
Abstract
In this study, participants with a self-reported history of depression, diabetes, or no illness underwent a simulated informed consent process for a hypothetical genetic study related to depression or diabetes. Participants completed a survey assessing their perceived understanding of the research process, perceptions of its risks and benefits, their satisfaction with the informed consent process, and their readiness to make a hypothetical enrollment decision. All participants indicated strong readiness to make an enrollment decision regarding the research characterized in the simulation. Participants reported understanding the consent process relatively well and being generally satisfied with it. Greater concerns were expressed regarding psychosocial risks than biological risks for genetic studies on mental disorders. Our study documented positive attitudes toward volunteering for research that involved the collection of genetic data.
Introduction
Factors that influence enrollment decisions for clinical research, primarily in relation to the investigation of serious illnesses, have been explored for decades (Candilis, Fletcher, Geppert, Lidz, & Appelbaum, 2008; Dunn & Jeste, 2001; Grisso & Appelbaum, 1995; Jeste et al., 2007; Palmer et al., 2005). It is well established, for example, that research volunteers living with either physical illness or mental disorders may enroll in clinical research with the hope that participation will reduce the symptoms of their illness or assist in their progress toward recovery, even though clinical research aims to advance knowledge and not to provide treatment (Thong et al., 2016). The experience of becoming ill, being unable to access treatment, feeling hopeless, or feeling pressure in the informed consent process may drive participation decisions and render volunteers vulnerable in the research situation (Barata, Gucciardi, Ahmad, & Steward, 2006; Calnan, Montaner, & Horne, 2005; Carpenter et al., 2000; Fields & Calvert, 2015; Leykin, Dunn, & Munox, 2017; Marco, 2008; Palmer et al., 2005). For research that involves the collection of genetic data, participation decisions of ill individuals may be additionally influenced by concerns about privacy or the future health of themselves or their family (Hoop, Roberts, & Hammond, 2009). As genetic research continues to advance, a deeper comprehension of the perspectives of potential participants is crucial to fulfill the Belmont principles of respect for persons, beneficence, and justice underlying ethically sound research (National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research, 1979).
One important ethical safeguard is informed consent, which seeks to ensure that individuals with adequate decision-making capacity have an accurate understanding of the intent, procedures, risks, and benefits associated with a research protocol. Informed consent serves to support free and uncoerced enrollment decisions by potential volunteers. Optimal practices and challenges in informed consent processes have been extensively studied (Cho et al., 2015; Faden, Beauchamp, & Kass, 2014; Kraft et al., 2016), but how healthy and ill individuals perceive informed consent for research involving a genetic component is less understood. Moreover, some have raised concerns on theoretical grounds that people living with mental disorders have differing views and vulnerabilities in relation to research participation when compared with people living with physical disorders (Leykin et al., 2017). Past empirical work has revealed that mentally ill, physically ill, and healthy populations have diverse perspectives and varied ways of framing ethical issues in clinical research (Kim & Roberts, 2015; Roberts & Kim, 2014), emphasizing the need for further testing and investigation of the perspectives of these populations. More recent empirical ethics work has focused on genetic research in particular, in part, due to the National Human Genome Research Institute’s (NHGRI) Ethical, Legal, and Social Implications (ELSI) Research Program, and the expansion of enabling technologies dedicated to genetics. In addition, very little is known about how people in good health view participation in genetic research compared with people with a history of physical illness or mental disorders.
To address these gaps in knowledge, we conducted a novel pilot study to simulate the informed consent process for a genetic study. We engaged with individuals who self-reported a history of diabetes or depression and with individuals who reported neither condition. We evaluated their understanding of the hypothetical genetic study presented in the simulation and assessed their views of the informed consent process (Roberts & Kim, 2017). Our aim in this article is to assess how lived experience with either a physical or mental disorder might be related to perspectives that are salient in the process of providing informed consent for a genetic research study. We examined perceived levels of understanding, views of the consent process, levels of comfort and satisfaction, and perceived readiness to make a decision about participation. We sought to understand whether responses would differ by health status. This study attempts to begin to address some of the unknowns in the recruitment of ill and healthy individuals to genetic research studies.
Method
In this minimal risk, institutional review board (IRB)-approved study led by LWR, we simulated an informed consent process for a hypothetical genetic study. We then administered a survey to query attitudes related to the simulated informed consent process and assessed aspects of the hypothetical consent procedure as perceived by our volunteers. The Human Research Review Committee of the University of New Mexico provided prospective approval of this minimal risk study.
