
Abstract
Despite its 40-year history, computerized diagnostic support is not used in routine clinical practice. As part of a European project to develop computerized diagnostic support for family physicians, we identified user decision requirements and made design recommendations. To this end, we employed multiple data types and sources. All data were elicited from U.K. family physicians and pertained to consultations with patients, either real or simulated. To elicit user requirements, we conducted in situ observations and interviews with eight physicians and performed a hierarchical task analysis of the diagnostic task. We also analyzed 34 think-aloud transcripts of 17 family physicians diagnosing detailed patient scenarios on a computer and 24 interview transcripts of 18 family physicians describing past cases of intuitive diagnoses from their experience. All transcripts were coded using the situation assessment record (SAR) method. We report our methods and results using the decision-centered design framework. Studies employing multiple human factors techniques and data types in order to elicit user requirements are rare. Our approach enabled us to propose interface design recommendations that go beyond existing “differential diagnosis generators,” with the aim to improve physicians’ performance and acceptance of the resulting tool.
Keywords
Introduction
Family physicians in the United Kingdom have a gatekeeping role, controlling access to specialist services. Thus, one of their key challenges is trying to balance the risk of missing a serious disease against unnecessary investigation or referral. Although the prevalence of serious disease is relatively low in primary care, the sheer volume of patient contacts (90% of contacts in the U.K. health care system) means that only very low risks can be tolerated. Data from both major U.K. medical defense organizations show that diagnostic error is the reason for most patient claims against family physicians (63% to 66%; Silk, 2000). It is also the most common reason for malpractice claims in the ambulatory care setting in the United States (59%; Gandhi et al., 2006)
Family physicians see a relatively large number of patients in short 10-min consultations, that is, around 20 patients per clinical session (3.5 hr). They deal with a wide range of disease areas and patients suffering from multiple conditions (Salisbury et al., 2013). They also deal with nonspecific symptoms that could be attributed to a number of causes. These are some of the factors that explain why diagnosis in family medicine can be challenging. In addition, the multiplicity and heterogeneity of tasks that U.K. family physicians are expected to perform during a 10-min consultation, such as screening for certain diseases and health promotion, and the cost considerations in relation to diagnostic tests and specialist referrals can exert more pressure on family physicians and reduce even further the time that they can dedicate to the important task of diagnosis. In the United States, family physicians are under similar pressures, with the average time for consultations declining and the added problem of increasing amounts of paperwork required for administration and billing purposes (Musen, Middleton, & Greenes, 2014).
Diagnostic error results from both factors in the health care system and clinical judgment (cognitive factors). Cognitive factors are thought to be the most prevalent cause of diagnostic error (Graber, Franklin, & Gordon, 2005). In a large retrospective study of diagnostic adverse events in Dutch hospitals, cognitive factors were found to have played a significant part in 96% of the events and system failures in only 25% (Zwaan et al., 2010). A U.S. study of closed malpractice claims (patients alleging missed or delayed diagnosis) in the ambulatory setting estimated that cognitive factors (e.g., judgment errors, vigilance and memory lapses, lack of knowledge) were implicated in virtually all diagnostic errors, either alone (in 55% of errors) or in association with patient- and/or system-related factors (Gandhi et al., 2006). The most frequent breakdowns in the diagnostic process were failure to order appropriate diagnostic tests (55%), failure to follow up appropriately (45%), inadequate history taking and physical examination (42%), and incorrect interpretation of diagnostic tests (37%), mostly imaging. It is apparent that failure to gather sufficient and appropriate information was responsible for most errors. In their seminal program of work, Elstein and colleagues ascertained the importance of diagnostic hypotheses driving both the search for and interpretation of clinical information (Elstein, Shulman, & Sprafka, 1978, 1990).
Family physicians report that they diagnose using mostly automatic or semiautomatic strategies, based on rules or the recognition of patterns, rather than any analytical reasoning (Heneghan et al., 2009). These heuristic strategies serve physicians well in familiar and routine situations because they can help them arrive at the right diagnosis or decision quickly, confidently, and efficiently. Nevertheless, heuristics that are adapted to one environment (Gigerenzer, Todd, & ABC Research Group, 1999) can easily turn to biases (Kahneman, Slovic, & Tversky, 1982), when changes in the environment go unnoticed by the decision maker. For example, in the absence of a back injury, back pain that feels worse when the patient wakes up in the morning is most likely mechanical. However, back pain that wakes up the patient during the night may suggest that it is possibly due to a more serious cause. If physicians have not generated the right hypotheses to account for the presenting symptoms, they may ignore them, explain them away (Kostopoulou, Devereaux-Walsh, & Delaney, 2009), or change their interpretation to fit their current hypothesis (Kostopoulou, Mousoulis, & Delaney, 2009; Kostopoulou, Russo, Keenan, Delaney, & Douiri, 2012; Nurek, Kostopoulou, & Hagmayer, 2014).
Computerized diagnostic support systems (referred to hereafter as diagnostic systems or simply systems) have been developed since the early 1970s (de Dombal, Leaper, Staniland, McCann, & Horrocks, 1972; Leaper, Horrocks, Staniland, & De Dombal, 1972). Studies assessing their effectiveness in improving physician performance have produced mixed results (Garg et al., 2005). Although they may remind physicians of diagnoses that they would otherwise have not considered, this benefit has been demonstrated only in experimental settings (Berner, 2009), and their use in clinical practice is very limited.
There are two major technical problems with existing diagnostic systems that constitute significant barriers to their adoption and effective use: lack of integration with the electronic health record (EHR) and lack of consideration of the physician’s diagnostic workflow (El-Kareh, Hasan, & Schiff, 2013; Kawamoto, Houlihan, Balas, & Lobach, 2005; Shibl, Lawley, & Debuse, 2013). Proper elicitation of user requirements is an essential prerequisite for the design of any application that is intended to support diagnosis within the clinical encounter, yet it has not been carried out previously. Commercial systems (“differential diagnosis generators”), such as DXplain, Isabel, and SimulConsult, are stand-alone applications, requiring physicians to switch from their EHR to the system and enter information twice. This requirement involves the presumption that physicians recognize the need for advice and are sufficiently motivated to spend the time entering information and examining system advice. The evidence for either of these assumptions is discouraging (Friedman et al., 2005; Ramnarayan et al., 2006). Furthermore, even when physicians decide to consult the system, they will do so after they have collected substantial information from the patient. It follows that system advice based on that information may well be biased by the hypotheses that the physician has already considered: “The system’s advice, and thus its potential value, depends on how users can convey to the [diagnostic support system] their personal understanding of a case by selectively entering clinical findings” (Friedman et al., 1999, p. 1852).
