
Abstract
Sarcopenia attenuates independence and mobility in older adults, and scalable nonpharmacological interventions are needed. This trial evaluated whether a 12-week exercise program improves activities of daily living, muscle mass and strength, physical performance, and systemic inflammation in older adults with sarcopenia. In this 12-week randomized controlled trial, adults aged 60–75 years with sarcopenia were randomized 1:1 to a control group or an exercise group. The exercise group performed postprandial multicomponent training (37 min/session, 3 days/week), combining resistance and aerobic exercise. Outcomes were measured at baseline and at week 12. The primary endpoint was the Modified Barthel Index (MBI). Secondary endpoints were Appendicular Skeletal Muscle Mass Index (ASMI), handgrip strength, the 6-minute walk test (6MWT), the Timed Up and Go Test (TUGT), and serum interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α). Of 224 enrolled participants, 120 were randomized and 94 were analyzed (control, n = 49; exercise, n = 45). At week 12, the exercise group showed higher MBI (68.89 ± 9.60 vs. 62.02 ± 10.35; p = 0.001), ASMI (6.074 ± 0.904 vs. 5.295 ± 0.739 kg/m2; p < 0.001), and handgrip strength (22.78 ± 5.02 vs. 19.95 ± 4.25 kg; p = 0.009); better 6MWT (395.6 ± 55.6 vs. 363.7 ± 53.8 minutes; p = 0.005), shorter TUGT (6.76 ± 1.41 vs. 7.66 ± 1.55 seconds; p = 0.005), and lower IL-6 (45.21 ± 10.66 vs. 53.73 ± 10.99 pg/mL; p < 0.001) and TNF-α (38.09 ± 8.64 vs. 45.45 ± 8.07 pg/mL; p < 0.001) compared with the control group. These findings suggested that a 12-week regular exercise program improved functional independence, muscle health, mobility, and inflammatory status in older adults with sarcopenia.
Keywords
Introduction
Sarcopenia is a progressive skeletal muscle disorder in older adults, characterized by loss of muscle mass, reduced muscle strength, and impaired physical function.1–4 Epidemiological studies indicate that sarcopenia is highly prevalent in older populations and is closely associated with low habitual physical activity and chronic low-grade inflammation.5,6 Elevated inflammatory cytokines, particularly tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), can promote muscle protein breakdown and impair myofiber regeneration, thereby accelerating muscle wasting.7,8
Exercise is the most effective nonpharmacological intervention for sarcopenia.9–11 Regular exercise, especially resistance training and multicomponent programs that combine aerobic and resistance modalities, can improve muscle mass, strength, and physical performance.12–14 Proposed mechanisms include satellite cell activation, increased muscle fiber cross-sectional area, and favorable modulation of inflammatory cytokines, which may mitigate chronic low-grade inflammation.15–17 Randomized controlled trials have shown that exercise interventions can reduce TNF-α and IL-6 levels while enhancing muscle function. 18 Additionally, exercise may improve activities of daily living (ADL), such as feeding and bathing, and enhance quality of life, which are important outcomes for older adults. 11 However, conventional exercise programs are often constrained by high learning demands, poor adherence, and limited individualization.19–21
Currently, resistance training is recommended as a first-line strategy for the prevention and treatment of sarcopenia because it can effectively reduce inflammation and preserve muscle function.17,22 Previous randomized controlled trials and meta-analyses have shown that exercise, particularly resistance training and multicomponent interventions, improves muscle strength, muscle mass, and physical performance in older adults with sarcopenia.10,20 Multicomponent exercise has also shown benefits in frailty studies, particularly for functional outcomes, with some studies also reporting improvements in inflammatory biomarkers.23,24 However, previous trials have mainly focused on muscle-related outcomes, with less consistent assessment of ADL and circulating inflammatory biomarkers. In addition, variations in diagnostic criteria and intervention delivery have limited direct comparisons across studies. 25 Therefore, practical and feasible exercise protocols for routine care that evaluate functional independence, muscle-related outcomes, physical performance, and inflammatory biomarkers remain underexplored.
This randomized controlled trial evaluated a simple postprandial multicomponent exercise program in older adults with sarcopenia diagnosed using consensus-based criteria. 25 Specifically, we aimed to examine its effects on ADL, muscle mass, muscle strength, physical function, and circulating inflammatory biomarkers. The findings may help inform individualized and scalable strategies for sarcopenia prevention and management.
Materials and Methods
Participants and study design
This was a 12-week randomized controlled trial. The study was approved by Longgang Central Hospital of Shenzhen. Older adults undergoing comprehensive geriatric assessment and routine health examinations were enrolled. Participants with identified sarcopenia who met the eligibility criteria were randomized 1:1 to a control group (usual care) or an exercise group (regular exercise). Data were collected and assessed at baseline and at week 12 postintervention.
Diagnosis of sarcopenia
Sarcopenia was diagnosed according to the Chinese Expert Consensus on Prevention and Intervention for Sarcopenia in Older Adults. 26 Screening was first performed using SARC-F or SARC-CalF. A SARC-F score ≥4, a SARC-CalF score ≥11, or a calf circumference <34 cm in men and <33 cm in women was considered positive. Individuals who screened positive then underwent further evaluation of muscle strength, physical function, and muscle mass. Muscle strength was assessed by dominant-hand handgrip strength, with values <28 kg for men and <18 kg for women defined as low muscle strength. Physical function was evaluated using the 6-minute gait speed test, and a gait speed <1.0 m/s was defined as impaired physical function. Muscle mass was measured by dual-energy X-ray absorptiometry (DXA), and low muscle mass was defined as an appendicular skeletal muscle mass index <7.0 kg/m2 in men and <5.4 kg/m2 in women. Sarcopenia was diagnosed as low muscle mass with either low muscle strength or impaired physical function, whereas severe sarcopenia was defined by all three abnormalities.
