
Abstract
Pacific Islanders are the second fastest-growing population in the United States; however, Pacific Islanders, and Marshallese specifically, are underrepresented in health research. A community-based participatory research (CBPR) approach was used to engage Marshallese stakeholders and build an academic-community research collaborative to conduct health disparities research. Our CBPR partnership pilot tested a multicomponent consent process that provides participants the option to control the use of their data. Consent forms used concise plain language to describe study information, including participant requirements, risks, and personal health information protections, and were available in both English and Marshallese. This study demonstrates that when provided a multicomponent consent, the vast majority of consenting study participants (89.6%) agreed to all additional options, and only five (10.4%) provided consent for some but not all options. Our description of the development and implementation of a multicomponent consent using a CBPR approach adds a specific example of community engagement and may be informative for other indigenous populations.
Keywords
Introduction
From 2000 to 2010, the Pacific Islander population increased by 40% making it the second fastest-growing population in the United States (Grieco, 2001; Hixson et al., 2012). Arkansas saw a 197% increase in the Marshallese population (a Pacific Islander population) from 2000 to 2016 and has the largest Marshallese community in the continental United States, with the largest concentration residing in the northwest region of the state (United States Census Bureau, 2000/2016). Rapid migration has been perpetuated by the Compact of Free Association (COFA) with the United States and the Republic of the Marshall Islands (RMI) that was signed in 1986. The COFA grants the U.S. military exclusive access and control over a strategic base of operations in the Pacific and allows Marshallese migrants to freely enter, live, work, and study in the United States without a visa (108th United States Congress). Marshallese in the United States experience significant health disparities and report a high prevalence of diabetes, heart disease, and obesity (Hawley & McGarvey, 2015; Look et al., 2013; Mau et al., 2009; McElfish et al., 2017a, 2017b; Okihiro & Harrigan, 2005; Schiller et al., 2012; Tung, 2012; US Department of Health & Human Services Office of Minority Health, 2015). Furthermore, Marshallese mothers are disproportionately likely to have poor maternal health outcomes compared to other racial and/or ethnic groups (Centers for Disease Control & Prevention, 2011; Chang et al., 2010, 2015; Lavery et al., 2017; Nembhard et al., 2019a, 2019b; Rao et al., 2006; Silva et al., 2006; Tsitas et al., 2015; Wartko et al., 2017). Pacific Islanders, and Marshallese specifically, are also underrepresented in research, which perpetuates and further obscures these health disparities impacting this vulnerable community (Compact of Free Association Community Advocacy Network, 2014; McGrath & Ka'ili, 2010; Palafox et al., 2002; Roehr, 2010).
Health disparities research with the Marshallese community is complicated by historical trauma resulting from a nuclear weapons testing program conducted by the U.S. military in the Marshall Islands from 1946 to 1958 (Barker, 2012). The atolls and islands of the RMI were ground zero for the denotation of 67 nuclear devices equivalent to 7,200 Hiroshima-sized bombs (Barker, 2012). Marshallese exposed to nuclear radiation were enrolled in Project 4.1 so U.S. scientists could study the health effects of radiation exposure; however, Marshallese participants did not provide informed consent, and study documents were not translated into Marshallese (Barker, 2012; Bond et al., 1955; Conrad, 1992; Cronkite et al., 1954). A legacy of the historical trauma of Project 4.1 is that many Marshallese distrust researchers and are often reluctant to participate in research (Duran et al., 1998; Evans-Campbell, 2008; Mohatt et al., 2014).
