
Abstract
Background:
The field of breastfeeding and lactation medicine (BFLM) is a developing area of clinical expertise among physicians and advanced practice providers, though it remains poorly described in the literature. We aimed to (1) characterize the workforce of U.S. prescribing clinicians who deliver BFLM and the clinical care they provide and (2) explore clinicians’ perceived barriers, facilitators, and attitudes related to BFLM care.
Methods:
We performed a descriptive, cross-sectional study of U.S. clinicians who self-identify as BFLM clinicians. Inclusion was limited to medical clinicians who (1) hold a license to prescribe medication (physicians, advanced practice providers) and (2) independently diagnose and manage breastfeeding-related concerns or complications.
Results:
Our sample of 138 U.S. clinicians had a median of 8 years of BFLM clinical experience and included physicians (81%), nurse practitioners (13.0%), midwives (3.6%), and physician assistants (2.2%). Among clinicians within large healthcare organizations, 20% held BFLM-related positions/titles. Of clinicians who delivered dedicated outpatient BFLM care, 64.5% offered telehealth, 67.4% billed for mother and infant, and 43% offered outpatient frenotomy. A median wait time of 5 days for initial BFLM outpatient evaluation was reported. Few participants provided inpatient and electronic consultation services (i.e., “e-consult”) dedicated to BFLM. Most agreed that BFLM care addresses critical gaps in U.S. healthcare (95%).
Conclusions:
We present the first description of a national sample of U.S. prescribing clinicians who practice BFLM. These findings may assist clinicians and organizations in implementing BFLM care and underscore a need for future research around the integration and impact of BFLM care within U.S. health systems.
Keywords
Introduction
Despite 83% of families initiating breastfeeding in the United States, only 25% exclusively breastfeed through 6 months postpartum, the duration of exclusivity widely recommended to optimize maternal and infant health benefits. 1 This attrition in part reflects the failure of U.S. healthcare systems to consistently provide evidence-based breastfeeding support as a standard of care, including a lack of in-depth counseling on infant feeding during routine prenatal care, inconsistent breastfeeding messaging from healthcare staff, poor insurance reimbursement for lactation support services, and insufficient clinician knowledge, training, and time to appropriately diagnose and manage breastfeeding complications.2–5 As a result of this knowledge gap, many clinicians rely on their personal infant feeding experiences to guide care, which although valuable, is often anecdotal, not evidence-based, and potentially biased.6,7 With over 3.6 million infants born within the US each year, 83% of whom are breastfed after delivery, clinicians who care for pregnant individuals and their infants should be prepared to diagnose and manage breastfeeding concerns and complications. 1 Nonetheless, prescribing clinicians report relying on other healthcare staff to deliver breastfeeding care to their patients, many of whom lack formal clinical training on the diagnosis and management of medical conditions related to breastfeeding and lactation. 4 Ultimately, discontinuity of messaging and gaps in breastfeeding care result. 4
Recognizing marked gaps in access to breastfeeding and lactation clinical expertise within U.S. health systems, a growing number of clinicians pursue advanced clinical training in breastfeeding and lactation medicine (BFLM) to independently diagnose and manage breastfeeding concerns and complications. Although many incorporate this BFLM expertise into routine care, other clinicians practice in dedicated BFLM clinics. Across the United States, clinicians increasingly seek guidance on the establishment of clinics and consultation services dedicated to BFLM specialty care, as evidenced by expanding professional societies and online communities for BFLM clinicians.8–11 Despite this expansion over recent decades, the BFLM professional workforce and the clinical care they provide are poorly understood, and limited data exist to help define the field and support future integration of BFLM into standard healthcare delivery. Given the unique characteristics of the U.S. health system, we aimed to characterize the BFLM workforce and clinical practice in the United States, specifically, including clinician training, responsibilities, and clinical care processes, and to explore clinicians' perceived barriers, facilitators, and attitudes regarding BFLM care delivery.
Methods
Study sample and design
In this cross-sectional study, we invited clinicians who deliver BFLM care to complete a 15-minute online survey available only in English. To be eligible, participants had to be practicing clinicians with a license to prescribe medication and independently diagnose and manage breastfeeding-related medical problems among parents and/or children in their clinical practice (either within a dedicated BFLM practice setting, or as BFLM-specific appointments in the course of another routine medical practice, e.g., primary care pediatrics). Within the United States, such clinicians include nurse practitioners, certified nurse midwives, physician assistants (often collectively referred to as advanced practice providers), physicians, and dentists. Those who were not eligible for this study included lactation consultants or specialists without a license to prescribe medication (e.g., a registered nurse/International Board Certified Lactation Consultant [IBCLC]), students or trainees who do not independently practice medicine, and retired clinicians who no longer practice medicine.
Participants were included in our analytic sample if they practiced within the United States and answered ≥50% of the eligible survey questions, a cutoff selected to optimize our description of clinician demographics, training, responsibilities, and care settings, as these questions were at the start of the survey. Data collection from BFLM clinicians outside of the United States, including a Spanish-language version of the survey, is ongoing and will be presented in a separate article.
Our survey was designed by five BFLM physicians (D.N., C.R.C., M.C.C., M.H.A., and K.S.) from five different institutions and two medical specialties, family medicine and pediatrics (Supplementary Data). To examine content validity, readability, and length of the survey, we piloted the survey with five additional BF clinicians (a midwife, nurse practitioners, and physicians) from different institutions, states, and private and public health systems.
The Yale Institutional Review Board deemed the study exempt from review. Informed consent was included at the start of the survey. The survey was disseminated using Qualtrics (Copyright 2020, Utah, USA).
Recruitment
The survey was distributed via several professional platforms likely to have BFLM clinician membership, including the Academy of Breastfeeding Medicine (ABM) annual conference and member online community, the American Academy of Pediatrics Section on Breastfeeding listserv, the Institute for the Advancement of Breastfeeding and Lactation Education (IABLE) listserv, the Lessons in Lactation Advanced Curriculum (LILAC) fellowship program, the American College of Nurse Midwives Breastfeeding and Lactation Subcommittee, and two BFLM-focused Facebook groups for nurse practitioners and physicians. The study invitation was posted 2–3 times across all platforms between November 2024 and February 2025. Snowball sampling was used, as participants were encouraged to share the survey with BFLM colleagues. Participation was voluntary, and the participants did not receive compensation. The answers were anonymized.