For our intervention, we designed simulated informed consent processes that were based on actual genetic studies on depression and diabetes. The creation of parallel genetic research studies for diabetes and depression in this simulation allowed for direct comparison of responses, based on whether mental disorders research or physical illness research was being proposed to potential volunteers. Participants with a self-reported history of diabetes or depression or no history of either illness allowed for contrasting responses of participants. Figure 1 describes the design of this study.

Study design.
Recruitment, Consent, and Settings
Adult participants were recruited through flyers posted in outpatient clinic settings at the University of New Mexico. Volunteers with self-reported diabetes were deterministically assigned to the diabetes simulated consent process; similarly, volunteers with self-reported depression were assigned to the depression simulated consent process. Volunteers without self-reported history of diabetes or depression were randomly assigned to either the diabetes or the depression simulated consent process.
This study design was not a randomized controlled trial, as deterministic assignment was used for a portion of the volunteers. Our intent was not to design a randomized trial to infer a “treatment” effect but rather to compare the perspectives, postprocedure, from individuals with diabetes, individuals with depression, and individuals without lived experience with either illness. The intent of the protocol assignments was to allow the simulated consent procedure, although hypothetical, to be tailored to participants and anchored in personally relevant history whenever possible; this meant that for volunteers without self-reported history of diabetes or depression, the procedure was entirely hypothetical. Our study involved the piloting of a previously untested instrument to generate hypotheses for a larger ethical survey regarding psychiatric genetics research.
Simulated Consent Procedure
Our project was designed to simulate or mimic a consent procedure that an investigator or researcher would go over with someone who was being considered for an actual genetic research study. Study personnel who administered the simulated consent procedure were required to follow a scripted consent form to receive oral consent for this study. Study participants who consented to our study then underwent the simulated consent procedure for a genetic study.
An interviewer, who was also a trained research professional, explained the simulated consent procedure and obtained verbal consent for participation. Participants read a simulated consent form for the diabetes or depression genetic study and discussed it with the interviewer. The consent form provided additional written information about a genetic research study as if the participant were actually being asked to participate in that genetic study. The consent form explained what the study was about, the risks and benefits of such a study, and how the participants’ identities would be protected. The two consent scenarios were evenly and randomly distributed between two interviewers. Participants then completed a written survey about their understanding, participation willingness, and satisfaction with the consent process. The procedure was designed to take no longer than 30 min.
Description of the Hypothetical Study
The interviewer explained the purpose of the study—“to understand how genetics and environment influence the development of diabetes (or depression)”—and the specifics of what would be done according to a written script. Specifically, all participants were told that they would be asked to (a) fill out a questionnaire about physical (or mental) health and family history of health, (b) fill out two diabetes (or depression) scales, and (c) give a blood sample that will be stored indefinitely and used by future studies only about physical (or mental) illnesses. Participants were told that the results of the depression or diabetes scales would be explained, but that the results of the genetic studies would not be disclosed to them and that reports from future research done using their blood samples would not be disclosed to them or to their doctor. Participants were told that if the hypothetical genetic study revealed information that would potentially be important to their health or the health of their families, they would be contacted to participate in a further study in which they would have the option of learning about the results. The physical and psychosocial risks of the study, the benefits, and other options were then explained to the participants.
Survey Instrument
Based on prior conceptual and empirical work in the area of informed consent and alternative decision making (Roberts, 2002; Roberts, Hammond, Warner, & Lewis, 2004; Roberts, Warner, & Brody, 2000; Roberts et al., 2002) and dialogue with community residents, a new written survey instrument was developed for this project to explore issues encountered by people living with and without depression or diabetes.
Author LWR constructed a survey in three parts: 31 scaled or open-ended questions concerning attitudes toward participation in genetic research, seven items concerning satisfaction with the simulated consent procedure, and 11 demographic questions. The survey portion concerning satisfaction with the consent process was administered in a written format and blinded from the interviewer. The survey instrument took approximately 30 min to complete. Data were collected anonymously. For this article, we used only the items in the survey related to respondents’ perceived understanding of the hypothetical genetic research study and expressed satisfaction with the consent procedure for the hypothetical genetic research study. All items used for analysis are presented in the supplemental table.
