
Abstract
Background:
Pasteurized donor human milk (PDHM) is frequently used to supplement healthy, breastfeeding newborns in birth hospitals, with varied practices and limited postdischarge outcomes. This review examines the use of PDHM supplementation in healthy, noncritically ill newborns cared for in postpartum units and level 1 nurseries and aims to understand its effects on lactation after hospital discharge.
Methods:
We conducted an integrative review of both qualitative and quantitative studies that were conducted in the United States, in English, and reported the use of PDHM in healthy or noncritically ill infants, and where the primary setting was a mother–baby unit or level 1 nursery. Data sources included PubMed, CINAHL, Scopus, Web of Science, Embase, Emcare, and the Maternity and Infant Care Database. We included 18 articles published between 2014 and 2025 in the final review. Common characteristics were categorized, quantified, and compared across the studies.
Results:
Inductively derived categories are as follows: (1) indication for PDHM supplementation, (2) hospital-level characteristics, (3) breastfeeding outcomes, (4) maternal and infant demographic and socioeconomic characteristics, and (5) opinions on the use of PDHM when reported from clinical and patient perspectives. In addition, we specifically examined each article for examples of the protection of milk supply (interventions to support lactation and/or pumping recommendations).
Conclusions:
PDHM is preferable to formula for supplementation and has been associated with improved breastfeeding outcomes. However, evidence suggested that supplementation without interventions to protect milk supply may pose a risk to breastfeeding after discharge.
Keywords
Introduction
The World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) 1 and the American Academy of Pediatrics (AAP) 2 recommend an exclusive human milk diet for the first 6 months of life and continued breastfeeding along with complementary feedings until age 2 years or beyond. Yet, in the United States, breastfeeding rates are persistently suboptimal. According to the Centers for Disease Control and Prevention, in 2022, 85.7% of infants were breastfed at birth, but only 27.9% of infants received an exclusive human milk diet by age 6 months. 3
Human milk and breastfeeding have short- and long-term health benefits for infants and women. Infants who are breastfed have a reduced risk of mortality and common childhood infections such as otitis media, gastrointestinal and respiratory illnesses, including respiratory syncytial virus, and a reduced risk of chronic diseases, including type 1 and type 2 diabetes, obesity, and leukemia. 4 Evidence also supports an association with breastfeeding and higher intelligence scores in children later in life. 5 Women who breastfeed have a lower risk of developing type 2 diabetes, hypertension, and cancers, including breast, ovarian, endometrial, and thyroid cancers. 4
Many benefits of breastfeeding are dose-dependent and enhanced when breastfeeding is done exclusively and for an extended duration. 4 Duration and exclusivity of breastfeeding are associated with the timely onset of a copious milk supply brought on by secretory activation.6,7 This stage of milk production, which typically occurs 2–4 days after birth, requires frequent and effective removal of milk from the breast.4,7
When a woman is unable to provide human milk due to maternal or infant illness or separation from the infant, pasteurized donor human milk (PDHM) is preferred over formula for infant feeding supplementation.1,4 Although PDHM was initially recommended for preterm and critically ill infants, the use of PDHM for supplementation in level 1 newborn nurseries and mother–baby units has increased. 8 Little is known about the practice of supplementation with PDHM for healthy newborns cared for in postpartum units and level 1 nurseries and its impact on lactation after hospital discharge. As PDHM supplementation becomes more common among well and noncritically ill infants, it is important to gain a clearer understanding of its use during the postpartum hospital stay and its potential effects on lactation and breastfeeding after hospital discharge.
