
Abstract
Background:
Lactation care providers (LCPs) are vital in supporting breastfeeding mothers. However, research on the emotional aspects of their work remains limited. This study investigated mothers’ and LCPs’ perceptions of the emotional aspects of lactation care and whether they differed by background characteristics and LCPs qualifications.
Methods:
Following phone calls or written correspondence, 149 LCPs (43.6% International Board-Certified Lactation Consultants [IBCLCs], 29.5% Registered Nurses Lactation Consultants [RNLCs], and 26.8% Lactation Educators [LEs]) and 201 mothers completed an identical 10-item online quantitative questionnaire assessing expectations of emotional support in lactation care and perceptions of providers’ competence and training adequacy in this domain. Mothers reported the duration of lactation care received.
Results:
LCPs perceived emotional support as part of their role but hesitated to engage in this domain. Confidence in providing emotional support was higher among RNLCs compared to IBCLCs and LEs. Mothers expected emotional support from their LCPs but questioned whether they were adequately trained. Mothers assisted by IBCLCs perceived them as significantly more capable of providing emotional support than those assisted by RNLC or LEs. A longer lactation care duration was associated with mothers’ positive perceptions of emotional support in lactation care.
Conclusion:
LCPs and mothers perceive emotional support as an important aspect of lactation care. However, they reported challenges in delivering and engaging in this aspect. These findings underscore the need to incorporate structured training in emotional support into the education and professional development of LCPs.
Introduction
Breastfeeding is the optimal form of infant nutrition, offering significant health benefits for both the child and the mother.1–3 Despite the well-documented health benefits of breastfeeding, only 48% of infants under 6 months of age are exclusively breastfed globally, across high-, middle-, and low-income countries. 4 Some of the most common reasons for early breastfeeding cessation are perceived inadequate milk supply, maternal breast or nipple pain, and lack of support and education.5,6
Lactation care emerged in response to the multifaceted challenges breastfeeding women face.7–9 Numerous studies have demonstrated that lactation care providers (LCPs) improve breastfeeding outcomes, including duration and exclusivity, as well as maternal self-efficacy, which in turn positively influences breastfeeding success and duration.10–12
Alongside maternal self-efficacy,13,14 other emotional factors, such as negative emotions during breastfeeding, may hamper breastfeeding success. For example, mothers who experience less positive emotions while breastfeeding at 2 months postpartum are less likely to breastfeed exclusively by 6 months postpartum, 15 and women experiencing postpartum anxiety are less likely to breastfeed exclusively and more likely to terminate breastfeeding earlier. 16 This raises a key question: To what extent should providing emotional support to mothers postpartum be part of LCPs’ professional responsibilities? This question is important given that in many high-income countries, LCPs often play a prominent role in early postpartum care and may be among the first professionals mothers encounter after birth.11,12 However, this issue has received little attention.
A handful of studies have examined the impact of lactation care on mothers’ emotional well-being, focusing on mothers with mental health conditions, such as postpartum depression.17,18 One of these studies demonstrated that interventions by midwives trained in breastfeeding support improved mothers’ postpartum mental health. 17 Another study indicated that registered nurses, lactation care providers (RNLCs), believed they could play a significant role in identifying and treating women with postpartum-related mental health issues. 18
However, emotional support provided by LCPs to mothers without mental health conditions remains understudied. These mothers may face emotional challenges such as fatigue, mood changes, anxiety symptoms, guilt, and shame related to their breastfeeding experiences.19,20 A recent study suggested that the quality of support mothers receive from their LCPs is associated with their emotional well-being and breastfeeding outcomes. Mothers who perceived the support they received from their LCPs less positively reported lower breastfeeding self-efficacy, less successful breastfeeding experiences, more significant anxiety symptoms, and shorter total duration of milk production. 21 Yet, this study assessed mothers’ overall perceptions of LCPs’ support, without specifically examining mothers’ views on its emotional component.
