1, and Papp was calculated according to the formula.
Experimental animals
One hundred and two SPF male C57BL/6 mice (aged 6–8 weeks, body weight 20–25 g) were purchased from Chengdu Dashuo Laboratory Animal Company Limited (License No.: SCXK [Sichuan] 2020-0030). The Shaanxi University of Chinese Medicine’s Ethical Review Board authorized the animal experimental procedure (No. SUCMDL20240610001). All animal experimental procedures were performed in accordance with the Animal Research: Reporting In Vivo Experiments 2.0 guidelines. The inclusion and exclusion criteria for experimental animals are supplemented as follows: Inclusion criteria were as follows: healthy male C57BL/6 mice aged 6–8 weeks, weighing approximately 20–25 g, and with an mNSS score of 1–12 were included in the study. Exclusion criteria were as follows: mice that did not meet the age and weight requirements, those with an mNSS score of 0 or >12, or those showing hemorrhage in the MCAO region during postmortem examination were excluded.
MCAO mice model preparation
In the sham group, only the longitudinal neck incision was made, and the right common carotid artery (CCA), external carotid artery (ECA), and internal carotid artery (ICA) were used without insertion of nylon suture. The model group and the SM–DO group were modeled using the MCAO mouse model established by the wire-bolus method to simulate the cerebral ischemia/reperfusion (I/R) injury state after the onset of IS. The mice were anesthetized by intraperitoneal injection of 1% pentobarbital sodium at a dose of 60 mg/kg. The mice were supine fixed, and the skin was disinfected. The anterior-middle longitudinal incision of the neck was made, and the subcutaneous tissue was separated by blunt dissection, exposing the right CCA, ECA, and ICA. One 5-0 nylon suture thread was hung on each of the CCA and ICA of mice, and the ECA thread was fastened tightly. A small cut was made near the bifurcation of the CCA, and the thread was slowly inserted into the ICA to enter the right middle cerebral artery. After feeling resistance, the thread was fixed, the threads on the CCA and ICA were fastened tightly, and the skin was sutured. After blockage of blood flow for 1 hour, some of the thread was removed, and reperfusion was performed for 24 hours. After 24 hours of reperfusion, the success of the model was judged by the appearance of left-sided paralysis, instability, and circling to the side when lifting the tail after the mice woke up from anesthesia for the surgery.
Before the experiment, the mice were reared in cages for a week. The temperature of the feeding environment was kept at 25°C ± 2°C, and the humidity was kept at 55%–75%. The light alternated between light and dark for 12 hours. The mice could drink and eat freely but fasted for 12 hours before the experiment. The room temperature throughout the entire surgical process was maintained at 22°C–25°C, and an automated temperature-controlled heating pad was used to keep the mice’s rectal temperature at 37°C ± 0.5°C. After surgery, the mice were placed in a clean cage with fresh bedding and had free access to food and water. At the end of the experiment, the mice were euthanized via carbon dioxide inhalation.
Mixture design
Experiment design
The experimental scheme was automatically generated using Minitab 17 software to develop a mixture design for SM and DO combinations. An augmented simplex centroid mixture design was employed, with each component’s proportion in the mixture ranging from 0 (0%) to 1 (100%). The design generated five distinct test points (each representing a unique composition ratio), with each test point being independently replicated at least three times.
Model fitting and analysis
The regression model was established using the proportions of SM and DO as independent variables (Xs) and nine response indicators as dependent variables (Ys), including modified neurological severity score (mNSS), forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarct volume, LDH and NSE levels in brain tissue, and LDH and NSE levels in serum. A second-order polynomial model was selected with the stepwise method to identify significant terms for model inclusion. Model coefficients were estimated using the least squares method. Goodness-of-fit was evaluated with R2 (coefficient of determination) and adjusted R2 values. The individual and interactive effects of SM and DO on the nine response variables were analyzed using Cox response trace plots. This graphical approach enabled visualization of how each component’s proportion variation influenced biological outcomes while maintaining constant proportional relationships among other components.
Multi-objective synchronization optimization
For response indicators including mNSS score, forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarction volume, LDH levels, and NSE levels, smaller values indicate a better therapeutic effect of the drug. Because it is unrealistic to completely lower the levels of the above indicators of the brain-injured mice to normal levels, the target values for optimization were set at 80% of the ideal curative effect, with the average values of the indicators from the normal group as ideal and the average values of the above indicators from the model group as the worst. Based on the established models and the settings for ideal targets, the optimal ratio of SM–DO for treating IS was searched automatically with the Minitab 17 software. The individual desirability (d) evaluates the optimization degree of a candidate ratio for a single response, while the composite desirability (D) assesses the overall optimization degree of a candidate ratio for a group of responses. The desirability value ranges from 0 to 1, where 1 represents the ideal scenario, and 0 indicates the worst.
Animal handling and grouping
The experiment was divided into two parts: the research objective of the first part of the experiment was to explore the optimal ratio of SM–DO for the treatment of IS, and the research objective of the second part of the experiment was to validate and evaluate the real effect of the optimal ratio of SM–DO for the treatment of IS.
In the first part, 42 male C57BL/6 mice were randomly divided into seven groups using the random number table method, which included a sham group, a model group, and five SM–DO subgroups corresponding to five distinct SM–DO ratios (1:0, 0:1, 0.5:0.5, 0.75:0.25, and 0.25:0.75 set as 2.5.1 described). MCAO model preparation was performed in all groups except the sham group, which had only a longitudinal neck incision, CCA, ECA, and ICA without wire bolus insertion. The animals in each group were administered by gavage 24 hours after reperfusion was achieved, once a day for 7 consecutive days, and the doses were calculated based on the conversion of animal and clinical human doses, with the SM formula pellets administered at a dose of 1.13 g/kg and the DO formula pellets administered at a dose of 0.38 g/kg. The sham group and the model group were given the same dose of saline (10 mL/kg) once a day for 7 consecutive days. The SM and the DO formula granules were dissolved in normal saline, and the solution was used immediately after preparation.
In the second part, 60 male C57BL/6 mice were randomly divided into six groups using the random number table method, which were the sham group, the model group, the SM–DO optimally rationed low (L)-, medium (M)-, and high (H)-dose groups, and the SM–DO clinically available maximum dose group (C). MCAO model preparation was performed in all groups, except for the sham group, which had only longitudinal neck incisions to expose CCA, ECA, and ICA, without wire bolus insertion. The animals in each group were administered by gavage 24 hours after reperfusion was achieved, and the administered dose was calculated based on the conversion of animal and clinical human doses, and the optimal SM–DO ratio derived from the first part were set for the medium-dose group, SM–DO (L): 0.35 + 0.07 g/kg, SM–DO (M): 0.69 + 0.15 g/kg, SM–DO (H): 1.38 + 0.30 g/kg, SM–DO (C): 1.13 + 0.38 g/kg once a day for 7 consecutive days. Sham and model groups were given the same dose of saline (10 mL/kg) once a day for 7 consecutive days.
Experimental design diagram for optimal ratio screening of SM–DO in the treatment of IS
Here is the experimental design diagram for optimal ratio screening of SM–DO in the treatment of IS, illustrating all procedures and assessments (Fig. 2).
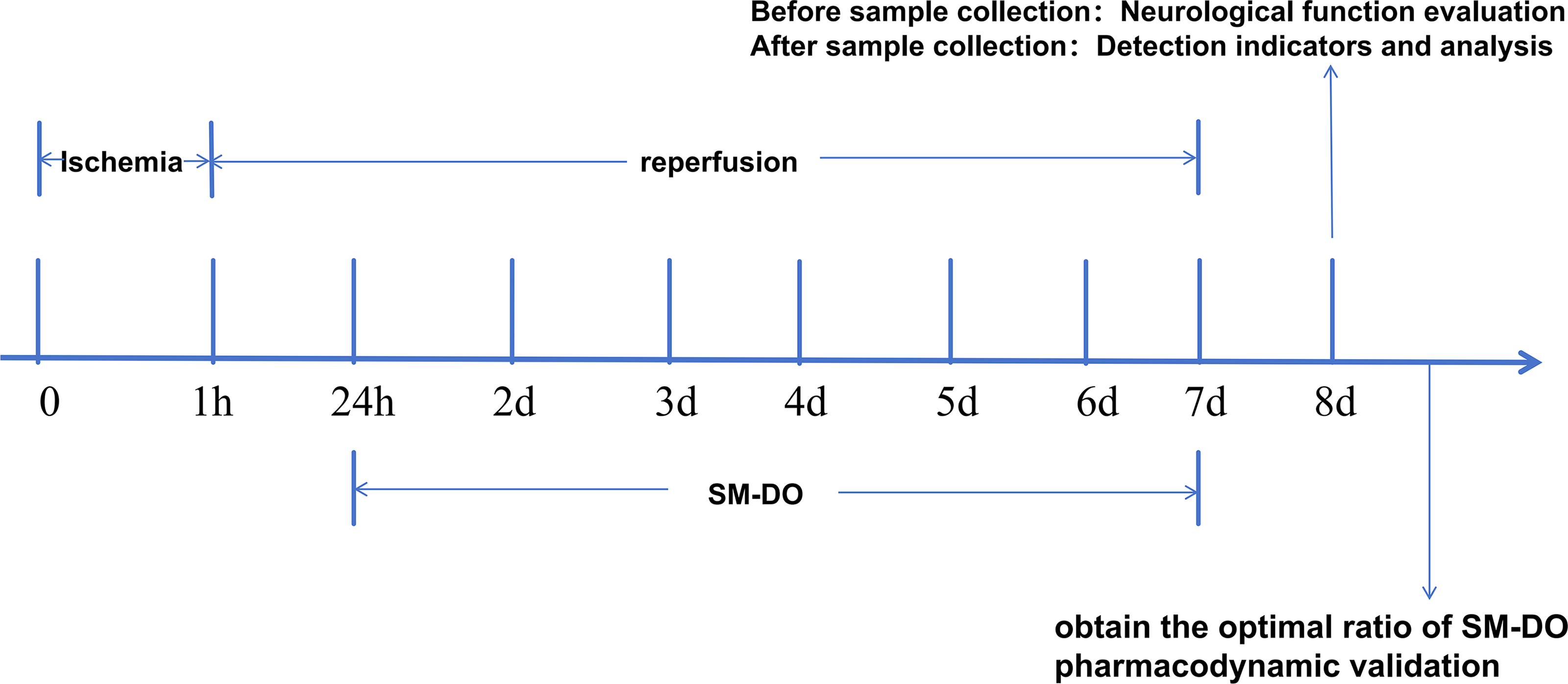
Experimental design diagram for optimal ratio screening of SM–DO in the treatment of ischemic stroke.