Background
Since 1979, the WHO and UNICEF have recommended an alternate source of “human breastmilk,” as the preferred form of infant supplementation when a mother’s own milk (MOM) is unavailable or contraindicated. 9 In 2012, the AAP recommended that all preterm infants receive human milk and that PDHM be given when the mother’s milk is not available or contraindicated. 10 The Baby Friendly Hospital Initiative (BFHI) was introduced by the WHO and UNICEF in 1991 and was updated in 2018 to improve breastfeeding care for infants in birthing hospitals. 11 The BFHI designation is given when hospitals demonstrate adherence to the Ten Steps to Successful Breastfeeding model designed to promote breastfeeding through practices such as parent education, skin-to-skin contact, early breastfeeding, rooming in, and avoiding the unnecessary use of any food or fluid other than breast milk unless medically indicated. 12 Hospitals must also comply with the International Code of Marketing of Breastmilk Substitutes, which discourages the promotion of formula in birth hospitals. 12
Standardized guidelines and best practices have not been widely established regarding the use of PDHM for noncritically ill infants, which highlights gaps in knowledge about the use of PDHM for supplementation, indications for use, methods of supplementation, and paired strategies to protect a mother’s milk supply. 8
Two recent systematic reviews were conducted, in which authors studied the use of PDHM in various populations.13,14 In the first, McCune and Perrin examined the use of PDHM in healthy infants, critically ill and noncritically ill infants, and other nontraditional recipients treated outside typical well-newborn care settings (e.g., adult cancer patients and children after bone marrow transplants). 13 The authors reviewed 26 studies and, among those focused on healthy infants, found limited and conflicting evidence supporting a relationship between PDHM use and health outcomes. 13 While some studies found PDHM was associated with increased breastfeeding duration, others found no impact on breastfeeding outcomes. 13 In the second, McClintock et al. reviewed 11 studies in which the authors investigated the benefits and risks of infant supplementation with PDHM, infant formula (IF), and MOM for late-preterm infants (LPIs) and early-term infants. 14 In two of the included studies, researchers suggested a positive association between the use of PDHM and exclusive breastfeeding at discharge for LPIs and early-term infants. 14 However, in most of the included studies, researchers reported no association or effect on other measured infant health outcomes. 14 These two systematic reviews included studies from the United States and the international community, and the reviewers concluded that more high-quality studies should be completed because of the unclear associations between the use of PDHM and breastfeeding outcomes.13,14 Neither McClintock et al. nor McCune and Perrin focused solely on the use of PDHM in healthy, noncritically ill infants in the birth hospital setting.13,14
The use of PDHM among healthy newborns in the United States is increasing. 8 Our integrative review 15 approach is distinct in that we included exclusively United States-based research to examine practices within the context of domestic policy and culture, and we incorporated both quantitative and qualitative studies to provide a more comprehensive understanding of the use of PDHM for supplementation in the birth hospital. The purpose of this integrative review 15 was to examine the use of PDHM for supplementation in healthy, noncritically ill newborns cared for in postpartum units and level 1 nurseries and to understand how PDHM supplementation affects lactation after hospital discharge. We acknowledge the gendered nature of some terms used throughout this review. We chose terms for consistency and clarity, and our aim is that all lactating persons and families who will provide human milk will be better informed based on the findings presented in this review.
Methods
We used Whittemore and Knafl’s methodology to conduct our integrative review. 15 An integrative review is an approach to synthesize evidence intended to present the current state of the science on a topic with direct applicability to practice and policy, which makes it an ideal method for contribution to nursing science. 15 Whittemore and Knafl described five stages for conducting an integrative review: problem identification, literature search, data evaluation, data analysis, and presentation. 15 The literature review, data evaluation, and data analysis are described below.
Literature search
The first author consulted with a medical librarian (F.C.) at the University of Pennsylvania to develop and refine the search strategies. PubMed, CINAHL (EBSCO), Scopus (Elsevier), Web of Science (Clarivate), Embase (Elsevier), Emcare (OVID), and the Maternity and Infant Care (OVID) databases were searched. Our search included terms referring to healthy, term, or well infant or newborn, PDHM, milk banks, breastfeeding, and breastmilk supplements. Subject headings were added when applicable, and search terms were modified based on the requirements of each database. The search results were filtered by date from 2014 or later and included studies conducted in the United States only to include the most relevant and contemporary practices. The full search strategy is provided in Supplementary Table S1. Search results were uploaded to Covidence, a web-based collaboration software platform that streamlines the production of systematic and other literature reviews. 16 Record screening, source selection, and appraisal were completed by the first author (N.C.) under the guidance of the supervising author, who was the secondary reviewer (D.L.S.).
Inclusion criteria
We included primary reports of qualitative and quantitative studies that examined the use of PDHM in healthy and noncritically ill infants; took place in or described the context of an inpatient mother–baby hospital unit, level 1 newborn nursery, or other setting where usual postpartum and newborn care are performed in the United States; and were written in English. We excluded sources that included infants primarily cared for in the neonatal intensive care unit. No gestational age was used to include or exclude participants, as policies regarding postpartum care for infants by gestational age vary among hospitals.
Study selection
An initial search was conducted in August 2024, and a secondary search was conducted in October 2025. Search yields from the October 2025 search are indicated heretofore in parentheses.
During the initial search in August 2024, we retrieved a total of 1,776 (+276) records from the database search. We removed 841 (+77) duplicates and screened the remaining 935 (+199) titles and abstracts based on our inclusion criteria. We excluded 885 (+190) records. Of the 50 (+9) remaining studies assessed for eligibility by full-text review, 34 (+7) studies were excluded. Studies were excluded due to the following reasons: unavailability of the full text or abstract only (n = 13) (+3), conducted outside of the United States (n = 5), using the wrong patient population (n = 4) (+1), wrong study design (n = 4) (+2), wrong intervention (n = 2), wrong setting (n = 2), and wrong outcomes (n = 2) (+1). The two aforementioned systematic reviews on the use of donor milk in populations other than critically ill infants13,14 were included in the search yield. We excluded these sources from our sample of included studies, but we used them to provide background and context in other areas of this article. Both systematic reviews were cross-referenced for additional articles. No additional articles were added. However, nine common articles included in the McCune and Perrin (2021) review17–25 and five common articles included in the McClintock (2024) review23–27 had already been selected from the original literature search. Our final review included 18 primary studies.17–34 The complete search and selection process is shown in a flow diagram using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline 35 in Figure 1.
