
Abstract
Diminished ovarian reserve (DOR), affecting more than 10% of reproductive-aged women, leads to impaired fertility and systemic health disturbances. Baozhu Granule, a novel Chinese herbal formulation, has shown potential ovarian-protective effects in preliminary studies. This exploratory clinical trial aimed to investigate the efficacy and safety of Baozhu Granule in patients diagnosed with DOR. In this prospective, single-arm, open-label trial, 134 women aged 18–45 years with confirmed DOR were enrolled. Participants received Baozhu Granule (20 g, twice daily) orally for 12 consecutive weeks. The primary outcome was the recovery rate of ovarian reserve, assessed by antral follicle count and serum biomarkers. Secondary outcomes included menstrual recovery and changes in the Kupperman menopausal index (KMI). Evaluations were performed at baseline and after 12 weeks of treatment. Of the 134 enrolled patients, 108 completed the full treatment course; 20 of these were unable to attend the final visit (Visit 3) due to COVID-19 restrictions. Among the 88 patients evaluable at Visit 3, 68.2% showed recovery of ovarian reserve. Menstrual recovery was reported in 45.9% of patients, and 42.9% showed alleviation of menopausal symptoms (reduction in KMI). Subgroup analyses indicated that younger age, detectable anti-Müllerian hormone levels, and lower baseline follicle-stimulating hormone levels were associated with higher rates of ovarian reserve and menstrual recovery. Specifically, the overall recovery rate was 85.2% at 12 weeks of observation. No serious adverse events were reported throughout the study period. In this exploratory study, Baozhu Granule was associated with improvements in ovarian reserve, restoration of menstrual cyclicity, and relief of menopausal symptoms in women with DOR, with a favorable safety profile. These preliminary findings suggest its potential as a therapeutic option for DOR; however, further randomized controlled trials are needed to confirm these results.
Introduction
Diminished ovarian reserve (DOR), characterized by a decline in both the quantity and quality of oocytes along with abnormal ovarian reserve test results, represents a critical clinical condition associated with subfertility and menstrual disturbances. 1 With a reported prevalence ranging from 10% to 35% in the general population,2,3 DOR not only serves as a key indicator of ovarian aging but also poses significant reproductive and long-term health risks, including infertility, premature ovarian insufficiency, and an elevated susceptibility to age-related comorbidities such as cardiovascular disease and osteoporosis. 4 Given these implications, the development of safe and effective therapeutic strategies to preserve ovarian function and mitigate associated health burdens is of paramount importance.
Current management of DOR remains largely centered on addressing fertility concerns, with limited options available for fundamentally improving ovarian reserve. Although hormone therapy (HT) may alleviate menopausal symptoms, its application is constrained by potential adverse effects, including increased risks of venous thromboembolism and breast cancer. 5 Thus, there is a compelling need for alternative interventions that are both effective and safe.
Traditional Chinese medicine (TCM) has gained recognition over recent decades for its efficacy in managing menstrual disorders and menopausal symptoms, with a favorable safety profile contributing to its widespread use, particularly among Asian populations. 6 Several TCM formulations have shown promise in enhancing ovarian function; however, existing studies are often limited by methodological shortcomings, such as small sample sizes, insufficient efficacy evaluation, and a narrow focus on assisted reproductive outcomes.7–9 These limitations underscore the necessity for rigorously developed and systematically evaluated TCM-based interventions specifically targeting DOR.
In response to this need, our research team has dedicated years to elucidating the etiology and mechanisms underlying ovarian aging. Leveraging modern bioinformatics tools, including the TCM Inheritance Support System, the TCM Systems Pharmacology Database, and GeneCards, we integrated network pharmacology and big data analyses to identify herbal candidates with potential ovarian-protective effects. Building on classical formulas such as Siwu Decoction and Dingjing Decoction, and through iterative consultations with senior TCM gynecologists and pharmacologists, we developed a novel herbal compound named Tongji Anti-Ovarian Aging 101 (TJAOA101), processed into Baozhu Granule. 10 Preclinical studies in Drosophila melanogaster and mice have demonstrated both the safety and efficacy of Baozhu Granule in preserving ovarian function, as evidenced by increased egg production and hatchability in flies, and improved ovarian reserve biomarkers in aged mice, without detectable adverse effects (unpublished). Nonetheless, clinical validation in human subjects remains essential.
In this study, we conducted a single-center, prospective, single-arm clinical trial to evaluate the safety and efficacy of Baozhu Granule in women with DOR. The findings from this study are expected to provide preliminary evidence supporting its clinical application and to offer a potential strategy for decelerating ovarian aging.
Methods
Trial overview
This is a single-center, prospective, and single-arm trial carried out in Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. The study was approved by the Medical Ethics Committee of Tongji Hospital (TJ-IRB20220634) and registered with ClinicalTrials.gov (NCT05459493). All participants were informed of the study details and signed a written informed consent prior to enrollment. The protocol for this study had been published previously. 10 The single-arm, open-label design was chosen for this exploratory study because the diagnosis of DOR follows an “OR” rule, making balanced group allocation challenging; moreover, patient enrollment resources were limited, and our primary focus was on within-subject changes before and after treatment.