Neurological function
mNSS score
The mNSS score 16 was used to evaluate mouse motor function, sensory function, reflex function, and balance ability. The highest score is 18, with 13–18 being severe impairment, 7–12 being moderate impairment, and 1–6 being mild impairment (Supplementary Table S1).
Seven days after cerebral I/R, an observer blinded to the group assignments scored the mice according to the mNSS criteria.
Corner test
The corner test was to evaluate the abnormality of sensation and movement. 17 The specific operation was to place two pieces of cardboard with a size of 30 cm × 20 cm × 1 cm at an included angle of 30° and place the mouse between the cardboard. When the mouse entered the depth of the included angle, the tentacles on both sides first touched the cardboard, and the mouse would stand up on its hind legs, forward, and then turned around to face the outside of the included angle. Only when the hind legs stood up completely along the included angle, and then turned around, it was recognized as completing a corner test. After 20 tests, the number of right turns was calculated. The more right turns, the more severe the injury. The score is obtained by using the formula: number of right turns/total number of turns × 100%. In normal mice, the equal intensity of stimulation signals from both sides results in approximately equal frequencies of right and left turns. In contrast, mice with ischemic brain injury exhibit a significantly increased frequency of right turns due to the effects of hemiparesis.
Sticker removal test
The sticker removal test was used to evaluate sensorimotor function. 18 The specific method was to attach a round sticker with a diameter of 5 mm to the two front paws of mice. Normal mice take almost the same time to remove each sticker, while mice with brain injury need a longer time to remove the sticker on the injured side. The longer it took, the more severe the motor function was. The time required for each group of mice to remove the left forelimb sticker was recorded. Three days before modeling, mice were gently grabbed and restrained for 30 seconds each day, and their forelimbs were gently touched.
Cylinder test
Also known as asymmetrical limb use test, it was used to evaluate the symmetry of mouse forelimb use and rotation. 19 The mouse was placed in a transparent beaker with a diameter of approximately 9 cm and a height of about 15 cm. When the mouse stood on its hind legs, the number of times that the left forelimb, right forelimb, and both forelimbs touched the cylinder wall for the first time was recorded, respectively. When one forelimb (e.g., the right) contacts the cylinder wall and the contralateral forelimb (left) subsequently contacts the wall before the initial limb is withdrawn, it is recorded as one right forelimb contact and one simultaneous contact. If both forelimbs alternately touch the wall, it is scored as a simultaneous contact. Three days before modeling, mice were individually placed in the cylinder apparatus for adaptation for 5 minutes. The test was repeated 20 times. Final score = (number of healthy forelimb touches − number of damaged forelimb touches)/total number of times × 100%.
Brain water content detection to evaluate the degree of brain swelling
The brain tissue was taken out, rinsed in precooled physiological saline, and then the wet weight of the brain was measured. After that, it was dried in an electrothermal constant temperature drying oven at 70°C for 48 hours, and the dry weight was measured. Brain water content = (wet weight − dry weight)/wet weight × 100%.
TTC staining to observe the volume of cerebral infarction
Brain tissues were harvested on day 7 after model establishment. After anesthesia, the mouse was thoracotomized to expose the heart. A perfusion needle was inserted into the left cardiac apex, and the right atrial appendage was incised. Precooled PBS was perfused until the effluent became clear, at which point the intact brain tissue was promptly removed. The brain tissue was extracted and rinsed in precooled physiological saline, followed by rapid freezing at −20°C for 30 minutes. On an ice platform, serially sectioned coronally along the bregma–lambda axis. Five consecutive coronal slices with a thickness of approximately 2 mm were obtained (from bregma +2.0 mm to bregma −8.0 mm). The brain slices were then immersed in 2% TTC staining solution and incubated in a 37°C incubator for 30 minutes under light-protected conditions, with mid-incubation flipping performed. Subsequently, the slices were fixed with 4% paraformaldehyde buffer and photographed. In the resulting images, red coloration indicated normal tissue, whereas white areas represented infarcted regions. Finally, the cerebral infarction volume was quantified using Image J 1.54g software. Infarct Volume (%) = [(ΣInfarct Area)/(ΣTotal Area of Same Hemisphere)] × 100%. Σ represents the summation of corresponding values from all consecutive brain slices (without edema correction).
Hematoxylin and eosin staining to observe the morphology of brain tissue
The brain tissue was removed and rinsed in precooled physiological saline, then fixed in 4% paraformaldehyde. Following fixation, the tissue was dehydrated, embedded in paraffin, and sectioned into 5 μm coronal slices. These sections were subsequently stained with hematoxylin and eosin (HE). Morphological and structural changes of cortical neurons in each group of mice were observed and analyzed under a microscope.
Kits to detect serum and brain tissue LDH and NSE levels
Mice were intraperitoneally injected with 1% pentobarbital sodium (60 mg/kg). After achieving deep anesthesia, blood was collected from the cardiac puncture. Blood was collected and centrifuged at 855 g for 10 minutes, the supernatant was collected and centrifuged at 4°C and 13,700 g for 10 minutes, and the supernatant was subpackaged and stored at −80°C. The brain tissues of mice from each group were taken and homogenized in an ice bath at a ratio of 1:9 (w/v, tissue mass [g]: reagent volume [mL]). Centrifuge at low temperature, 13,700 g for 10 minutes at 4°C, and collect the supernatant for storage at −80°C for later use.
According to the LDH test kit instructions provided by Nanjing Jiancheng Bioengineering Research Institute, add samples, substrate buffer, and coenzyme I in sequence, vortex to mix well, incubate at 37°C for 15 minutes; then add 2,4-dinitrophenylhydrazine, vortex mix well, incubate at 37°C for 15 minutes; finally, add sodium chloride solution and place at room temperature for 3 minutes, use an enzyme-linked immunosorbent assay (ELISA) reader to measure the absorbance at 440 nm.
According to the NSE test kit instructions provided by Shanghai Enzyme-Linked Biotechnology Co., Ltd, an ELISA was performed following the kit instructions. Different concentrations of standards were added to the standard wells, and the samples to be tested were added to the sample wells; horseradish peroxidase–labeled detection antibody was added, incubate at 37°C for 60 minutes, then the liquid was discarded, the plate was washed, patted dry, and this washing step was repeated five times; reaction substrates A and B were added, and the mixture was incubated at 37°C in the dark for 15 minutes; the stop solution was added to terminate the reaction, and the absorbance (optical density) was measured at 450 nm using an ELISA reader, a standard curve was generated, and the concentration of the sample to be tested was calculated based on the standard curve.
Statistical analysis
The mixture design was fitted using stepwise regression, and then the optimal solution was obtained based on this model with the Minitab 17 software.