An additional question is whether the type of training that LCPs receive influences the importance they attribute to emotional support and their ability to provide it effectively to mothers. Most lactation care studies have focused on LCPs with International Board-Certified Lactation Consultant (IBCLC) qualifications. Only a few studies have examined LCPs with other qualifications. 12
The International Board of Lactation Consultant Examiners is the primary global certifying body for LCPs, ensuring adherence to clinical and ethical standards.11,22,23 IBCLCs are trained in biomedical, evidence-based lactation management, as well as communication-based interpersonal support techniques and problem-solving strategies.24,25 Training includes teaching methods and message delivery skills and emphasizes active learning, attentive listening, empathy, and motivational strategies to foster maternal self-efficacy and breastfeeding confidence, as well as verbal and nonverbal communication skills as essential tools in building trust and connection. 23 These skills are designed to support mothers in navigating ambivalence about the investment in and demands of breastfeeding and the challenges of implementing lactation plans while managing the competing needs of early parenthood. 26 In Israel, where the current study was conducted, there are two additional types of LCP qualifications. The first is RNLC, involving a 1-year advanced breastfeeding course authorized by the Ministry of Health as an additional specialization following the attainment of a bachelor’s degree in nursing education and training. The second type is lactation educators (LEs), who complete a course focusing on human lactation and breastfeeding support. This training is based on the content of the IBCLC certification, but it involves fewer hours of clinical practice and varies in content per teaching establishment. These differences in training may influence both the priority given to emotional support in lactation care and the effectiveness of delivery.
The Current Study
This study examined how LCPs and mothers without diagnosed mental health conditions perceived the emotional aspects of lactation care. Specifically, it assessed the extent to which LCPs and mothers viewed emotional support as an integral part of lactation care. It also examined whether LCPs’ and mothers’ perceptions vary with LCPs’ qualifications (i.e., IBCLC, RNLCs, and LEs). Finally, the study explored whether background variables, particularly LCPs’ and mothers’ education, age, and duration of lactation care, are associated with their perceptions. No a priori hypotheses were formulated due to the lack of relevant research.
Materials and Methods
Participants
The study included 149 LCPs and 201 mothers who had received assistance from LCPs in the past year.
Procedure
This study was conducted between June 2023 and September 2023. LCPs and mothers were recruited through social media and professional networks. Potential participants received an explanation about the study by phone or email from the research team, and informed consent was obtained. Those who agreed to participate were provided with a link to an anonymous online survey. LCPs and mothers each received a separate survey link. The survey included the Attitudes Toward the Emotional Aspects of Lactation Care Questionnaire and a demographic questionnaire. The study was approved by the Ethics Committee of the University of Haifa, Israel (approval #204/23).
Measures
Attitudes toward the emotional aspects of lactation care questionnaire (AEALC-Q)
This 10-item questionnaire was adapted for the current study from the Positivity of Attitudes and Sense of Competence Questionnaire. 27 Six items assessed expectations that LCPs would address emotional aspects, including mothers’ emotional needs and their relationship with the infant, as part of lactation care (e.g., “The LCP must pay attention to what the mother feels during the lactation care session, even if it comes at the expense of success in breastfeeding”; “It is the LCP’s role to guide the mother and mediate the infant’s cues and emotions, to help her become more attuned to them.”). Four items assessed perceptions of LCPs’ competence, knowledge, and training in emotional aspects (e.g., “The LCP is capable of supporting the mother with emotional difficulties related to breastfeeding and early parenthood”; “LCPs are trained and knowledgeable about how to support mothers emotionally”). Responses were rated on a 6-point Likert scale, ranging from “1” (“Strongly Agree”) to 6 (“Strongly Disagree”). See the complete list of items in Table 1. The internal consistency of the questionnaire (Cronbach’s alpha) was acceptable for LCPs (α = 0.65), and good for mothers (α = 0.73).