In a recent experimental study (Kostopoulou, Rosen et al., 2015), family physicians diagnosed a number of patient scenarios on a computer. The authors examined two types of automated diagnostic support: one whereby a list of diagnostic suggestions is provided early on in the clinical encounter, triggered by the reason for encounter and the patient’s risk factors before physicians start asking questions to test their hypothesis/hypotheses, and one whereby an individualized, shorter list of diagnostic suggestions is provided late in the encounter, based on information that the physician has collected and triggered by the physician entering his or her diagnosis. Both types of support were tested against an unaided control group. The study showed that early support significantly improved diagnostic accuracy over control without lengthening information search and time taken, whereas late support was no more accurate than control. The effect was replicated in Greece, a European country with a very different medical training and healthcare organization systems, demonstrating the generalizability of this generic early intervention to improve diagnostic accuracy (Kostopoulou, Lionis et al., 2015). We adopted the principle of early support in the design of a computerized diagnostic support system for family medicine and carried out a user requirements elicitation process described in this paper.
Elicitation of user requirements is a critical and complex phase in the design and development of information systems. Inappropriate or insufficient elicitation, for example, based on a single method or limited numbers of participants, can lead to failed system functionality and user adoption (Davey & Cope, 2008; Zowghi & Coulin, 2005). We aimed to elicit user requirements for the design of a prototype for computerized diagnostic support for family physicians to be developed as part of the TRANSFoRm project (transformproject.eu).
Method
We employed a decision-centered design (DCD) framework (Crandall, Klein, & Hoffman, 2006; Militello & Klein, 2013), one of several frameworks for cognitive systems engineering. DCD advocates focusing on difficult key decisions and nonroutine situations, wherein errors may lead to injury and/or death. It is therefore suitable for designing support for medical diagnosis. DCD uses cognitive task analysis (CTA) methods to identify the key decisions. It then translates them into cognitive requirements. The system design process focuses on these requirements to support decision making in challenging situations, assuming that the routine requirements will be incorporated along the way. The aim of using DCD is to ensure that the design addresses cognitive challenges so that cognitive performance is improved and the human–computer interface reflects the users’ needs.
The DCD framework includes five phases. Here, we describe the first three phases for the design of the prototype: preparation, knowledge elicitation, and analysis and representation. We are currently engaged in the last two DCD phases, application design and prototype evaluation; hence these are not reported in this paper. Figure 1 shows the first three phases of the DCD framework, with their respective data sources, analyses, and outputs.
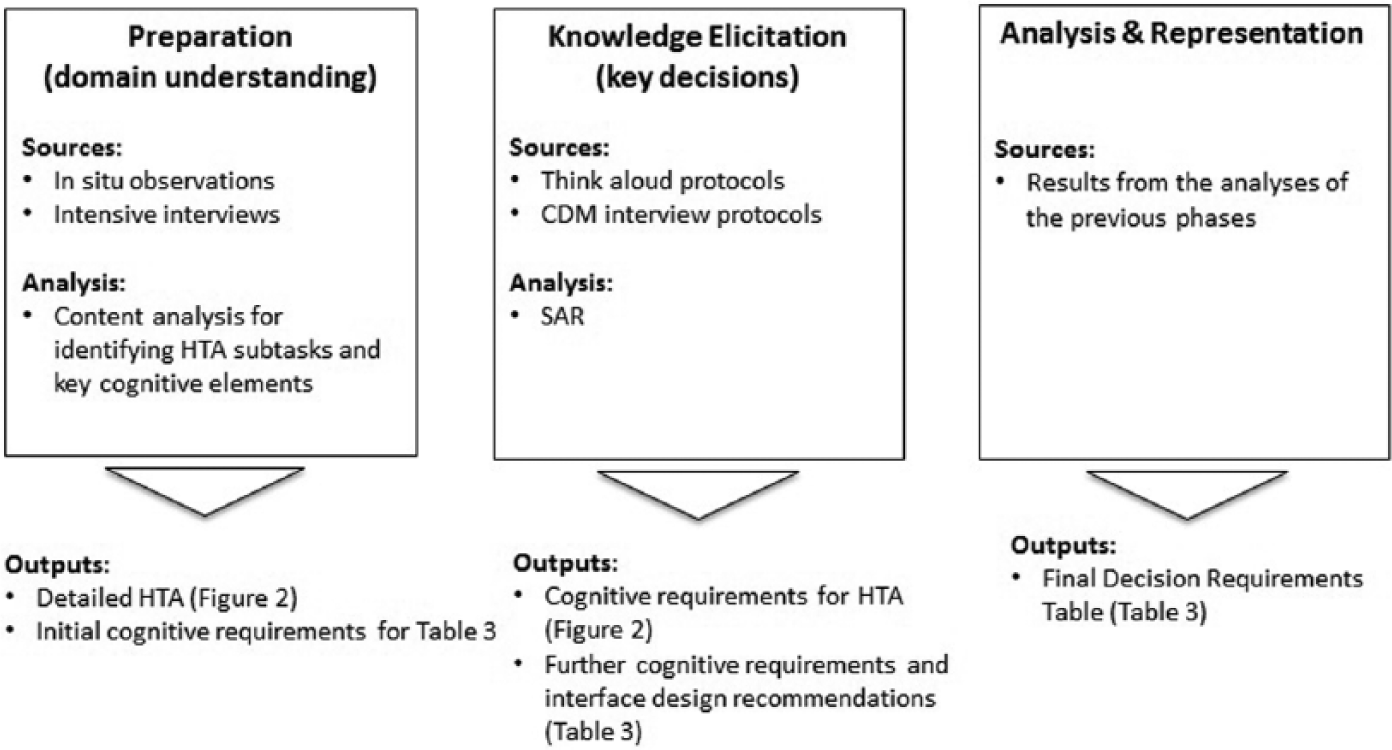
The decision-centered design (DCD) framework: Sources of data, methods of analysis, and outputs of each DCD phase.