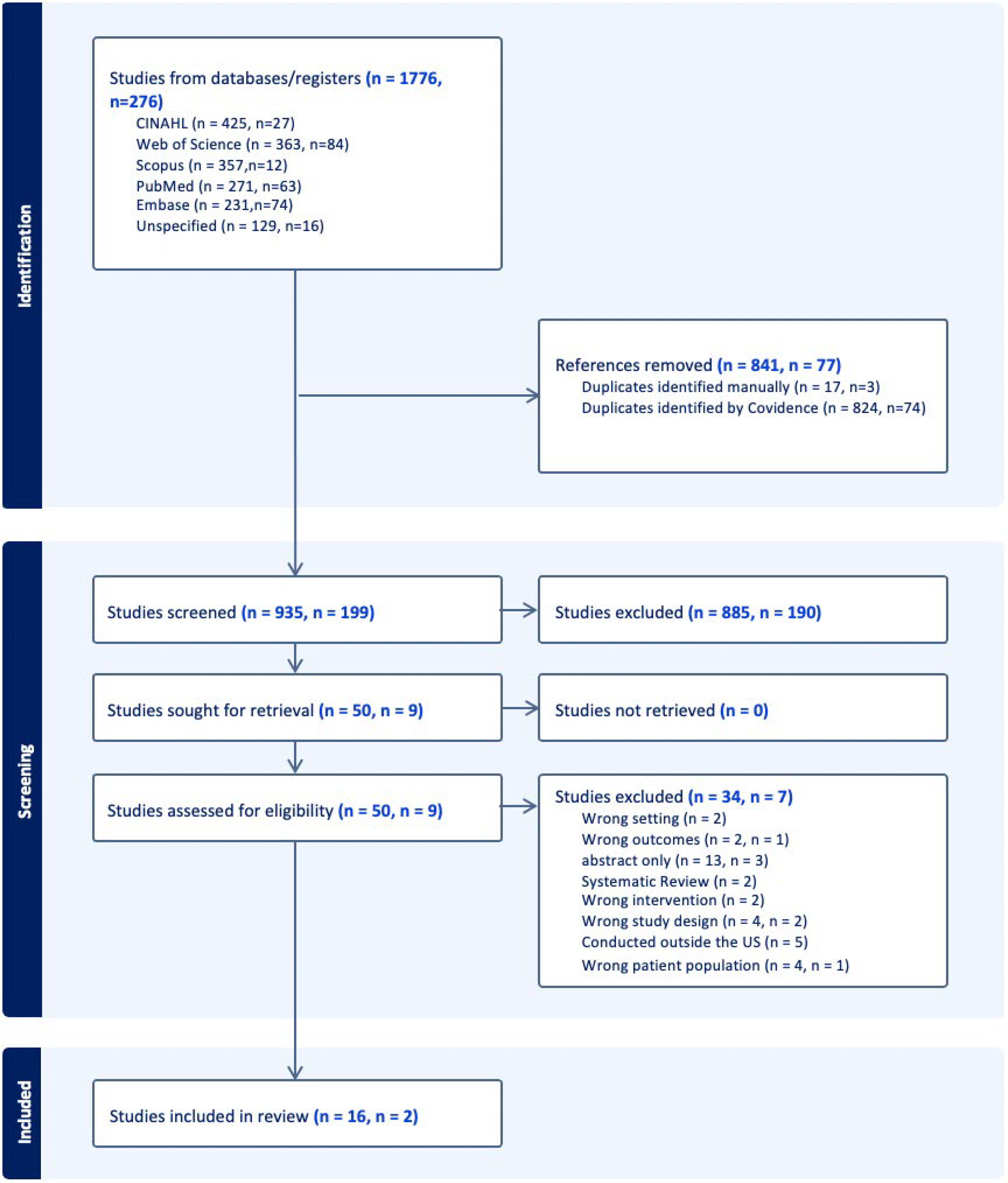
PRISMA flow diagram. PRISMA outlines the initial and secondary literature search. Initial search conducted in August 2024, results indicated by first value; secondary search results, conducted in October 2025, indicated by second value.
Data evaluation
Joanna Briggs Institute (JBI) (2024) critical appraisal tools were used to assess the quality of evidence for each study based on its design.36–39 The JBI appraisal tool lists items to assess the methodological quality and risk of bias based on study design, and each criterion is evaluated by answering “yes,” “no,” “unclear,” or “not applicable.”36–39 The quality of evidence was scored based on how many “no” or “unclear” responses were elicited, and the study’s quality was rated as “very high” if no items identified a risk of bias, “high” if one or two items identified a risk of bias, “moderate” if three or four items identified a risk of bias, “low” if five or six items identified a risk of bias, and “very low” if seven or more items identified a risk of bias (see Supplementary Table S2).36–39
Data analysis
We used the data analysis strategy described by Whittemore and Knafl, which included data reduction, data display, data comparison, conclusion drawing, and verification. 15 Common characteristics and broad concepts were categorized and quantified. Codes were inductively generated based on recurring patterns identified across the primary sources. In addition, the provision of the protection of a mother’s milk supply was deductively coded, as evidenced by pumping recommendation, lactation education, or IBCLC (internationally board-certified lactation consultant) consultation. Data collected within each category were compared across sources, integrated, and narratively presented.