Measures
To capture participants' demographic and professional backgrounds, as well as their BFLM clinical training and responsibilities, we asked their age, years in practice, gender, race and ethnicity, credentials (e.g., IBCLC, medical degree, specialty), state of medical practice, professional title(s), BFLM clinical training, and responsibilities related to BFLM.
To describe clinical care processes, we first asked about practice setting (i.e., academic, public, government, or private health system; urbanicity of clinic setting and patients served) and type of BFLM care delivered: (1) as part of routine specialty-specific medical practice (e.g., BFLM care as part of a routine newborn appointment), (2) within a dedicated BFLM clinic where patients are referred for BFLM concerns, and (3) dedicated BFLM inpatient and/or electronic consultation services. Those who reported practicing the second and/or third of these BFLM care options were asked additional questions about the clinical care process of these respective BFLM clinical services, such as patient volume, wait time, staffing, coding/billing, and procedures.
To explore barriers and facilitators, the survey provided six possible factors (i.e., leadership support; billing and compensation; available trained clinicians; financial support to hire staff; space and supplies; clinical workflow and logistics) and asked participants to select if each factor was a barrier and/or facilitator to the development and management of their BFLM practice. Finally, to explore participant attitudes around BFLM care delivery, they were asked to report how strongly they agreed/disagreed (5-point Likert scale) with six statements related to health system culture and capacity, if the care they provide addresses critical gaps in standard health care, and future directions of the BFLM field.
Analytic approach
Descriptive summary statistics such as mean (standard deviation), median (25th, 75th percentiles, range), and count (n, percentage %) were used to summarize responses across questions. Since questions on clinical care processes appeared based on participants’ BFLM practice setting and type, response rates varied for each question (included in all tables). All data were analyzed in STATA 17.0 (StataCorp LLC, Copyright 2021 Texas, USA). The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were used to structure the presentation of our results. 12
Results
A total of 174 participants responded to the survey. We excluded 14 participants for missing or “no” responses regarding providing BFLM care, and 22 for having responded to <50% of eligible questions, resulting in a final sample of 138 participants. Among included participants, 90% responded to ≥80% of questions (71% responded to all questions). A response rate for our overall survey was unable to be determined as the number of BFLM clinicians within all platforms used for recruitment is unknown (many members are nonclinicians and/or clinicians who do not practice BFLM), hence the aim of our study.
Demographics, training, and responsibilities
Participants practiced within 38 U.S. states and the District of Columbia (Table 1). They were physicians (81.2%), nurse practitioners (13.0%), midwives (3.6%), and physician assistants (2.2%), most often trained in either general pediatrics (45.7%) or family medicine (31.2%). Most respondents identified as women (97.8%), had a median age of 45 years (25th, 75th percentiles: 38.0, 54.5), and identified as non-Hispanic White (81.2%). Participants reported a median of 8.0 years practicing BFLM (range: 0.0–50.0) and 11.0 years practicing medicine broadly (1.0–51.0), largely working within academic or university-affiliated health systems (42.0%) or private practice (34.8%).
Characteristics of 138 Prescribing Clinicians a Who Deliver Breastfeeding and Lactation Medicine Care in the United States in 2024–2025
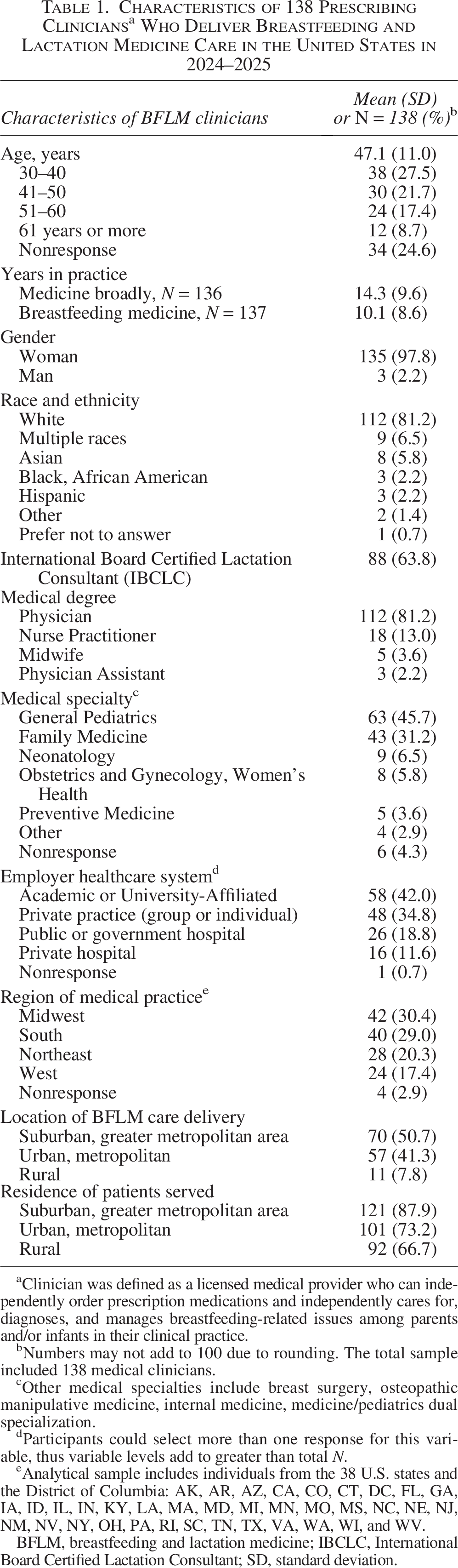
Clinician was defined as a licensed medical provider who can independently order prescription medications and independently cares for, diagnoses, and manages breastfeeding-related issues among parents and/or infants in their clinical practice.
Numbers may not add to 100 due to rounding. The total sample included 138 medical clinicians.
Other medical specialties include breast surgery, osteopathic manipulative medicine, internal medicine, medicine/pediatrics dual specialization.
Participants could select more than one response for this variable, thus variable levels add to greater than total N.