Sample
Ninety-one study individuals were eligible for study inclusion. Of these, 12 individuals were not willing to undergo the simulated informed consent procedure (87% participation rate in our project). Among these 12, five individuals cited “no time” as a reason for not participating, three cited no interest in the particular study, and two stated other reasons. In total, 79 individuals participated in the study. Study volunteers were compensated US$20 in cash for their time and effort.
Outcome Measures
Primary outcomes
The main measures for this analysis included (a) respondents’ perceived understanding of the hypothetical genetic research study and (b) respondents’ expressed satisfaction with the interactions of the consent process. Nine items were rated on a 9-point scale, and four items were open ended. The organization of themes and items are shown in the supplemental table.
Coding of qualitative data
Study participants expressed their concerns regarding a genetic study about a mental (or physical) illness in open-ended qualitative responses. We coded the responses as being one of the following: no concerns, psychosocial, biological, both psychosocial and biological, or “other.” Qualitative responses regarding perceived benefits of being in a genetic study about a mental or physical illness were coded as one of the following: “finding a cure or new scientific knowledge,” “a personal benefit,” “helping others or helping society,” or “two or more reasons stated above.”
Statistical Analysis
T tests and chi-square tests were used for continuous and categorical data, respectively, as appropriate. Contingency tables were used to assess the association between explanatory variables and outcome variables, and Fisher’s exact tests or chi-square tests of associations were performed. Single items of outcome responses (9-point rating scaled responses) were analyzed with univariate analysis of variance, and multivariate analysis of variance was used to test items together as a theme. SPSS and R were used for statistical analysis.
Results
Characteristics of Respondents
Complete data were obtained from 79 individuals, 34% (n = 27) of whom had a previous history of depression, 19% (n = 15) of whom had a history of diabetes, and 47% (n = 37) of whom were healthy by self-report and denied prior history of either depression or diabetes. Of the 79 volunteers, 54% were women (n = 43) and 46% were men (n = 36). The mean age was 42.5 years (SD = 13.2 years). During the study, two individuals were given a simulated protocol that did not match their prior history of either depression or diabetes. We excluded these two cases, resulting in 77 individuals for analysis (Table 1).
Demographic Characteristics of Study Participants Assigned to Simulation of Consent to a (Hypothetical) Depression or Diabetes Genetic Protocol.

Note. HS = high school; GED = general educational development.
M and interquartile range reported.
Study Participants’ Expressed Satisfaction With Informed Consent Simulation.

Note. A significance level of .05 was used.
Participants diagnosed with a major illness were older than healthy participants (M ages = 45.8 vs. 48.8 years, t test P = .02). A greater majority of participants in the simulated consent for a diabetes study were married or living with a partner, compared with a minority of participants in the simulated consent for a depression study (63% vs. 32%, χ2 test P = .01). Race was also unbalanced across diabetes and depression groups; the latter group had a greater proportion of individuals who identified as white, but not Hispanic compared with the former (proportion identifying as white in depression and diabetes groups: 56% vs. 18%, χ2 test P = .01).
Perceived Understanding of the Hypothetical Genetic Research Study
Respondents stated that they understood the information very well (M = 7.8, SD = 1.4) and 96% (n = 74) expressed that they understood the information at least fairly well. A similarly high proportion of respondents, 92% (n = 71), felt that they could explain to a friend or family member what was involved in participating at least fairly well (M = 6.8, SD = 1.7).
More women than men reported a strong perceived understanding of the information in the consent form, as measured by rating a 7 or higher on a 9-point scale (94%, n = 40, vs. 77%, n = 26, P value from Fisher’s exact test = .05).