Results
Study characteristics
Study designs included three interventional single-site studies,19,22,33 three survey-based cohort studies,24,26,27 five multisite survey-based studies,17,29–31,33 four retrospective case-control or cohort studies,23,25,28,32 two qualitative studies,18,21 and a single case report. 20
All studies were based on data collected in the hospital setting. Most studies were completed in hospitals based in the northeastern United States.17–19,25–27,30,33 Four studies were completed in Iowa,20–22,28 one study was set in the Pacific Northwest, 32 one study was set in Oklahoma, 23 one study was set in Florida, 24 and three studies surveyed hospitals across the country.29,31,34
Among the 18 studies included in the review, some repetition in authorship was noted. Five studies were authored by Kair,20–22,28,31 and two were authored by Ferrarello.18,19 Common authors were also noted within four studies based in the northeastern United States.17,25,27,30 Despite common authorship, different samples, variables, methods, and analyses were used. See Table 1 for a summary of the included studies.
Summary of Included Studies
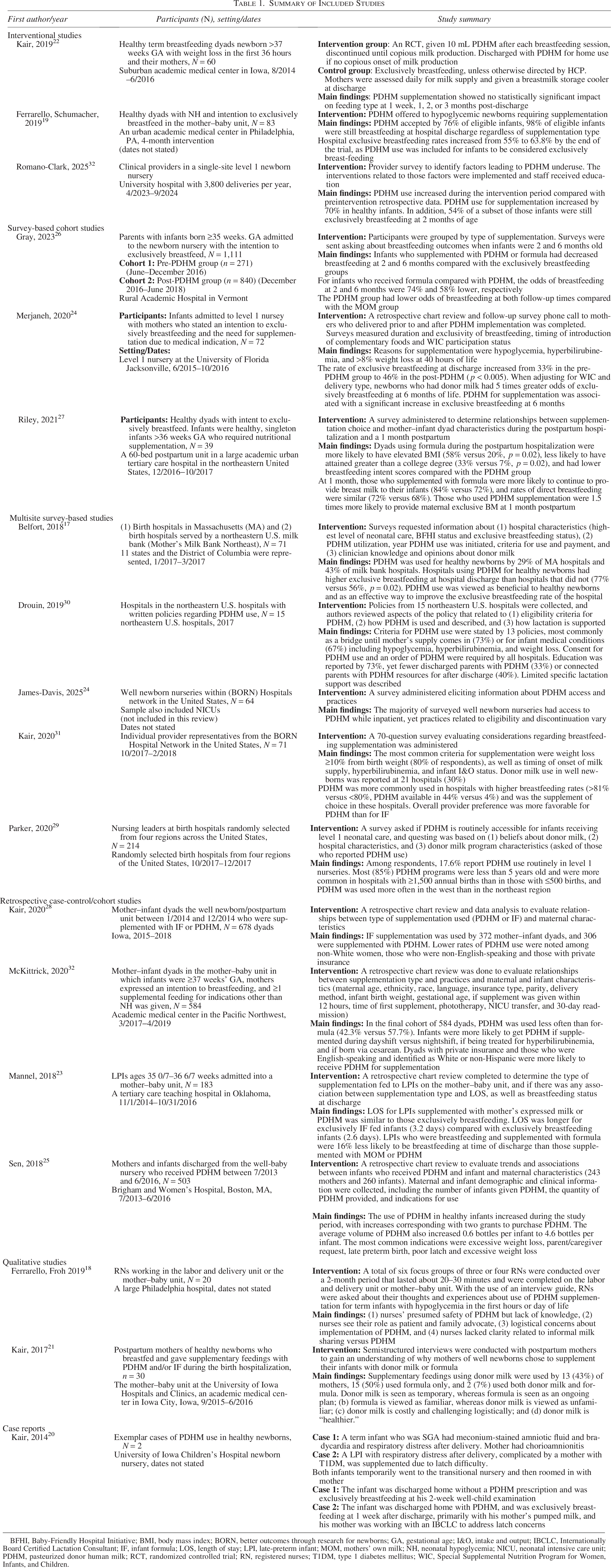
BFHI, Baby-Friendly Hospital Initiative; BMI, body mass index; BORN, better outcomes through research for newborns; GA, gestational age; I&O, intake and output; IBCLC, Internationally Board Certified Lactation Consultant; IF, infant formula; LOS, length of stay; LPI, late-preterm infant; MOM, mothers’ own milk; NH, neonatal hypoglycemia; NICU, neonatal intensive care unit; PDHM, pasteurized donor human milk; RCT, randomized controlled trial; RN, registered nurses; T1DM, type 1 diabetes mellitus; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Quality of evidence
The 18 included studies were appraised using the JBI critical appraisal tools (2024) based on their study design.36–39 Two articles were rated to be of very high quality,18,23 12 were rated as high quality,19–22,24–26,29,31–34 and 4 were rated as moderate quality.17,27,28,30 No studies were rated as low or very low quality. See detailed quality assessment data in the Supplementary Table S2.