The data were expressed as mean ± standard deviation (
Results
Component analysis of SM formula granules and DO formula granules
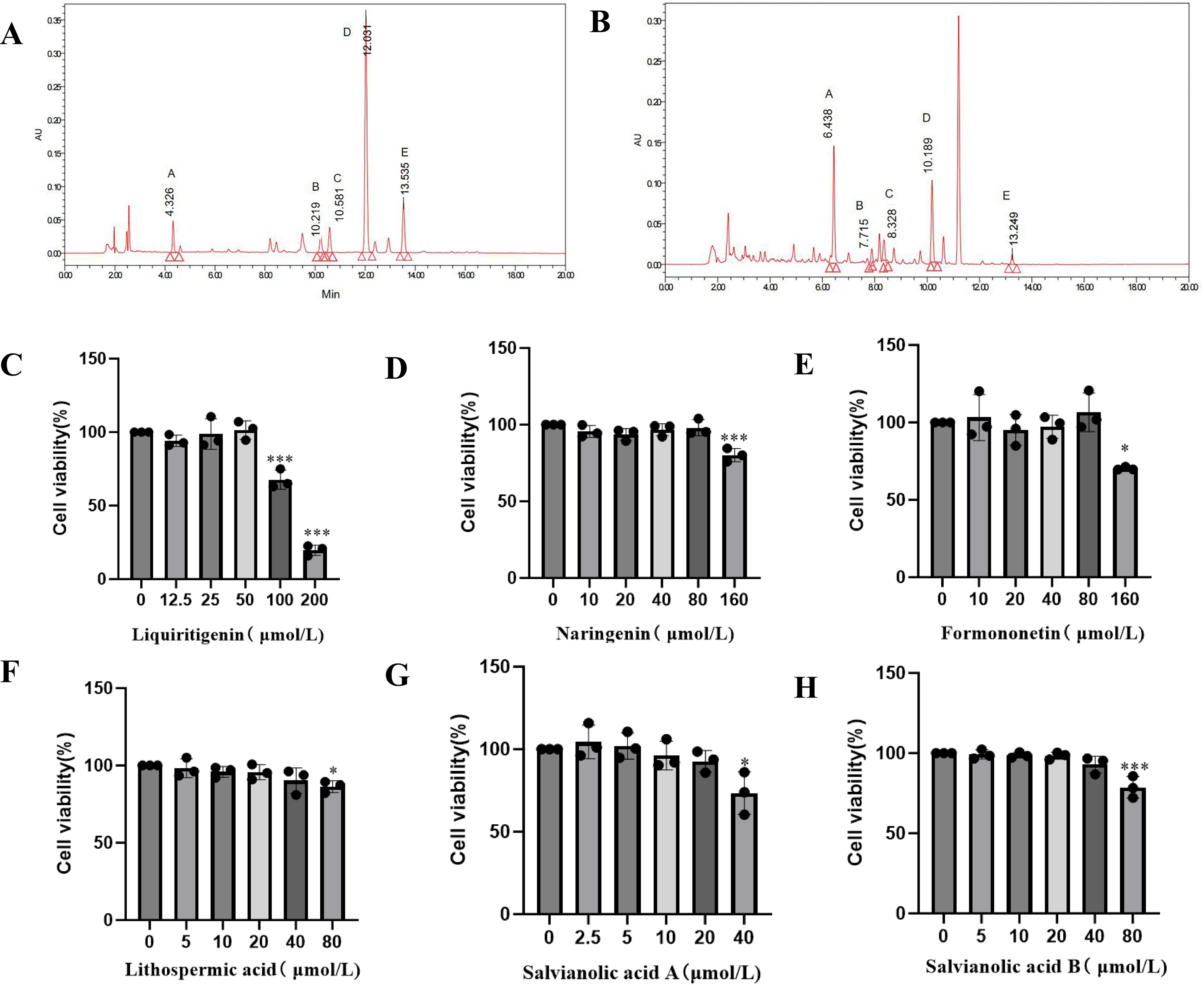
Component analysis of SM formula granules, as shown in Figure 3A, the retention times of the measured samples were compared with those of the standards. We found that the peak A was protocatechualdehyde, with a retention time of 4.326 minutes and a content of 79.64 μmol/L. The peak B was rosmarinic acid, with a retention time of 10.219 minutes and a content of 52.73 μmol/L. The peak C was lithospermic acid, with a retention time of 10.581 minutes and a content of 59.43 μmol/L. The peak D was salvianolic acid B, with a retention time of 12.031 minutes and a content of 502.36 μmol/L. The peak E was salvianolic acid A, with a retention time of 13.535 minutes and a content of 66.74 μmol/L. Based on the determination of effective ingredient contents, salvianolic acid B, salvianolic acid A, and lithospermic acid have relatively higher contents.
Potential pharmacodynamic substance analysis of SM–DO.
Component analysis of DO formula granules, as shown in Figure 3B, the retention times of the measured samples were compared with those of the standards. We found that the peak A was liquiritigenin, with a retention time of 6.448 minutes and a content of 288.78 μmol/L. The peak B was butein, with a retention time of 7.715 minutes and a content of 7.35 μmol/L. The peak C was naringenin, with a retention time of 8.328 minutes and a content of 51.42 μmol/L. The peak D was formononetin, with a retention time of 10.189 minutes and a content of 70.83 μmol/L. The peak E was biochanin A, with a retention time of 13.249 minutes and a content of 7.04 μmol/L. Based on the determination of effective ingredient contents, liquiritigenin, formononetin, and naringenin have relatively higher contents.
Optimal drug concentration screening
According to the results of the component analysis experiment, three effective components with relatively high contents were selected from the SM and DO formula granules, respectively, and these components were selected for subsequent experiments.
After different concentrations of effective components were applied to bEnd.3 cells, the cell viability results showed that within the tested concentration range, the cell viability was relatively high when the concentrations were 50 μmol/L for liquiritigenin, 80 μmol/L for naringenin, 80 μmol/L for formononetin, 40 μmol/L for lithospermic acid, 20 μmol/L for salvianolic acid A, and 40 μmol/L for salvianolic acid B. Therefore, the above concentrations were selected for subsequent permeability experiments (Fig. 3C–H).
Functional integrity evaluation of the BBB chip model
The experiment examined the permeability of macromolecules through this BBB chip model. FITC-Dextran is widely used to assess permeability. The Papp measured in this chip model was 8.8 × 10−6 cm/s, which showed that the chip model had formed a tight barrier.
Evaluation of drug permeability in the BBB chip model
This study selected three active components with relatively high contents from each formula (three from DO: liquiritigenin, naringenin, and formononetin and three from SM: lithospermic acid, salvianolic acid A, and salvianolic acid B). Transport of six effective components across the BBB was evaluated on the constructed chip model. And the content of each component was determined by HPLC to obtain the corresponding Papp values. The results showed that the permeation concentration of liquiritigenin was 6.63 µmol/L, naringenin was 2.57 µmol/L, and formononetin was 0.75 µmol/L. The Papp values of liquiritigenin, naringenin, and formononetin were 2.06 × 10−9, 4.98 × 10−10, and 2.31 × 10−10 cm/s, respectively. Lithospermic acid, salvianolic acid A, and salvianolic acid B were not detected.
Experimental ratios provided by the mixture design
The study employed SM and DO as constituent components of the mixture system. An augmented simplex centroid mixture design was implemented with each component’s proportion ranging from 0 to 1. Based on the automated experimental scheme generated by Minitab 17 software for establishing the regression model, five distinct mixture ratios were created (Table 1). Each ratio formulation would be independently tested with a minimum of three replicates.
Experimental Ratios Provided by Mixture Design
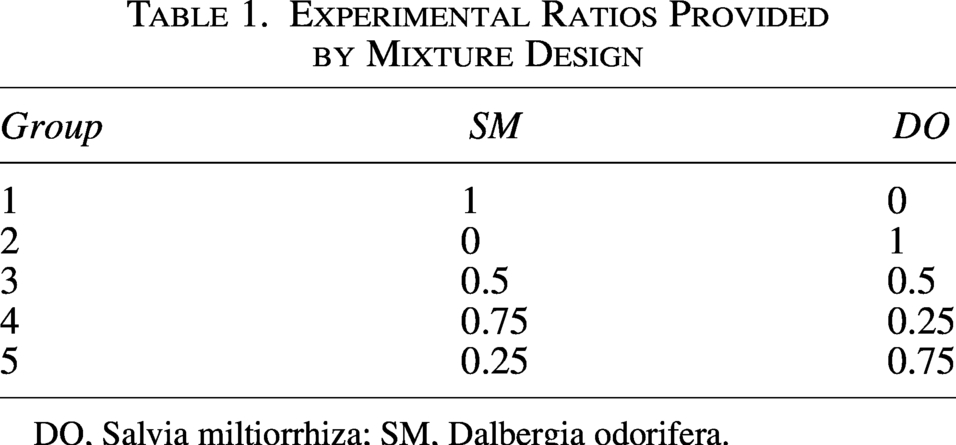
DO, Salvia miltiorrhiza; SM, Dalbergia odorifera.
Experimental ratios of SM–DO improved neurological function in MCAO mice
Before the mice were executed in each group, the mice were scored for neurological function using four different evaluations, namely, mNSS score (Fig. 4A), cylinder test (Fig. 4B), corner test (Fig. 4C), and sticker removal test (Fig. 4D). The results showed that the mNSS score, right turn rate, left forelimb removal time of sticker, and forelimb use asymmetry rate were significantly increased in the model group compared to the sham group (p < 0.001), suggesting that there was significant neurobehavioral impairment in the mice in the model group and that the MCAO mouse model was successfully prepared. Compared with the model group, the mNSS scores of four experimental ratio groups of SM–DO (i.e., 1:0, 0.5:0.5, 0.75:0.25, 0.25:0.75) were significantly decreased (p < 0.05), and there was a decreasing tendency of mNSS scores in the SM–DO group (0:1), but there was no significant difference. The results of the cylinder test and sticker removal test showed that SM–DO experimental ratio groups (i.e., 0.5:0.5, 0.75:0.25, 0.25:0.75) could significantly decreased (p < 0.05) forelimb use asymmetry rate and left forelimb sticker removal time (p < 0.05) compared to the model group, and the SM–DO experimental ratios (i.e., 1:0, 0:1) had an improving trend (p < 0.05) impact on forelimb use asymmetry rate and left forelimb sticker removal time, there were no significant differences. The results of the corner test showed that the SM–DO experimental ratio groups (i.e., 0.75:0.25, 0.5:0.5) had a significant decrease (p < 0.01) rightward turn compared with the model group, and the SM–DO experimental ratio groups (i.e., 1:0, 0:1, 0.25:0.75) tended to rightward turn, but there were no statistically significant differences.