Inclusion criteria
The inclusion criteria included: (1) women aged 18–45 years, (2) diagnosed with DOR, and (3) willing to participate in this trial and sign a written informed consent. The diagnostic criteria for DOR were determined as follows: anti-Müllerian hormone (AMH) < 1.1 ng/mL; or bilateral antral follicle count (AFC) < 6; or basal follicle-stimulating hormone (FSH) > 10 IU/L (the interval between two consecutive tests should be more than 4 weeks, and the values of both tests should reach this level).11,12
Exclusion criteria
The exclusion criteria were as follows: (1) allergies or intolerances to the studied prescription; (2) pregnancy or lactation; (3) cessation of menstruation for a duration exceeding 1 year; (4) abnormal uterine bleeding not due to ovulatory disorders; (5) history of hormone use within 3 months preceding enrollment; (6) endometriosis, adenomyosis, submucosal uterine fibroids, or nonsubmucosal uterine fibroids with a diameter greater than 4 cm; (7) pelvic mass of unknown nature; (8) polycystic ovary syndrome, hyperprolactinemia, hyperandrogenemia, thyroid or adrenal dysfunction, diabetes, or any other endocrine disorders affecting ovulation; (9) severe primary diseases of vital organs or systems (such as moderate anemia), malignant neoplasms, or psychiatric diseases; (10) history of participation in other clinical trials within 1 month preceding enrollment; (11) and unsuitable for this study as assessed by the investigators.
Subject population
A total of 139 eligible participants were enrolled from Tongji Hospital between October 2022 and May 2024.
Treatment
DOR patients were orally treated with Baozhu Granule at a dosage of 20 g twice daily for 12 weeks. Baozhu Granule contains 10 kinds of Chinese herbs: Gynostemma pentaphylla, Radix Rehmanniae, Angelica sinensis, Radix paeoniae alba, Salvia miltiorrhiza, Astragalus membranaceus, Lycium fructus, Poria cocos, Ligustrum lucidum ait, and Radix bupleuri. The development process of Baozhu Granule has been delineated in the previously published protocol. 10 Baozhu Granule preparations were made by the Department of Pharmacy of Tongji Hospital in accordance with the standards of Good Manufacturing Practice. The treatment was temporarily suspended during menstruation. This safety-driven pause was implemented because Baozhu Granule contains blood-activating herbs (e.g., Salvia miltiorrhiza and Angelica sinensis); continuous administration during menstruation might theoretically increase uterine blood flow and potentially worsen menstrual bleeding. To minimize adherence issues, we provided all patients with written/oral instructions and distributed diaries to record menstrual periods and daily medication intake.
The use of hormonal medications or other TCM medicines was prohibited during the study. Concomitant treatments were monitored via patient self-reporting and verified by study staff at each visit. In addition, patients received general dietary recommendations based on TCM theory to avoid potential interference with the herbal effect. These included avoiding smoking, alcohol, tea, spicy or greasy food, and moderating the intake of white radish, mung bean, and other cold foods.
Visits during treatment and follow-up periods
Participants enrolled in the study were required to complete a total of five visits throughout the treatment and follow-up periods. These visits were scheduled at 4 weeks (Visit 1), 8 weeks (Visit 2), and 12 weeks (Visit 3) of treatment, followed by 4 weeks (Visit 4) and 12 weeks (Visit 5) after treatment discontinuation. For participants with regular menstrual cycles, each visit should be scheduled between the 2nd and 5th day of menstruation. The assessments conducted during the visits encompassed measurement of AMH, AFC, and sex hormone levels, evaluation of menstrual status and Kupperman menopausal index (KMI), documentation of adverse events (AEs), and tests of liver and kidney function.
Outcome measures
The primary outcome is the recovery rate of ovarian reserve. According to the diagnostic criteria for DOR, recovery of ovarian reserve is defined as meeting any of the following posttreatment criteria, provided the corresponding baseline value was abnormal: (1) AMH ≥ 1.1 ng/mL, (2) AFC ≥ 6, (3) FSH ≤ 10 IU/L, or (4) a ≥ 50% increase in either AMH or AFC from baseline.
Secondary outcomes include the menstrual recovery rate and KMI. For patients presenting with oligomenorrhea or amenorrhea at enrollment, menstrual recovery is defined as the occurrence of at least two consecutive normal menstrual cycles from the initiation of Baozhu Granule treatment to the end of follow-up. 13 Furthermore, some patients with DOR may exhibit menopausal symptoms. Their severity is assessed using the KMI score, categorized as follows: normal (0–6), mild (7–15), moderate (16–30), and severe (>30). 14 The overall recovery rate is defined as meeting any of the criteria for recovery of ovarian reserve, menstrual recovery, or at least a one-grade improvement in menopausal symptoms on the KMI.