Preparation
In the preparation phase, one seeks to gather background material about the domain and the nature and range of the tasks involved, and to identify cognitively complex task elements. Preparation started with reviewing an existing hierarchical task analysis (HTA) of the family practice consultation (Kostopoulou, 2006). HTA models tasks as hierarchies of goals and subgoals, with plans that show how subgoals should be carried out (Annett & Duncan, 1967; Shepherd, 2001). We aimed to refine the parts of the HTA that related to diagnosis. For this purpose, we observed eight family physicians (five male; mean 8.6 years in family medicine, SD = 6) consulting with their patients, which resulted in the observation of 104 clinical encounters (23.5 hr) in total. A researcher (TP) sat in the consulting room and unobtrusively observed the clinical interaction, taking notes of the tasks the physicians performed, their work flow, and how they used their EHR, that is, for which tasks and at which stage in the work flow. Notes from all observations were compared, which helped us to focus on the observable behaviors and interactions with the EHR and refine the existing HTA (Figure 2).
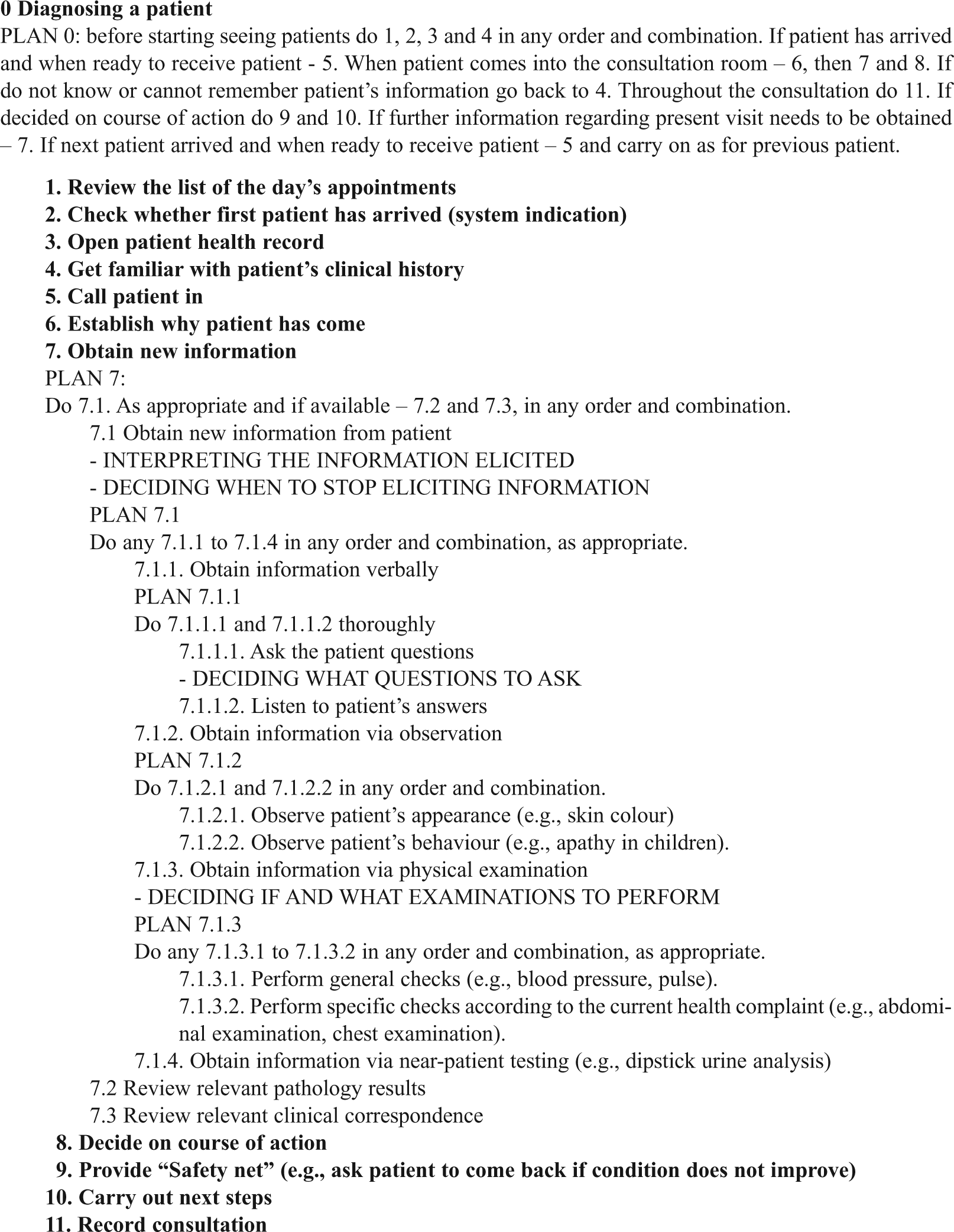
An extract from the hierarchical task analysis of diagnosis. Plan 0: “Diagnosing a patient” with associated plan and goals. For illustration purposes, only Goal 7.1 is redescribed. Cognitive requirements were added (in uppercase).
The notes also guided the postobservation interviews of the eight physicians, which focused on the clinical encounters observed earlier. The aim of these interviews was to confirm the flow and tasks involved in diagnosing a patient, as were observed, and to identify cognitively complex task elements in the diagnostic process. We employed “intensive interviewing” (Legard, Keegan, & Ward, 2003) rather than a structured interview. Intensive interviews are adaptive to the situation of interest and allow the content and order of the questions to vary from one interviewee to another. In addition to specific questions about each clinical encounter observed, we asked physicians to think back to past diagnostic errors and suggest how computerized diagnostic support might have helped to avoid these errors.