Lactation Care Providers’ and Mothers’ Perceptions of the Emotional Aspects in Lactation Care (N = 350)
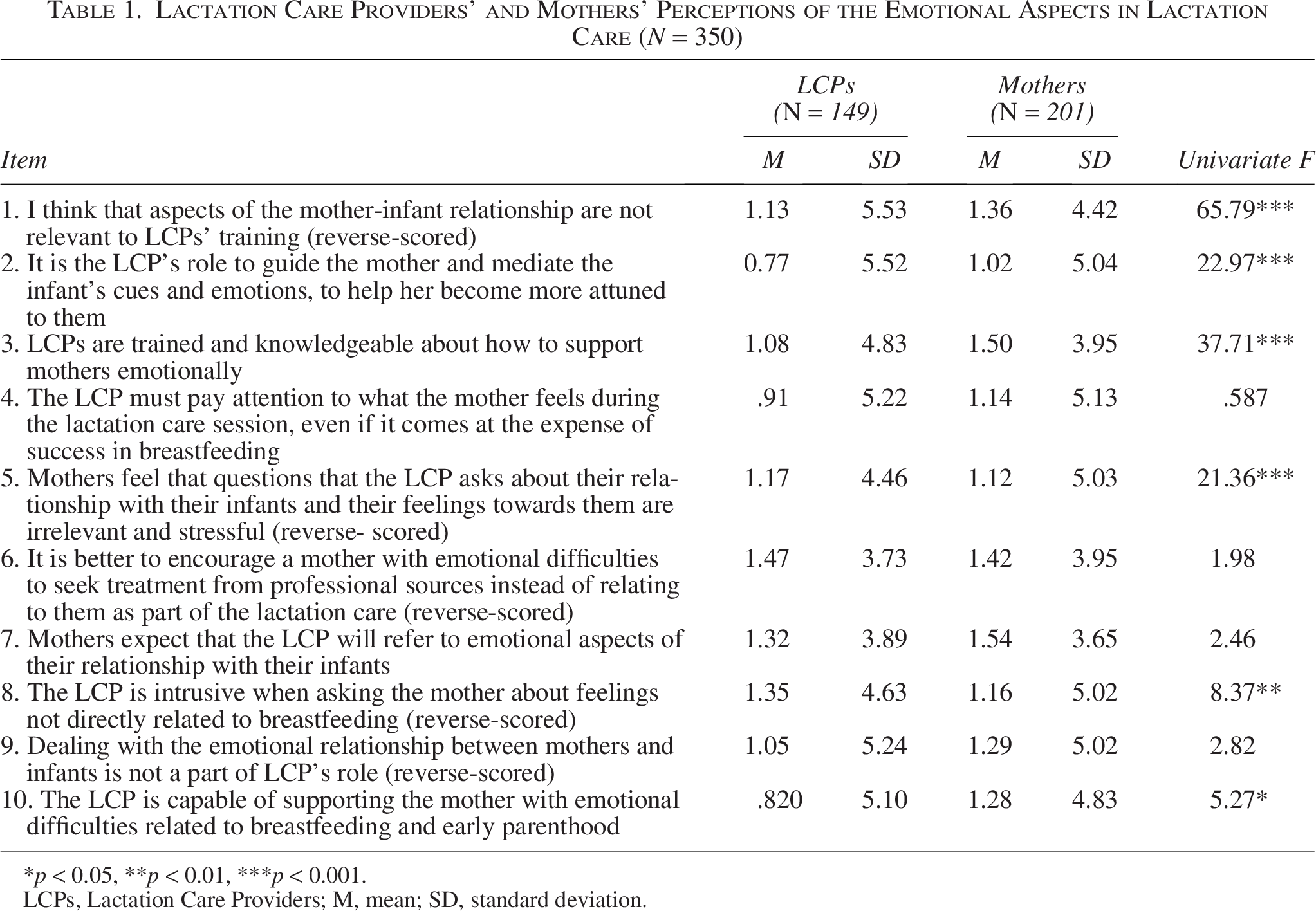
p < 0.05, **p < 0.01, ***p < 0.001.
LCPs, Lactation Care Providers; M, mean; SD, standard deviation.
Demographic questionnaire
Participants completed a questionnaire developed for this study. LCPs reported their age, type of LCP qualification (i.e., IBCLC, RNLC, LE), years of LCP experience, and educational level. Mothers reported their age, number of children, education level, and their LCP’s qualification (i.e., “What was the qualification of the lactation consultant you met?) (1 (Registered Nurse Lactation consultant) (2 (IBCLC) (3 (Lactation Educator,) (4 (I don’t know”). It should be noted that LCPs in Israel, typically state their qualification when introducing themselves to mothers or in the consent form for counseling that mothers sign. Mothers also reported the duration of lactation care received by answering two questions: “For how long have you been in contact with the LC? Specify in months,” and “How often did you meet the LC?) (1 (Only once, (2) Once a week, (3) Once in two weeks, (4). Once a month.” The final score was calculated by multiplying months of contact by session frequency.
Data analysis
Statistical analyses were conducted using SPSS (version 27). Descriptive statistics summarize the background characteristics of the LCPs and mothers. Independent-sample t-tests were conducted to compare the overall AEALC-Q mean scores between LCPs and mothers. To assess item-level differences, multivariate analyses of variance (MANOVA) were employed, followed by univariate tests with Scheffé post hoc comparisons. One-way ANOVAs were used to assess differences in perception by LCP qualification type. Pearson correlation coefficients were calculated to assess the links between background characteristics and the AEALC-Q scores.