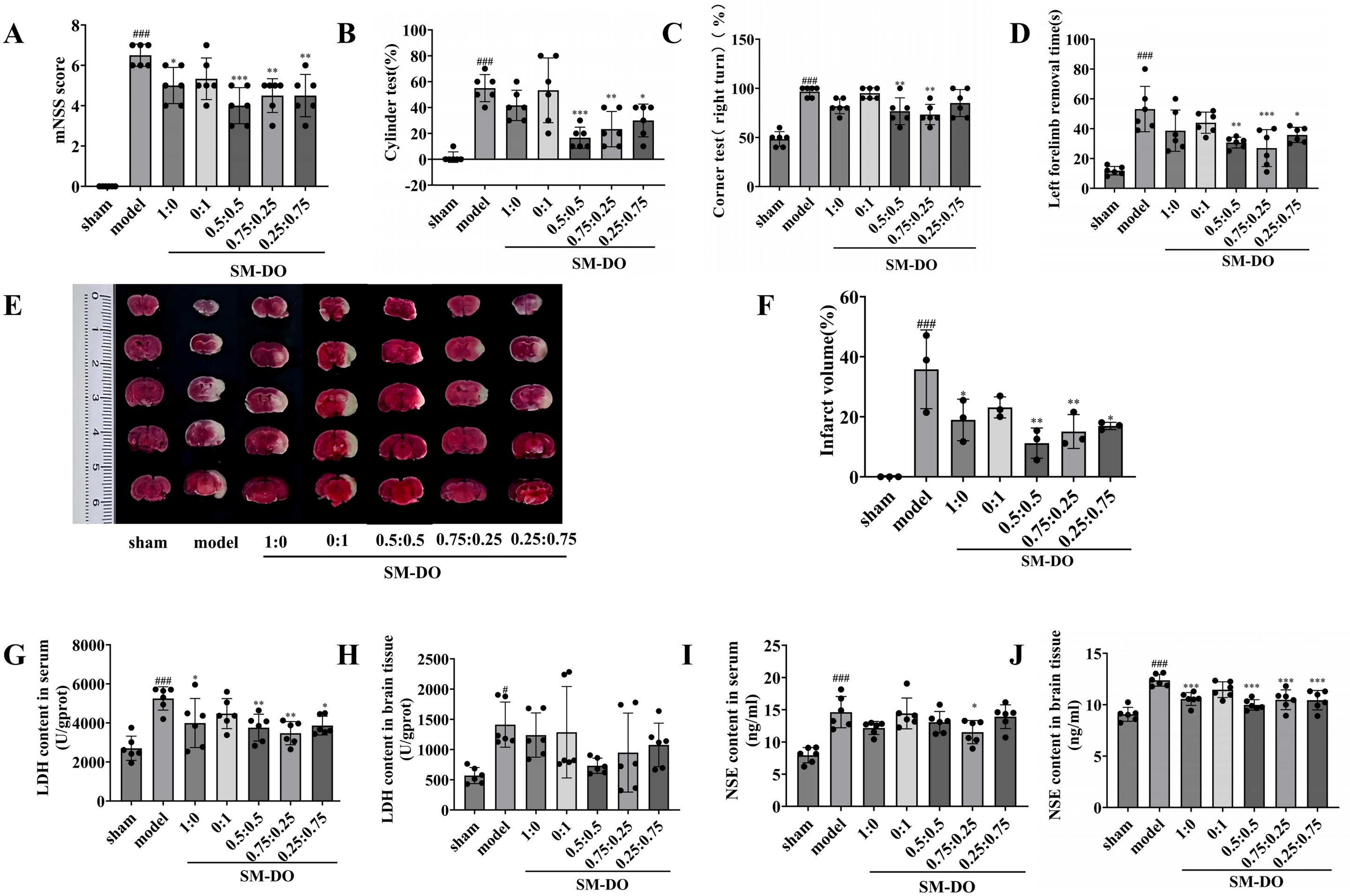
Effect of experimental ratios of SM–DO in middle cerebral artery occlusion (MCAO) mice.
Experimental ratios of SM–DO reduced the volume of cerebral infarction in MCAO mice
The results of cerebral infarction volume in mice (Fig. 4E, F) showed that compared with the sham group, an obvious infarcted area was visible in the mice of the model group (p < 0.001), suggesting that the MCAO mouse model was successfully prepared. Compared with the model group, the experimental ratios of the SM–DO group (i.e., 1:0, 0.5:0.5, 0.75:0.25, 0.25:0.75) had significantly decreased cerebral infarction volume (p < 0.05), and there was a decreasing trend in cerebral infarction volume in the SM–DO group (0:1), but there was no significant difference.
Experimental ratios of SM–DO reduced the release of LDH and NSE in MCAO mice
The results of LDH (Fig. 4G), NSE levels in serum (Fig. 4I), and LDH (Fig. 4H) and NSE levels in brain tissue (Fig. 4J) showed that compared with the sham group, the LDH and NSE levels in serum and brain tissue of the model group were significantly higher (p < 0.05 and p < 0.001, respectively), suggesting that the MCAO induced brain tissue injury in the mice. Compared with the model group, SM–DO groups with experimental ratios (i.e., 1:0, 0.5:0.5, 0.75:0.25, 0.25:0.75) significantly decreased LDH levels in serum (p < 0.05) and NSE levels in brain tissue (p < 0.001); the SM–DO group (0.75:0.25) significantly reduced NSE levels in serum (p < 0.05), suggesting that SM–DO can improve brain damage caused by brain I/R.
Fitting and analysis of regression models
The experimental data of nine response indicators obtained from experimental ratios of SM and DO acting on MCAO mice by mixture design (Supplementary Table S2).
Based on the experiment data, regression equations for the nine response indicators were obtained using the stepwise method. The p-values obtained from the overall F test of each model were <0.05, suggesting that each model was statistically significant. The p-values obtained from the lack-of-fit test of each model were >0.05, suggesting that each model did not miss significant terms, as shown in Table 2.
Regression Model of Response Indicators
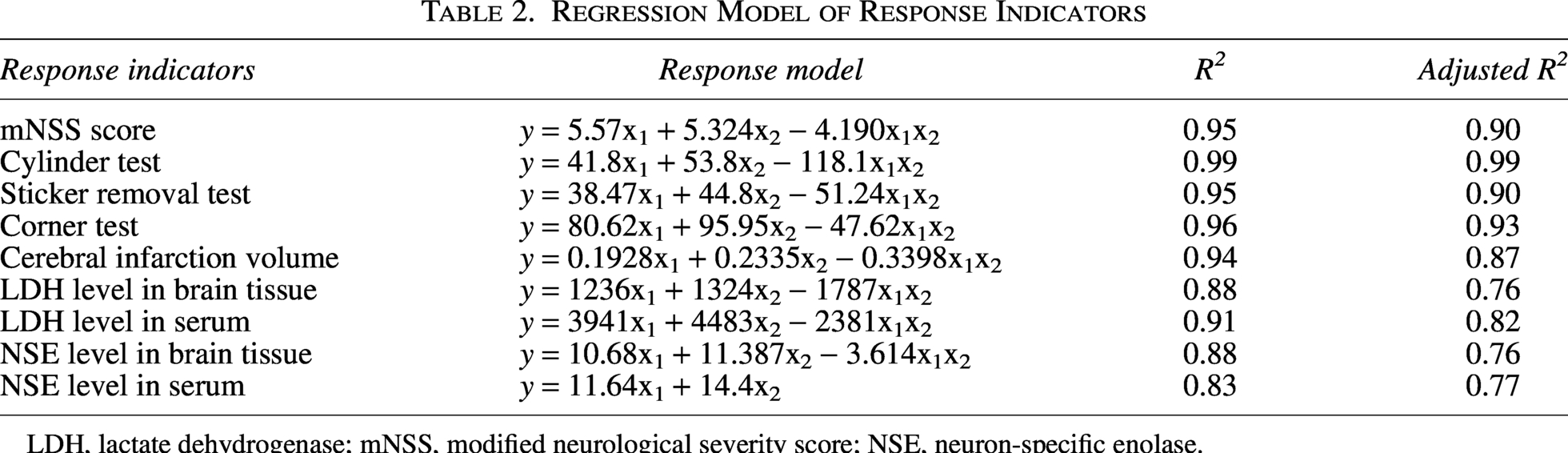
LDH, lactate dehydrogenase; mNSS, modified neurological severity score; NSE, neuron-specific enolase.