Analytical sample includes individuals from the 38 U.S. states and the District of Columbia: AK, AR, AZ, CA, CO, CT, DC, FL, GA, IA, ID, IL, IN, KY, LA, MA, MD, MI, MN, MO, MS, NC, NE, NJ, NM, NV, NY, OH, PA, RI, SC, TN, TX, VA, WA, WI, and WV.
BFLM, breastfeeding and lactation medicine; IBCLC, International Board Certified Lactation Consultant; SD, standard deviation.
Sixteen percent of participants owned their practice (Table 2). Among those who worked within larger healthcare organizations (79.0%), 20.3% had a BFLM-related position/title, which they were most often the first to hold (78.6%) and for which most had paid, protected time for nonclinical duties (78.6%). For BFLM clinical training, most participants were International Board Certified Lactation Consultants (63.8%, IBCLC) and had completed clinician-level training in BFLM offered through ABM, IABLE, and/or LILAC (75.4%). BFLM professional duties most often included outpatient BFLM care (73.9%), education of healthcare staff and trainees (63.0%), administrative duties (46.4%), and community engagement and advocacy (43.5%).
Professional Titles, Training, and Responsibilities (Clinical and Nonclinical) of 138 Breastfeeding and Lactation Medicine (BFLM) Prescribing Clinicians in the United States from 2024 to 2025
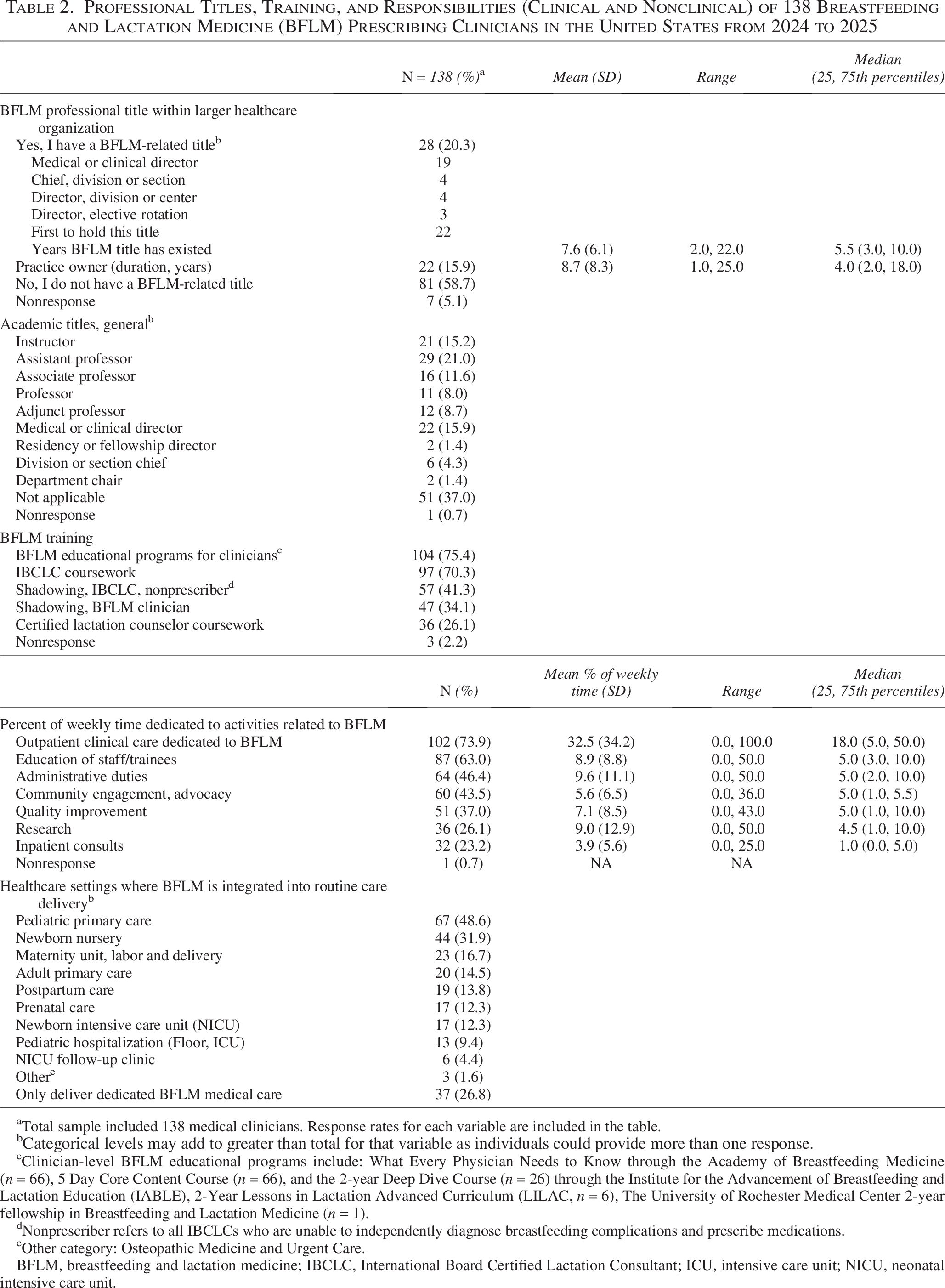
Total sample included 138 medical clinicians. Response rates for each variable are included in the table.
Categorical levels may add to greater than total for that variable as individuals could provide more than one response.
Clinician-level BFLM educational programs include: What Every Physician Needs to Know through the Academy of Breastfeeding Medicine (n = 66), 5 Day Core Content Course (n = 66), and the 2-year Deep Dive Course (n = 26) through the Institute for the Advancement of Breastfeeding and Lactation Education (IABLE), 2-Year Lessons in Lactation Advanced Curriculum (LILAC, n = 6), The University of Rochester Medical Center 2-year fellowship in Breastfeeding and Lactation Medicine (n = 1).
Nonprescriber refers to all IBCLCs who are unable to independently diagnose breastfeeding complications and prescribe medications.
Other category: Osteopathic Medicine and Urgent Care.
BFLM, breastfeeding and lactation medicine; IBCLC, International Board Certified Lactation Consultant; ICU, intensive care unit; NICU, neonatal intensive care unit.