Eligibility criteria
Participants were included if they met the following criteria: (1) age 60–75 years with complete clinical data; (2) sarcopenia diagnosed according to the Chinese Expert Consensus on Prevention and Intervention for Sarcopenia in Older Adults (2023) 26 ; (3) normal cognitive function; (4) ability to participate in regular exercise; and (5) written informed consent.
Participants were excluded from the analysis if they met any of the following criteria: (1) safety concerns during testing, including severe osteoporosis or low back pain with lower-limb functional limitation; (2) recent fracture surgery; (3) acute exacerbation of a chronic disease; (4) severe cardiovascular, cerebrovascular, or pulmonary disease within the past year; (5) regular exercise before the intervention; or (6) high exercise-related risk assessed by physicians, not recommended for exercise intervention.
Exercise protocol
The exercise group performed postprandial exercise for 12 weeks, 3 days per week, with ≥24 hours between sessions. All sessions were scheduled 1.5–2 hours after lunch. Each 37-minute session included 5 minutes warm-up (slow walking), 20 minutes of resistance exercise (wall push-ups, sit-to-stand, heel raises, and lifting exercises; 5 minutes each), 10 minutes of aerobic exercise (slow jogging), and 2 minutes of cool-down (slow walking). A hospital–home combined supervision model was used to improve adherence. The exercise group was prescribed a total of 36 sessions (3 sessions/week for 12 weeks). During the first 4 weeks, all sessions were conducted in the hospital under direct supervision by research staff to ensure correct technique and appropriate intensity. From week 5 onward, participants continued the exercise program at home. Home-based sessions were monitored using an exercise check-in app, through which participants uploaded heart rate data and exercise photographs. Research staff reviewed the uploaded records daily, conducted weekly telephone follow-up, and performed on-site reassessments every 2 weeks to ensure exercise quality.
Exercise intensity was evaluated using heart rate reserve: target heart rate (beats/min) = 40%–59% × (HRmax − HRrest) + HRrest, where HRmax = 220 − age. Participants wore a heart rate monitor to maintain moderate exercise intensity during each session. Perceived exertion was also assessed using the Borg Rating of Perceived Exertion scale, with a target score of 12–14, indicating slight breathlessness while still being able to speak comfortably.
The control group maintained their usual lifestyle throughout the 12-week study and received no exercise intervention. Research staff conducted telephone follow-up every 4 weeks to record general health status and adverse events, without offering advice on exercise, nutrition, or lifestyle.
Outcome measures
All outcomes were measured at baseline and at week 12.
Handgrip strength
Dominant-hand handgrip strength was measured using an electronic dynamometer (Guangdong Senssun Weighing Apparatus Group Ltd., Guangdong, China). Participants stood with their upper arms held vertically. Three measurements were taken, and the highest value was recorded.
Muscle mass and Appendicular Skeletal Muscle Mass Index
Appendicular skeletal muscle mass was measured by DXA (Norland XR-800, Fort Atkinson, WI, USA), and ASMI was calculated. ASMI = appendicular skeletal muscle mass (kg)/height 2 (m2).
Six-minute walk test
The test was conducted on a 30-m flat corridor with cones placed every 3 m. After 10 minutes of seated rest, blood pressure and heart rate were measured. Participants were instructed, using standardized prompts, to walk as fast as possible without running or jumping. Distance was recorded every minute, and blood pressure and heart rate were remeasured immediately after the test.
Timed Up and Go Test
Participants started seated in a chair with armrests and a backrest (seat height ∼43 cm). A marker was placed 2.44 m in front of the chair. Timing started when the participant’s back left the backrest and ended when it contacted the backrest after walking to the marker, turning, and returning. Two trials were performed with 1–2 minutes of rest, and the mean time was used.
Serum inflammatory markers
Fasting venous blood samples were collected in the morning (7:00–9:00 AM) at baseline and after 12 weeks of intervention, following an overnight fast of 8–12 hours. Blood samples were immediately placed in EDTA anticoagulant tubes and centrifuged at 3000 rpm for 10 minutes at 4°C. The supernatant was aliquoted and stored at −80°C until analysis. All samples were measured in the same batch to reduce interassay variability. Serum TNF-α (ab181421, Abcam, Cambridge, UK) and IL-6 (ab178013, Abcam) were quantified by enzyme-linked immunosorbent assay (ELISA) according to the manufacturer’s instructions. For TNF-α, the assay sensitivity was 4.32 pg/mL, with a linear range of 15.63–1000 pg/mL; the intra and interassay coefficients of variation were both <5%. For IL-6, the corresponding values were 1.6 pg/mL, 7.8–500 pg/mL, and <3%, respectively.
Adherence and safety
Adherence was evaluated by the number of completed exercise sessions and the proportion of participants who achieved the prescribed exercise dose. Safety was monitored throughout the 12-week intervention by recording adverse events during both hospital- and home-based training. Exercise dose attainment was defined as achieving both the target heart rate range (40%–59% of heart rate reserve) and the target Borg score (12–14) in at least 80% of prescribed sessions.
Modified Barthel Index
ADL were assessed using the Modified Barthel Index (MBI), with scores ranging from 0 to 100, where higher scores indicate greater functional independence.
Statistical design and randomization
Eligible participants were randomly assigned in a 1:1 ratio to the control or exercise group using simple randomization. The random sequence was generated by an independent statistician who was not involved in participant recruitment, intervention delivery, or outcome assessment. Allocation was concealed using sequentially numbered, sealed, opaque envelopes, which were opened by a research nurse after written informed consent was obtained. Due to the nature of the intervention, participants and intervention staff could not be blinded. However, outcome assessors were blinded to group allocation and conducted assessments in a separate room without access to intervention records. Statistical analyses were performed on participants who completed the 12-week intervention and all outcome assessments.