Perceived concerns and benefits about being in a genetic study
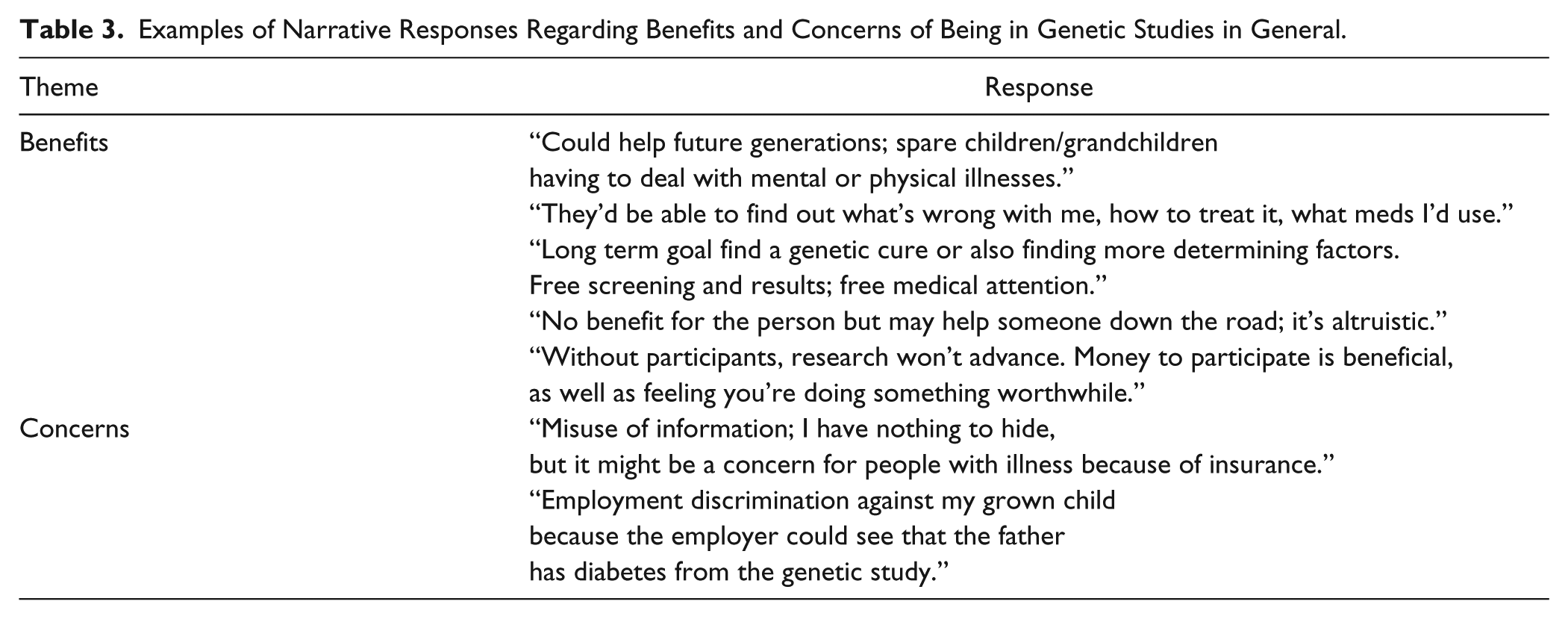
Thirty-one percent of participants expressed psychosocial concerns about being in a genetic study about mental disorders (n = 25); 21% (n = 16) expressed concerns related to biological or physical risk (Tables 3 and 4). Thirty-eight percent of participants had no concerns to report (n = 30).
Examples of Narrative Responses Regarding Benefits and Concerns of Being in Genetic Studies in General.
Examples of Narrative Responses Regarding Perceived Safeguards of Genetic Research.
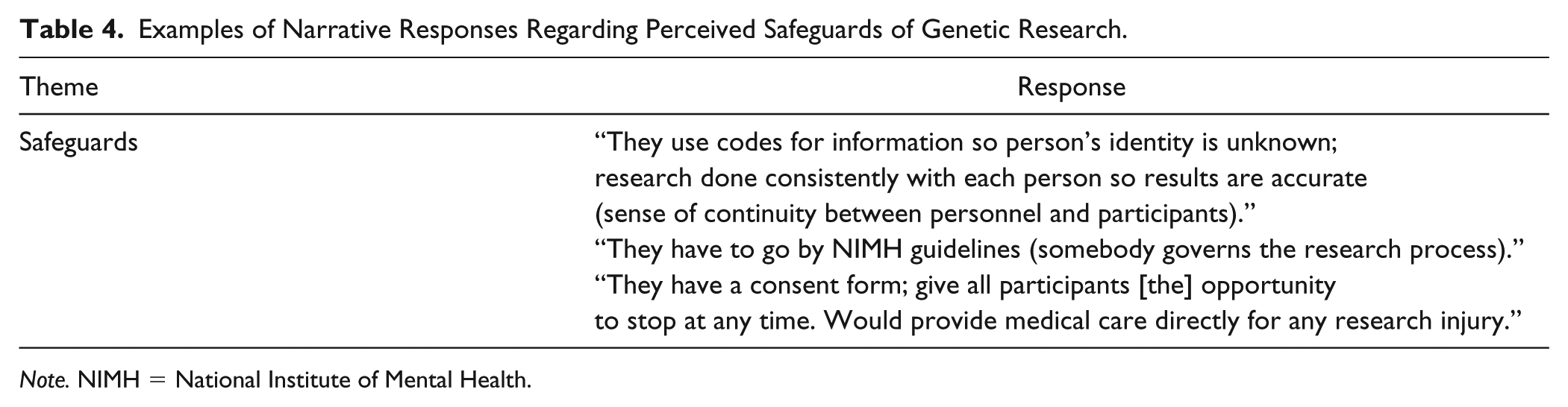
Note. NIMH = National Institute of Mental Health.