Physicians’ answers were documented and examined for important concepts and their relationships. We identified the cognitive aspects and elements (e.g., potential for errors, difficulties, and strategies) of the diagnostic task. For example, in relation to the HTA subtask “get familiar with patient’s clinical history,” the physicians described the difficulty in identifying and retrieving from the patient record information that could potentially be critical for diagnosis—for example, similar previous episodes, comorbidities, and risk factors—and their strategies of doing so, for example, filtering according to high-priority problems. This information was then used in the decision requirements table.
Knowledge Elicitation
The knowledge elicitation phase uses CTA methods to elicit critical incidents and key components of expert decision making. For this purpose, we used CTA methods to analyze two types of existing verbal data: (a) think-aloud protocols of family physicians diagnosing patient cases presented on a computer and (b) interview protocols of family physicians describing past cases of intuitive diagnoses.
The think-aloud protocols were collected during a study by the second author, investigating how family physicians deal with early presentations of cancer (Kostopoulou, Sirota, Round, Samaranayaka, & Delaney, 2015). Participating physicians viewed a series of patient cases on computer. After some initial information about the patient and his or her main health complaint, physicians requested further information in order to diagnose. They could take a history and request results of physical examinations and laboratory tests. A researcher provided responses from a predetermined list. Furthermore, participants were instructed to think out loud (Ericsson & Moxley, 2011). We used the first 34 think-aloud protocols from this study. Eleven pertained to a lung cancer scenario, 11 to a myeloma scenario, and 12 to a colorectal cancer scenario. Lung and colorectal cancers are common cancers, and myeloma is rare.
Using data thus obtained provided considerable control, because it enabled us to study challenging diagnostic situations with predetermined difficulty, presented in a standard way to multiple participants, which enabled comparisons between transcripts and identification of diagnostic strategies. In addition, each scenario contained critical information that could be obtained upon the physician’s request, so we could identify omissions in information search and interpretation errors. The computer program in the original study automatically recorded each physician’s sequential information acquisition, which gave a structure to the verbal reports and provided a validity check. Finally, each scenario had an optimal solution, that is, depicted a specific diagnosis, against which participants’ accuracy was measured.