Sample size calculation
The MBI was used as the primary endpoint for sample size estimation. An 8-point greater mean improvement in MBI was expected in the exercise group compared with the control group after 12 weeks. With a two-sided α = 0.05, 80% power, 1:1 allocation, and an anticipated 15% dropout rate, the required sample size was 43 participants per group. This was calculated using PASS 11.0 (NCSS Statistical Software, Kaysville, UT) using a two-sample independent t-test.
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as n (%). For the primary outcome (MBI) and all secondary outcomes, between-group comparisons at week 12 were performed using analysis of covariance (ANCOVA), with group as the fixed factor and the corresponding baseline value as a covariate. Within-group changes from baseline to week 12 were evaluated using paired t-tests. Categorical variables were compared using Fisher’s exact test. Effect sizes are reported as adjusted between-group differences with 95% confidence intervals (CIs). All tests were two-sided, and p < 0.05 was considered statistically significant. Because multiple secondary outcomes were assessed without adjustment for multiple comparisons, these analyses should be considered exploratory.
Results
Participant flow and study attrition
Among 224 older adults with sarcopenia, 104 volunteers (46.4%) were excluded because they were ineligible (n = 58) or declined participation (n = 46), as shown in Figure 1. The remaining 120 participants were randomized in a 1:1 ratio to the control or exercise group (n = 60 per group) and completed baseline assessment. During the 12-week intervention, 11 participants in the control group (18.3%) and 15 in the exercise group (25.0%) withdrew from the study (control: two voluntary withdrawals, six lost to follow-up, and three unable to continue for personal reasons; exercise: seven voluntary withdrawals, four lost to follow-up, and four unable to continue for personal reasons). Consequently, 49 participants in the control group (81.7%) and 45 participants in the exercise group (75.0%) completed follow-up and were included in the final analysis.
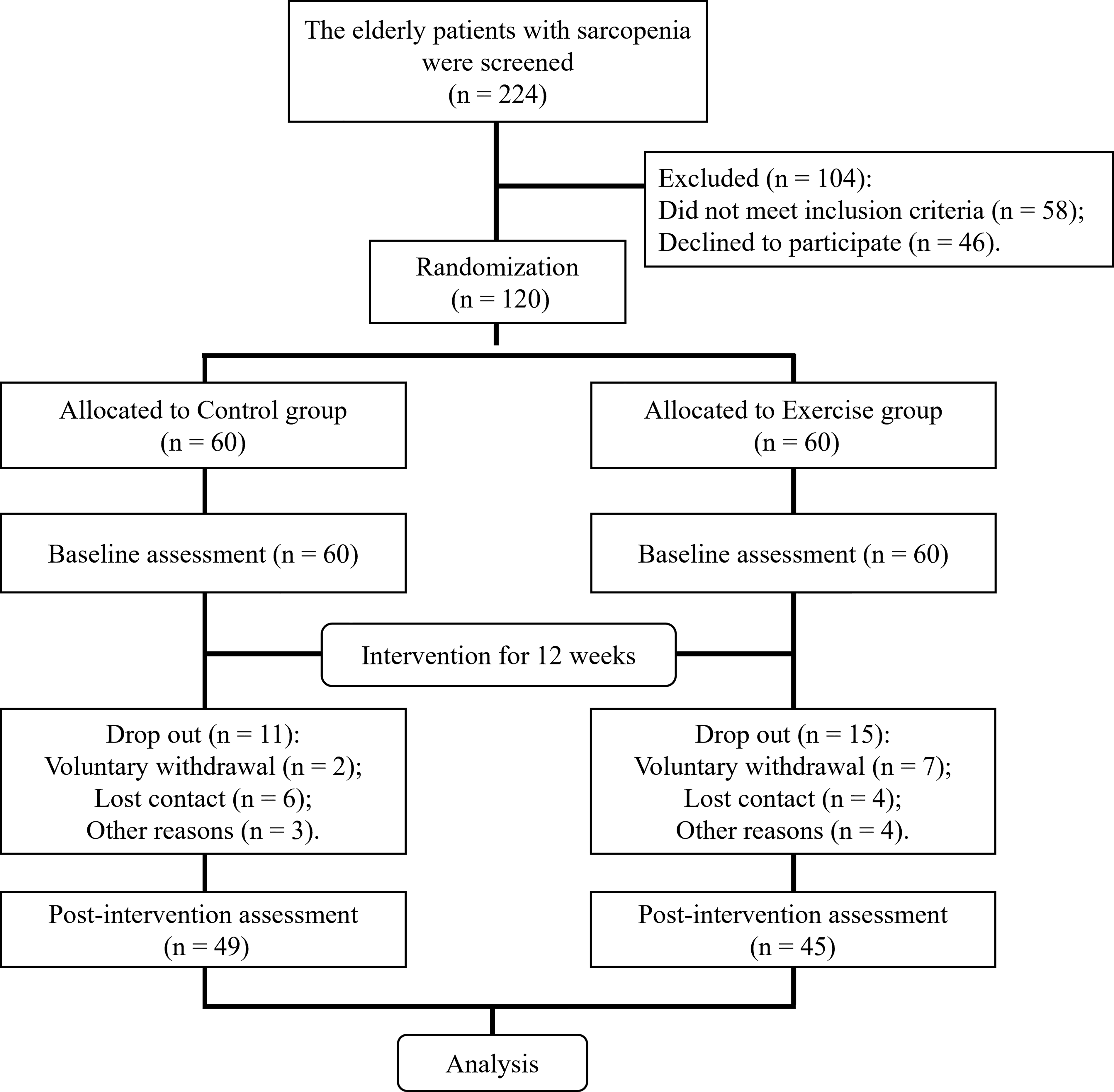
Flow diagram of the study.