Community-based participatory research (CBPR) has effectively been used as a research approach for studies with populations facing barriers perpetuated by historical trauma (Minkler, 2004; Minkler & Wallerstein, 2008; Vaughn et al., 2016; Wallerstein, 1999; Wallerstein & Duran, 2006). The CBPR paradigm is one of inclusiveness and engagement in which community stakeholders and researchers share power and responsibility over the research process (Gaventa, 1995; Gaventa & Cornwall, 2006; McElfish et al., 2015). Researchers at the University of Arkansas for Medical Sciences (UAMS) and Marshallese stakeholders have built an academic-community research collaborative founded on the principles of CBPR to include community partners in all aspects of the research process with continual engagement over the last 6 years (McElfish et al., 2015, 2017a, 2017b, 2018a, 2018b). A full description of the engagement and development of the CBPR collaborative is available elsewhere (McElfish et al., 2017a, 2017b, 2018a, 2018b).
One of the first objectives of the CBPR collaborative was to determine and prioritize the primary health concerns Marshallese community members wanted researchers to investigate. Cardiometabolic diseases and maternal health were identified as top priorities. To address the health disparities experienced by the Marshallese community, the CBPR partnership has conducted several research projects (McElfish et al., 2018a, 2018b, 2019a, 2019b, 2019c, 2019d, 2020) and used a multicomponent consent process that provides participants the option to control the use of their data while also allowing researchers to link different data sources across multiple studies.
Research practices such as data sharing, linking of data across multiple studies, linking medical record data, and biobanking are important components of biomedical research (Federer et al., 2015). A systematic review of the literature related to attitudes about consenting to expanded and secondary use of research data showed that participants reported a high willingness to participate in biobanking and data sharing; however, willingness to share remains low among individuals from underrepresented minorities (Garrison et al., 2016). A systematic literature review analyzing empirical U.S.-based studies related to American Indian/Alaska Native and Native Hawaiian or other Pacific Islander perspectives on health data privacy reported that many participants voiced a variety of individual and community-level concerns about the potential misuse of their health data, such as discrimination or stigma and confidentiality breaches, and indicated that these concerns deter their willingness to participate in health research (Taitingfong et al., 2020). Metaconsent has emerged as a solution to the ethical concerns related to participants providing consent to expanded and secondary use of research data research (Plough & Holm, 2016). Metaconsent has been implemented for research with clinical data and biological specimens and is built on the concept that participants should be asked how and when they wish to be presented with consent requests (Plough & Holm, 2016).
Regulatory requirements state that consent materials should present concise, understandable study information to ensure that potential participants truly understand all aspects of the study and make an informed and autonomous decision (Larson et al., 2015; Office for Human Research Protections, 2009). Participants who do not speak English or have limited English proficiency face additional barriers that require researchers to implement extended time for discussion while completing the consent process (Koyfman et al., 2016; Wall & Pentz, 2016). The CBPR partnership engaged Marshallese community stakeholders in the development of informed consent materials related to the use of participants' health data for biomedical research. The partners decided to implement a multicomponent informed consent process utilizing the principles of metaconsent. Participants provide consent on a metalevel by designing how they would like to provide consent to the future use of their personal health data or biological specimens (Plough & Holm, 2016) as opposed to providing broad consent to all future use. The multicomponent consent was developed to allow participants to decide how much or how little data they wished to provide and allow for use in future studies. The first study in which the multicomponent consent was implemented was in a mixed-method, longitudinal study to document and characterize gestational weight gain (GWG) for pregnant Marshallese women living in Arkansas. Data were collected at multiple time points and augmented by postpartum data abstraction, which requires linking participant study information to electronic health records. The complex nature of the study made it particularly appropriate for the multicomponent consent. The full study protocol for the GWG study is available elsewhere (Ayers et al., 2020), and the study has been approved by the UAMS Institutional Review Board (IRB#228023). This paper reports the development and pilot implementation results of a multicomponent consent with Marshallese participants.
Methods
Approach
A CBPR approach was utilized for the development, design, and implementation of the multicomponent consent. A Community Action Network (CAN) that included Marshallese community members was collaboratively engaged in all aspects of the research, including developing consent materials. The CBPR research team was composed of interprofessional researchers, study staff, and Marshallese community health workers (CHWs).