Based on the fitted models, the Minitab software plotted the corresponding trend of each response indicator when the proportion of SM or DO changes relative to the reference ratio (0.5 for each)—the response trace curve. The gray dashed vertical line in the figure indicates the “reference level” of the response indicators, that is, the value of the response indicators when the proportion of SM and DO each accounts for 0.5. The blue solid line represents the corresponding trend of the response indicators value when the proportion of SM increases (or decreases) relative to 0.5, and the red dashed line represents the corresponding trend of the response indicators value when the proportion of DO increases (or decreases) relative to 0.5. As can be seen from the figure, when the mNSS score, forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarction volume, LDH and NSE in brain tissue, and LDH in brain tissue were used as the response indicators, the apex of the response trace curves representing SM was to the right with respect to the gray dashed vertical line, suggesting that a moderate increase in the percentage of SM (relative to 0.5) could make the indicators take lower values; when NSE level in serum was used as the response indicator, the response trace curves representing SM and DO showed opposite linear trends, with NSE levels in serum showing a decreasing trend as the percentage of SM increased (relative to 0.5) (Fig. 5A–I).
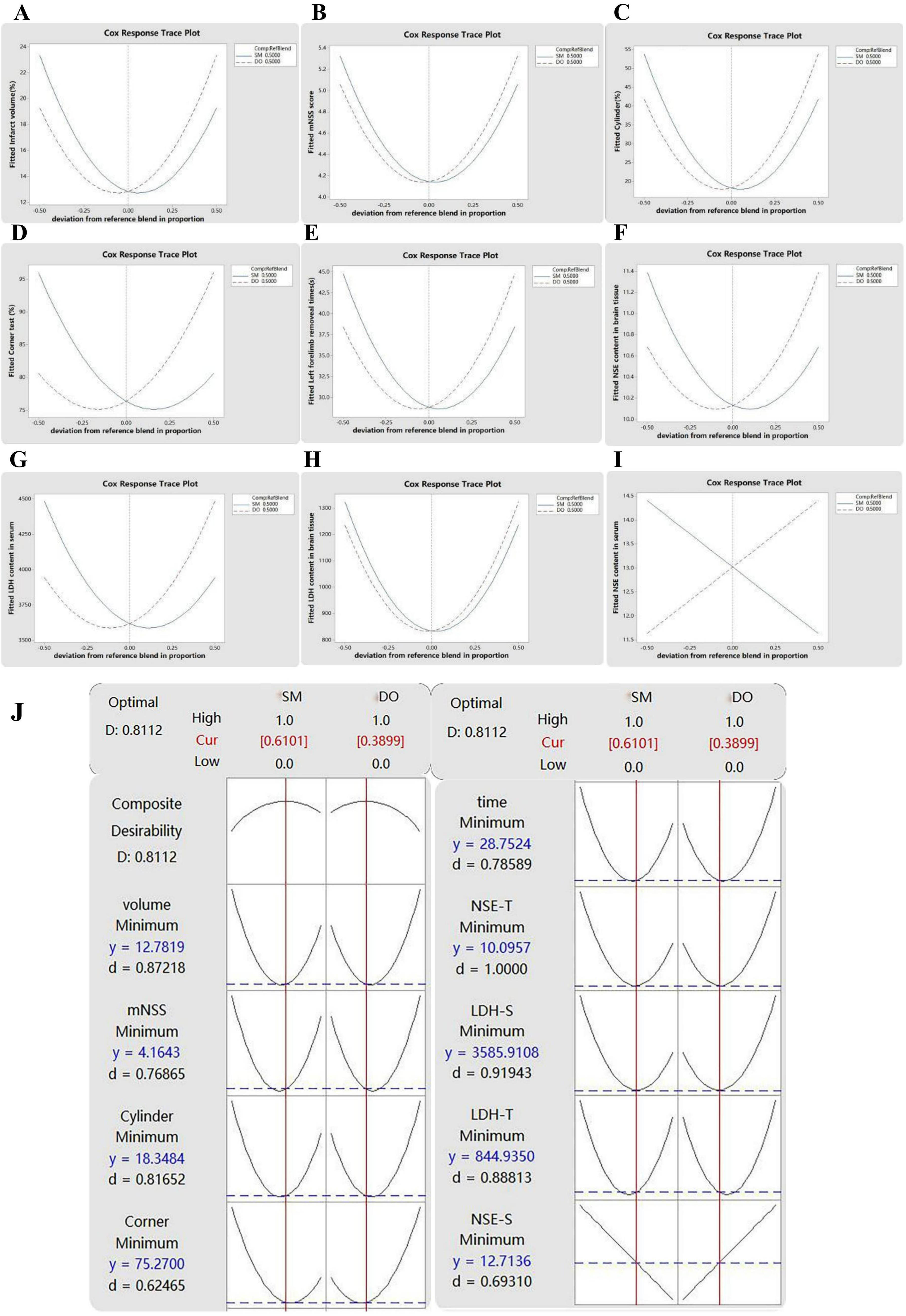
Mixture design results analysis.
Multi-objective simultaneous optimization
The optimization plot (Fig. 5J) was generated by Minitab software to display the results of simultaneous optimization on the nine response indicators. The numeric result of the simultaneous optimization indicated that 0.6101:0.3899 was the optimal ratio for SM:DO, with the composite desirability of 0.8112.
An optimal ratio of SM–DO improved neurological function in MCAO mice
The results showed that the mNSS score (Fig. 6A), forelimb use asymmetry rate (Fig. 6B), right turn frequency (Fig. 6C), and sticker removal times (Fig. 6D) were significantly increased in the model group compared to the sham group (p < 0.001). Compared with the model group, the SM–DO (L), SM–DO (M), SM–DO (H), and SM–DO (C) all significantly reduced mNSS scores (p < 0.01). The results of the cylinder test and sticker removal test showed that compared with the model group, SM–DO (M), SM–DO (H), and SM–DO (C) significantly reduced forelimb use asymmetry rate (p < 0.01) and right turn frequency (p < 0.01), while SM–DO (L) showed a tendency to decrease but no statistical difference was observed. The results of the corner test showed that SM–DO (H) and SM–DO (C) significantly reduced sticker removal time from the left forelimb (p < 0.01), and there was a trend to reduce sticker removal time from the left forelimb in SM–DO (L) and SM–DO (M), but there were no statistically significant differences, compared with the model group. The efficacy of SM–DO showed a dose-effect-dependent relationship.
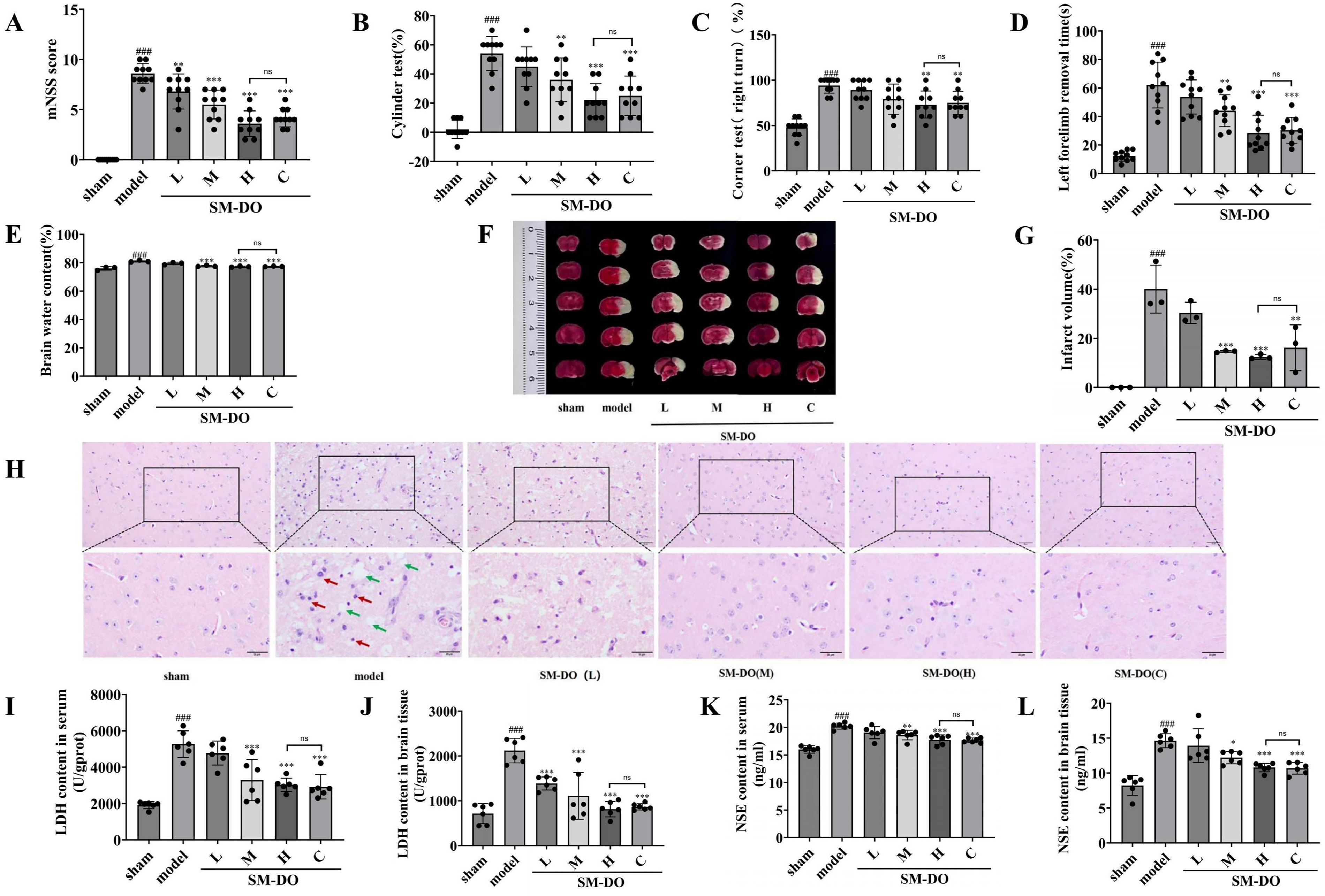
Effect of optimal SM–DO ratios in MCAO mice.