Clinical care processes
Most participants (73.2%) reported integrating their BFLM expertise into routine specialty-specific medical care, most often within pediatric primary care (48.6%) and the newborn nursery (31.9%, Table 2).
Dedicated BFLM outpatient care
Nearly two-thirds (64.5%) of participants delivered dedicated BFLM outpatient care, 24.7% of whom were private practice owners (n = 22; 14 physicians, 5 nurse practitioners, 2 midwives, and 1 physician assistant, Table 3). Most delivered BFLM care within academic or university-affiliated clinics (38.8%) or private practices (38.8%), and two-thirds (66.3%) used telehealth for an average of 15.0% of total weekly visits. The median wait time for outpatient BFLM evaluation was 5 days (interquartile range: 3.0, 10.0; range 0.0–36.0). Initial outpatient visits were most often scheduled ≤1 month postpartum for a duration of 60 minutes. Top indications for referral were low milk production, latch difficulties, nipple/breast pain, infant slow weight gain, and ankyloglossia. During outpatient evaluation, screenings for depression (70.8%) and high blood pressure (55.1%) were most often performed. After outpatient evaluation, BFLM clinicians most commonly referred patients to behavioral health support (46.1%). Participants reported an average of 2.8 full-time equivalent staff (SD 3.2, range 0–18) within their dedicated BFLM clinics, often with a single prescribing clinician (93.5% of whom were physicians), a single nonprescribing staff member credentialed as an IBCLC (75.0% nurses), and a single nonprescribing staff who was not an IBCLC (29.6% administrative, 22.2% nurses, 20.4% medical assistants, or 18.5% certified lactation counselors). Our Figure 1 illustrates key BFLM outpatient clinical care process measures as reported by participants within our analytic sample.
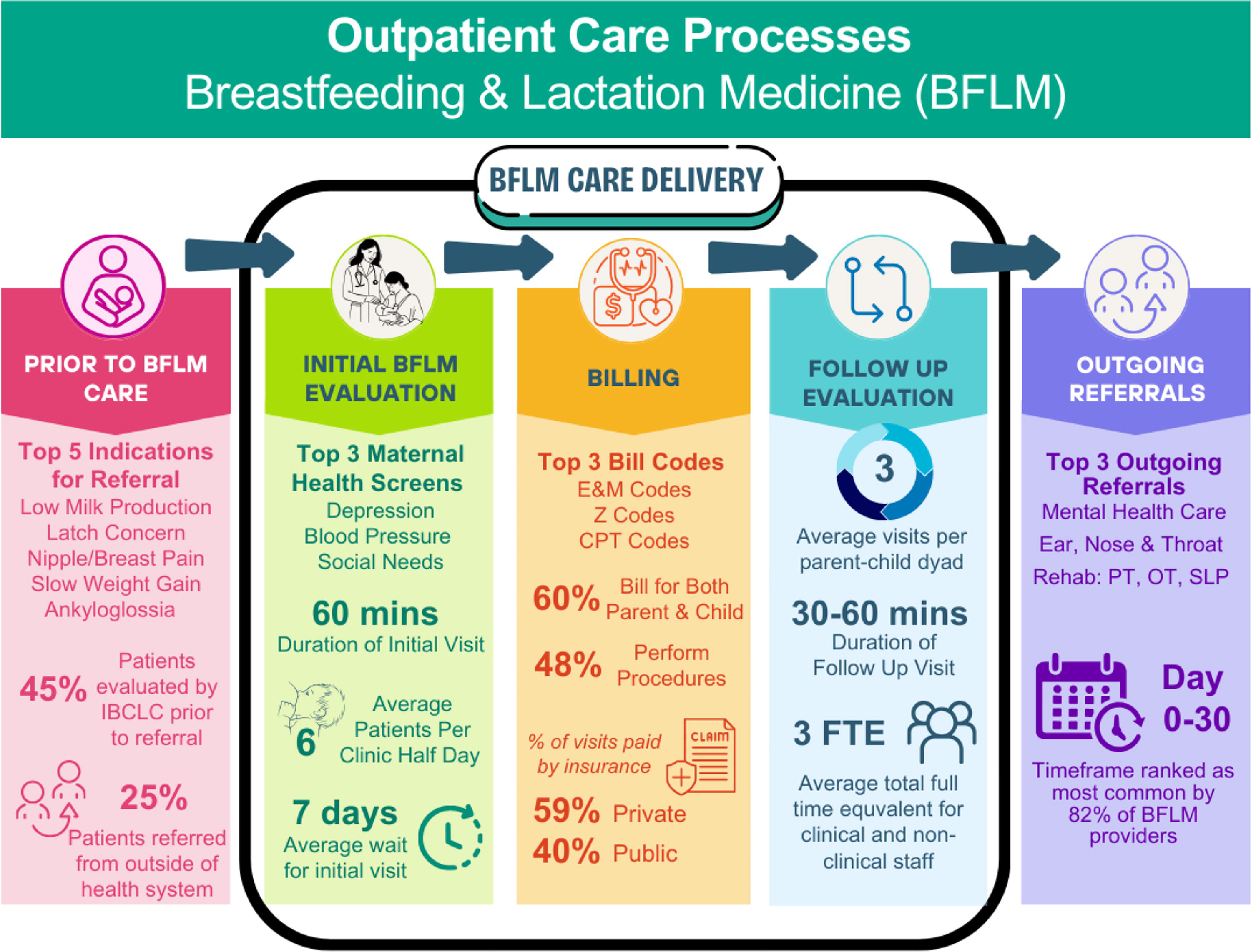
Infographic depicting key clinical care process measures based on survey responses from 89 clinicians who delivered outpatient care dedicated to breastfeeding and lactation medicine in the United States from 2024 to 2025.