Materials for recruitment and consent were collaboratively developed with CAN members and the Marshallese CHWs. Informed consent forms were drafted by the researchers. The CAN members and CHWs reviewed and discussed the content of the consent form and the presentation of information to potential participants in an iterative process that continued until consensus was reached. This process ensured that cultural and linguistic appropriateness were integrated with scientific rigor and regulatory requirements. The consent form was revised 11 times before it was finalized. Female, bilingual (Marshallese and English) study staff, the CAN, and Marshallese CHWs worked with researchers to develop a detailed plan and process for consenting potential participants. Study staff received training on the consent process that included role-playing practice scenarios and were certified by the study manager to begin recruitment of participants after training was completed. Study staff utilized extended time during the consent process to discuss with participants and answer questions. Consent forms used concise plain language to describe study information, including participant requirements, risks, and personal health information protections, and were available in both English and Marshallese.
After consenting to the study and primary data collection, potential participants had the option to agree or decline to: (1) release of medical information about only the mother, (2) release of medical information about the mother and the infant, (3) link to information about the participant in the Arkansas All-Payer Claims Database, (4) use the information for future research studies related to this study and approved by the UAMS IRB, and (5) allow UAMS to link information from this study to other UAMS studies the participant took part in.
Initially, there was only one data abstraction question that combined both mother and child. However, the CAN recommended potential participants be provided options to agree to or opt out of data abstraction for themselves and then separately for their child. Potential participants were asked to select two options: “release of medical information about myself only” and “release of medical information about myself and my infant.” Arkansas has created the Arkansas All-Payer Claims Database to systematically collect healthcare data from a variety of sources; this dynamic tool furthers the state's transparency objectives and empowers Arkansans with information to better understand how and where healthcare is being delivered (Arkansas Center for Health Improvement). Participants were asked to opt in or out of consent to “have my data from this study linked to information about me in the Arkansas All-Payer Claims Database which stores healthcare claims (billing) data from public and private sources.”
Because UAMS has a long-term CBPR commitment to the Marshallese community and anticipates conducting many future studies, potential participants were asked about the use of their information for futures studies and the linking of data across multiple studies with UAMS. Participants were asked to agree to allow UAMS researchers to “use my information for future research related to this study that is approved by the UAMS IRB” and to opt in or out of allowing “UAMS to link information from this study to other UAMS studies I have participated in.” In addition to consenting to participate in a GWG study, the participants were asked the questions in Figure 1. Study results will be disseminated to participants, Marshallese research stakeholders such as federally qualified health centers, community clinics, faith-based organizations and community-based organizations, the broader Marshallese community, and fellow researchers (Purvis et al., 2020, 2021).

Multicomponent consent form options were used in the mixed-methods study with pregnant Marshallese participants.
Recruitment and Consent Procedures
Female bilingual Marshallese CHWs with extensive research training conducted the recruitment and consent. CHWs received training for the consent process that included role-playing practice scenarios and began recruitment after being certified on the consent process by the study manager. Women were recruited through local health clinics, community-based organizations, and faith-based organizations well known by Marshallese community members. Inclusion criteria required that participants be pregnant women who self-reported as Marshallese and were 18 years of age or older.
The consent form was collaboratively developed with Marshallese stakeholders using a CBPR approach that incorporated cultural and linguistic appropriate language. The consent form used plain language to explain the purpose of the study, its requirements, and privacy information. CHWs provided participants with a copy of the consent form and then read the consent aloud to the participants in their preferred language (Marshallese or English). The consent form described what participants were being asked to do if they joined the study, how researchers would collect and use information, and how participants would be remunerated. Participants were also provided information about the All-Payer Claims. Because the consent provided the option for medical records abstraction, the consent form explained the Health Insurance Portability and Accountability Act (HIPAA) release, how this information would be used by researchers if they consented, and instructions about how to revoke the HIPAA release if they wished to do so in the future. Ample time (∼30 min) was provided so participants could review the multicomponent consent options and discuss the study requirements, risks, benefits, and alternatives to participation. CHWs explained the study required participants to complete surveys, interviews, and biometric data collection to record height and weight. The risk to participating was a possible loss of confidentiality, which the consent form explained. Participant privacy protections were included in the consent form and included password protected files, organized in dated folders and stored in locked cabinets. Participant data is also protected by assigning a unique identifying code or number kept separately from data collection forms. The consent process was conducted in a private setting either in the participant's home or in a private room at a local community center. Participants could consent to all, some, or none of the data release options. CHWs explained that the alternative to participation was not to participate and that there were no penalties for not joining the study. The contact information for the principal investigator and coinvestigator was provided on the consent form if participants had further questions about the study. The participant and CHW obtaining the consent each signed the form, and a copy of the signed informed consent form was provided to the participant.