Optimal ratio of SM–DO reduced brain swelling and infarct volume in MCAO mice
The results of brain water content (Fig. 6E) and cerebral infarct volume (Fig. 6F–G) of mice showed that compared with the sham group, the brain water content of mice in the model group was significantly higher (p < 0.001), and obvious infarct areas were visible (p < 0.001), suggesting that the MCAO mice model was successfully prepared. Compared with the model group, SM–DO (M), SM–DO (H), and SM–DO (C) significantly reduced brain water content (p < 0.001) and infarct volume (p < 0.01), and there was a tendency to reduce brain water content and infarct volume in SM–DO (L), but there were no statistically significant differences. The efficacy of SM–DO showed a dose-effect-dependent relationship.
Optimal ratio of SM–DO improved brain morphology in MCAO mice
Morphological examination of brain tissue showed (Fig. 6H) that the brain tissue of mice in the sham group had a clear structure; the cells did not show any obvious abnormality; and the neurons were arranged in a dense and orderly manner, with regular morphology, a large central nucleus, and a clear contour. In the model group, the brain tissue had a sparse structure; disorganized neurons were arranged in a disordered manner; the nuclei of the cells were deeply stained; the solidification and contraction were unclear; and the cellular shrinkage caused cracks and vacuolization. Compared with the model group, SM–DO (L), SM–DO (M), SM–DO (H), and SM–DO (C) treatments resulted in normalized cell structure and a more regular cell outline. Brain cell necrosis was reduced; nuclei were mildly solidified; peripheral fissures and interstitial vacuoles were reduced to different degrees; and nuclear staining became lighter. These indicated that the optimal ratio of SM–DO could improve the pathomorphology of brain tissue.
Optimal ratio of SM–DO reduced the release of LDH and NSE in MCAO mice
Detection of LDH (Fig. 6I), NSE levels (Fig. 6K) in serum and LDH (Fig. 6J), NSE levels (Fig. 6L) in brain tissue in mice showed that LDH and NSE levels in serum and brain tissue of mice in the model group were significantly higher (p < 0.001) compared to the sham group, suggesting that MCAO led to the damage of the brain cells in mice. Compared with the model group, SM–DO (M), SM–DO (H), and SM–DO (C) significantly reversed LDH and NSE levels in serum and brain tissue (p < 0.05), and SM–DO (L) significantly decreased LDH levels in brain tissue (p < 0.001). For SM–DO (L), there was a decreasing trend in the levels of serum LDH and NSE and the level of NSE in brain tissue, but no statistical difference.
Experimental validation
Experimental validation of the obtained optimal ratios of SM and DO was carried out to examine the actual predictive effect of the statistical model, and the results are listed in Table 3.
Analysis of Differences Between Measured and Predicted Values
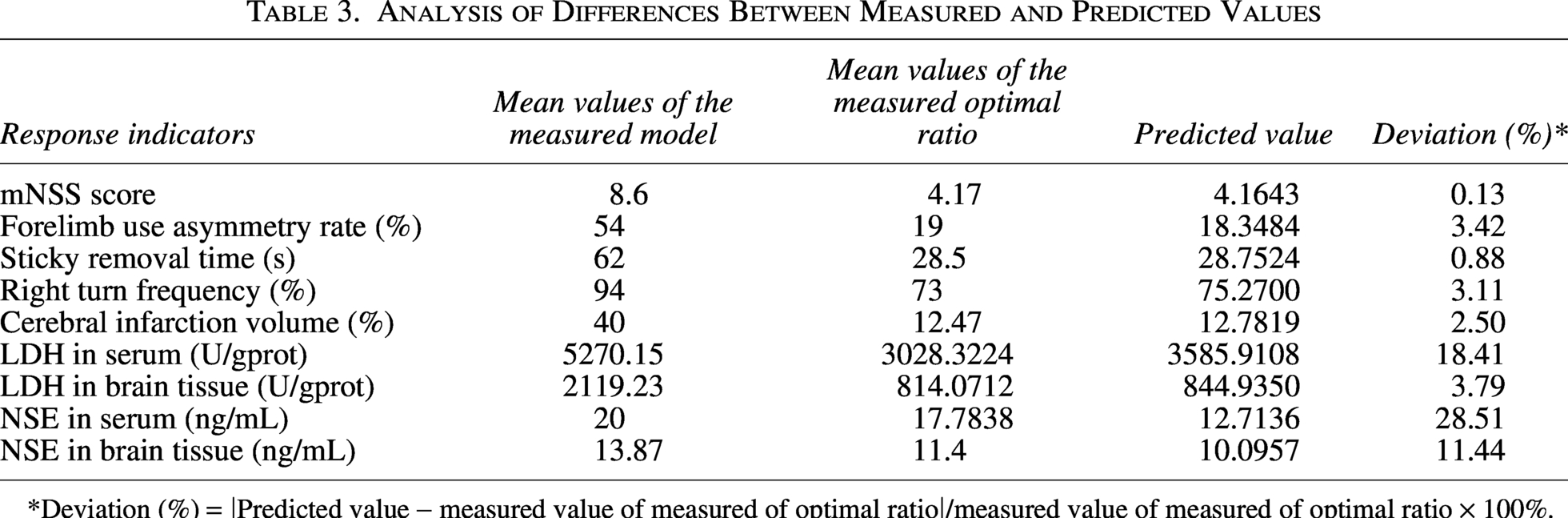
*Deviation (%) = |Predicted value − measured value of measured of optimal ratio|/measured value of measured of optimal ratio × 100%.
The validation results showed that the deviations of the measured mean values of the optimal ratio of the mNSS score, the forelimb use asymmetry rate, the sticker removal time, the right turn frequency, the volume of the cerebral infarction, and the LDH levels in tissue from the predicted values were <5%. The deviations of the measured mean values of the optimal ratio of LDH, NSE levels in serum, and NSE levels in brain tissue from the predicted values were 18.41%, 28.51%, and 11.44%. The measured mean values of the optimal ratio were significantly lower than those of the model (p < 0.05), indicating that the optimal ratio predicted by the model was effective in modulating the response indicators.
Discussion
In recent years, BBB microfluidic chip models have been gradually applied in vitro for studying the pathogenesis of brain diseases, evaluating drug permeability, and screening new drugs. By recreating the cerebral vascular microenvironment and simulating physiological fluid flow in a controllable manner, the BBB microfluidic chip model can mimic the basic physiological structure and function of the in vivo BBB. This study established an in vitro BBB model by combining mouse brain microvascular endothelial cells with microfluidic chip technology. The permeability behavior of six effective components of TCM (liquiritigenin, formononetin, naringenin, lithospermic acid, salvianolic acid A, and salvianolic acid B) was investigated. The results showed that the effective components of DO, namely liquiritigenin, formononetin, and naringenin, all had varying degrees of permeability, suggesting that the effective components in DO formula granules can penetrate the BBB to exert therapeutic effects. In the penetration experiment of SM effective components, lithospermic acid, salvianolic acid A, and salvianolic acid B were not detected. This result may be attributed to either their low content in the sample or their failure to cross the BBB. Lithospermic acid, salvianolic acid A, and salvianolic acid B are macromolecular polyphenolic compounds with high molecular weight, strong polarity, and low lipophilicity. Given the strict lipophilicity-dependent screening mechanism of the BBB, these macromolecular substances can hardly cross the intact BBB into the brain parenchyma.20,21 Although these compounds exhibit low direct BBB permeability, they may exert neuroprotective effects through indirect pathways, including peripheral regulation, BBB protection, and anti-inflammatory action.22,23 In TCM theory, DO is pungent and warm in nature, with a fragrant aroma that can penetrate deeply. It is known for its property of “guiding medicine upward” and facilitating the transmission of drug effects to the head and face, clearing orifices. Studies have shown that the effective components in DO have the ability to penetrate the BBB. They may improve the permeability of the BBB by regulating cell membrane fluidity and inhibiting the activity of efflux transporters. 24 This suggests that under the pathological conditions of IS, the synergistic combination of SM and DO can promote the delivery of water-soluble phenolic acids and other components from SM into the brain, thereby exerting neuroprotective effects.