Characteristics of Clinical Care Provided Within Dedicated Breastfeeding and Lactation Medicine (BFLM) Clinics in the United States
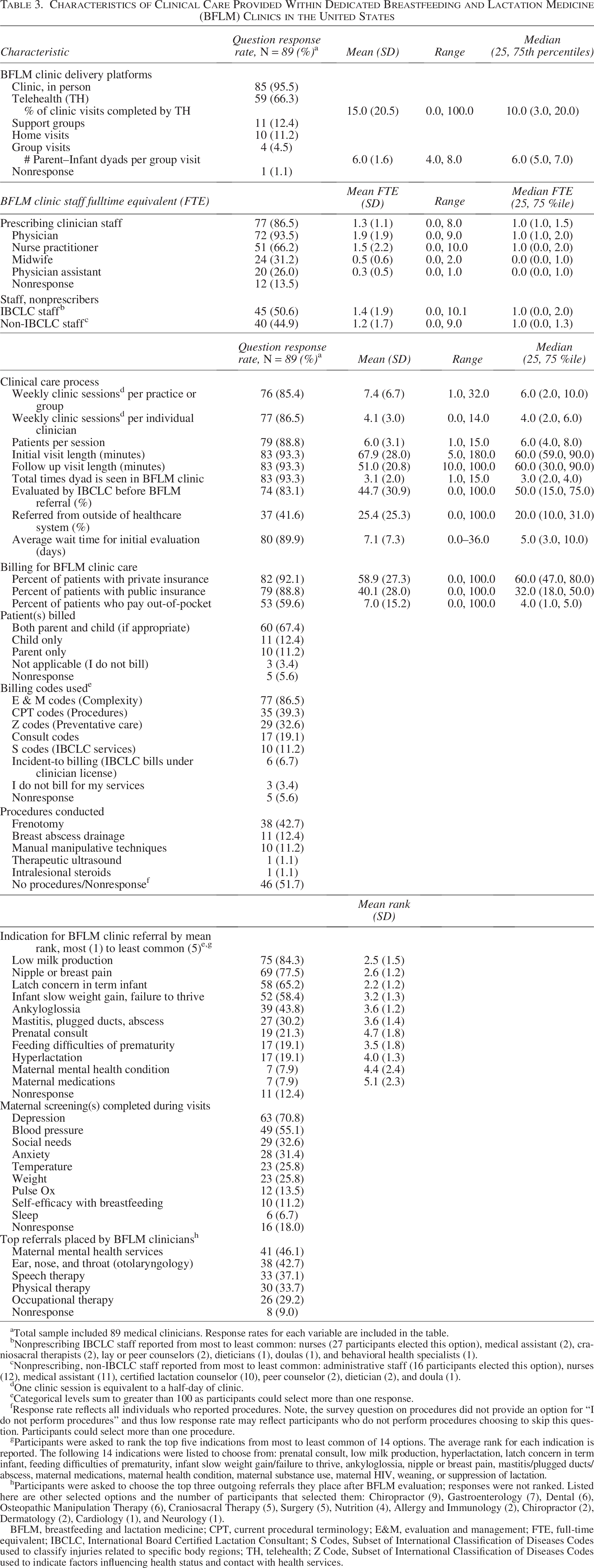
Total sample included 89 medical clinicians. Response rates for each variable are included in the table.
Nonprescribing IBCLC staff reported from most to least common: nurses (27 participants elected this option), medical assistant (2), craniosacral therapists (2), lay or peer counselors (2), dieticians (1), doulas (1), and behavioral health specialists (1).
Nonprescribing, non-IBCLC staff reported from most to least common: administrative staff (16 participants elected this option), nurses (12), medical assistant (11), certified lactation counselor (10), peer counselor (2), dietician (2), and doula (1).
One clinic session is equivalent to a half-day of clinic.
Categorical levels sum to greater than 100 as participants could select more than one response.
Response rate reflects all individuals who reported procedures. Note, the survey question on procedures did not provide an option for “I do not perform procedures” and thus low response rate may reflect participants who do not perform procedures choosing to skip this question. Participants could select more than one procedure.
Participants were asked to rank the top five indications from most to least common of 14 options. The average rank for each indication is reported. The following 14 indications were listed to choose from: prenatal consult, low milk production, hyperlactation, latch concern in term infant, feeding difficulties of prematurity, infant slow weight gain/failure to thrive, ankyloglossia, nipple or breast pain, mastitis/plugged ducts/abscess, maternal medications, maternal health condition, maternal substance use, maternal HIV, weaning, or suppression of lactation.
Participants were asked to choose the top three outgoing referrals they place after BFLM evaluation; responses were not ranked. Listed here are other selected options and the number of participants that selected them: Chiropractor (9), Gastroenterology (7), Dental (6), Osteopathic Manipulation Therapy (6), Craniosacral Therapy (5), Surgery (5), Nutrition (4), Allergy and Immunology (2), Chiropractor (2), Dermatology (2), Cardiology (1), and Neurology (1).
BFLM, breastfeeding and lactation medicine; CPT, current procedural terminology; E&M, evaluation and management; FTE, full-time equivalent; IBCLC, International Board Certified Lactation Consultant; S Codes, Subset of International Classification of Diseases Codes used to classify injuries related to specific body regions; TH, telehealth; Z Code, Subset of International Classification of Diseases Codes used to indicate factors influencing health status and contact with health services.
Inpatient and electronic BFLM consultation
Although 20 participants provided BFLM consultation for hospitalized patients, only 9 worked within formal inpatient BFLM consultation services, of whom 8 provided responses to eligible survey questions (Table 4). Other respondents likely provided informal “curbside” consultations or recommendations to colleagues (n = 7) or had missing data (n = 4). Participants reported an average of six new BFLM consultations per week (SD 6.8, range 1.0–20.0) to which most responded within 12–24 hours. Consult codes were most often used to bill for these services. Common referral indications were similar to those reported for outpatient clinic referral but also included infant feeding difficulties of prematurity and ankyloglossia, maternal medications and medical problems, HIV, and substance use disorder.