Results
Participant Characteristics
Table 1 shows that 48 women were recruited and consented to enroll in the study. The majority of the Marshallese women participants were born in the RMI (89.6%) with only five participants reporting being U.S. born (10.4%). The mean age of participants was 27.2 years old (SD = 5.7), and most participants were married or in a partnership/unmarried couple (33.3% and 52.1%, respectively), with seven participants reporting their relationship status as single (14.6%). The majority of participants had a high school education or lower (79.2%) reported as their highest level of educational attainment. Approximately two-thirds of participants reported being unemployed: 16 for less than a year (33.3%) and 15 for 1 year or more (31.2%). Only nine participants reported that they were employed (18.8%). Seven participants reported their employment status as homemakers or family caretakers (14.6%), and one participant was a student (2.1%). Approximately half of participants stated they either did not have health insurance (54.2%) or they did not know if they had health insurance (2.1%).
GWG Longitudinal Study Participant Characteristics.
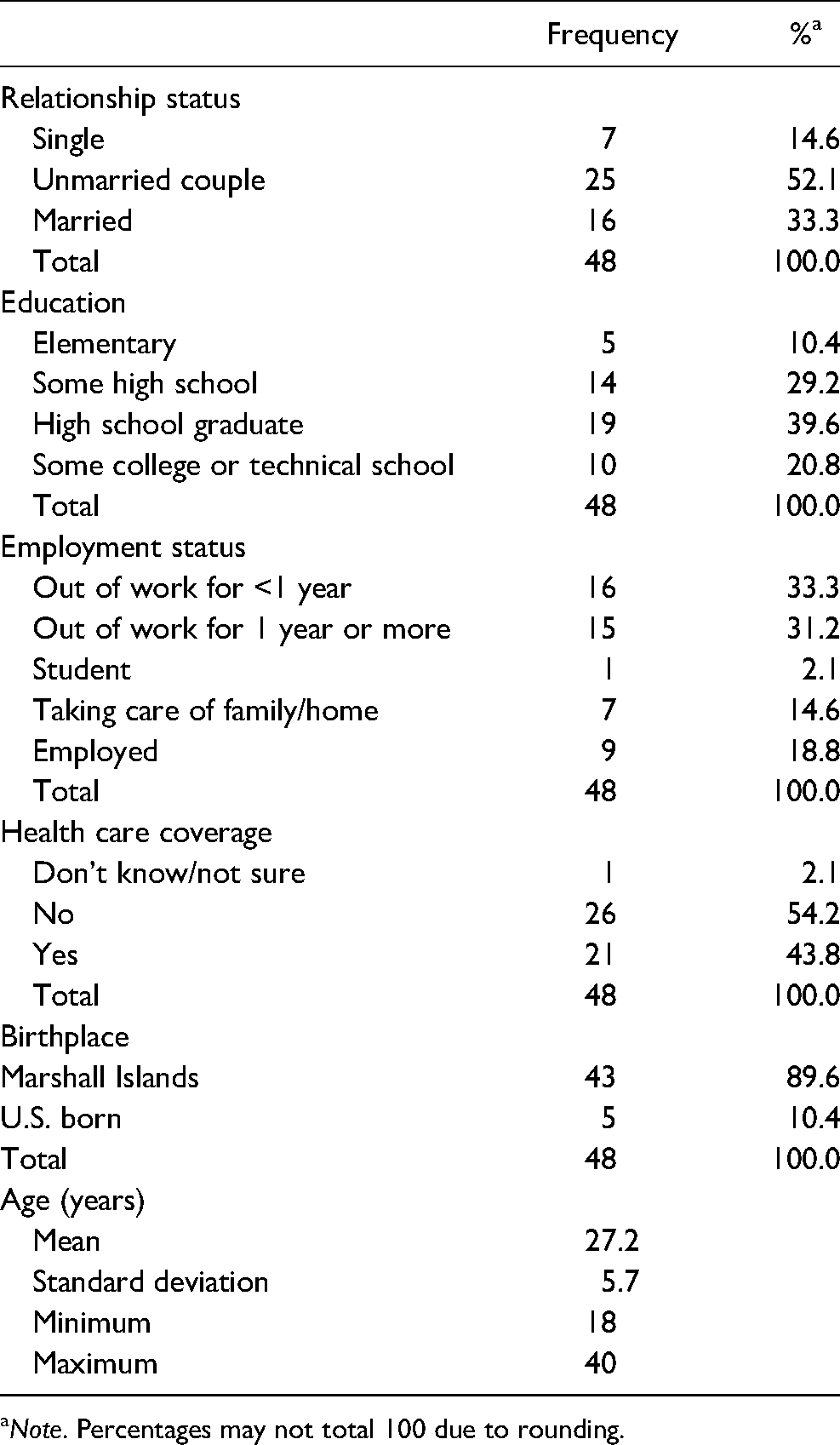
Note. Percentages may not total 100 due to rounding.
Participant Response
A total of 48 participants were enrolled and provided consent to participate in the study. Forty-three participants (89.6%) opted in and consented to all options for data abstraction. One participant only consented to the option to release medical information about herself and her infant; three participants did not consent to release medical information about themselves or their infants but consented to all other options, and one participant consented to release medical information about herself but not her infant, but consented to all other options. Participants who opted out of specific options were not excluded from the study; they participated in the primary data collection events including the study's quantitative surveys and qualitative interviews related to their experiences and perceptions of GWG during their pregnancy (Figure 2).