Twenty-nine percent of respondents felt that a perceived benefit of being in a genetic study about mental illness was “finding a cure or new scientific knowledge” (n = 23), whereas 28% of respondents felt that there was a personal benefit (n = 22). A similar proportion of respondents, 23%, thought that “helping others or helping society” was a benefit of being in a genetic research study about mental disorders (n = 18). Only 4% stated that there were no perceived benefits of being in a genetic study about mental disorders (Figure 2).
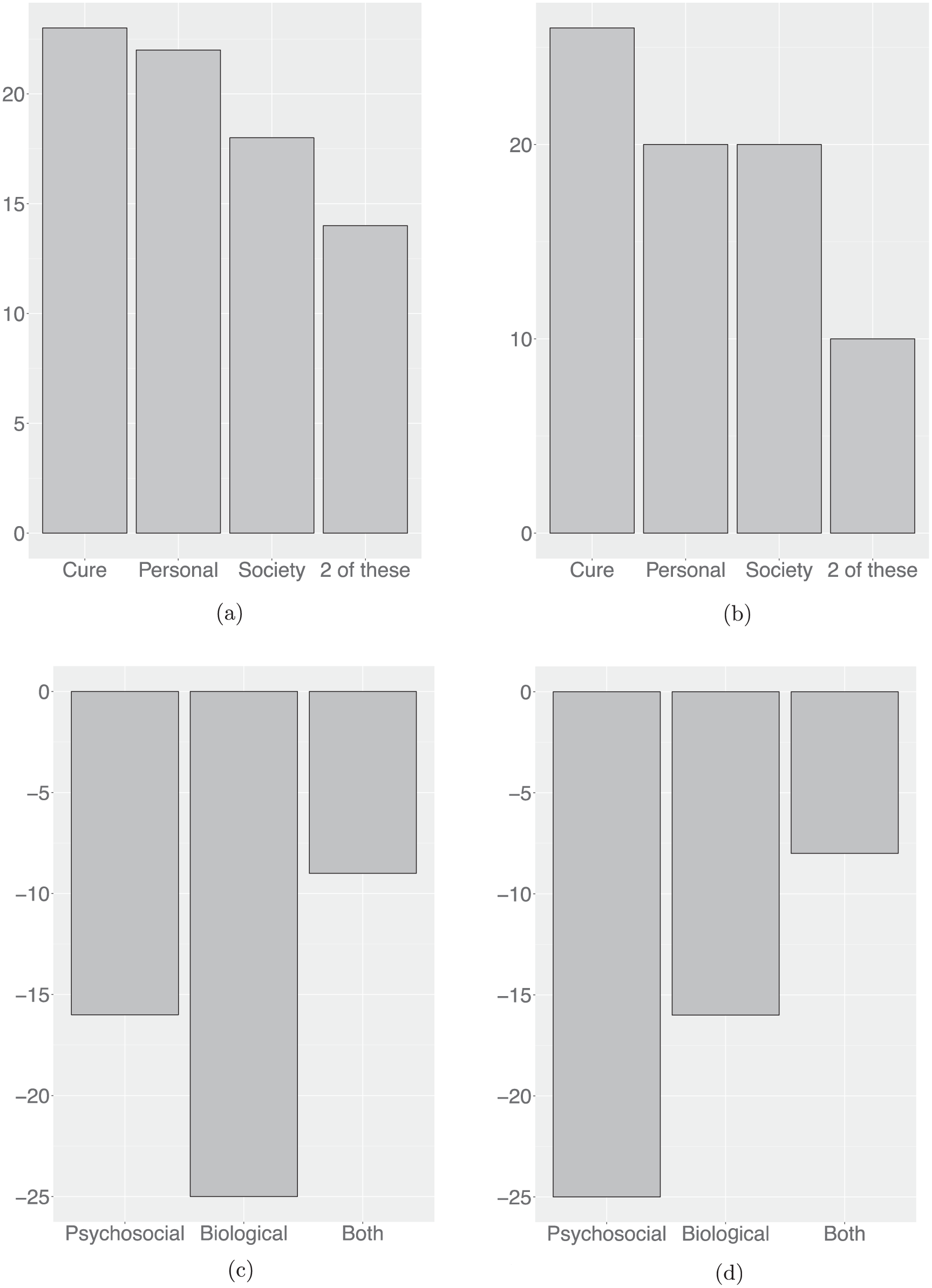
Perceived benefits and concerns of genetic studies in general: (a) benefits of a study about physical illness, (b) benefits of a study about a mental disorder, (c) concerns for a study about physical illness, and (d) concerns for a study about a mental disorder.