The think-aloud protocols were elicited in a study wherein all information was provided in written form, the physicians did not have the opportunity to see the patients, and they were instructed to ask targeted rather than general questions (e.g., “Do you have fever?” rather than “What other symptoms do you have?”). Therefore, it was expected that their verbalizations reflected a relatively analytical approach to diagnosis. For this reason, additional data, reflecting a more intuitive diagnostic approach, were analyzed for knowledge elicitation purposes. These data were 24 protocols from a study wherein 18 family physicians were interviewed about patient cases that they believed to have diagnosed by intuition (Woolley & Kostopoulou, 2013). At the interviews, the researchers prompted the physicians systematically, following the critical decision method (CDM). The CDM has been used in numerous domains to investigate the cognitive components of proficient performance (Klein, Calderwood, & Macgregor, 1989). It is a semistructured interview method used to elicit information and knowledge from experienced users in relation to their decision making during nonroutine, critical incidents (Crandall et al., 2006). Using the CDM, the researchers elicited from the physicians the cues, expectancies, and goals associated with each judgment point. During the interviews, they also asked the physicians to identify potential errors at each decision point and how and why errors might occur.
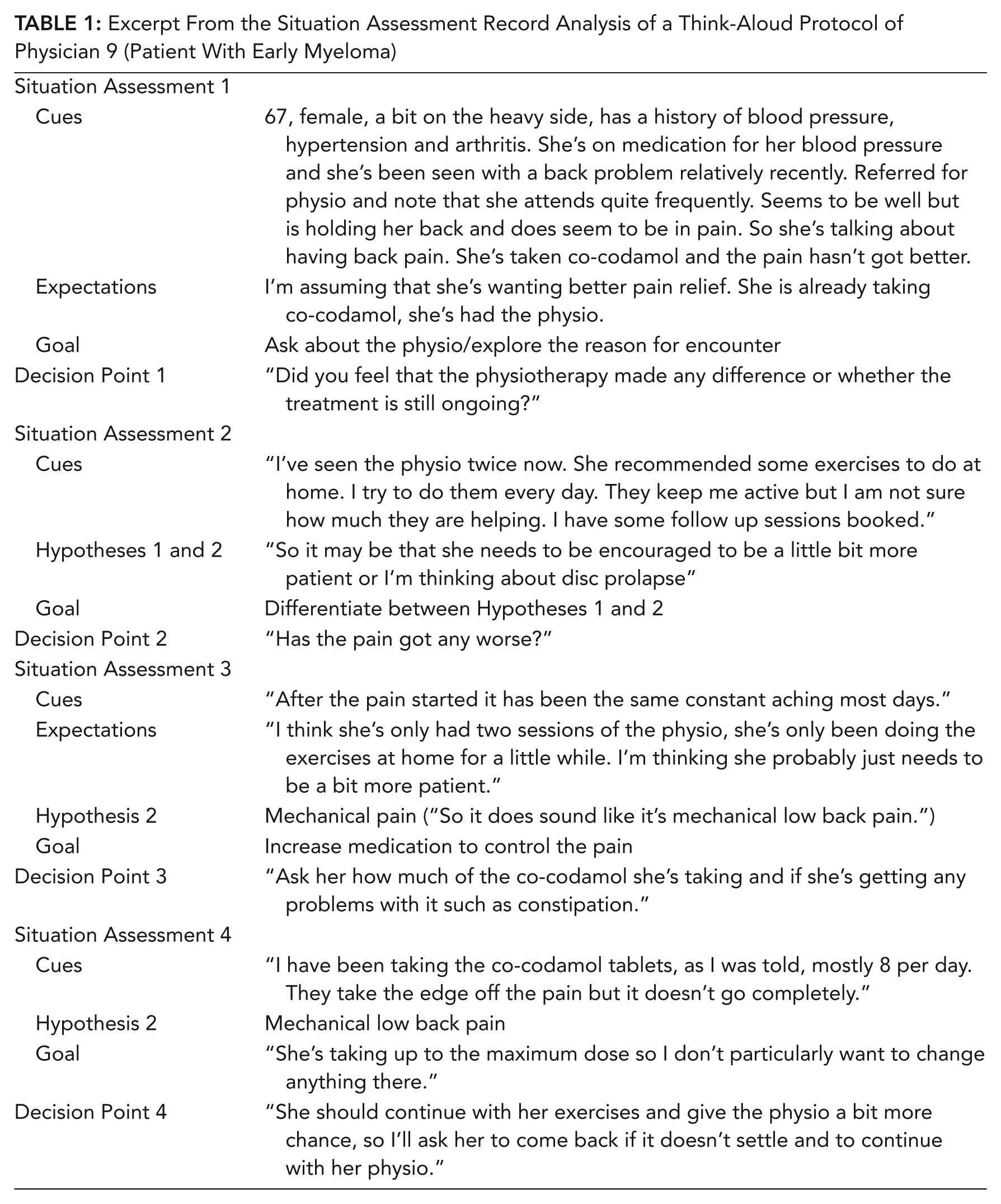
We used the situation assessment record (SAR) method to analyze both the think-aloud and interview protocols to enable comparisons between them (Hoffman, Crandall, & Shadbolt, 1998). In SAR, the timeline for an event specifies the points at which the expert engaged in situation assessment and decision making. For each patient case, we constructed a chronological chart that showed how situation awareness evolved during the event: the types of knowledge, cues, interpretations, and inferences that led to the situation awareness and how situation awareness led to the course of action. Two examples of such a chart are presented in Table 1 and Table 2. Table 1 depicts an excerpt from the SAR analysis of a think-aloud protocol; the scenario features the first consultation of a patient with early myeloma. Table 2 depicts an excerpt from the SAR analysis of a CDM interview; the scenario features a patient with ovarian cancer.
Excerpt From the Situation Assessment Record Analysis of a Think-Aloud Protocol of Physician 9 (Patient With Early Myeloma)
Excerpt From the Situation Assessment Record Analysis of a Critical Decision Method Protocol of Physician 8 (Patient With Ovarian Cancer)
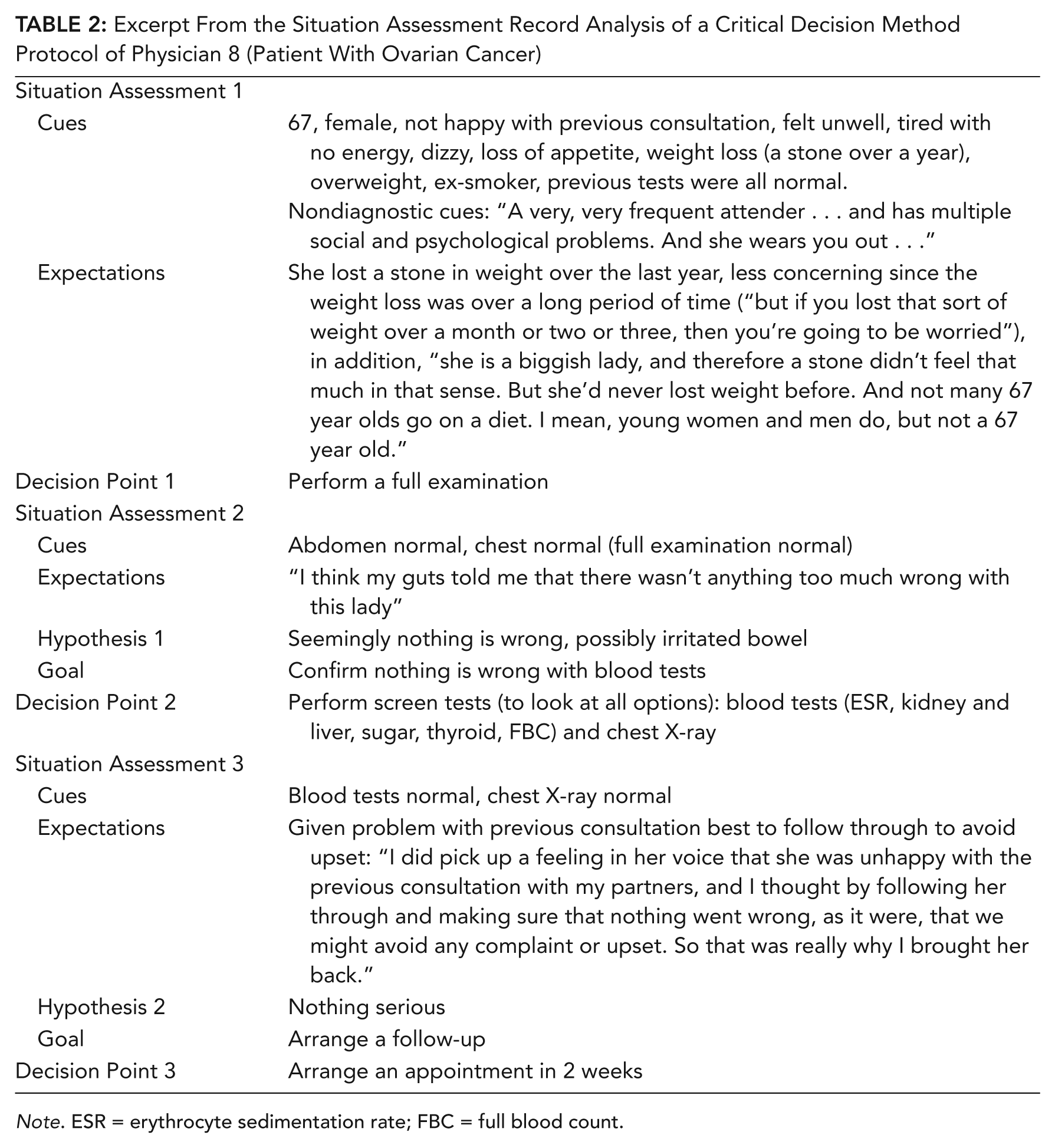
Note. ESR = erythrocyte sedimentation rate; FBC = full blood count.