Adherence, exercise dose attainment, and safety
The exercise group was prescribed 36 sessions over 12 weeks. The mean number of completed sessions was 32.4 ± 3.1, corresponding to an overall adherence rate of 90.0%. In total, 82.2% of participants completed at least 30 sessions, and 95.6% completed at least 27 sessions. Regarding exercise dose attainment, 92.3% of participants in the exercise group achieved both the target heart rate range and the target Borg score in at least 80% of completed sessions. During the 12-week intervention, three mild adverse events were reported in the exercise group, all of which were mild postexercise muscle soreness that resolved completely within 24–48 hours after rest and stretching. No serious adverse events, including falls, fractures, or cardiovascular events, occurred. No study-related adverse events were reported in the control group.
Baseline characteristics of the study participants
To assess baseline comparability before the 12-week intervention, demographic and clinical characteristics, inflammatory biomarkers, and sarcopenia-related measures were compared between the control and exercise groups as shown in Table 1. The groups were similar in age and body mass index, with no differences in sex or marital status. Comorbidity profiles were comparable, including hypertension, diabetes, coronary heart disease, hyperlipemia, and prior-year falls. Baseline TNF-α and IL-6 did not differ between groups, nor did ASMI, handgrip strength, 6MWT distance, TUGT time, or MBI. In conclusion, all baseline variables were well balanced between groups, indicating good comparability before the intervention.
Baseline Characteristics of Elderly Patients with Sarcopenia
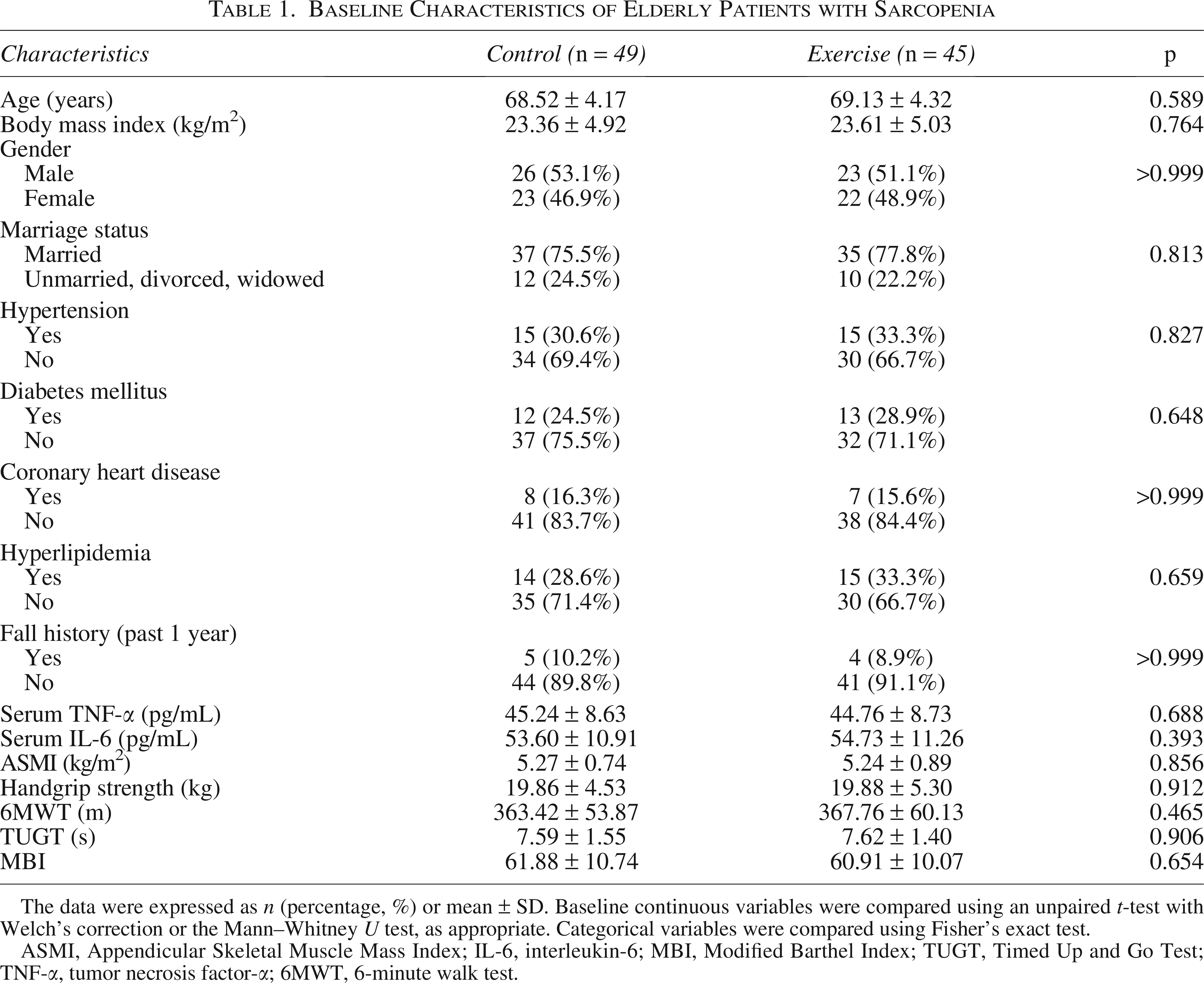
The data were expressed as n (percentage, %) or mean ± SD. Baseline continuous variables were compared using an unpaired t-test with Welch’s correction or the Mann–Whitney U test, as appropriate. Categorical variables were compared using Fisher’s exact test.
ASMI, Appendicular Skeletal Muscle Mass Index; IL-6, interleukin-6; MBI, Modified Barthel Index; TUGT, Timed Up and Go Test; TNF-α, tumor necrosis factor-α; 6MWT, 6-minute walk test.