Results
Participants’ characteristics
Of the LCPs, 43.6% were IBCLCs, 29.5% were RNLCs, and 26.8% were LEs. Among mothers, 64.2% were assisted by IBCLCs, 14.4% by RNLCs, and 9.0% by LEs, whereas 12.4% did not know their LCP’s qualification. Most LCPs (86.6%, n = 129) held a bachelor’s degree or higher, 10.7% (n = 16) had professional post-secondary education, and 2.7% (n = 4) had secondary education. Their ages ranged from 28 to 78 years (M = 45.95; SD = 9.85), and their professional experience ranged from 1 to 27 years (M = 8.48; SD = 6.14). Mothers’ ages ranged from 23 to 46 years (M = 33.58; SD = 4.28). 192 mothers (95.5%) held bachelor’s degrees or higher. Six mothers (3.0%) had professional post-secondary education, and three (1.5%) had secondary education. The average number of children was 1.7, ranging from 1 to 7 (SD = 1.02). More than half of the mothers (56.8%; n = 113) had one child. The duration of lactation care ranged from 1 to 10 months (M = 3.70; SD = 2.51).
LCPs and mothers’ perceptions of the emotional aspects in lactation care
Analysis of the average AEALC-Q scores revealed that LCPs were more likely (M = 4.81, SD = 0.55) than mothers (M = 4.60, SD = 0.69) to view emotional aspects as essential to lactation care, t (346) = 3.18, p = 0.002. To further explore the differences in specific perceptions of LCPs and mothers, a MANOVA was conducted with each AEALC-Q item as the dependent variable and LCPs versus mothers as the independent variable. The multivariate effect was significant: Wilks’ Λ = 0.673, F(10, 339) = 16.45, p < 0.001, η2 = 0.33. As shown in Table 1, follow-up analyses of univariate effects revealed a complex pattern. Both LCPs and mothers agreed at a similar level that mothers expect their LCPs to address the emotional aspects of their relationship with the infant, that dealing with the mother-infant relationship is part of the LCPs’ role, and that addressing mothers’ emotions is more important than achieving the breastfeeding success level (items #4, #7, and #9). Furthermore, both LCPs and mothers concurred that mothers with emotional challenges should be referred to appropriate professionals (item #6). At the same time, LCPs perceived themselves as more able, competent, and trained in managing emotional aspects, particularly those associated with breastfeeding difficulties, than mothers perceived them to be (Items #1, #2, #3, and #10). Finally, LCPs were more likely than mothers to think that mothers would perceive questions about their own feelings, their relationship with their infants, and their feelings toward their infants as irrelevant to lactation care stressful and intrusive (Items #5 and #8).
Differences in perceptions of the emotional aspects in lactation care by LCP qualification type
LCPs’ perceptions
Next, to examine whether the LCPs’ perceptions varied by the type of their qualification, a one-way ANOVA was conducted. The analysis revealed a significant difference in overall perception of emotional support (as reflected in mean AEALC-Q scores), F(2, 146) = 3.51, p = 0.033. However, post-hoc tests revealed no significant differences between the three LCP groups (p’s > 0.05).
To further examine differences in specific perceptions across LCPs’ qualifications (i.e., at the AEALC-Q item level), a MANOVA was conducted. The multivariate effect was not significant, Wilks’ Λ = 0.834, F(20, 274) = 1.31, p = 0.175, η2 = 0.087. Nevertheless, a follow-up analysis of the univariate effects revealed significant differences in four items (#3, #6, #7, and #10). As shown in Table 2, Scheffé post hoc tests indicated that RNLCs scored significantly higher than LEs on item #3 (p = 0.012). RNLCs also scored significantly higher than both LEs (p = 0.016) and IBCLCs (p = 0.044) on Item #10. This suggests that although LCPs’ perceptions generally did not vary by qualification, RNLCs felt better trained to provide emotional support than LEs and as more capable of providing it than both IBCLCs and LEs.