Among all respondents, 73% (n = 57) expressed the same benefits for being in a genetic study about a physical illness as they did for being in a genetic study about mental disorders. Only 27% (n = 22) expressed different benefits for a genetic study about a physical illness. For example, a different benefit expressed about being in a genetic study about a physical illness was “It would help doctors increase their knowledge.” Other mentioned benefits are listed in Tables 3 and 4.
Expressed Satisfaction With the Consent Process for the Hypothetical Genetic Study
Sufficiency of information provided
Respondents endorsed strong positive views of the consent process (Table 2). In particular, respondents felt that their questions about the study were answered very well during the simulated consent process (M = 8.01, SD = 1.51). Respondents endorsed that sufficient information was provided to allow them to decide whether to participate (M = 5.84, SD = 1.51, scaled from 1 = too little information, 5 = enough information, and 9 = too much information), with no differences found by study type, health status, or gender.
Readiness to make a decision
Overall, respondents felt very ready to make the decision about participation (M = 7.62, SD = 1.75, scaled from 1 = not at all ready to 5 = somewhat ready to 9 = very ready). Respondents reported feeling very little to no pressure to participate in the study (M = 1.85, SD = 1.78, scaled from 1 = no pressure at all to 5 = some pressure to 9 = a lot of pressure).
Comfort with interaction
Overall, respondents indicated that the process of reviewing or going over the consent form was very comfortable (M = 8.12, median = 9, SD = 1.41, scaled from 1 = not at all comfortable to 5 = somewhat comfortable to 9 = very comfortable) and that the interaction with the researcher made them more likely to participate in the study (M = 7.13, SD = 1.60, scaled from 1 = much less likely to 5 = no difference to 9 = much more likely).
Discussion
This preliminary study examines the views of individuals of differing health status regarding their attitudes toward informed consent for genetic research. Our novel methodology involved a carefully designed informed consent simulation for a hypothetical genetics study focusing on either depression or diabetes. To understand the influence of health status, we compared responses of individuals living with depression, diabetes, or neither condition.
Respondents felt that the consent process gave them adequate understanding to make an enrollment decision, with nearly all feeling that they understood the information fairly well. Women expressed a strong perceived understanding of the information in the consent form. Reasons for participation included the desire to help others, to help advance science, and to attain personal benefit. Depression studies and diabetes studies were seen as having similar benefits, with narrative comments spread almost uniformly across the goals of “finding a cure” and “helping society.” These findings are consistent with other published reports suggesting interest in learning about genetics and in enrolling as a volunteer in genetic research (Groth et al., 2016; Kerath et al., 2013; Michie, Henderson, Gerrett, & Corbie-Smith, 2011). The vast majority of our participants endorsed “privacy” as the safeguard of greatest importance, for instance, and emphasized the role that investigators might play in protecting individuals who participate in their research studies.
We did find some contrasts in concerns (e.g., risks or negatives) based on the nature of the genetic research study to be conducted. For genetic research studies on depression, greater concern was expressed regarding psychosocial risks than biological risks, perhaps reflecting the importance of stigma in the context of mental disorders. Participants were sensitive, for instance, to the impact of learning worrisome information or of experiencing worsened feelings of depression in the depression-related genetic study. By contrast, the blood draw was the greatest concern associated with the diabetes-related genetic study.