Characteristics of Inpatient and Electronic Breastfeeding and Lactation Consult Services Delivered Within U.S. Health Systems
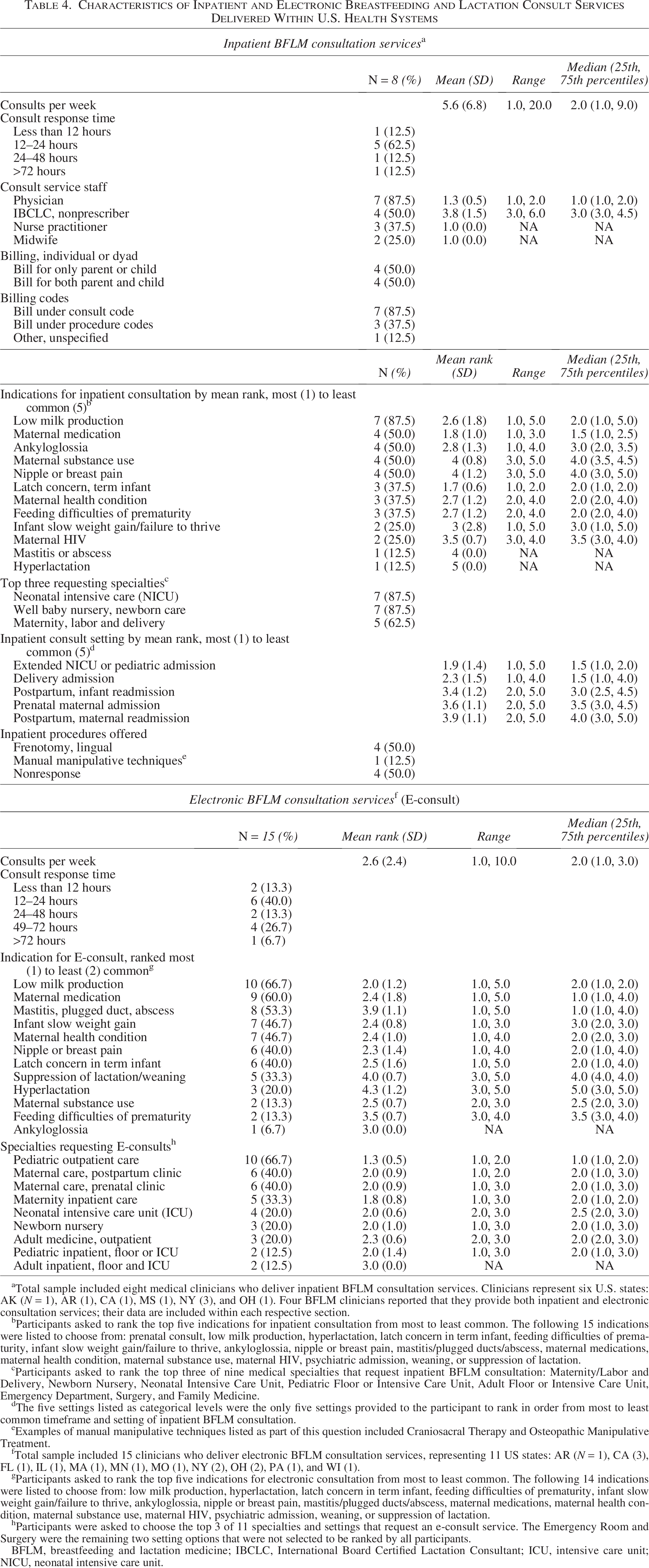
Total sample included eight medical clinicians who deliver inpatient BFLM consultation services. Clinicians represent six U.S. states: AK (N = 1), AR (1), CA (1), MS (1), NY (3), and OH (1). Four BFLM clinicians reported that they provide both inpatient and electronic consultation services; their data are included within each respective section.
Participants asked to rank the top five indications for inpatient consultation from most to least common. The following 15 indications were listed to choose from: prenatal consult, low milk production, hyperlactation, latch concern in term infant, feeding difficulties of prematurity, infant slow weight gain/failure to thrive, ankyloglossia, nipple or breast pain, mastitis/plugged ducts/abscess, maternal medications, maternal health condition, maternal substance use, maternal HIV, psychiatric admission, weaning, or suppression of lactation.
Participants asked to rank the top three of nine medical specialties that request inpatient BFLM consultation: Maternity/Labor and Delivery, Newborn Nursery, Neonatal Intensive Care Unit, Pediatric Floor or Intensive Care Unit, Adult Floor or Intensive Care Unit, Emergency Department, Surgery, and Family Medicine.
The five settings listed as categorical levels were the only five settings provided to the participant to rank in order from most to least common timeframe and setting of inpatient BFLM consultation.
Examples of manual manipulative techniques listed as part of this question included Craniosacral Therapy and Osteopathic Manipulative Treatment.
Total sample included 15 clinicians who deliver electronic BFLM consultation services, representing 11 US states: AR (N = 1), CA (3), FL (1), IL (1), MA (1), MN (1), MO (1), NY (2), OH (2), PA (1), and WI (1).
Participants asked to rank the top five indications for electronic consultation from most to least common. The following 14 indications were listed to choose from: low milk production, hyperlactation, latch concern in term infant, feeding difficulties of prematurity, infant slow weight gain/failure to thrive, ankyloglossia, nipple or breast pain, mastitis/plugged ducts/abscess, maternal medications, maternal health condition, maternal substance use, maternal HIV, psychiatric admission, weaning, or suppression of lactation.
Participants were asked to choose the top 3 of 11 specialties and settings that request an e-consult service. The Emergency Room and Surgery were the remaining two setting options that were not selected to be ranked by all participants.
BFLM, breastfeeding and lactation medicine; IBCLC, International Board Certified Lactation Consultant; ICU, intensive care unit; NICU, neonatal intensive care unit.
Fifteen participants from 11 states delivered BFLM electronic consultation services (“e-consults”), reporting an average of three new consults per week (SD 2.4, range 1.0–10.0) to which most responded in 12–24 hours. E-consult was most often requested from pediatric primary care and postpartum maternal clinics. The top three e-consult indications were (1) low milk production, (2) maternal medication concerns, and (3) mastitis or abscess.
Barriers, facilitators, and attitudes of BFLM care delivery
Ninety-seven participants reported on barriers, facilitators, and attitudes regarding BFLM care delivery. Financial support to hire staff was the most common barrier (77.3%); support from leadership was the most frequently reported facilitator (48.5%) but was also often reported as a barrier (51.5%) (Table 5). Regarding perceptions and attitudes of the field, 94.8% of participants felt that BFLM care addresses a critical gap in standard health care, wanted to see the field expand (98.5%), and believed further research on the diagnosis and management of breastfeeding/lactation conditions is needed to improve patient outcomes (93.8%) (Supplementary Table S1). Over 40% of participants (42.3%) disagreed with the statement “My healthcare practice or organization is able to provide BFLM clinical care to all families in need of these services.”