Lactation Care Providers’ Perceptions by the Type of Their Qualification (N = 149)
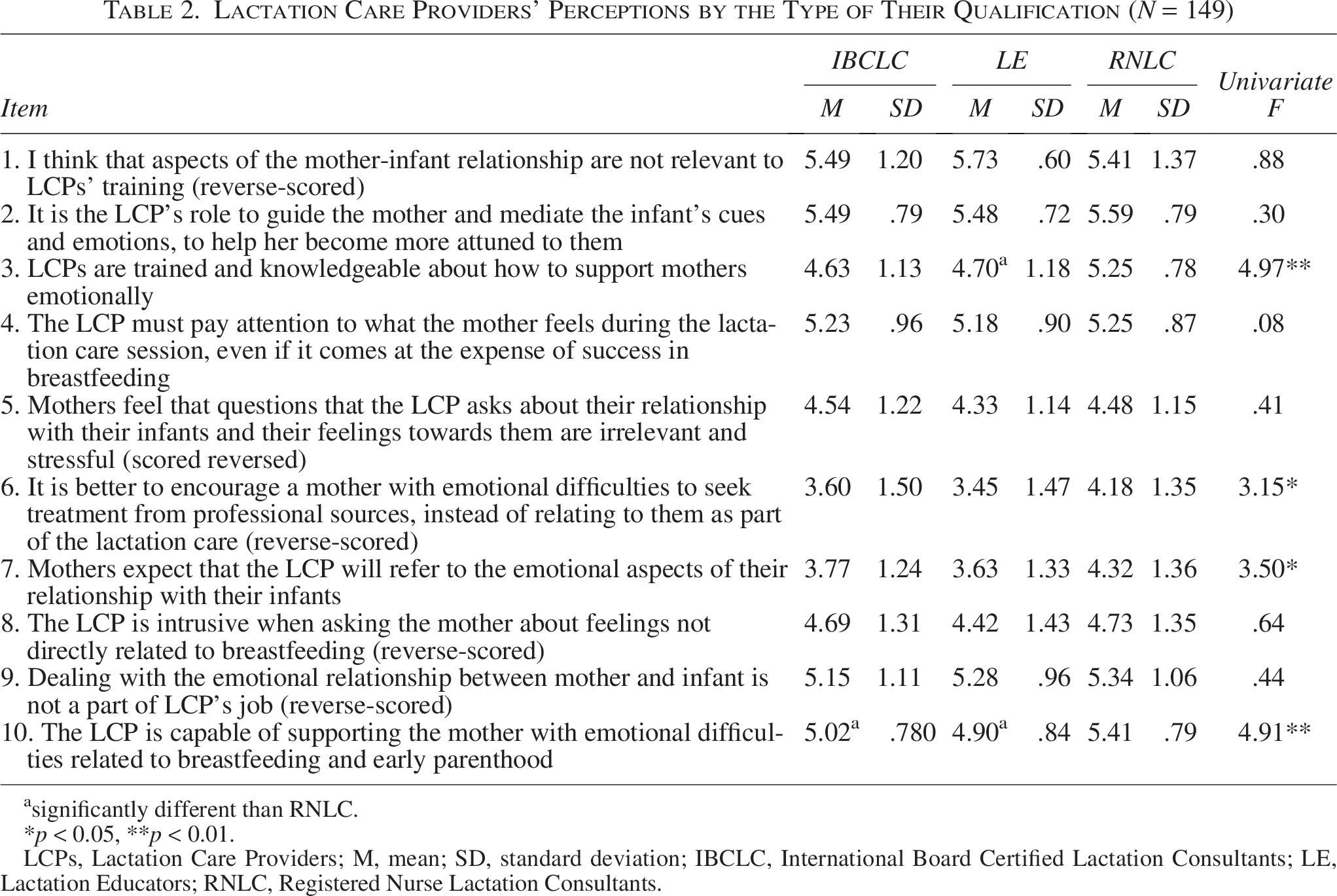
significantly different than RNLC.
p < 0.05, **p < 0.01.
LCPs, Lactation Care Providers; M, mean; SD, standard deviation; IBCLC, International Board Certified Lactation Consultants; LE, Lactation Educators; RNLC, Registered Nurse Lactation Consultants.
Mothers’ perceptions
A one-way ANOVA revealed no significant differences in mothers’ overall perceptions of the emotional aspect of lactation care (as reflected in AEALC-Q mean scores) by qualification of their LCPs, F(3, 197) = 1.50, p = 0.216.