Effects of 12-week exercise on MBI, ASMI, and handgrip strength
To evaluate the effect of the 12-week exercise intervention on ADL and muscle-related outcomes, changes from baseline to week 12 were assessed within each group, and outcomes at week 12 were compared between groups. In the exercise group, MBI increased after the intervention from 60.91 ± 10.07 to 68.89 ± 9.60 (Δ + 7.98; 95% CI: 7.20–8.75; p < 0.001; Fig. 2A). In the control group, MBI did not change after the intervention (61.88 ± 10.74 to 62.02 ± 10.35; p = 0.688; Fig. 2B). ANCOVA showed that the adjusted between-group difference in MBI at week 12 was 6.87 points (95% CI: 4.23–9.51; p = 0.001; Fig. 2C), indicating a clinically meaningful improvement in ADL. ASMI increased after the intervention in the exercise group from 5.241 ± 0.894 to 6.074 ± 0.904 kg/m2 (Δ + 0.834; 95% CI:0.720–0.948; p < 0.001; Fig. 2D). ASMI remained stable after the intervention in the control group (5.272 ± 0.741 to 5.295 ± 0.739 kg/m2; p = 0.249; Fig. 2E). The adjusted between-group difference in ASMI at week 12 was 0.779 kg/m2 (95% CI: 0.521–1.037; p < 0.001; Fig. 2F). Handgrip strength increased after the intervention in the exercise group from 19.88 ± 5.30 to 22.78 ± 5.02 kg (Δ + 2.90; 95% CI: 2.57–3.23; p < 0.001; Fig. 2G). No significant change was observed after the intervention in the control group (19.86 ± 4.53 to 19.95 ± 4.25 kg; p = 0.268; Fig. 2H). The adjusted between-group difference in handgrip strength at week 12 was 2.83 kg (95% CI: 0.72–4.94; p = 0.009; Fig. 2I). Overall, the 12-week exercise program improved ADL performance, appendicular muscle mass, and muscle strength compared with usual care.
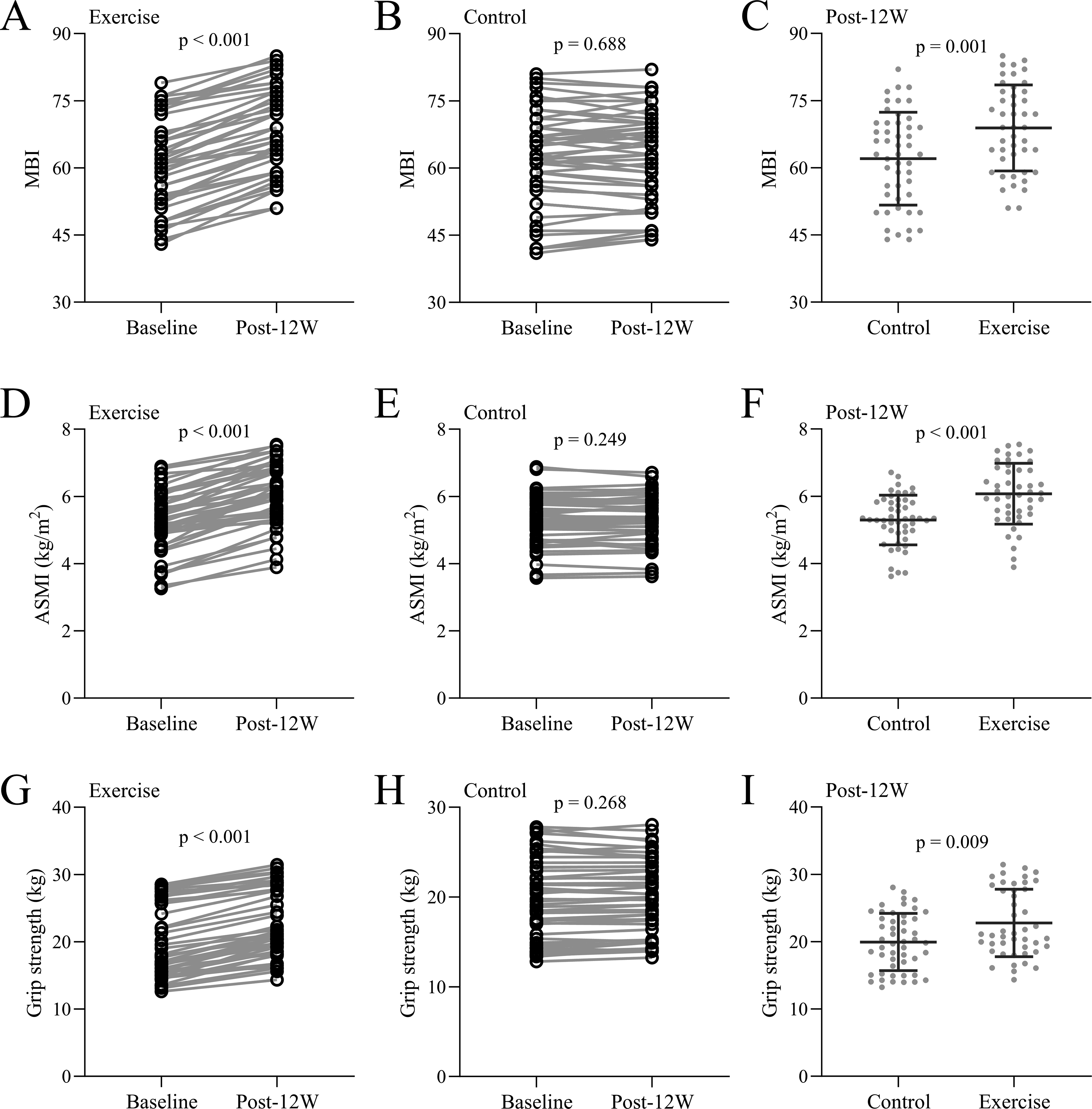
Comparisons of the Modified Barthel Index (MBI) and muscle-related indicators between the two groups after 12-week intervention. Comparisons of MBI between the time of baseline and week 12 in the exercise group
Effects of 12-week exercise on 6MWT and TUGT
To evaluate the effect of the 12-week exercise program on physical function, 6MWT distance and TUGT time were compared within groups (baseline vs. week 12) and between groups at week 12. In the exercise group, 6MWT distance increased after the intervention from 367.8 ± 60.1 to 395.6 ± 55.6 m (Δ + 27.8; 95% CI: 23.7–32.0; p < 0.001; Fig. 3A). No change was observed in the control group after intervention (363.4 ± 53.9 to 363.7 ± 53.8 m; p = 0.805; Fig. 3B). The adjusted between-group difference in 6MWT at week 12 was 31.9 m (95% CI: 10.2–53.6; p = 0.005; Fig. 3C). TUGT time decreased in the exercise group after the intervention from 7.62 ± 1.40 to 6.76 ± 1.41 seconds (Δ – 0.86; 95% CI: −1.01 to −0.71; p < 0.001; Fig. 3D). It did not change in the control group after the intervention (7.59 ± 1.55 to 7.66 ± 1.55 seconds; p = 0.237; Fig. 3E). The adjusted between-group difference in TUGT at week 12 was −0.90 seconds (95% CI: −1.45 to −0.35; p = 0.005; Fig. 3F). Overall, the exercise intervention improved walking capacity and mobility compared with usual care.