Safety assessments
Safety parameters, encompassing liver function tests (alanine aminotransferase [ALT] and aspartate aminotransferase [AST]) and renal function tests (blood urea and creatinine), were systematically monitored during treatment periods. AEs were assessed and recorded at each clinical visit, with appropriate interventions implemented to safeguard participants’ well-being. The AEs were categorized in accordance with the Common Terminology Criteria for Adverse Events (CTCAE) v5.0, and their relevance to trial medications was thoroughly analyzed. A serum β-human chorionic gonadotropin test was performed at screening to exclude pregnancy. During the trial, all participants were instructed to use condoms for contraception.
Sample size calculation
At present, the natural recovery rate of DOR remains unreported in the literature. According to preliminary findings from our earlier small-sample clinical study (TJIRB20210927), treatment with Baozhu Granule was associated with a recovery of ovarian reserve in ∼71.4% of DOR patients. We hypothesize that Baozhu Granule can increase the recovery rate by at least 15% compared with the natural course of DOR. Based on this assumption, a sample size calculation was performed using a one-sample proportion test with a power of 90% and a two-sided significance level of α = 0.05. Allowing for a dropout rate of 20%, a total of 134 participants will be required for this clinical trial. Since the exact natural recovery rate of DOR is unavailable, the originally planned one-sample proportion test was not performed; instead, an indirect comparison with an external historical control was conducted as an exploratory analysis (see the Statistical Analysis section).
Statistical analysis
Statistical analyses were conducted using SPSS software. Categorical variables were presented in frequencies, percentages, and 95% confidence intervals (CI), while numerical variables were described using means, standard deviations (SD), medians, and interquartile ranges (IQR). Values below the limit of detection (LOD) were imputed as LOD/2 prior to analysis. Missing data were not imputed.
The primary analysis set is the full analysis set (FAS), defined as all participants who received at least one dose of Baozhu Granule and had at least one postbaseline assessment. All efficacy analyses were conducted on the FAS using an available-case approach, that is, for each visit, the denominator was the number of participants who actually completed that visit and had the required measurements.
The primary efficacy analysis was performed by calculating the recovery rate of ovarian reserve in the Baozhu Granule group, with a two-sided 95% CI based on the Clopper–Pearson (exact) method. As a secondary analysis, we compared the observed recovery rate with an external historical control derived from a published study, in which the placebo group (n = 26) achieved a recovery rate of 26.9%. 15 The risk difference (absolute difference in recovery rates) and its 95% CI were calculated using the normal approximation method, incorporating the sampling errors of both groups. No causal inference was drawn from this indirect comparison. Stratified analyses were performed utilizing chi-square tests or Fisher’s exact tests. Statistical significance was set at p < 0.05 using two-sided tests.
Results
Baseline characteristics of the study population
The baseline characteristics of the study population are summarized in Table 1. Briefly, 139 female patients with a confirmed DOR diagnosis were initially enrolled (Fig. 1). Of these, 134 proceeded to the treatment phase and had at least one postbaseline assessment, constituting the FAS with a mean age of 37.59 years at enrollment. Within this cohort, 79 patients (59.0%) fulfilled all three DOR diagnostic criteria. Menstrual disturbances were observed in 75 patients (56.0%), with the majority presenting as oligomenorrhea or amenorrhea. Based on KMI scores, 64 patients (47.8%) reported mild-to-moderate menopausal symptoms.
Baseline Data of the Participants Treated with Baozhu Granule

AFC, antral follicle count; AMH, anti-Müllerian hormone; FAS, full analysis set; FSH, follicle-stimulating hormone; IQR, interquartile range; KMI, Kupperman menopausal index; SD, standard deviation.