Categories
During the data analysis stage, common categories emerged through the process of identifying patterns, counting, clustering, and comparing and contrasting studies. 15 Codes were inductively generated based on recurring patterns identified across the selected studies. Five categories were identified: (1) indications for supplementation with PDHM, (2) hospital-level characteristics, (3) breastfeeding outcomes, (4) maternal and infant characteristics, and (5) opinions on the use of PDHM. The provision of measures to protect the maternal milk supply was deductively sought out and coded in each study when available.
Indications for supplementation
Among the 18 studies, 15 (83%) included specific indications for supplementation.17–21,23–26,29–34 Neonatal hypoglycemia, hyperbilirubinemia, and weight loss were the most frequent indications for PDHM supplementation.18–21,23–26,29–34 Delayed lactation or lactation problems,30,31,33 feeding difficulties,22,23,25,26,33,34 and gestational age or birth weight criteria17,23,29,30 were also frequently mentioned indications for supplementation of healthy infants with PDHM.
LPIs were specifically identified as a population at higher risk for indications for supplementation by seven studies.17,21,23,25,29–31 LPIs were either not defined21,29–31 or defined as 35–36 weeks17,23 or 35–37 weeks. 25 Mannel and Peck found that while most mothers of LPIs in their study initiated breastfeeding, 80.7% of these infants received some supplementation during the birth hospitalization, with the most frequent reason being maternal request, followed by physician order (not otherwise specified). 23
Parental request was another common indication for supplementation with PDHM.21,22,23,25,26,29,32–34 Kair and Flahermanfound that the most common maternal self-reported reasons for PDHM or IF supplementation were low milk supply, difficulty latching, and maternal preference. 22
Hospital-level characteristics
Five studies sent surveys to hospitals in the United States to assess the use of PDHM in well newborn nurseries.17,29–31,34 The number of respondents from multisite surveys varied from n = 15 to n = 214.29,30 Kair et al. found that hospitals with higher breastfeeding rates (>81% versus <80%) were more likely to have PDHM available for healthy infants (44% versus 4%). 31 Belfort et al. reported that hospitals using PDHM for healthy newborns had higher rates of exclusive breastfeeding at discharge. 17 Parker et al. reported that most donor milk programs in level 1 nurseries were less than 5 years old and were more common in hospitals with greater than 1,500 births per year. 29 However, James-Davis et al. surveyed 64 well newborn nurseries across the United States and found no association between yearly newborn admissions and access to PDHM. 34 Parker et al. found that PDHM programs for healthy infants were more frequently available in hospitals located in the West and Midwest compared with the northeastern and southern regions of the United States. 29 Similarly, James-Davis et al. reported a decreased availability in the northeastern United States compared with other regions in their more recent study. 34
Five studies included in this review describe hospitals that have a written policy for PDHM use,17,19,20,30,34 five studies describe hospitals where signed consent is required for PDHM use,17,19,27,29,30 and nine studies describe an order being required for the use of PDHM, typically written by a physician or advanced practice provider.17,19,29,30,34 James-Davis et al. found that among 64 well newborn nurseries surveyed, 32 (58%) hospitals had a policy in place for PDHM provision, yet only 22 (40%) had a policy in place for discontinuation of PDHM. 34 McKittrick et al. found that infants receiving their first supplemental feeding during the day shift were twice as likely to receive PDHM over formula than if the first supplemental feeding was given on the night shift. 32
Drouin et al. examined 15 policies regarding PDHM use from U.S. hospitals and found that while lactation-focused patient education was reported in the PDHM policy by 11 (73%) of hospitals, it was not specifically detailed and focused mainly on education about breastmilk, breastfeeding, and PDHM. 30 Few hospitals routinely discharged patients with PDHM (33%) or connected parents with local resources to obtain PDHM after discharge (40%). 30
Ferrarello et al. described a nurse-led trial initiative with a written guideline to provide PDHM to well newborns with hypoglycemia which was defined as “a blood glucose level of less than 45 mg/dl in the first 4 hours of life, less than 50 mg/dl between 4 hours and 48 hours, and less than 60 mg/dl after 48 hours.” 19 , p.321. The authors found that the majority of mothers in their study chose PDHM as a supplement for their infant, and hospital breastfeeding rates increased during the trial period. 19 Sen et al. examined PDHM use in healthy infants with a retrospective chart review and found that an increase in PDHM use, as well as an increase in the volume of PDHM used, corresponded to the obtainment of two grants designated to purchase PDHM. 25
Nine studies were set in or included hospitals that had received BFHI designation or were on the pathway to BFHI designation.17,19,23,27,29,31–34 No direct association between BFHI hospitals and PDHM use, or breastfeeding outcomes, was measured.