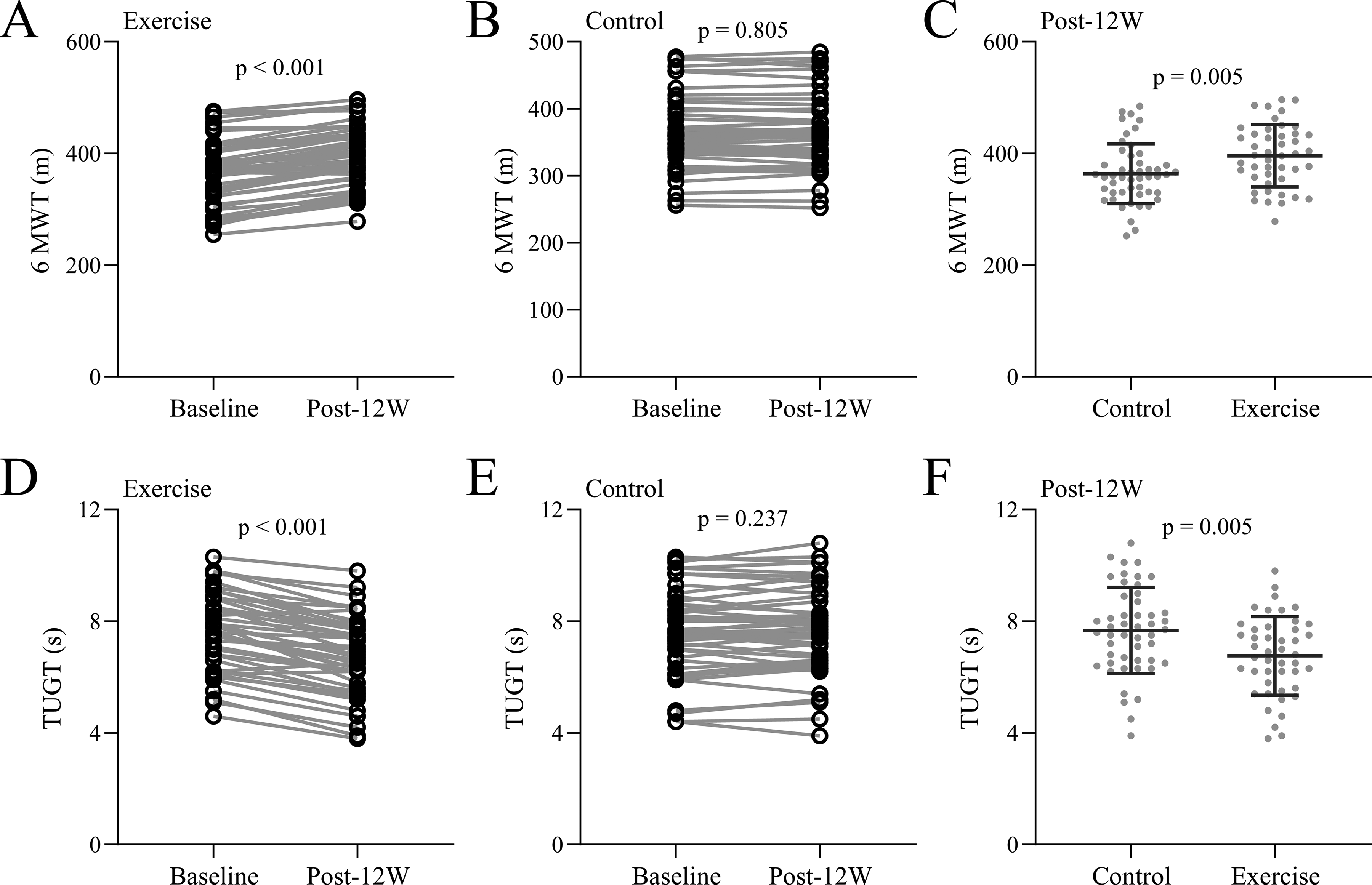
Comparison of physical function indicators. The 6-minute walk test (6MWT) was compared between the time of baseline and week 12 in the exercise group
Effects of 12-week exercise on serum IL-6 and TNF-α
To evaluate the effect of the 12-week exercise program on systemic inflammation, serum IL-6 and TNF-α were compared within groups (baseline vs. week 12) and between groups at week 12. In the exercise group, IL-6 decreased after the intervention from 54.73 ± 11.26 to 45.21 ± 10.66 pg/mL (Δ − 9.52; 95% CI: −11.61 to −7.44; p < 0.001; Fig. 4A). No change was observed in the control group after intervention (53.60 ± 10.91 to 53.73 ± 10.99 pg/mL; p = 0.543; Fig. 4B). The adjusted between-group difference in IL-6 at week 12 was −8.52 pg/mL (95% CI: −12.34 to −4.70; p < 0.001; Fig. 4C). TNF-α also decreased in the exercise group after the intervention from 44.76 ± 8.73 to 38.09 ± 8.64 pg/mL (Δ − 6.67; 95% CI: −7.88 to −5.47; p < 0.001; Fig. 4D). It remained unchanged in the control group (45.24 ± 8.63 to 45.45 ± 8.07 pg/mL; p = 0.668; Fig. 4E). The adjusted between-group difference in TNF-α at week 12 was −7.36 pg/mL (95% CI: −10.21 to −4.51; p < 0.001; Fig. 4F). Overall, the exercise intervention reduced circulating IL-6 and TNF-α compared with usual care.