Analysis and Representation
Analysis and representation uses the results from the analyses of the previous phases and sets them out in a decision requirements table (Table 3), as suggested by the DCD framework.
Decision Requirements Table

Note. EHR = electronic health record.
Findings
On the basis of the observations and follow-up interviews with eight family physicians, we refined and expanded the diagnostic component of the HTA (Figure 1). Based on the HTA, intensive interviews, and analyses of the 34 think-aloud and 24 CDM protocols, we elicited four main cognitive requirements, which we encountered in both types of verbal protocols: (a) retrieving information from the patient record, (b) generating diagnostic hypotheses, (c) testing diagnostic hypotheses, and (d) deciding on a patient management plan (Table 3). In most of the protocols, the initial situation assessment depended on retrieving information from the patient record and integrating it with the patient’s current health complaint (e.g., Table 1, Situation Assessment 1). Throughout the diagnostic process, situation assessment depended on the generation and testing of diagnostic hypotheses (e.g., Table 1, Situation Assessments 2 and 3; Table 2, Situation Assessment 2). Physicians generate and test their hypotheses by asking the patient questions, performing examinations, and ordering investigations while constantly integrating and interpreting the information thus elicited. Each one of the aforementioned tasks is also a cognitive requirement: Physicians need to decide what information to elicit and when to stop eliciting more information and decide on a course of action, that is, a management plan. Deciding on a management plan usually occurs toward the end of the diagnostic process (see Table 1, Situation Assessments 3 and 4; Table 2, Situation Assessment 3).
For each of the main four cognitive requirements, we reviewed all the diagnostic events to identify how the decision makers used cues, made inferences, and employed strategies to fulfill the requirements. For each requirement, we then made interface design recommendations.
The different types of verbal protocols (think-aloud and CDM), reflecting the intuitive-to-analytical spectrum of diagnostic reasoning, revealed the same key cognitive requirements in the diagnostic process. However, we identified different types of errors and strategies in the different types of protocol. For example, in the think-aloud protocols, we frequently identified omissions in information search (physicians not asking diagnostic questions/not performing important examinations or investigations). In the CDM protocols, on the other hand, we identified “sticking” to an initial diagnostic hypothesis as the most frequent cause of errors. Such hypotheses were based on, for example, a colleague’s opinion, an earlier diagnosis, or previous knowledge about the patient leading to erroneous inferences about the current problem.
The process of transforming decision requirements into design recommendations is a critical one (Klein, Kaempf, Wolf, Thorsden, & Miller, 1997). For each requirement, we reviewed the diagnostic events to identify human–computer interaction (HCI) concepts that could have provided useful support to the physician. We worked from the decision requirements themselves, but also went back to the protocols, to identify the type of information or perspective that could have made it easier to fulfill the requirement. This process enabled us to recommend HCI features for each decision requirement (Table 3). We limited the scope of the design recommendations to the diagnostic tool and its interaction with the EHR and did not attempt to redesign the whole EHR system.
1. Retrieving Information From the Patient Record
Family physicians must retrieve and integrate information from the patient record to build an understanding of the patient’s condition. They scan the EHR and its summary screen looking for significant information, either by browsing in a structured way (problems, medications, previous consultations) or by actively filtering information (e.g., display only high-priority problems). Important information may, however, be missed if it is not well presented and emphasized in the record or due to time constraints and distractions:
I missed once a cancer case. It was a woman in her 50s coming with a headache, I missed the information that when she was young she had cancer, it was in the record but at the very bottom, I didn’t scroll down. (Physician 3, postobservation interview)
Design recommendation
To help retrieve and integrate critical information from the EHR that is relevant to the presenting problem, information should be displayed effectively, for example, as text or icons, in the diagnostic support tool. Such critical information includes risk factors (smoking, excessive alcohol intake, hypertension) and serious past conditions, such as cancers, which are relevant to the patient’s current presenting problem. By making highly visible important patient information, the physician’s situation awareness can be supported better (Stanton, Chambers, & Piggott, 2001).
2. Generating Diagnostic Hypotheses
Physicians generated one or a small number of diagnostic hypotheses early in the consultation. “So it may be that she needs to be encouraged to be a little bit more patient or I’m thinking about disc prolapse” (Physician 9, think-aloud protocols, early myeloma scenario). Different factors, such as a colleague’s opinion and assumptions about the patient (e.g., frequent consulter), may install a leading hypothesis at the exclusion of other alternatives. “I think I was agreeing with the earlier doctor, who saw her a week earlier, that maybe it was a sprain.” “I think it was that feeling of . . . she comes here often, and she’s quite anxious because her husband left her recently and she was all alone and she’s struggling. And she wants reassurance that everything is doing okay” (Physician 1, CDM protocols, missed foot fracture).
Design recommendation
Displaying a list of potential diagnoses by integrating important information about the patient (e.g., age, gender, risk factors) from the EHR with the current health complaint could help physicians generate more diagnostic hypotheses. This design could reduce narrow focus on one diagnosis developing early in the clinical encounter, expand the hypothesis space, and remind physicians of other possibilities that should be considered. Following the results of two recent experimental studies wherein diagnostic accuracy improved over control with the mere presentation of a list of diagnostic hypotheses at the start of the consultation (Kostopoulou, Lionis et al. 2015; Kostopoulou, Rosen et al., 2015), a diagnostic support system could display a list of possible diagnoses as soon as the physician enters the patient’s main health complaint. The list could accommodate information entered before the consultation by other health care staff, such as physician assistants, or patients themselves.
3. Testing Diagnostic Hypotheses
In addition to deciding what questions to ask, examinations to perform, and investigations to order, physicians have to decide when to stop gathering information and proceed to diagnosis and/or management. Physicians seeing the same patient can differ greatly in their diagnostic approach, as illustrated in the following example from the think-aloud protocols. At the first patient visit, Physician 3 asked 18 questions, performed four examinations, and ordered eight investigations before deciding to refer the patient to hospital:
So it’s becoming a bit more, looking like this lady may unfortunately have myeloma, which would fit with this persistent worsening back pain, mild anaemia and raised globulins and urine proteins. . . . So I’m referring her to the haematologist and I’m going to ask as an urgent . . .