Our study did not demonstrate a pattern of consistent differences in attitudes based on health status, that is, whether individuals had had personal, lived experience with diabetes or depression or neither condition. Across ill and non-ill groups, perceived benefits were heavily weighted over potential risks, with participants most commonly expressing no concerns about a genetic research study. We did find one difference, which was not large in magnitude but bears emphasis; responses from those in the depression group suggest that more time to consider the decision to participate in research would be valuable. In addition, respondents assigned to the simulated genetics protocol group for depression felt less strongly that they had sufficient time to think about their decision to participate in the study, compared with the respondents assigned to the simulated genetics protocol group for diabetes (Ms 7.3 vs. 8.2, P = .05).
Best Practices
Advances in science to foster human health are reliant on the engagement and participation of volunteers who generously collaborate with researchers in learning about illnesses’ causes, consequences, and cures. This preliminary study suggests that individuals with depression diabetes and individuals in good health bring similar attitudes to the research situation. It appears that these individuals also bring many hopes to the research situation and may naturally wish to think less about possible negatives that may arise in relation to their enrollment in research studies. Our study suggests that individuals with depression may desire a bit more time in making decisions or in engaging with researchers during the informed consent process. These observations underscore the importance of the informed consent safeguard in assuring the accurate understanding and capable and free decision making of potential volunteers. Rigor in the informed consent process is also essential in grounding and demonstrating the ethical attentiveness of investigators who are participants’ partners in the research collaboration that they have undertaken together.
Research Agenda
Our results suggest that potential volunteers may de-emphasize risks and amplify benefits of research when weighing whether or not to enroll, reinforcing concerns about the potential biases shaping informed consent in the research situation (Thong et al., 2016). Our findings merit further exploration and validation. These results serve as a reminder to those who conduct genetic research to clarify the knowledge base and motivations associated with enrollment decisions when obtaining informed consent from potential volunteers.
The strengths of this preliminary study include the ability to compare perspectives of individuals with depression or diabetes and individuals in good health. A key limitation of this study is that the individuals who volunteered for this minimal-risk project may be relatively inclined to volunteer for human studies, and so, their responses may not be representative of all potential participants. We used recruitment methods that are common in health research, however, and believe that this allows our project to have strong relevance and greater ecological validity. This said, our project cannot answer the question of how individuals would act in nonhypothetical (“real life”) situations, as our approach involved a simulation, a fact that was disclosed as part of our own consent procedure. Although the design mimicked an “experiment,” this was not a randomized trial and the goal was not to test the effect of a so-called treatment; therefore, resulting inferences are not causal but are associative. Our goal was to compare differences in views about salient issues of informed consent and whether these attitudes differed on the basis of self-reported history of illness, while exploring other personal characteristics that could be relevant.
Educational Implications
Our findings provide insight into how potential participants of genetic studies perceive the risks and benefits of research, and whether potential participants understand and are satisfied with informed consent procedures. In our study, psychosocial concerns clearly outnumbered biological concerns for genetic research studies on mental disorders. For genetic research studies on physical disorders, the reverse was true. Researchers and review board members should be aware of the potential tendency of research participants to de-emphasize risks over benefits. It is crucial that psychosocial concerns are appropriately addressed when dealing with genetic research about mental disorders. Psychosocial risks should be afforded the proper weight and attention during the informed consent process. As privacy and confidentiality concerns become increasingly paramount, researchers and IRBs will need to anticipate risks associated with research in which genetic or other identifying materials may be stored for future use and risks associated with studies using next-generation technologies.
Supplemental Material
6_PGRE_supplementary_table_0402 – Supplemental material for Attitudes Regarding Enrollment in a Genetic Research Project: An Informed Consent Simulation Study Comparing Views of People With Depression, Diabetes, and Neither Condition
Supplemental material, 6_PGRE_supplementary_table_0402 for Attitudes Regarding Enrollment in a Genetic Research Project: An Informed Consent Simulation Study Comparing Views of People With Depression, Diabetes, and Neither Condition by Jane Paik Kim, Katie Ryan and Laura Weiss Roberts in Journal of Empirical Research on Human Research Ethics
Footnotes
Acknowledgements
The authors express their appreciation to Jessica Alcalay Erickson; Jennifer Niskala Apps; Teddy Warner, PhD; Kate Green Hammond, PhD; and Rene M. Paulson, PhD, for their assistance in the development of this project and the data analyses performed; and to Megan Smithpeter, MD, who served as the project assistant for this work. Additional appreciation is expressed to Gabrielle Termuehlen for editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health and National Human Genome Research Institute under Grant 5R01MH074080.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.