Perceived Barriers to and Facilitators of the Development and Management of Breastfeeding and Lactation Medicine Clinical Care Within U.S. Health Systems from 97 Medical Clinicians a
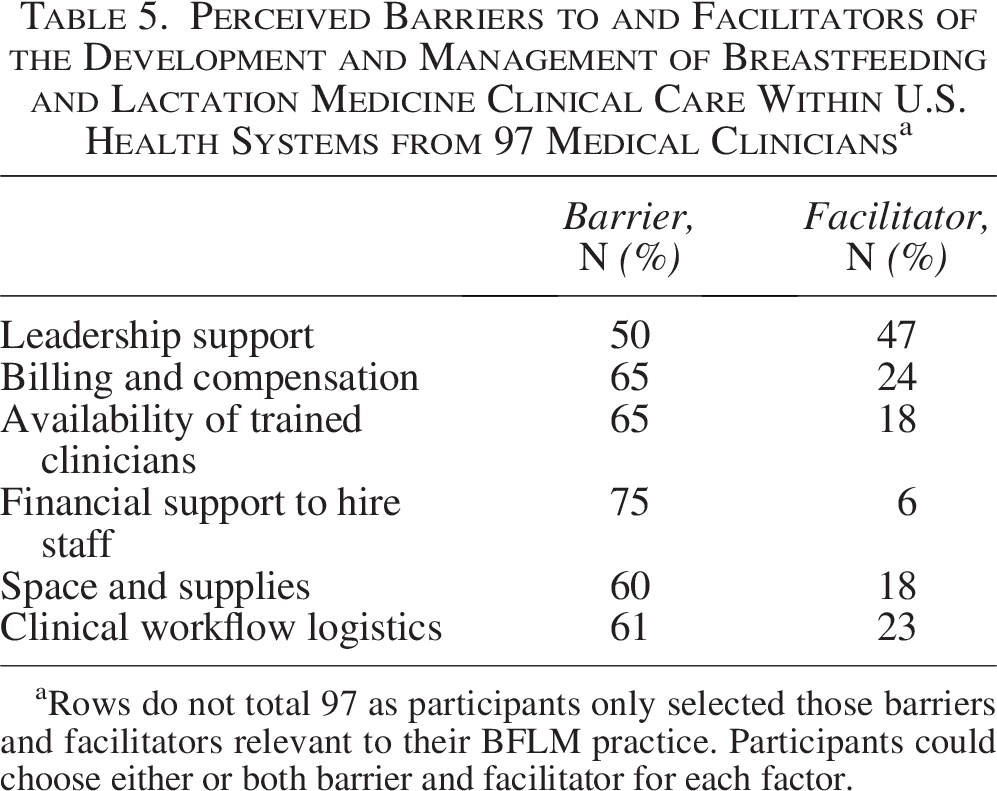
Rows do not total 97 as participants only selected those barriers and facilitators relevant to their BFLM practice. Participants could choose either or both barrier and facilitator for each factor.
Discussion
We present the first description of the training, responsibilities, and clinical care processes of prescribing clinicians who deliver BFLM care within the United States. Although the largest share were pediatric or family physicians delivering care in outpatient pediatric clinics or newborn nurseries, nearly one-fifth of participants were nurse practitioners, midwives, and physician assistants, highlighting their important contribution to the BFLM workforce. Clinicians largely obtained advanced training in BFLM through IBCLC certification and completion of clinician-level BFLM training programs. Institutional leadership support was nearly equally reported as a barrier and facilitator to the development and management of BFLM services, and over 40% of participants felt their health system or practice was unable to provide BFLM clinical care to all families in need of these services. Nearly all participants felt that the BFLM care they provide addresses a critical gap in standard models of U.S. healthcare delivery.
Two prior observational studies described small samples of BFLM physician leaders. Shaikh and Smillie surveyed lead physicians from 13 U.S. breastfeeding and lactation clinics in both private and academic settings, six of which were solo private practices, and most (n = 7) were led by pediatricians. 13 Ten of 13 clinics delivered specialized BFLM care in addition to standard pediatric or adult primary care. As in our study, most clinics (10 of 13) were affiliated with teaching hospitals in which clinicians treated an average of 6 mother–infant dyads (pairs) per 4-hour clinic session, booked 45-to-60-minute initial visits, billed for mother and child (54%), and reported similar referral indications (low milk supply, nipple pain, and infant latch). In 2017, Rosen-Carole surveyed medical directors of breastfeeding services in academic settings; of 32 respondents, 25 practiced in the United States. 14 Most BFLM positions (75%) had been created within the last 10 years (one-third under 2 years) and were housed within the Departments of Pediatrics (75%). Similar to our findings, the most common BFLM professional responsibilities were outpatient clinical care and staff/trainee education, with 56% of clinicians delivering BFLM care within university-affiliated clinics. Our study adds to these data by including a larger sample and expanded representation across clinical disciplines (physicians and advanced practice providers), roles (those with and without leadership roles), and settings (academic and nonacademic).