A MANOVA that assessed differences in specific maternal perceptions by LCPs’ qualifications (i.e., at the questionnaire item level) revealed a significant multivariate effect, Wilks’ Λ = 0.775, F(30, 552.49) = 1.67, p = 0.015, η2 = 0.081. Follow-up univariate analyses indicated a significant difference only in mothers’ perceptions of the LCPs’ ability to support mothers with emotional difficulties at the transition to parenthood (item #10), F(3, 197) = 7.23, p < 0.001. Scheffé post hoc test revealed that mothers assisted by IBCLCs agreed with this statement (M = 5.08, SD = 1.14) significantly more often than mothers assisted by RNLCs (M = 4.10, SD = 1.50), F (3, 197) = 7.23, p = 0.002. No significant differences were observed for the other items (p’s > 0.05).
Differences in perceptions of the emotional aspect of lactation care by mothers’ and LCPs’ background
Finally, Pearson correlations were used to explore the associations between LCPs’ and mothers’ background characteristics and their overall perceptions of the emotional aspects of lactation care, as measured by AEALS-Q mean scores. The LCPs’ characteristics included education level, age, and years of professional experience. Mothers’ characteristics included education level, age, and duration of lactation care.
No significant correlations were found except for one. A longer duration of lactation care was associated with mothers’ more positive perceptions of emotional support in lactation care (r = 0.18, p = 0.010). Notably, one-way ANOVA revealed no significant differences in lactation care duration by the qualification of the LCPs mothers met, F(3, 197) = 1.22, p = 0.305.
Discussion
LCPs engage with mothers during the postpartum period, 21 where emotions significantly affect breastfeeding outcomes.15,28 Yet, LCP research has given limited attention to the emotional component of lactation care.9,11,29 The current study addressed this gap by examining how mothers and LCPs with various qualifications perceive this emotional aspect.
Ambivalence regarding the emotional aspect of lactation care
The findings revealed ambivalence among LCPs and mothers regarding the emotional aspect of lactation care. While both LCPs and mothers agreed that addressing mothers’ feelings during lactation care sessions is more important than achieving breastfeeding success, their perspectives on the LCP’s role in providing emotional support diverged.
LCPs viewed this aspect as part of their role and believed that their professional experience equipped them to address emotional aspects effectively. Yet they also expressed concerns about overstepping professional boundaries and about the possibility that addressing emotional issues might be perceived by mothers as intrusive. In contrast, mothers considered such discussions relevant and expected emotional engagement from their LCPs. However, they perceived the LCPs as lacking sufficient training and expertise in this area. These discrepancies may underscore a gap in LCPs’ training.
Professional literature for LCPs and their training emphasizes teaching methods, attentive listening, empathy, and motivational strategies to foster maternal self-efficacy and breastfeeding confidence, as well as verbal and nonverbal communication skills as essential tools in building trust and connection. 23 Our findings suggest that these resources may not provide sufficient guidance on how to enact emotional support in ways that are responsive to mothers’ needs while maintaining clear professional boundaries and avoiding a shift toward the role of emotional therapists.23–26
LCPs’ training programs may benefit from incorporating findings from developmental research, particularly studies on bonding, 30 early mother-infant interactions, 31 and maternal sensitivity to infant cues, 32 which are closely linked to responsive breastfeeding. 33 Training programs can also integrate evidence-based practices that support maternal well-being and infants’ development,34,35 and are associated with increased breastfeeding duration and exclusivity. 36 These practices include emotional regulation 37 and relaxation techniques, like mindfulness training, 38 and psychoeducational tools to help mothers respond more appropriately to infant cues, 39 and encourage partner support. 40 Providing such developmental knowledge and practices may enhance LCPs’ competence and reduce their concern about being perceived as intrusive. Working within a multidisciplinary health care team may also support LCPs in navigating professional boundaries. 7
Differences in LCPs’ and mothers’ perceptions of LCPs’ emotional support across LCPs’ qualification types
A novel aspect of this study was the examination of differences in perceptions between LCPs and mothers across LCPs with varying qualifications. For the most part, no significant differences were found. Additionally, the LCPs’ perceptions did not vary with their educational level or years of experience. However, there were two exceptions. RNLCs reported greater confidence in their ability, knowledge, and capacity to provide emotional support to mothers compared to IBCLCs and LEs. This finding may reflect RNLCs’ more comprehensive professional training and greater clinical experience. This result aligns with qualitative research indicating that RNLCs view themselves as playing a significant role in identifying and supporting women with postpartum-related mental health issues. Our study complements this work by using a quantitative approach and comparing RNLCs’ perceptions with those of LCPs who received other training programs. 18
At the same time, mothers assisted by IBCLCs tended to report to a greater extent that LCPs could help mothers with postpartum emotional difficulties than did mothers assisted by RNLCs and LEs. Thus, mothers’ perception that LCPs lack sufficient training in this domain is less evident in the context of IBCLC lactation care. Previous studies examining mothers’ perceptions of LCPs’ support did not take LCPs’ training into account. 21 Our study highlights the importance of addressing this factor. Together with the finding that RNLCs perceived themselves as more capable than IBCLCs in addressing emotional aspects, these results suggest that IBCLCs may underestimate their capabilities, whereas RNLCs may overestimate theirs.