Physician 9, seeing the same patient, asked only three questions and told her to come back if the back pain persisted. At the second patient presentation (with prolonged and worsening symptoms), Physician 9 ordered a single investigation (X-ray of the back), and upon discovering that it was normal, the physician decided to prescribe pain relief:
Am I concerned that there’s something that we’re missing or should I just try her for a bit longer with better analgesia? So I think, given that we haven’t tried better analgesia, I think that’s the next thing that I would do. So I’d stick with my diagnosis for now and increase her analgesia.
This example illustrates two factors in the diagnostic process that may lead to error: first, that asking too few questions (presumably driven by a single hypothesis) may lead to misdiagnosis, as important information will not be discovered; second, that once the physician adopts an interpretation, it may prove resistant to change, despite discovering new information that is inconsistent with that interpretation (Kostopoulou, Devereaux-Walsh, et al., 2009; Kostopoulou, Mousoulis, et al., 2009). Information that is unexpected and/or cannot be easily integrated with the physician’s leading hypothesis may be dismissed or normalized: “His hemoglobin is absolutely fine,” declared Physician 1 while thinking aloud after being presented with an out-of-range hemoglobin, even though the abnormal result was marked with an asterisk and the normal range was also provided next to it (“Hb 13.0 g/dL*—normal range 13.5–18 g/dL”).
Design recommendation
In addition to presenting a list of diagnostic suggestions, a support tool should enable users to click on a suggested diagnosis and view the important features (symptoms and signs) that can change the likelihood of the diagnosis. Users can check for these features in the patient and tick either yes or no to indicate their presence or absence. The EHR will be updated automatically and so will the list of suggested diagnoses, if appropriate. For example, the order of the diagnoses may change according to their updated likelihood, and diagnoses may be added or removed. The tool should also propose examinations and investigations that could differentiate between the suggested diagnoses. In this way, physicians are likely to elicit and consider more information.
Data visualization based on the principles of gestalt theory (gaining information “at a glance”) can support perception and situation awareness (Kim & Hoffmann, 2003). When appropriate, the system could contextualize abnormal or borderline investigation results according to patient demographics, risk factors, and main health complaint and present information in a combined visual display.
Coding information into the EHR is necessary for the operation of a diagnostic support system. If information is not coded or is entered in free text, the system cannot use it to support the diagnostic process in any interactive way, for example, by updating its diagnostic suggestions. A diagnostic support system should therefore provide an easy interface for the coding of clinical information (symptoms and signs) during the consultation. In our observations of physicians consulting with patients, we noted that physicians recorded information either during the consultation or after the patient had left the room. Physicians may not record during the consultation, so that they can concentrate on their interaction with the patient. Entering information after the patient has left, however, can result in loss of information and omission errors. Furthermore, we noted that physicians often did not code information but entered it as free text, which cannot be clinically interpreted by a computer. This finding reflects Salisbury and colleagues’ finding that 81% of problems discussed in consultations were recorded as free text and only 37% were coded (Salisbury et al., 2013).
Enabling physicians to indicate quickly either the presence or the absence of important features for specific diagnoses, as recommended earlier, can facilitate and encourage coding. Several other ways are facilitated by EHR systems, for example, hiding clinical codes that are redundant and not in use, auto-complete functionality, providing default values and supporting quick access to previously inserted information, and allowing keyboard shortcuts and the use of abbreviations. The most effective encouragement for the physician to code is likely to be the automatic transferring of the coded information in the appropriate locations of the patient’s EHR. Another solution that also merits consideration and further research is for patients to enter their health complaint and associated symptoms on the computer, in the physician’s waiting room, before the start of the consultation.
Facilitating coding is important for both the acceptance of the tool by physicians and the specificity of its advice, as the coded information would be used by the diagnostic tool to update its list of suggested diagnoses. Furthermore, detailed recording of coded symptoms, including the main health complaint, would enable additional diagnostic evidence to be gathered and subsequently analyzed, consistent with the concept of the “learning health system” (Friedman, Wong, & Blumenthal, 2010).
4. Deciding on Course of Action
Errors in management decisions can stem directly from misdiagnosis. They can also occur if the physician does not “safety net” for serious possibilities and manages only for what he or she considers to be the most likely diagnosis: “Normally, there’s lots of things that I didn’t do. To come back if worse—that’s the usual safety net; to come back if worse, covering myself” (Physician 2, CDM protocols). Finally, errors may occur due to insufficient knowledge about the most appropriate way to manage a specific disease. “So I’m going to be referring her for an urgent rheumatology review” (Physician 4, think-aloud protocols, suspected myeloma but referred to rheumatology rather than oncology).
Design recommendation
When the physician enters a diagnosis, he or she should be able to link directly to the relevant clinical guidelines and forms for referring to specialists, ordering investigations, and/or prescribing. This linking could be done by context-dependent information tools, such as “infobuttons.” Infobuttons can be incorporated into the diagnostic support tool and integrate data about the patient and the clinical context to provide immediate, point-of-care access to relevant knowledge resources (Cimino, Li, Bakken, Patel, 2002). Clicking on the infobutton, next to the selected diagnosis, could display to the physician specific information about the management steps that she or he should take. Selecting a step could then display the relevant form (e.g., request form for referral or investigation). The infobutton would be linked to the latest clinical guidelines to provide accurate information at the point of care and prevent management errors. Many U.K. EHR systems already provide an infobutton or equivalent functionality, so it does not need to be redesigned into the diagnostic tool.