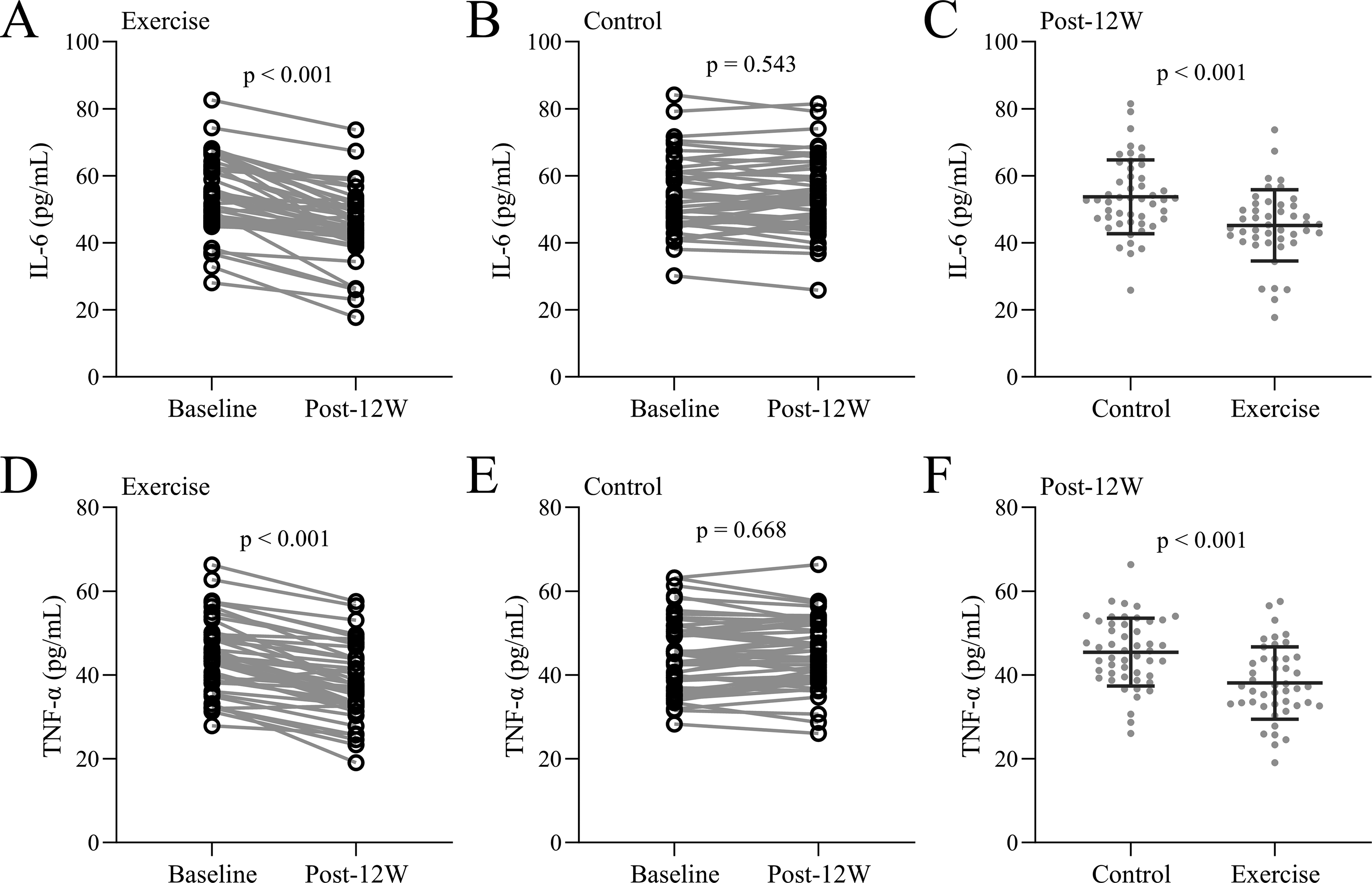
Comparison of serum inflammatory factors. Serum tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) levels were detected by ELISA at the time of baseline and week 12. The comparisons between the time of baseline and week 12 in the exercise group
Discussion
This randomized controlled trial showed that a 12-week exercise program improved multiple outcomes in older adults with sarcopenia. Compared with usual care, exercise improved ADL, increased appendicular muscle mass and strength, and enhanced physical function. Serum inflammatory markers also decreased with exercise, whereas no significant changes were observed in the control group. Together, these results extend previous evidence by showing improved functional independence, as reflected by the MBI.
Our results align with the established role of exercise as a core nonpharmacological strategy for sarcopenia management.9–11,22 Previous systematic reviews and network meta-analyses have consistently shown that resistance training and multicomponent exercise improved muscle strength and physical performance in older adults with sarcopenia,10–12 and similar benefits have been reported across different clinical contexts. 17 Accordingly, the improvements in handgrip strength, ASMI, 6MWT, and TUGT in the exercise group are consistent with evidence supporting combined aerobic–resistance training.14,20
This study addresses an important gap. Most previous work has focused on muscle mass and strength, while everyday independence has been assessed less often. 27 These findings suggest that exercise can improve daily self-care, a key patient-centered goal in geriatric care, as the MBI was the primary outcome, and a clear between-group difference was observed at 12 weeks.