The duration of lactation care
The background characteristics of LCPs and mothers were not associated with their perceptions, except for lactation care duration. Longer duration was associated with more positive maternal perceptions of the emotional aspect of lactation care. This finding complements previous studies showing that long-term, continuous relationships between mothers and their LCPs, whether predefined for a duration of 1 year or based on ongoing availability for problem-solving (responsive care), are associated with increased breastfeeding self-efficacy, longer duration of breastfeeding, and greater exclusivity.11,12
It could be that a longer duration of lactation care is associated with more trust, intimacy, and confidence, enabling emotional issues to arise in communication between the mother and her LCP. It is also possible that addressing emotional aspects in a manner attuned to mothers’ needs facilitates longer lactation care. Prospective studies assessing the quality of emotional support provided by LCPs are needed to elucidate the nature of these associations. Another possible interpretation of this finding is that mothers who experienced greater breastfeeding difficulties may have required longer or more intensive lactation consultation and, as a result, perceived receiving higher levels of emotional support from their LCP. Alternatively, experiencing more significant breastfeeding difficulties may have heightened mothers’ awareness of, or need for, emotional support from their LCP, influencing their perception of the emotional support received. These interpretations should be examined in future research by including a systematic assessment of breastfeeding difficulties using tools such as the Maternal Breastfeeding Evaluation Scale (MBFES) or the LATCH (Latch, Audible swallowing, Type of nipple, Comfort, Hold) Assessment Tool. 26 Nevertheless, the findings suggest that fostering continuous relationships with mothers and increasing LCPs’ awareness of their meaningful roles in mothers’ lives may prove beneficial.
Strengths and limitations
This study’s strengths include a sample of LCPs with diverse training and assessments of both the perspectives of both LCPs and mothers. However, this study has several limitations that may guide future research. First, the study was based on a convenience sample, which limits its generalizability. Second, the study mainly consisted of IBCLCs, restricting the ability to draw definitive conclusions regarding differences related to other LCPs’ qualifications. Additionally, it was conducted within the qualification frameworks of LCPs in Israel. Exploring the perceptions of IBCLCs and LCPs with other qualifications in different countries might yield different conclusions. A related limitation is the relatively small sample size of mothers supported by RNLCs and LEs, which restricted the ability to study their differing perceptions. Finally, the study relied on self-reported questionnaires, which may be subject to social desirability. However, because perceptions are inherently subjective, self-reporting remains an appropriate and informative method for assessing them.
Conclusions
This study is innovative in addressing the understudied and often-overlooked aspect of LCPs’ support for breastfeeding mothers: the provision of emotional support. It suggests that both LCPs and mothers view the role of LCPs as extending beyond breastfeeding to encompass the broader emotional aspects of early parenthood. LCPs feel well-educated to offer emotional support to mothers but perceive it as potentially intrusive, whereas mothers perceive LCPs as lacking sufficient training and knowledge to provide such support. These findings highlight the need to increase attention in LCP training to the emotional needs of mothers and infants and to enhance LCPs’ sense of competence in addressing these needs sensitively and non-intrusively.
Authors’ Contributions
H.L.R.H. designed the study, collected the data, conducted the statistical analyses, and led the writing of the article. E.S.C., the PhD advisor of H.L.R.H., co-designed the study and contributed to the statistical analyses and article writing.
Footnotes
Acknowledgments
The authors thank the mothers and lactation care providers who participated in this study.
Disclosure Statement
There are no financial, commercial, or personal relationships that could be construed as a potential conflict of interest.
Funding Information
The Graduate Studies Authority of the University of Haifa supported this work.