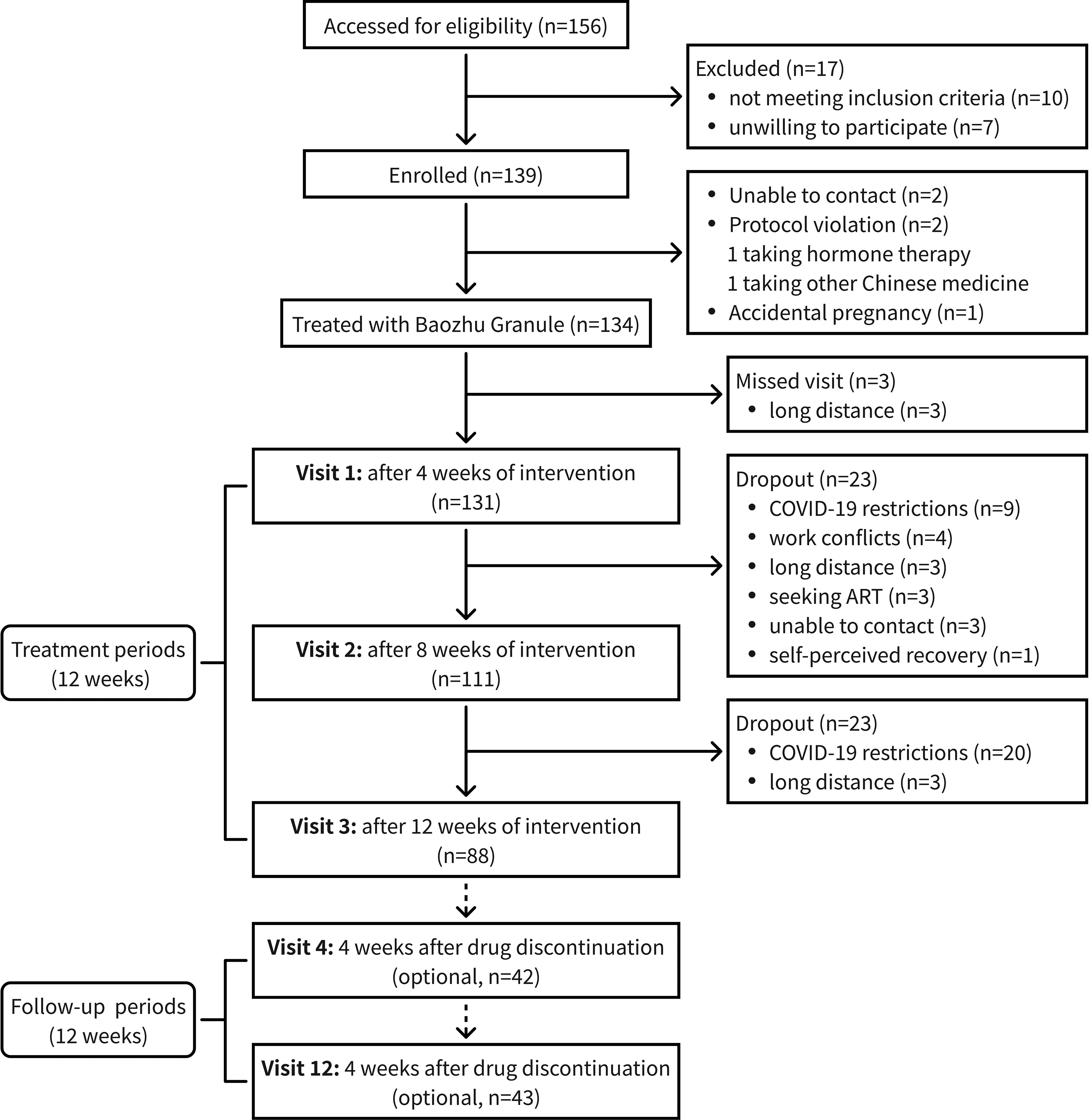
Study flowchart. ART, assisted reproductive technology.
Recovery rate of ovarian reserve based on diagnostic indices
Following the efficacy evaluation criteria outlined in the protocol, we determined the recovery rate of ovarian reserve and the improvement rates of individual or combined indices relative to baseline at each visit, as presented in Table 2. Visit 3 is a critical evaluation point for patients receiving a full course of Baozhu Granule. Of the 88 patients who completed Visit 3, 60 achieved improvements in at least one of the following indices: AMH, AFC, or FSH, resulting in a recovery rate of 68.2% (95% CI: 57.4%−77.7%). In a published study, the placebo group (n = 26) showed a recovery rate of 26.9% (7/26). 15 The risk difference between our Baozhu Granule group and the external control was 41.3% (95% CI: 21.7%−60.9%). The lower bound of this CI exceeds the prespecified clinically meaningful benefit of 15%. However, this indirect comparison is exploratory and does not imply a causal effect of Baozhu Granule.