Consort chart.
Discussion
This study demonstrates that when provided a multicomponent consent, the vast majority of consenting study participants (89.6%) agreed to all additional data abstraction options. No participants abstained from all options, and only five (10.4%) provided consent for some but not all options. This finding is consistent with previous literature that reports broad consent is often preferred by participants when consent options are clearly communicated and privacy is protected (Garrison et al., 2016; Hammack-Aviran et al., 2020). Our findings are also consistent with studies that demonstrated participants' level of willingness to share data was associated with the researchers' affiliations and the design of the consent forms (Hammack-Aviran et al., 2020; Kim et al., 2019; Taitingfong et al., 2020). However, this study contrasts prior literature which demonstrated lower rates of broad consent among minority communities (Garrison et al., 2016).
Cultural considerations are especially important to consider when developing an informed consent process for expanded data use with participants from vulnerable populations. The development of the informed consent process with the active involvement of the CAN fully engaged the Marshallese community in the research and data usage process. The development and refinement of the multicomponent consent is an important example of how CBPR can be used to redress historical trauma by cocreating a consent process. CBPR principles compel the stakeholders and researchers to share the authority and responsibility over the research, from formulating the research question to designing and implementing the research study, and disseminating the research findings. Our findings support the guidelines and recommendations that research with vulnerable communities should involve consultation with the local community in the development of the consent process and materials (Fitzpatrick et al., 2016; Taitingfong et al., 2020).