Breastfeeding outcomes
Nine studies included data about breastfeeding outcomes, specifically breastfeeding rates at or after discharge, among well infants cared for in the postpartum unit or newborn nursery who used PDHM for supplementation.17,19,20,22–24,26,27,33 Kair et al. conducted a randomized controlled trial (RCT) in which a small volume of PDHM supplementation was administered after breastfeeding sessions in the intervention group until the mature milk supply was established, yet investigators found no association with PDHM supplementation and breastfeeding rates at 1 week or at 1, 2, or 3 months postpartum. 22 Investigators also found that at the 3-month follow-up time point, the prevalence of directly feeding at the breast within the last 24 hours was lower in the intervention group compared with the control group. 22
Eight studies support a positive association between PDHM use for supplementation and improved breastfeeding outcomes.17,19,20,23,24,26,27,33 Supplementation with expressed MOM resulted in similar or higher breastfeeding rates than PDHM for supplementation in four studies.23,24,26,27 Gray et al. found that infants supplemented with formula were 74% less likely to breastfeed at 2 months and 58% less likely to breastfeed at 6 months compared with those supplemented with PDHM; however, infants who supplemented with PDHM had lower odds of breastfeeding at 2 and 6 months compared with those who supplemented with MOM. 26 Merjaneh et al. found that using PDHM for supplementation among mothers who expressed an intention to breastfeed was associated with a significantly increased likelihood of exclusively breastfeeding at 6 months compared with those who supplemented with IF. 24 Belfort et al. found that hospitals that offer donor milk to healthy infants had higher rates of exclusive breastfeeding at discharge compared with hospitals that do not. 17
Maternal and infant characteristics associated with PDHM use
Mother–infant dyads were more likely to use PDHM for supplementation if the mother identified as White,27,28,32,33 was primarily English-speaking,27,28,32,33 or had private insurance.28,32 Kair et al. and McKittrick et al. both conducted retrospective reviews and hypothesized that disparities in PDHM use may be influenced by institutional barriers, language barriers, health care provider bias, and personal or family experiences.28,32 Kair et al. found that in a national survey of hospitals, Hispanic women were 72% less likely to use PDHM than non-Hispanic White women. 28 Non-Hispanic White women were also more likely to use PDHM when compared with non-Hispanic Black and Asian women, as well as those who reported their race as “other.” 28
Lower education levels 27 and participation in the Special Supplemental Nutrition Program for Women, Infants, and Children were associated with more formula use.24,27 Riley et al. found that infants in one urban tertiary care hospital were more likely to be supplemented with formula if they were born to mothers with an elevated body mass index (BMI) and those who had obtained less than a college degree. 27
Opinions on the use of PDHM
Clinical opinion
Five studies included data regarding clinician or patient opinions and acceptance of the use of PDHM supplementation in healthy infants.17,18,22,31,33 Opinions among physicians and ordering clinicians were generally positive regarding the use of PDHM.17,18,31 Both providers and nurses viewed PDHM as healthy when compared with formula.17,18,29,31 In a national survey, Kair et al. found that 62% of providers felt “very positive” or “somewhat positive” about the use of PDHM in healthy and noncritically ill infants outside the NICU and expressed a preference for PDHM supplementation over formula. 31 Romano-Clarke et al. created a quality improvement initiative to improve provider education about PDHM and found an increased acceptance and use of PDHM in their well newborn nursery. 33 Belfort et al. found that while the majority of the providers surveyed (n = 66) agreed that PDHM showed health benefits for LPIs (n = 56, 88%) and healthy newborns (n = 51, 78%), fewer providers felt that PDHM use in the well-baby nursery would be accepted by parents (n = 25, 38%), nurses (n = 25, 38%), and pediatricians (n = 26, 39%). 17
Maternal opinion
Kair and Flaherman surveyed mothers on the use of PDHM for supplementation and found most mothers viewed PDHM as “healthy” and “temporary,” yet many had concerns that it was “unfamiliar” compared with formula and worried it would be “costly” or “logistically challenging” to obtain after discharge. 21 In comparison, supplementation with IF was more often regarded as a long-term plan. 21 Two mothers viewed PDHM supplementation as “weird,” and one mother said, “I don’t feel comfortable with having someone else’s bodily fluids going into my child.” 21 , p.713.
When given the option, Ferrarello et al. found that a majority of mothers chose to use PDHM (n = 63) over formula (n = 20) for supplementation in the case of neonatal hypoglycemia. 19 Comments from parents in this study were positive, with mothers stating, “Mother’s or human milk is best,” and “If I would know who the mother that donated this milk is, I would like to thank her.” 19 , p. 324.