Recovery Rate of Ovarian Reserve and Improvement of Specific Indices at Each Visit
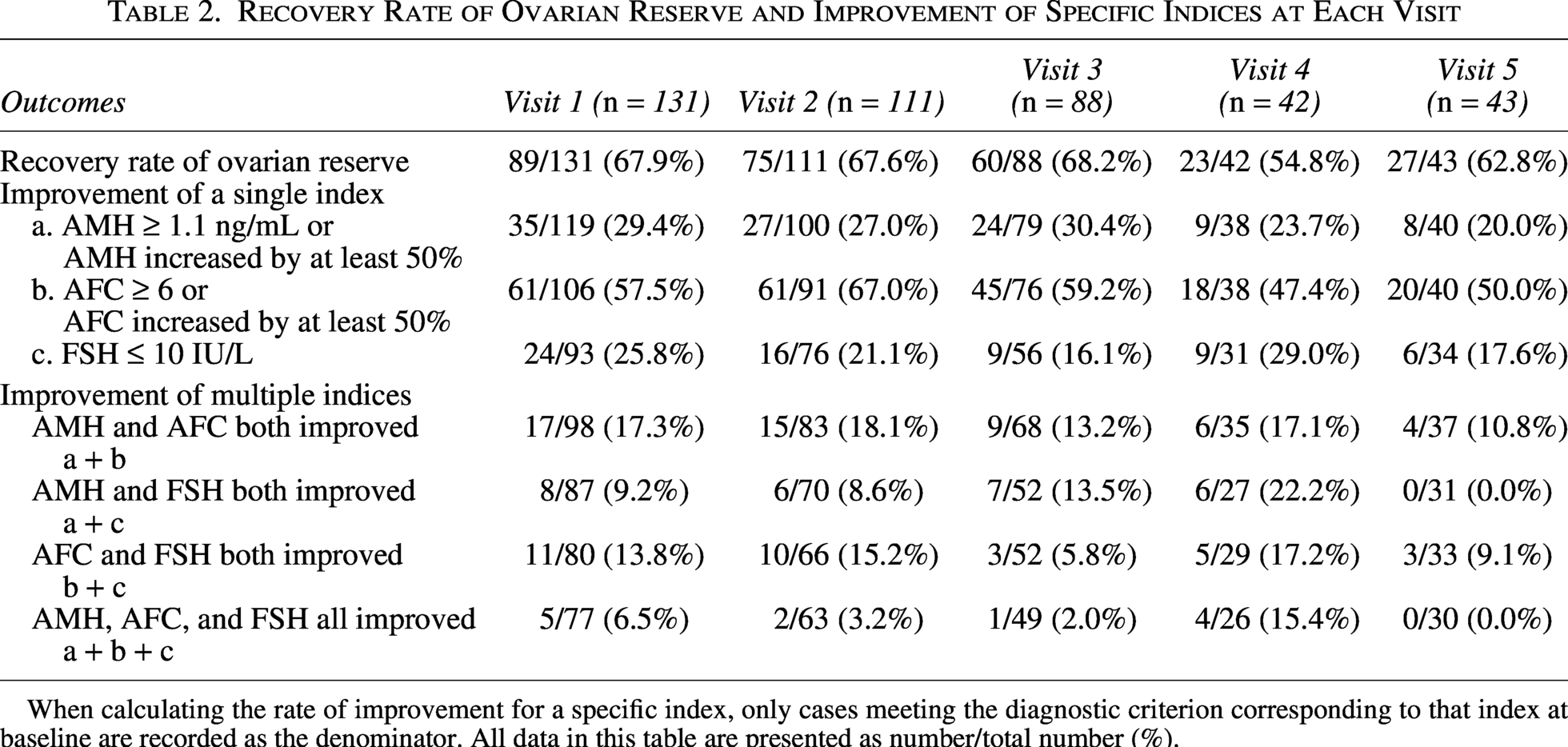
When calculating the rate of improvement for a specific index, only cases meeting the diagnostic criterion corresponding to that index at baseline are recorded as the denominator. All data in this table are presented as number/total number (%).
During the follow-up period, although the recovery rate of ovarian reserve showed a declining trend, it consistently remained above 54%. The summary statistics for AMH, AFC, and FSH at each visit are presented in Supplementary Table S1. AFC was significantly higher at Visits 1, 2, and 3 compared with baseline. Collectively, the findings suggest that a majority of DOR patients achieved clinical improvements following 12-week Baozhu Granule intervention.
Menstrual recovery and improvement of menopausal symptoms
Among the 74 patients with oligomenorrhea or amenorrhea at enrollment, 34 (45.9%) patients experienced menstrual recovery prior to Visit 3 (Table 3). A small number of patients achieved menstrual recovery during the follow-up period, culminating in a cumulative recovery rate of 48.6% by Visit 5.
Menstrual Recovery and Improvement of Menopausal Symptoms at Each Visit
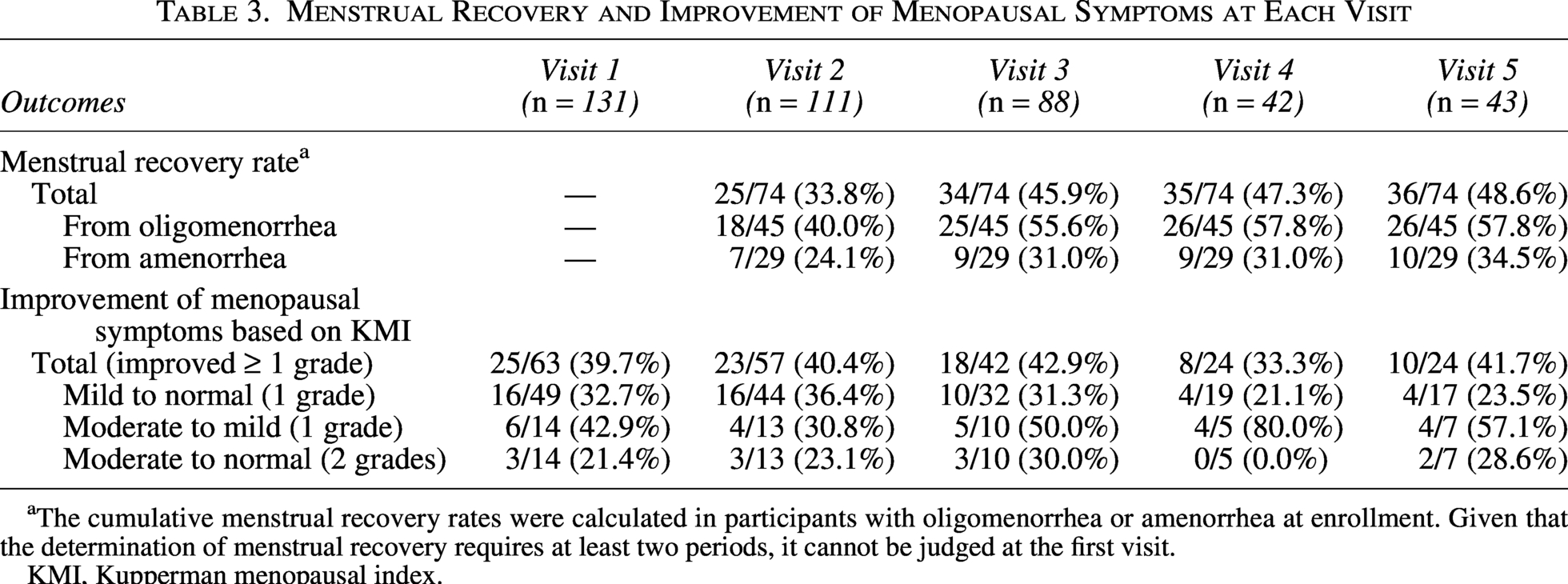
The cumulative menstrual recovery rates were calculated in participants with oligomenorrhea or amenorrhea at enrollment. Given that the determination of menstrual recovery requires at least two periods, it cannot be judged at the first visit.
KMI, Kupperman menopausal index.
For patients whose menopausal symptoms were initially categorized as mild or more severe by KMI score, changes in symptom severity are summarized in Table 3. At Visit 3, 42.9% of these patients showed a reduction of at least one KMI grade compared with baseline. Notably, of the 10 cases initially classified as moderate, 5 were reclassified as mild and 3 as normal. In addition, the distribution of KMI grades for the entire study population at each visit is presented in Supplementary Figure S1.