Research practices that include data sharing, linking of data across multiple studies, linking medical record data, and biobanking introduce ethical concerns related to confirming truly informed consent from participants (Nishimura et al., 2013; Plough & Holm, 2016; Sheehan et al., 2019). Metaconsent practices have emerged as a possible solution to ethical issues with obtaining fully informed consent in these types of research (Plough & Holm, 2016). With metaconsent, participants have an opportunity to influence the future use of their data in various contexts by selecting the level of consent they provide (Plough & Holm, 2016). It is important to note that not all researchers embrace this approach. Sheehan et al. (2019) argued against the use of metaconsent and proposed that participants should be provided with the choice of broad consent and that future use should be determined through a research governance structure with the expertise to determine the future research (Sheehan et al., 2019). Although metaconsent is more time consuming and therefore more expensive than broad consent for researchers to keep track of individual participant's choices (Manson, 2019), it can be an important tool for increasing trust and participation among populations who have experienced historical trauma through prior research.
Best Practices
Although ethical guidelines stress the importance of upholding indigenous values of the participating community, they fail to provide specific methods for engaging communities or obtaining culturally sensitive consent (Fitzpatrick et al., 2016). Our description of the development and implementation of a multicomponent consent using a CBPR approach adds a specific example of community engagement and may be informative for other indigenous populations. The multicomponent consent design empowered participants with more nuanced control over the release of their health information. The high proportion of Marshallese participants who gave consent to all options was likely shaped by the use of bilingual (Marshallese and English) CHWs with extensive research training who conducted the informed consent process. The CHWs ensured that participants had time for discussion about the study requirements, risks, and benefits in their preferred language. Prior research has shown that time for discussion in a participant's native language is effective in improving participant understanding of the informed consent process (Al Tajir, 2018; Nishimura et al., 2013; Purvis et al., 2020, 2021). The limitations of the study include a nonrandom, small sample size from one racial group in a single geographic area. This limits the generalizability of the results. We did not capture why participants accepted or declined all or some of the data abstraction options, which limits our understanding of their considerations in the consent process. Despite these limitations, the study makes a significant contribution as the first study with Marshallese participants to implement a multicomponent consent form developed through a CBPR approach.
Research Agenda
Further work is needed to build upon our findings through exploratory research on Marshallese and Pacific Islanders' concept of collective privacy in more depth. Community-level risks related to secondary health data privacy and control are a barrier that researchers need to address in research with vulnerable and underrepresented populations. Additionally, qualitative research with Pacific Islanders is needed to understand gendered concerns related to the privacy of health data. In particular, there is a lack of understanding of Pacific Islander men's perceptions of health data privacy (Taitingfong et al., 2020). This research can potentially explain any role that sociodemographic factors may play in how participants view health data privacy (Taitingfong et al., 2020).
Educational Implications
Our findings have implications for educating research participants, review boards, and researchers. First, research participants may benefit from having bilingual study staff conduct the informed consent process about secondary data privacy and use so that participants can ask questions and provide fully informed consent to the release of their medical information. It may be helpful to provide participants with a study information sheet in their preferred language that explains what records are being released and who will have access to their records that also provides reasons they may or may not want to release their medical information. Review boards may require further education about barriers to research participation that populations like the Marshallese encounter and how alternative consent processes may help researchers overcome these challenges. Finally, there is a need to educate researchers who wish to work with underrepresented populations with specific examples and lessons learned from developing and implementing a multicomponent consent process for health data research using a CBPR approach.
Footnotes
Acknowledgments
The research reported in this publication was supported by the National Institute of General Medical Sciences of the National Institutes of Health (NIH) (#5P20GM109096). Additional support was provided by a Translational Research Institute grant from the National Center for Translational Sciences of the NIH (#1U54TR001629-01A1). The project described was also supported by the Translational Research Institute (TRI) grant (KL2 TR003108) through the National Center for Advancing Translational Sciences of the National Institute of Health (NIH). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funders. The data from this study will be publicly available in published manuscripts in PubMed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of General Medical Sciences (grant nos. 5P20GM109096, 1U54TR001629-01A1, KL2 TR003108).