Our findings suggest expansion of the BFLM workforce and practice over the last decade, as evidenced by clinicians’ median 8 years of BFLM clinical experience and most being the first to hold their BFLM-related position/title. However, like earlier studies, professional recognition of clinician BFLM expertise and clinical and nonclinical contributions remains low. Rosen-Carole found that despite 25 of the 32 surveyed academic BFLM medical directors having a formal job description, 69% were not paid for their BFLM-related work. 14 Only one-fifth of our sample reported a BFLM-related position/title despite half or more carrying out important BFLM administrative duties, teaching, and outpatient care delivery. Moreover, leadership support was nearly equally reported as a barrier to and facilitator of BFLM clinical care. Our findings underscore the critical role of institutional support for the development and management of BFLM clinical services, including the recognition of the nonclinical duties required to sustain this specialized care.13,14
Some of our participants were consulted to provide clinical recommendations for patients with medically complex peripartum courses, including maternal substance use disorder, HIV, other medical conditions and/or medications, and infant prematurity. As such, the demand for BFLM clinical expertise is likely to rise across healthcare settings amidst increasing rates of maternal diabetes, 15 obesity, 16 hypertension, 17 and substance use disorders, 18 as well as infant prematurity, 19 all conditions known to complicate the establishment and maintenance of lactation.20–24 In addition, participants most often evaluated patients within the first month postpartum, and more than half screened for two leading causes of postpartum maternal morbidity and mortality, depression, and hypertension. 25 Given known difficulties with postpartum healthcare engagement, BFLM clinicians may be well-positioned to expand access to valuable maternal health screenings by taking a dyadic approach to care. 26 BFLM care also has the potential to advance health equity, as U.S. populations at the highest risk for cardiometabolic comorbidities also experience the highest risk of early breastfeeding cessation (and thus the lowest exposure to the cardioprotective benefits of breastfeeding).27–29
Although most participants offered telehealth, a platform to improve care access, barriers to accessing timely breastfeeding care were nonetheless observed. Many participants reported that their practice/organization could not meet community BFLM care needs. Few clinics were located within rural settings, and an average 1-week wait time was reported across participants (and as long as 36 days). Lack of access to breastfeeding care disproportionately impacts rural and/or low-income communities.30–32 Reported indications for referral, including low supply, pain, latch, and infant weight concerns, often require rapid 24–48 hour assessment to treat the underlying concern and sustain breastfeeding. Wait times observed in our study could result in breastfeeding cessation for many individuals, underscoring the growing need for systemic economic investment and policy reform to support the expansion of BFLM services in the United States. In 2025, the U.S. Preventive Services Task Force (USPSTF) called for research to examine clinic-based breastfeeding interventions for populations experiencing heightened challenges with breastfeeding, including those living with low-income and/or rural residence. 33 As such, studies are needed to examine how care provided by existing, financially sustainable BFLM clinics impact timely (i.e., short clinic wait times) and equitable (i.e., accepting patients with public insurance27,34) access to breastfeeding care, as well as how this care influences key patient outcomes (e.g., breastfeeding exclusivity and duration; maternal health, satisfaction, and well-being). Such studies should characterize how existing evidence-based models of outpatient breastfeeding support, including but not limited to care from peer counselors 35 and lactation consultants, 36 should be integrated alongside or within BFLM clinics to accurately identify and efficiently treat issues related to breastfeeding and lactation using cost-effective care.
Less than 5% of participants self-identified as Black or Hispanic race and ethnicity, despite collectively representing approximately 35% of the U.S. population. 37 All but three of 138 clinicians self-identified as women, illuminating a clear need for more gender diversity within the field. Understanding that racial, cultural, and linguistic concordance between clinicians and patients positively influences patient satisfaction with care, promotes trust, and enhances communication,38,39 we suggest that continued efforts to diversify the BFLM workforce are likely to improve care delivery. Payers should incentivize the integration of evidence-based, culturally aligned breastfeeding care into health systems, including peer counselors. 35 In addition, increasing representation among BFLM clinicians to include individuals from communities with historically lower breastfeeding rates 27 and/or who are underrepresented within the broader clinician workforce 40 is recommended. Health systems and professional organizations should invest in programs to recruit, train, and mentor individuals with diverse backgrounds who are interested in BFLM training, offering financial sponsorship to minimize cost as a barrier to entry.
Limitations
Limitations of this study include the inability to determine a response rate due to the lack of prior description or enumeration of the population of BFLM clinicians, nor data around number of existing BFLM clinicians within the groups targeted for recruitment. This limitation was part of the rationale for the study to describe the size and characteristics of this emerging field. Recruitment through these communities may have led to selection bias and underrepresentation of clinicians and/or specialties who do not belong to the professional societies and online communities targeted by our recruitment efforts. Due to overlapping membership among the recruitment platforms, repeat responses are possible. However, to mitigate this risk, participants were reminded that the survey was cross posted. Given the survey’s length and unique focus, we anticipate that participants would not have repeated the survey within the 3-month period during which it was advertised. The decision to recruit from specific listservs and organizations was intentional, as BFLM remains poorly understood by medical professionals outside of the field, and thus widespread recruitment could have increased the risk for inaccurate or inappropriate responses and miscategorization of ineligible participants. Lastly, we designed this study to capture clinician-level data, and thus our descriptions of care access may be biased by the possibility that single health systems may be represented by several employee participants.
Conclusion
We present the first description of the clinical and nonclinical professional duties of U.S. prescribing clinicians who practice BFLM, or clinical care dedicated to the diagnosis and management of breastfeeding and lactation concerns or complications. Although most U.S. BFLM clinicians were physicians trained in general pediatrics or family medicine, nearly one fifth of the BFLM clinician workforce were advanced practice providers, highlighting their important role in BFLM care delivery. Nearly all clinicians agreed that the BFLM care they provide addresses a critical gap in standard U.S. healthcare and reported wanting to see the field of BFLM expand in years to come. Aligned with 2025 USPSTF recommendations, future studies should evaluate the impact of outpatient BFLM care on breastfeeding care access and outcomes, in particular for communities with higher barriers to care and lower breastfeeding rates.
Authors’ Contributions
D.N.: Conceptualization (lead), investigation (co-lead), methodology, data curation and formal analysis (lead), funding acquisition, project administration, software, writing—original draft (lead), and review and editing (lead). C.R.C.: Conceptualization, methodology, and writing—review and editing. M.C.C.: Conceptualization, methodology, writing—review and editing. M.H.A.: Conceptualization, methodology, and writing—review and editing. M.Y.: Writing—review and editing. E.S.R.: Writing—review and editing. M.S.: Visualization and writing—review and editing. V.S.: Methodology, visualization, and writing—review and editing. K.S.: Conceptualization, investigation (co-lead), methodology, supervision (lead), and writing—review and editing.
Footnotes
Acknowledgments
The authors would like to acknowledge all participants who completed this survey and shared their experiences and attitudes regarding the field of BFLM.
Funding Information
This research is supported by the Yale Department of Pediatrics and the Yale Pediatric Scholars Award (DN).
Disclosure Statement
The authors of this article have no financial disclosures to report.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.