IS is one of the most common cerebrovascular diseases in China, with the second-highest morbidity rate worldwide. Due to its high mortality and disability rate, it poses a serious economic and health burden on society. 25 TCM offers a theoretically grounded approach to treating IS, with an herb pair demonstrating unique therapeutic advantages through synergistic interactions. As articulated in TCM theory: “Individual herbs possess distinctive properties, while combinations of herbs achieve coordinated efficacy.” The combination of herb pairs embodies the basic theories of TCM such as the four natures, five flavors, and meridian tropism, which are major features of TCM prescriptions and clinical practice. 26 SM–DO is a clinically common herbal pair with circulating blood and transforming stasis for the treatment of cardiovascular diseases. Our research group has demonstrated that SM–DO has cardioprotective effects. In TCM theory, the concept of “the heart governing the mind” highlights that during the process of brain thinking, the heart also plays a decisive role. There is a connection through blood vessels between the brain and the heart, and the circulation of blood is dominated by the heart. Only when the brain receives blood can it perform the function of governing the mind. In modern medical theory, the heart and the brain are closely connected through blood circulation, the nervous system, hormonal signals, and so on, interacting physiologically and influencing each other pathologically. 27 Therefore, this study investigates the role of SM–DO in the treatment of IS through the MCAO mouse model.
The MCAO model28,29 prepared by the thread embolization method can avoid the damage caused by craniotomy. The ischemic site is constant, and the time of ischemia and reperfusion can be accurately controlled. Moreover, its pathogenesis is relatively closer to that of clinical IS. Therefore, this model has been widely used to study the protective effect of drugs against IS-induced damage. In TCM, IS is divided into seven major types: wind-phlegm-fire hyperactivity, wind-fire disturbance, phlegm-heat viscera solidity, wind-phlegm-stasis obstruction, phlegm-dampness obscuring the mind, qi deficiency and blood stasis, and yin deficiency and wind driven. The MCAO model established by the thread embolization method causes infarction of the middle cerebral artery, which leads to hemodynamic stagnation and consequent blood stasis. Following blood stasis, impaired body fluid metabolism leads to persistent condensation of fluids, ultimately forming phlegm, and also a pathological cycle emerges wherein phlegm aggravates stasis and stasis generates phlegm, resulting in phlegm-stasis intermingling. Additionally, perioperative stress responses severely deplete qi and blood. In this model, the predominant TCM syndrome patterns include wind-phlegm-stasis obstruction syndrome, qi deficiency with blood stasis syndrome, and wind-phlegm obstructing collaterals syndrome, so the animal models exhibit characteristic TCM clinical manifestations, including hemiplegia, sensory deficits, and spasticity. 30 In IS, elevated levels of NSE reflect neuronal damage, and elevated levels of LDH reflect brain tissue damage. TCM holds that wind-phlegm-stasis obstruction is the pathological basis leading to poor qi-blood circulation and occlusion of the brain orifices. This syndrome may contribute to cerebral microcirculatory dysfunction, exacerbating neuronal and brain tissue damage, thereby elevating levels of NSE and LDH. In this study, the MCAO mouse model was prepared, and the behavioral evaluation after ischemia/reperfusion (I/R) showed that the MCAO mice showed circumduction or even tilting toward the paretic side, weakening of visual and tactile sensation, loss of reflexes, and dystonia. Elevated levels of NSE and LDH in serum and brain tissues were detected by the kit, which suggests that the MCAO mouse model has been successfully prepared, and that it showed phlegm-stasis and was consistent with the wind, phlegm, and stasis syndrome pattern.
Tong et al. 31 found that when SM and DO were paired in a ratio of 3:1, it could significantly improve cerebral I/R injury and exert neuroprotective effects. Further studies by Wang et al. 32 showed good clinical efficacy in treating patients who have experienced stroke when SM was compounded with DO in a ratio of 5:1. The above studies suggest that SM–DO has a brain-protective effect, but the existing studies on SM–DO for cerebrovascular diseases have a wide range of dispensing ratios and a lack of consistency, making it difficult to form a clear clinical practice.
Mixture design is a research method to quickly explore the optimal ratio of the components that make up the mixture to achieve the desired response indicator. Mouhcine et al. 33 used the mixture design to study the antimicrobial activity of essential oil formulations of thyme, rosemary, and myrtle in the hope of increasing the susceptibility of Salmonella typhimurium strains and thus exerting optimal antimicrobial activity. The fitted regression model predicted that the three blends in the ratio of 55%:0%:45% showed the highest susceptibility to S. typhimurium, which was close to the measured values. Chraibi et al. 34 used the mixture design to study the optimal ratio of the antimicrobial effects of a mixture of essential oils of thyme, myrtle, and Artemisia alba. The fitted regression model predicted that, first of all, the best inhibitory effect against Escherichia coli was observed when the ratio of thyme to myrtle was 60%:40%. Second, the best antibacterial effect on Staphylococcus aureus was observed when the ratio of thyme to A. alba was 72%:28%. Third, when thyme and A. alba were used at a ratio of 75%:25%, the best antibacterial effect on Candida tropicalis was observed. The measured results showed that the two essential oils are used in combination to improve their antibacterial effect. Mechchate et al. 35 used the mixture design to optimize the combination of catechin, epicatechin, and rutin to obtain a new antidiabetic formulation. The results showed that a binary mixture of 25% rutin and 75% epicatechin significantly reduced blood glucose levels in mice with tetraoxone-induced diabetes, demonstrating better efficacy than glibenclamide without adverse reactions. The above study shows that the mixture design is useful for the development of multi-component formulations and the search for the optimal ratio of components. In the present study, we applied the strategy of mixture design, using the MCAO mouse model, with SM and DO as the constituent substances, and mNSS score, forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarction volume, LDH, and NSE as the response indicators. Through multi-objective synchronization optimization, the optimal ratio of SM–DO for IS treatment was determined to be 0.61:0.39. The experimental validation results showed that the results of the optimal ratio of SM–DO (H) produced superior results for mNSS score, forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarction volume, cerebral edema, LDH and NSE levels in brain tissue, as well as NSE level in serum, compared to the clinically available maximum dosage group. This suggests that the mixture design can provide the optimal ratio of SM–DO for the treatment of IS.
In the regression model, the coefficient of the interaction term reflects the effect of the interaction between the two components on the response indicator. In this study, the optimization objective is to minimize the response value. The positive coefficient indicates antagonism between the two components, while the negative coefficient suggests synergy. And the larger the absolute value of the coefficient is, the stronger the interaction they have. The results showed that, except for the model corresponding to the NSE level in serum, the other eight regression models contained interaction terms, with negative coefficients, suggesting that SM and DO may have a synergistic effect to reduce the values of the corresponding response indicators. The model corresponding to the NSE level in serum did not contain the coefficients of the interaction terms, suggesting that the interaction regulation of NSE level in serum by the combination of SM and DO did not reach statistical significance.
In the regression model, R2 (coefficient of determination) and adjusted R2 (adjusted coefficient of determination) are important indicators for assessing the goodness of fit of the model. The results showed that the minimum R2 value of the model was 0.83 and the minimum adjusted R2 value was 0.76, both of which were closer to 1 (the theoretical maximum value), and the adjusted R2 had no obvious decrease compared with R2, suggesting that the regression of each model was well fitted and no overfitting was observed.
The Cox response trace plots show the effect of each component on the response indicator and are mainly used to reflect the individual effects of each component in the mixture design. The Cox response trace plots on the nine response indicators consistently showed that the optimal pairing of the two is possible only when the share of SM comprises a greater proportion than DO.
Multi-objective synchronization optimization is a method to determine the optimal ratio of each component based on the comprehensive evaluation of multiple response indicators. The results of this study showed that the optimal ratio of SM and DO obtained by multi-objective synchronization optimization was 0.61:0.39 (SM:DO), and the composite desirability was 0.8112. Under the conditions of this ratio, the high individual desirability of the response indicators was observed for mNSS score, forelimb use asymmetry rate, sticker removal time, cerebral infarcts volume, the LDH and the NSE levels in brain tissue, and the LDH level in serum, while the right turn frequency and NSE level in serum response indicators had low desirability. These results suggest that the optimal solution obtained by multi-objective synchronization optimization is a comprehensive optimal solution taking into account the response indicators, and it may not guarantee that the single indicator reaches the optimal.
The optimal ratios obtained from the model estimation were experimentally verified, and the results showed that the optimal ratios of the SM–DO (H) significantly reduced the values of the response indicators compared with those of the model group, and the p-values were all >0.05. In terms of the six response indicators of the mNSS score, forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarcts volume, and the LDH level in brain tissue, the measured values of the optimal ratios and the predicted values were relatively similar. This suggests that the obtained model has good reliability. For LDH and NSE levels in serum and NSE level in tissue, the measured values deviated from the predicted values to a certain extent, probably due to the small sample size, but it still has great significance in the search of a ratio solution for IS treatment.
Behavioral evaluation of neurological deficits is an important indicator for judging the severity of cerebral ischemia, 36 which mainly includes the evaluation of the conscious state, movement, sensation, vision, and neurological reflexes, 37 and the guidelines related to cerebral ischemia point out that the evaluation of neurological function should focus on the comprehensive assessment of multiple methods.38,39 Therefore, in this study, four behavioral evaluation methods were used, which are named as mNSS score, corner test, sticker removal test, and cylinder test, so we could utilize multiple indicators to comprehensively evaluate the success of modeling in MCAO mice and the effectiveness of SM–DO for treating IS.