Protection of milk supply
Measures to protect maternal milk supply were mentioned in 13 of the 18 studies.18–22,24,26–28,30,31,33,34 In the single RCT, Kair et al. stopped all supplementation in the intervention group once copious milk supply came in. 22 Lactation education was reported to be provided by IBCLCs or nurses in 10 studies.19–21,24,26–28,30,31,33 A formal lactation consultation as a standard of care with the use of PDHM for supplementation was reported in five studies.19–21,26,31
Pumping was specifically recommended for mothers using PDHM in three studies.27,28,34 In addition, Kair et al. reported that both mothers were pumping before or after discharge in their case report. 20 Kair et al. (2020) reported that, in a national survey of 71 hospitals, only 76% (n = 54) of respondents reported pumping recommendations for women who were supplementing their infants. 31 James-Davis et al. found that 74% of the 64 well newborn nurseries surveyed did not require parents to actively pump or express milk during their birth hospitalization. 34
While access to PDHM at discharge may provide exclusivity of a human milk diet, this alone does not account for measures to help protect milk supply. Obtaining PDHM after discharge was mentioned in two studies and one case report.20,22,30 Kair et al. described cases where patients were discharged with PDHM or arrangements to obtain PDHM after hospital discharge were made. 20 Kair et al. supplied PDHM at discharge to mothers in the intervention group who did not report copious milk supply by the time of discharge. 22 Gray et al. described that in a rural academic hospital in Vermont, due to logistical constraints of obtaining PDHM outpatient, infants are routinely transitioned to formula supplementation just before discharge if supplementation is required. 26
Discussion
With this review, we highlight current practices, opinions, and potential benefits and shortcomings of PDHM supplementation in healthy and noncritically ill newborns. The use of PDHM for supplementation, when necessary or recommended, is a growing option in birth hospitals across the United States. Common diagnoses in healthy and noncritically ill newborns that require supplementation, such as neonatal hypoglycemia, hyperbilirubinemia, and weight loss, are frequently managed in mother–baby and postpartum units. 40 These conditions are typically transient and may only necessitate temporary supplementation before hospital discharge.
LPIs are a population in which PDHM may be specifically important. LPIs are often cared for in well-baby areas, and their specific needs can be easily overlooked. 41 LPIs have lower breastfeeding rates than their term counterparts and have a higher likelihood of the need for supplementation, driven by their immaturity, which can be associated with ineffective milk removal and delayed onset of lactation. 4 Supplementing with PDHM instead of formula may be protective of breastfeeding for this population, promoting health benefits that are particularly important for this higher-risk group. 4
Any supplementation in the early postpartum period, regardless of type, can interfere with secretory activation.7,42 Women whose infants receive supplementation should be proactively managed to maximize milk supply and promote the onset and maintenance of secretory activation, both in the inpatient and outpatient settings. 42 The protection of milk supply during PDHM supplementation was described by 13 out of 18 articles (72%) included in this review.18–22,30,31,33,34 The provision of lactation education to families by nurses or IBCLCs may help ensure that families are well equipped to continue stimulating milk supply while their infant is being supplemented.
Hospitals with policies or guidelines aimed toward supporting breastfeeding may contribute to consistency in care delivered to breastfeeding families supplementing with PDHM, which reinforces current evidence. 43 Consent for the use of PDHM for supplementation was frequently described and implies that PDHM is viewed similarly to medications or other biospecimens. The informed consent time point also presents an additional opportunity for education and clarification in managing milk supply while supplementing.
Nine of the studies included hospitals with, or on the pathway to, BFHI designation.17,19,23,27,29,31–34 Seeking or having obtained BFHI status may reflect a priority toward the use of human milk. These hospitals may nurture a supportive breastfeeding culture in multiple ways in addition to the use of PDHM. While BFHI supports PDHM use for supplementation over IF, the availability of PDHM is not required for BFHI designation. 12
Volumes of PDHM supplied were only mentioned in one study, 25 and reassessment and discontinuation criteria for PDHM were infrequently outlined in hospital policies.30,34 Ongoing, early supplementation is an important factor in developing the mother’s milk supply and future breastfeeding, and the necessity should be carefully evaluated to support appropriate supplementation practices.
Pumping recommendations were infrequently described in policies and practices when supplementing with PDHM.27,30,31,34 In the single case report, Kair et al. described that both families initiated pumping at the birth hospital, yet did not specify if this was a standard of care. 20 All patients who use PDHM for supplementation after birth should have a proactive pumping plan during their inpatient hospitalization, before hospital discharge, and during early outpatient management based on their short- and long-term breastfeeding goals.