Upon the integration of ovarian reserve indices, menstrual status, and menopausal symptoms, the overall recovery rate exceeded 70% at each visit (Table 4). Specifically, the overall recovery rate was 85.2% following 12 weeks of medication.
Overall Recovery Rate at Each Visit

All data in this table are presented as number/total number (%).
Stratified efficacy analyses of Baozhu Granule
Age serves as a pivotal determinant of ovarian reserve, with DOR occurring before age 40 being generally regarded as pathological.11,16 Thus, we conducted an age-stratified analysis with a 40-year cutoff point to ascertain the effect of age on the efficacy of Baozhu Granule in the treatment of DOR. AMH and AFC are the most valuable ovarian reserve tests. 17 Compared with AFC, AMH is less susceptible to the subjective influence of operators. In patients with DOR, serum AMH levels may be undetectable, which is associated with an increased risk of menopause within 5 years in middle-aged women. 18 Consequently, a stratified analysis was performed to investigate whether an undetectable baseline AMH level would affect the efficacy of Baozhu Granule. The lower limit of AMH detection in this study was 0.06 ng/mL.
Current diagnostic criteria for DOR do not stipulate an upper threshold for FSH. Nonetheless, two consecutive FSH measurements exceeding 25 IU/L may support a diagnosis of premature ovarian insufficiency, a condition considered more severe than DOR. 19 Hence, the cutoff value of 25 IU/L was employed for an FSH-stratified analysis to explore potential differences in the efficacy of Baozhu Granule among patients with distinct FSH levels.
As shown in Table 5, DOR patients who were younger than 40 years of age or had FSH levels below 25 IU/L at baseline demonstrated higher recovery rates of ovarian reserve by Visit 3. Among those exhibiting oligomenorrhea or amenorrhea at enrollment, individuals aged <40 years, or with AMH ≥ 0.06 ng/mL, or with FSH < 25 IU/L consistently showed higher cumulative rates of menstrual recovery across all the visits. Regarding menopausal symptoms, stratified analysis revealed no differences. Of note, these subgroup results are exploratory and hypothesis-generating, and all P-values should be interpreted descriptively, not as confirmatory evidence.