Chronic low-grade inflammation, which plays a key role in the pathophysiology of sarcopenia, is well established. Patients with sarcopenia exhibited significantly elevated circulating proinflammatory cytokines, such as TNF-α and IL-6, which correlate positively with disease severity, whereas the anti-inflammatory cytokine IL-10 showed an inverse association. 28 These inflammatory mediators can directly impair muscle structure and function by promoting muscle protein catabolism and inhibiting regenerative processes.29,30
Exercise interventions, particularly multicomponent training, can effectively downregulate chronic low-grade inflammation. In the present study, serum IL-6 and TNF-α levels decreased after the 12-week intervention, whereas no significant changes were observed in the control group. These changes are more likely to reflect an improvement in chronic inflammatory status than an acute exercise response, because blood samples were collected in the fasting state in the early morning after 12 weeks of intervention and at least 48 hours after the last exercise session. Exercise-induced increases in circulating IL-6 are usually transient, whereas the anti-inflammatory effects of regular exercise accumulate over time. Previous randomized controlled trials have shown that combined resistance and aerobic training can reduce TNF-α and IL-6 levels in older adults, 23 while improving mitochondrial function and attenuating systemic inflammatory responses. 31 This reduction in inflammatory signaling may support muscle remodeling, partly through attenuation of inflammatory pathways such as NF-κB.32,33 In our study, the decreases in IL-6 and TNF-α occurred in parallel with improvements in muscle mass, muscle strength, and physical function, further supporting the concept that reduced chronic inflammation may be one mechanism through which regular exercise improves sarcopenia.
Multicomponent exercise may improve neuromuscular performance through complementary actions. Resistance training supports hypertrophy, whereas aerobic training improves metabolism and tissue perfusion.2,20 In previous studies, gains in handgrip strength and physical performance (6MWT and TUGT) have occurred alongside reductions in inflammatory biomarkers, 34 and cytokine changes have been linked to functional measures such as gait speed and muscle mass index.6,35 Although causality cannot be established in this study, the parallel improvements in inflammation, muscle, and function are biologically plausible and align with mechanistic evidence. 36
These findings have practical implications for routine sarcopenia care. The program was feasible and time-efficient (37 minutes/session, 3 days/week) and combined resistance and aerobic exercise, consistent with current recommendations. 22 Improvement in MBI further suggests that exercise can enhance functional independence, an outcome that is directly relevant to older adults and health systems. Importantly, the intervention was feasible. Adherence in the exercise group was high. Participants completed a mean of 32.4 ± 3.1 of the 36 prescribed sessions, corresponding to an overall adherence rate of 90.0%. In addition, 92.3% of participants achieved the prescribed exercise dose in at least 80% of sessions. The hospital–home model may have contributed to these findings. This model combined initial in-hospital supervision with app-based monitoring, daily record review, weekly telephone follow-up, and biweekly on-site reassessment. 21 Safety was also acceptable. Only three mild cases of postexercise muscle soreness were reported, and all resolved within 24–48 hours. No serious adverse events occurred. Overall, these findings suggest that structured exercise prescriptions may be a feasible and safe approach in health examination and geriatric assessment settings. However, larger studies are still needed to confirm broader scalability.
However, this study has several limitations. First, this was a single-center study with a modest sample size, which may limit generalizability. Second, follow-up was only 12 weeks, so longer-term effects and adherence remain uncertain. Third, analyses were restricted to participants who completed follow-up, and unequal dropout between groups may have introduced bias. Fourth, blinding of participants and intervention staff was not feasible due to the nature of the exercise intervention. Although exercise intensity was monitored using heart rate data and Borg scores, adherence to home-based exercise was still partly dependent on self-report and app-based check-ins. Fifth, diet and nutritional supplement use were not strictly controlled and may have introduced confounding. Because nutritional status strongly influences sarcopenia progression, inadequate protein intake may have impaired muscle protein synthesis and affected muscle-related outcomes. In addition, because multiple secondary outcomes were analyzed without adjustment for multiple comparisons, findings for secondary endpoints should be considered exploratory and require confirmation in future studies.
Given the single-center design, modest sample size, short follow-up, and completer-only analysis, larger multicenter randomized controlled trials with longer follow-up are needed to improve generalizability and evaluate the durability of the observed benefits. Future studies should also adopt an intention-to-treat approach, better control diet and nutritional supplement use, and maintain objective monitoring of training dose. Broader biomarker assessment may further clarify the association between inflammatory changes and functional recovery.
Conclusion
This single-center randomized controlled study showed that a 12-week postprandial multicomponent exercise intervention improved ADL, muscle mass, muscle strength, and physical function, and reduced serum IL-6 and TNF-α levels in older adults aged 60–75 years with sarcopenia compared with usual care. However, the generalizability of these findings remains limited due to the single-center study, with a modest sample size, short follow-up, and completer-only analysis. Larger multicenter randomized controlled trials with longer follow-up, intention-to-treat analysis, and better control of dietary confounding are needed to further validate these findings.
Ethical Approval
The study was approved by the Longgang Central Hospital of Shenzhen. The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent
All patients signed the informed consent.
Data Availability Statement
Data are available upon reasonable request.
Authors’ Contributions
J.Z., H.L., Z.Z., S.W., T.M., and Y.M. conducted the experiments, analyzed the data, and wrote the article. T.M. and Y.M. conceived and supervised the study.
Footnotes
Author Disclosure Statement
The authors declare they have no conflict of interest regarding this research study.
Funding Information
The study was supported by the