Only three studies22,30,34 and one case study 20 mentioned discharging families with PDHM or arranging for obtaining outpatient PDHM. Kair et al. incorporated a small supply of PDHM given at discharge to certain mothers into the intervention arm of their RCT. 22 Alternatively, Gray et al. describe that due to logistic constraints of obtaining PDHM outpatient, infants who need continued supplementation are routinely transitioned to IF before discharge, interrupting exclusive human milk feeding. 26 To facilitate the transition to home feeding, clinicians should be aware of PDHM availability outside of the hospital and discuss feeding plans and expectations with families. Discussions with families based on short- and long-term breastfeeding goals can inform an individualized lactation management plan upon discharge. 4
Although it is beyond the scope of this review, the practice of informal milk sharing should be acknowledged. Informal milk sharing involves feeding an infant human milk obtained from a donor found within the community or via the internet and carries risks, including exposure to medications, diseases, or contaminants. 44 While the AAP discourages informal milk sharing, clinicians must be aware of and screen for this practice and can advise recipients to ensure that the donor is medically screened and the milk is handled properly.4,44
Generally, physicians and nurses had positive opinions about PDHM as an option for infant supplementation.17,18,31 The presence of guidelines and policies might help clinicians advocate for the use of PDHM for supplementation and create more familiarity with its use and potential benefits. Parents generally felt positive toward PDHM use, though some felt it was “unfamiliar” or “weird.” 21 Interestingly, Kair and Flaherman found supplementation with PDHM was commonly perceived as a temporary bridge to overcome the early hurdles of breastfeeding, yet IF was viewed as a more permanent feeding substitute. 21 Insights into the motivations and rationales for choosing PDHM or IF for supplementation will help guide the development of best practices, education for parents and clinicians, and hospital policies and guidelines that center on the feeding goals of the individual family.
An increased association between PDHM supplementation and improved breastfeeding rates was demonstrated by several studies.19,20,23,24,26,27 Parental intention and motivation to breastfeed, lack of exposure to or comfort with formula, or other factors likely play a role in the choice to supplement with PDHM and continued breastfeeding. An important note is that many hospitals include PDHM use in their exclusive breastfeeding rates, so some infants who are said to be exclusively breastfeeding were supplemented with PDHM, and not exclusively receiving MOM. This may inflate a hospital’s exclusive breastfeeding rates at discharge due to the use of PDHM supplementation.
Differences were described in PDHM supplementation based on race, ethnicity, primary language, insurance type, education levels, and BMI.27,28,32,34 The racial and socioeconomic trends demonstrated in this review mirror the larger racial and socioeconomic inequities in overall breastfeeding and maternity care in the United States. 4 Overall, breastfeeding initiation rates in the United States vary by race, with Black mothers initiating breastfeeding up to 16.7% less often than other ethnicities, based on 2019 National Vital Statistics System birth certificate data. 45 Similarly, Isiguzo et al. examined the impact of stress, support, and race on exclusive breastfeeding and found that, in general, Black mothers were less likely to exclusively breastfeed when compared with White mothers. 46
While supplementation choice may be multifactorial, findings associated with demographic characteristics suggest that certain groups may be less likely to be offered PDHM for supplementation, particularly those who identify as non-White, are non-English-speaking, and have lower socioeconomic status. Clinicians should be aware of the possibility of implicit or explicit biases affecting the supplementation choices offered to parents. All parents deserve accurate and complete information to be able to make informed and realistic feeding choices, and awareness of current trends will help clinicians partner with parents to achieve their personal feeding goals.
Limitations
We only included studies conducted within the United States, which limits the relevance of the findings for other countries. Furthermore, half of the studies in this review were conducted in the northeastern United States, which may limit generalizability.
Eleven of the 18 included studies had common authors, which may skew the findings based on researcher bias and a limited participant pool. It is possible that some data may have been analyzed and included more than once. The relatively small group of authors that contributed to this review is a limitation of this study; however, it reflects that the topic of PDHM use in healthy and noncritically ill infants is a growing field of research.
Conclusions
Practices surrounding PDHM supplementation for healthy infants vary, and the evidence about the effect on breastfeeding is mixed. While some findings support an association between PDHM supplementation with better breastfeeding outcomes compared with IF, these associations are likely multifactorial. Moreover, the availability of PDHM for supplementation aligns with and supports the feeding intentions of mothers who aim to provide human milk for their infants.
PDHM use should be thoughtfully considered and used in combination with other practices that are supportive of exclusive and prolonged breastfeeding. Hospital policies and practices that outline measures to equitably and proactively support lactation during PDHM supplementation may enhance breastfeeding and optimize the use of PDHM as a tool to improve breastfeeding outcomes. Further research is needed to determine best practices for PDHM supplementation in healthy infant populations and to explore the experiences of mothers whose infants were supplemented and the effect of PDHM supplementation on feeding after hospital discharge.
Authors’ Contributions
N.C.: Conceptualization, methodology, formal analysis, writing—original draft, and writing—review and editing. D.L.S.: Conceptualization, methodology, review of analysis, writing—review and editing, and supervision.
Footnotes
Acknowledgments
Librarian assistance and review of the qualifying examination by faculty at the University of Pennsylvania School of Nursing.
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this research.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.