Stratified Analysis of Drug Efficacy
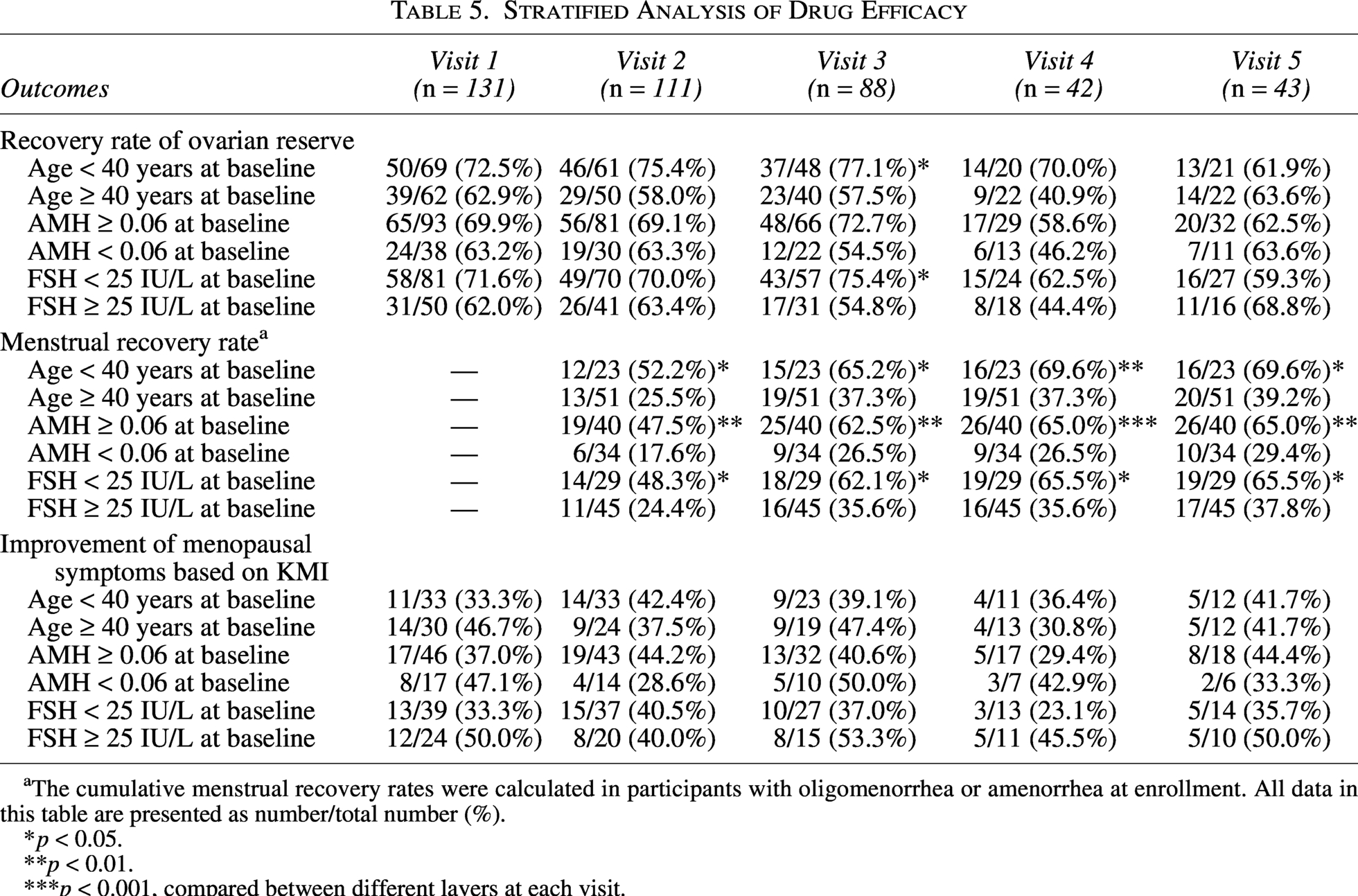
The cumulative menstrual recovery rates were calculated in participants with oligomenorrhea or amenorrhea at enrollment. All data in this table are presented as number/total number (%).
p < 0.05.
p < 0.01.
p < 0.001, compared between different layers at each visit.
Safety monitoring during the trial
AEs observed during the study period are detailed in Table 6. In brief, ALT/AST increases occurred in 5 cases (3.7% of the safety set, n = 134), all mild and transient. Gastrointestinal symptoms included diarrhea (4 cases, 3.0%), dyspepsia (3 cases, 2.2%), and constipation (2 cases, 1.5%). These symptoms resolved after temporary drug discontinuation and did not recur upon rechallenge. According to CTCAE v5.0, all AEs were classified as Grade 1. No participants withdrew from the trial due to AEs.
Safety and AEs During the Study

All data in this table are presented as number (%).
CTCAE, Common Terminology Criteria for Adverse Events; SS, safety set.
Discussion
The escalating global prevalence of DOR, particularly among younger women, underscores a growing clinical and public health concern. 3 A recent Korean study revealed that DOR affects up to 37.2% of women of reproductive age, emphasizing its substantial threat to female fertility and long-term health. 20 Despite ongoing medical advances, current therapeutic options for DOR remain limited, with no treatment demonstrating definitive efficacy in restoring ovarian reserve. This critical gap underscores the urgent need for novel interventions. In response, our team developed Baozhu Granule, an innovative Chinese herbal compound designed to address this unmet clinical need.