The most widely used animal model of stroke produces focal lesions in the parietal cortex and striatum via transient or permanent MCAO. The sensory and motor areas of the cerebral cortex are crucial for receiving external stimuli and executing motor functions, while also playing a central role in higher thought and behavior. The primary function of the striatum is to regulate muscle tone and coordinate a variety of fine and complex movements. The cerebral cortex is the highest level center that regulates somatic movement or controls somatic movement. Studies have shown that IS damages the cerebral cortex through multiple mechanisms, leading to neuronal death, inflammatory responses, oxidative stress, apoptosis, and altered synaptic plasticity, consequently causing motor and cognitive dysfunction. In this study, we performed tail lifting test and walking test on mice through the locomotor test in mNSS, observing whether the forelimbs and hindlimbs were flexed, whether the head would deviate from the vertical axis within 30 seconds, whether the mice could walk normally in a straight line, and whether they turned around or tilted to the paralyzed side. The number of times the mice used both forelimbs when their palms were touching the wall of the cylinder during the cylinder test in order to comprehensively assess balance, reflexive function, and sensory function in mice. The results showed that after MCAO, the mice exhibited several notable impairments. These included the inability to fully extend their forelimbs and hindlimbs, a decrease in resistance when pushing toward the paralyzed side, a tendency to turn or tilt toward the paralyzed side when lifting their tails, an absence of spontaneous activities such as drinking and eating, and a deviation of their heads from the vertical axis within 30 seconds. Additionally, the mice were unable to walk normally in a straight line and exhibited a greater propensity to use the limbs on the healthy side when exploring the cylinders. The results showed that when using the mNSS score and cylinder test as the response indicators, all the SM–DO groups had a tendency to reduce the mNSS score and the forelimb use asymmetry rate, and the optimal ratio was an equal ratio of SM and DO. This is consistent with previous findings, which reported that SM has the ability to reduce neuroinflammation, minimize neuronal cell damage, modulate neurotransmitters, and reduce cerebrospinal fluid marker deposition, thereby protecting against cortical damage. 40 Meanwhile, DO and its active components can improve cerebral blood flow while exhibiting antioxidant, anti-inflammatory, and neuroprotective effects, consequently enhancing synaptic plasticity and neuronal function in the cerebral cortex. 41 It is suggested that SM–DO may improve blood flow in the cerebral cortex, promote the recovery of motor function and voluntary activity in MCAO mice, thus alleviating the prognostic symptoms of IS and exerting a therapeutic effect on IS.
The striatum is an important component of the basal ganglia, and its main function is to regulate muscle tone and coordinate a variety of advanced fine and complex movements. 42 Studies have shown that damage to the striatum after IS leads to muscle weakness, impaired motor control of the affected limb, limited range of motion, and muscle pain. 43 In this study, we recorded the length of time taken by mice to remove the adhesive stickers from the forelimbs and observed the number of times when the mice turned to the paralyzed side at the corner after the bilateral tentacles. These tests provided a comprehensive evaluation of balance, reflexes, and other motor coordination, the degree of dystonia, and the sensory function of the mice. The results showed that after MCAO, the mice developed limb movement disorder and decreased balance, and the removal time of the sticky sticker was substantially prolonged. When placed before a corner, the mice entered deep into the corner, and the mice had abnormal balance, reflex function, and sensory function, such as turning to the injured side several times after the bilateral tentacles were stimulated. The study showed that different ratios of SM–DO improved the neurological function of MCAO mice, suggesting that SM–DO may play a role in the treatment of IS by alleviating striatal injury, restoring the integrity of the basal ganglia loop, and promoting the restoration of motor function and voluntary activity in MCAO mice, which may, in turn, alleviate the prognostic symptoms of IS. In addition, the results of this study showed that the SM content in the optimal ratio was contained a higher proportion of SM when the sticker removal test and the cylinder test were used as the response indicators, and it was hypothesized that tanshinone I, the SM active ingredient, could improve the locomotor function of the mice and maintain the normal level of neurotransmitters in the striatum.
Cerebral ischemic injury leads to excessive storage of fluid content in the brain tissue, which causes a pathological state of increased brain volume, with greater cellular interstitial and cellular permeability. Measurement of brain water content can determine the extent of cerebral ischemic injury. The reaction between TTC and tissue dehydrogenase can be used to identify the activity of tissue, and the degree of infarction of brain tissue can be identified according to the location of TTC staining and the depth of staining. The degree of ischemic injury can be quantified by the staining results. HE staining can clearly observe the morphology, structural changes, and damage of neurons in the cerebral cortex for all experimental groups. NSE and LDH are abundantly present in the cytosol of neuron cells. After cellular damage caused by ischemia, NSE and LDH are first released into the interstitial space of cells, then diffused into the cerebrospinal fluid, and finally enter the blood and brain tissues through the damaged BBB, causing a rapid elevation of NSE and LDH levels in serum and brain tissue.44,45 Therefore, elevated NSE and LDH levels in serum and brain tissue may reflect cerebral ischemic injury. It has been found that elevated NSE and LDH levels are closely associated with increased neurological function scores, cerebral swelling, and volume of cerebral infarction. 46 The results of this study showed that when cerebral infarction volume, NSE and LDH levels in brain tissue were used as the response indicators, the optimal ratio of SM and DO was determined to be 1:1. SM–DO decreased NSE and LDH levels in brain tissue, reduced cerebral infarction volume, and improved neuronal and pathological damage of the brain tissue significantly, which may be related to the existence of interactions between SM and DO. Wang et al. 47 investigated the interaction between SM and DO in Astragali Sen Yi-Qi Dropping Pills, demonstrating that DO can improve the absorption and utilization of danshensu from SM, and transfer danshensu to the liver and the brain so as to improve therapeutic efficacy, which provided a basis for the elucidation of the interaction between “SM” and “DO” in the drug. When NSE and LDH levels in serum were used as the response indicators, the optimal ratios contained a higher proportion of SM. These findings suggest that SM may play a more critical role in reducing neuronal damage and lowering serum neurotoxicity biomarker levels. In addition, the results showed that the optimal ratio of SM–DO could reduce NSE and LDH levels in serum and brain tissue, decrease cerebral infarction volume and brain water content, and improve neuronal and pathological damage of the brain tissue to varying degrees in a dose-effect-dependent relationship. These findings suggest that SM–DO can effectively alleviate brain injury and neurological dysfunction after IS, exerting comprehensive neuroprotective effects.
The main purpose of this study was to screen the optimal ratio of SM–DO for the treatment of IS, and thus, no positive drug control was included. However, after completing this primary objective, we further explored the specific mechanism underlying the neuroprotective effect of the optimal SM–DO ratio against IS. In this mechanistic study, a positive drug control treated with butylphthalide (NBP) was established. The experimental results showed no significant difference between the optimal SM–DO ratio group and the NBP group, suggesting that the optimal ratio identified in this study exerts a neuroprotective effect comparable to that of the clinically used positive drug. These findings further validate the efficacy and therapeutic advantages of the optimal SM–DO ratio (see Supplementary Data).
We applied five ratios of SM and DO designed by Minitab 17 software to the MCAO mice. The results showed that when using mNSS score, forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarct volume, LDH, and NSE as the response indicators, the groups with different ratios of SM–DO (0.5:0.5, 0.75:0.25, 0.25:0.75) had significantly better efficacy than the groups with SM and DO alone (1:0, 0:1), suggesting that SM–DO combination was more effective than SM and DO alone. There was no statistically significant difference in the comparison of the optimal ratio of SM–DO (H) and the maximum dose of SM–DO available in the clinical (C), indicating that the mixture design can provide a new strategy to find the optimal ratio of SM and DO for clinical IS treatment.
Conclusion
In the study, we used the proportions of SM and DO as independent variables, and mNSS score, forelimb use asymmetry rate, sticker removal time, right turn frequency, cerebral infarction volume, LDH, and NSE as dependent variables to fit a mixture design. The results of simultaneous optimization based on the model showed that the optimal ratio of SM–DO for IS treatment was 0.61:0.39. Further experimental validation showed that SM–DO at the optimal ratio significantly reduced the mNSS score, the recovery of motor function of the left forelimb, the recovery of sensory function of the left palm, the gradual normalization of motor function of the right steering, and the reduction of the volume of cerebral infarction, cerebral edema, and the release of LDH and NSE, suggesting its therapeutic potential in IS. Our findings suggest the possibility of applying the mixture design to explore the optimal ratio of SM–DO for the treatment of IS and provide a new methodological reference for the study of the ratio of TCM herb pairs.
Authors’ Contributions
Z.D., K.L., C.L., and W.L. performed the experiments, investigation, and methodology and contributed to writing—original draft. Q.D., H.Y., H.W., and X.C. performed the data curation. P.W. and M.X. supervised all research and contributed to writing—review and editing. M.X. contributed to funding acquisition, project administration, and writing—review and editing. All data were generated in-house, and no paper mill was used. All authors agree to be accountable for all aspects of work, ensuring integrity and accuracy.
Footnotes
Author Disclosure Statement
The authors have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This work was supported by the projects of the
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.