Discussion
Using multiple methods and data sources, we elicited cognitive requirements of the diagnostic task and made specific user interface design recommendations for a computerized diagnostic support tool that will integrate seamlessly with the patient’s EHR and will be triggered upon entry of the patient’s current health complaint. The tool will suggest diagnoses for physicians to consider early in the process, so that a narrow focus on a single hypothesis is lessened. The tool should also facilitate data coding and insertion, so that physicians enter more coded information into the EHR. It should suggest symptoms and signs that are important for the relevant diagnoses and highlight significant information in the EHR. These features should enhance the tool’s usefulness and acceptability.
Existing design recommendations for decision support systems emphasize the importance of integration with the EHR, the consideration of the physicians’ work flow (Musen et al., 2014), and support of the physicians’ cognitive tasks (Patel & Kaufman, 2014). According to Stead and Lin’s (2009) National Academy of Sciences seminal report, current systems provide little support for the cognitive tasks and work flows of clinicians. One of the report’s main conclusions is the need to provide “patient-centered cognitive support” that helps to “integrate patient-specific data where possible and account for any uncertainties that remain” (Stead & Line, 2009, p. S-4). By eliciting and analyzing family physicians’ decision making and cognitive requirements during the diagnostic process, we provide design recommendations to ensure that cognitive challenges are addressed for the spectrum of diagnostic reasoning, from the more intuitive to the more analytical. By integrating diagnostic support with the EHR and using patient-specific information to produce diagnostic recommendations, we are making an important step in the design of patient-centered cognitive diagnosis support.
Strengths and Limitations
The strength of our work resides in its use in its use of a unique combination of multiple methods for data collection and analysis (observations, interviews, HTA, CTA, and SAR) that helped to elicit cognitive user requirements of the diagnostic task. There are many CTA methods and tools available. Using a CTA entails selecting and applying a combination of methods and tools appropriate to the task and domain being investigated (Baxter, Monk, Tan, Dear, & Newell, 2005). Combining different techniques is encouraged for eliciting requirements in software engineering (Nuseibeh & Easterbrook, 2000). Nevertheless, most studies still tend to use one or a subset of these methods, and traditional techniques, such as questionnaires and interviews, are still most commonly used (Zowghi & Coulin, 2005). CTA extends those traditional task analysis techniques to facilitate the collection of information about the cognitive processes underlying observable task performance (Chipman, Schraagen, & Shalin, 2000).
We used two different types of secondary data: think-aloud protocols of family physicians diagnosing challenging cases (early presentations of cancer) and interview transcripts wherein family physicians described past cases of intuitive diagnoses. By using different types of secondary data, we wanted to ensure that the requirements elicited and design recommendations proposed are relevant to and can support the different modes of clinical thinking, from intuition to analysis (Evans & Stanovich, 2013), on a range of clinical cases. For most of these cases, the correct diagnosis was known. It was therefore possible to identify errors and difficulties in the diagnostic process, for example, important information omitted, hypotheses considered or not considered, and misinterpretations, which would have been less likely by simply observing patient consultations in real time and relying on physicians’ self-reports. This use of multiple data sources is novel in the requirements elicitations literature.
A limitation of our work is its focus on the diagnostic task at the exclusion of other tasks that family physicians routinely perform, for example, prescribing. Authors of future work to develop a fully functional diagnostic support tool will need to take into account how the EHR is used to manage other tasks during the consultation and whether these tasks might be affected by the diagnostic tool. Furthermore, for our design recommendations to be effective, some physicians will need to change the way that they are currently interacting with their computer. For example, they will need to enter the patient’s current health complaint at the start of the consultation and read the diagnoses initially suggested by the system. The requirement for such behavioral changes is likely to increase resistance to system adoption. We believe, however, that a fully integrated and fully functional tool will offer substantial benefits to users, so that resistance is reduced and adoption motivation increased. Apart from the current benefits (integration with the EHR, ease of coding, automatic transfer of coded information into the EHR), a fully functional diagnostic support system would be driven by the latest diagnostic information, be constantly updated, and be configured to allow patients and/or other caregivers to enter symptoms preconsultation, so that time for the routine aspects of information gathering is reduced. In addition to these benefits, introduction of the system would require a carefully thought-out “change management” plan to include time for training users on the system. Clear prerequisites for these next steps are that (a) an improvement in diagnostic accuracy is obtained first in a controlled environment (a relevant study is under way), (b) the evidence base driving the tool (symptoms/signs and their link to diagnoses) is rich and trusted by physicians, and (c) the tool’s usability is improved, for example, by less cumbersome ways of data entry.
We envisage (and propose the first steps in) the development of a “learning health system” for diagnosis, where a cycle of evidence-based quality improvement is created, use of the tool supports better coding and structure of routine diagnostic data, the data are made available to researchers to analyze and enrich the clinical diagnostic evidence, and the evidence is fed back into the tools’ recommendations to support better decision making.
Footnotes
Acknowledgements
Ellen Wright and Thomas Round, family physicians and clinical academic fellows at King’s College London, provided clinical advice and helped with piloting the follow-up interviews and recruiting physicians for observation. This study received funding from the European Union’s Seventh Framework Programme for research, technological development and demonstration under Grant Agreement No. 247787 [TRANSFoRm]. Financial support for the study that elicited the think-aloud protocols was provided by Cancer Research UK to Olga Kostopoulou, under the NAEDI scheme (ref. C33754/A12222). Financial support for the study that elicited the critical decision method interview protocols was provided by a departmental PhD studentship to Amanda Woolley. Ethical approvals were obtained from the North West London Research Ethics Committee 2 (10/H0720/50) and West London Research Ethics Committee 2 (11/LO/0079).
Talya Porat is a researcher in human–computer interaction, human factors, and cognitive engineering, with a special interest in the medical field. She led the work on user requirements and design for the diagnostic support system.
Olga Kostopoulou is a psychologist studying judgment and decision making, with a focus on diagnostic reasoning, error, and cognitive biases. She led the overall project for the development and evaluation of the computerized diagnostic support tool.
Amanda Woolley obtained her PhD in psychology under the supervision of Olga Kostopoulou. She researched clinical intuition in family medicine from a cognitive psychology perspective.
Brendan C. Delaney is the scientific director of TRANSFoRm (transformproject.eu). He is an academic primary care physician with an interest in diagnosis and medical informatics.