The primary outcome of this trial was the recovery rate of ovarian reserve, which was observed as 68.2% after 12 weeks of oral administration of Baozhu Granule. Previous studies evaluating TCM for DOR have largely relied on composite efficacy endpoints that combine objective biomarkers with subjective symptom scores. 21 Variability in how efficacy is defined across trials hinders cross-study comparisons and obstructs the establishment of a standardized evaluation framework in the field. 22 In this study, we introduced the recovery rate of ovarian reserve as a unified primary outcome, defined strictly by the core biochemical and sonographic criteria used for DOR diagnosis: AMH, AFC, and FSH. This approach minimizes information bias and enhances the reliability of efficacy assessment, thereby facilitating future comparative research.
Although DOR diagnosis is based on objective metrics rather than symptomatology, a considerable proportion of participants presented with clinical manifestations at enrollment: 56.0% reported menstrual abnormalities and 47.8% exhibited menopausal symptoms such as hot flushes, night sweating, and insomnia. We therefore explored changes in these parameters. After 12 weeks of treatment, approximately half of the affected participants reported resumed menstruation or alleviation of menopausal symptoms. When integrating improvements in ovarian reserve, menstrual cyclicity, and menopausal symptoms, the overall recovery rate was 85.2%. Stratified analysis revealed that patients under 40 years of age, those with detectable AMH levels at baseline, or those with FSH levels below 25 IU/L were more likely to achieve recovery of ovarian reserve or menstrual function following Baozhu Granule treatment. This suggests that earlier intervention in the course of DOR may be associated with better therapeutic outcomes.
From a TCM perspective, the Kidneys (Shen) are considered fundamental to ovarian function. Shen deficiency is recognized as the core pathogenesis of DOR, often accompanied by liver (Gan) stagnation, Qi deficiency, and blood deficiency. 21 Baozhu Granule is formulated with herbs known to tonify the Kidneys (Bushen), soothe the liver (Shugan), replenish Qi (Yiqi), and nourish blood (Yangxue). 23 Several key components—including Radix Rehmanniae, Angelica sinensis, Salvia miltiorrhiza, and Lycium fructus—have been reported to improve ovarian function through antioxidant, anti-inflammatory, and proangiogenic mechanisms, thereby aligning TCM theory with biomedical evidence.24–27 However, as these mechanisms were not directly tested in the present study, they should be considered hypothetical and warrant further investigation. Importantly, Baozhu Granule did not induce serious AEs in this trial, and its constituents have a longstanding history of safe use, devoid of the risks associated with HT, such as thromboembolism and cancer.
This study was conducted during the latter phase of the COVID-19 pandemic, during which some participants missed scheduled visits due to mobility restrictions, leading to higher rates of dropout and missing data. Nonetheless, among the 20 participants who completed treatment but missed Visit 3, 70% showed positive outcomes, suggesting that the impact on overall efficacy estimation was limited. The single-arm design allowed for within-subject comparisons before and after treatment, but the lack of a control group precludes definitive attribution of the observed effects to Baozhu Granule. Moreover, the provision of general dietary recommendations means that we cannot rule out a potential contribution of dietary modifications, although these recommendations are routine health advice with no recognized direct effect on ovarian reserve. Besides, the intermittent regimen (with a pause during menstruation) may interfere with dose–response interpretation. Thus, the findings of this exploratory study are not extrapolated to a continuous daily dosing regimen. Future multicenter, randomized, placebo-controlled trials with larger sample sizes are warranted to conclusively establish Baozhu Granule’s efficacy and safety.
In summary, this exploratory study observed that Baozhu Granule was associated with improving ovarian reserve, restoring menstrual cyclicity, and relieving menopausal symptoms in women with DOR, with a favorable safety profile. These findings suggest that Baozhu Granule may exert a positive effect on ovarian aging, rather than merely alleviating general menopausal symptoms. It may represent a potential therapeutic option, especially for patients with contraindications to or reservations about HT. This first-in-human study provides preliminary evidence and a rationale for further large-scale, randomized controlled trials to investigate the potential of Baozhu Granule as a treatment for DOR.
Authors’ Contributions
Y.Z.: Conceptualization, methodology, project administration, and funding acquisition. Y.G.: Writing—original draft, data curation, and formal analysis. Aiyue L.: Resources. A.L.: Investigation. M.Z.: Methodology. Y.Y.: Investigation. T.W.: Investigation. J.F.: Resources. W.W.: Resources. W. Xiong: Resources. W. Xie: Investigation. M.W.: Investigation. J.Z.: Conceptualization, project administration, and writing—review and editing. S.W.: Conceptualization, supervision, funding acquisition, and writing—review and editing.
Data Availability
Anonymous data that support the findings of this study are available from the corresponding authors upon reasonable request.
Footnotes
Acknowledgments
The authors thank all the patients and investigators who participated in the clinical trial and appreciate their dedication of time and expertise.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This work was supported by grants from the National Natural Science Foundation of China (82405147 to Y.Z. and 82471678 to S.W.) and the Interdisciplinary Research Program of HUST (2025JCYJ034 to J.Z.).
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.