
Abstract
Background:
Pediatricians play a central role in breastfeeding support, yet educational gaps persist in training programs worldwide. Understanding how educational priorities vary across career stages may help optimize breastfeeding education for health care professionals.
Objective:
This study aimed to identify distinct professional profiles among physicians providing pediatric care attending the Brazilian Congress of Pediatrics and to characterize their self-reported educational priorities regarding breastfeeding in order to inform continuing education initiatives tailored to the needs of different professional profiles.
Methods:
A cross-sectional electronic survey was conducted during the 41st Brazilian Congress of Pediatrics (Florianópolis, Brazil; October 2024). Participants included 290 physicians providing pediatric care—board-certified pediatricians (n = 164), pediatric residents (n = 109), and physicians without pediatric specialty certification providing pediatric care (n = 17). Fourteen binary variables representing clinical practice context and perceived causes of early weaning were used for cluster analysis. Educational priorities were assessed through classification of open-ended responses into thematic categories.
Results:
Three distinct clusters were identified, forming a career-stage gradient. Cluster 1 (n = 111, 38.3%) comprised predominantly early career professionals (mean age, 31.7 years; 64.9% residents) who prioritized technique/management. Cluster 2 (n = 44, 15.2%) showed intermediate characteristics, with emphasis on mother/family education and support network. Cluster 3 (n = 135, 46.6%) included mostly senior pediatricians (mean age, 44.7 years; 77.8% board-certified) who prioritized legislation/work, myths/misinformation, and the pediatrician’s role. This gradient emerged despite demographic variables being excluded from the clustering algorithm.
Conclusions:
Three distinct professional profiles with differing educational priorities were identified. Educational needs followed a career-stage gradient, ranging from practical clinical skills among early-career professionals to leadership, coordination, and policy competencies among senior pediatricians. The emphasis on the pediatrician’s role among senior professionals underscores a perceived need to reassert the pediatrician as the central coordinator of the breastfeeding support team. These findings support the development of career-stage-tailored educational strategies to maximize the relevance and effectiveness of continuing education initiatives.
Introduction
Exclusive breastfeeding (EBF) for the first 6 months of life is recognized as the optimal infant feeding strategy by the World Health Organization (WHO) and United Nations Children's Fund (UNICEF). 1 Despite its established benefits for infant health, maternal well-being, and public health systems, global EBF rates remain suboptimal at ∼44%, far below the WHO/UNICEF target of at least 70% by 2030, with projections indicating this target is unlikely to be achieved. 2
Brazil mirrors this global challenge. According to the National Survey on Child Nutrition (ENANI-2019), EBF rate for infants under 6 months increased from 38.6% in 2006 to 45.8% in 2019. However, this remains far from the 70% target, with marked regional and socioeconomic disparities. 3 Analysis of ENANI-2019 data identified previous bottle exposure, infant age, and pacifier use as the strongest factors associated with EBF discontinuation, highlighting the critical 2–4-month period for maintaining breastfeeding support. 4
Pediatricians play a central role in breastfeeding support by providing evidence-based counseling and early identification of lactation problems. 5 However, educational gaps persist across different settings. A national survey of pediatricians in Lebanon revealed significant deficiencies in knowledge, attitudes, and practices regarding breastfeeding support. 6 The International Pediatric Association has emphasized that all pediatricians, regardless of subspecialty, should acquire core competencies in breastfeeding. However, current training programs do not consistently ensure this preparation. 7 A systematic review of breastfeeding skills training found a paucity of educational interventions specifically offering skills-based training, with a lack of standardization in curricula, educator qualifications, and assessment strategies. 8 Furthermore, existing training tends to focus on healthy newborns, with limited preparation for supporting breastfeeding in medically complex children. 9 These training deficits may compromise the quality of clinical counseling and contribute to suboptimal breastfeeding outcomes.
Given this context, understanding the educational needs of physicians providing pediatric care across different career stages may help optimize breastfeeding training programs. This study, conducted by the Scientific Department of Breastfeeding of the Brazilian Society of Pediatrics, aimed to identify distinct professional profiles among physicians providing pediatric care attending the Brazilian Congress of Pediatrics and to characterize their self-reported educational priorities regarding breastfeeding in order to inform continuing education initiatives tailored to the needs of different professional profiles.
Methods
Study design and data source
This cross-sectional study used data from a structured electronic survey conducted during the 41st Brazilian Congress of Pediatrics (Florianópolis, Santa Catarina, Brazil; 22–26 October, 2024), a national event attended by ∼5,500 registered participants from all 27 Brazilian states. The survey was designed by the Scientific Department of Breastfeeding of the Brazilian Society of Pediatrics (SBP) and administered through Google Forms. Participants accessed the questionnaire via a QR code displayed at the SBP booth during all 5 days of the congress. Recruitment was passive: Attendees who visited the booth and expressed interest were invited to participate without active approach and without compensation or incentives. The questionnaire included an electronic informed consent as the only mandatory item; all subsequent items could be skipped by respondents. The questionnaire comprised sections on demographic characteristics, year of medical graduation, year of pediatric specialty certification, clinical practice context, perceived causes of early weaning in routine practice, perceived age of early weaning, and an open-ended question on desired educational topics related to breastfeeding support. The complete instrument is available in the study repository.
The primary aim of the data collection was to identify educational themes desired by pediatricians affiliated with the SBP. The present study is a secondary analysis of the resulting dataset, focused on identifying professional profiles and their associated educational priorities through unsupervised clustering.
Study population and eligibility criteria
Inclusion criteria were defined a priori as physicians attending the 41st Brazilian Congress of Pediatrics who met one of the following criteria: (1) board-certified pediatricians (with a numeric year of pediatric specialty certification); (2) pediatric residents (who reported “Residente” in the certification-year item); or (3) physicians without pediatric specialty certification and without any other medical specialty, who reported providing pediatric care (who reported “Não tem” in the certification-year item). Exclusion criteria were: nonphysicians (including nurses, nutritionists, and other allied health professionals), medical students, and physicians with a specialty other than pediatrics (e.g., obstetrics/gynecology). Eligibility was confirmed through two complementary mechanisms: (1) verbal verification by the research team at the SBP booth before providing the QR code to the prospective participant and (2) self-identification within the questionnaire through the year-of-certification item.
A total of 290 participants completed the survey and were included in the analysis: 164 (56.6%) board-certified pediatricians, 109 (37.6%) pediatric residents, and 17 (5.9%) physicians without pediatric specialty certification and without another specialty—a profile consistent with early-career general practitioners and primary care physicians who provide pediatric care (mean age = 28.1 years; standard deviation [SD] = 3.9; graduated 2018–2024). Professional status was derived post collection from the year-of-certification item and is presented in Table 1. Age, sex, parental status (mother, father, or no children), year of medical graduation, year of pediatric specialty certification, primary areas of clinical practice (up to three options), perceived age of early weaning, and perceived causes of early weaning (up to three options) were also collected. All responses were anonymous, self-reported, and collected between October 22 and 26, 2024.
Sample Characteristics (N = 290)
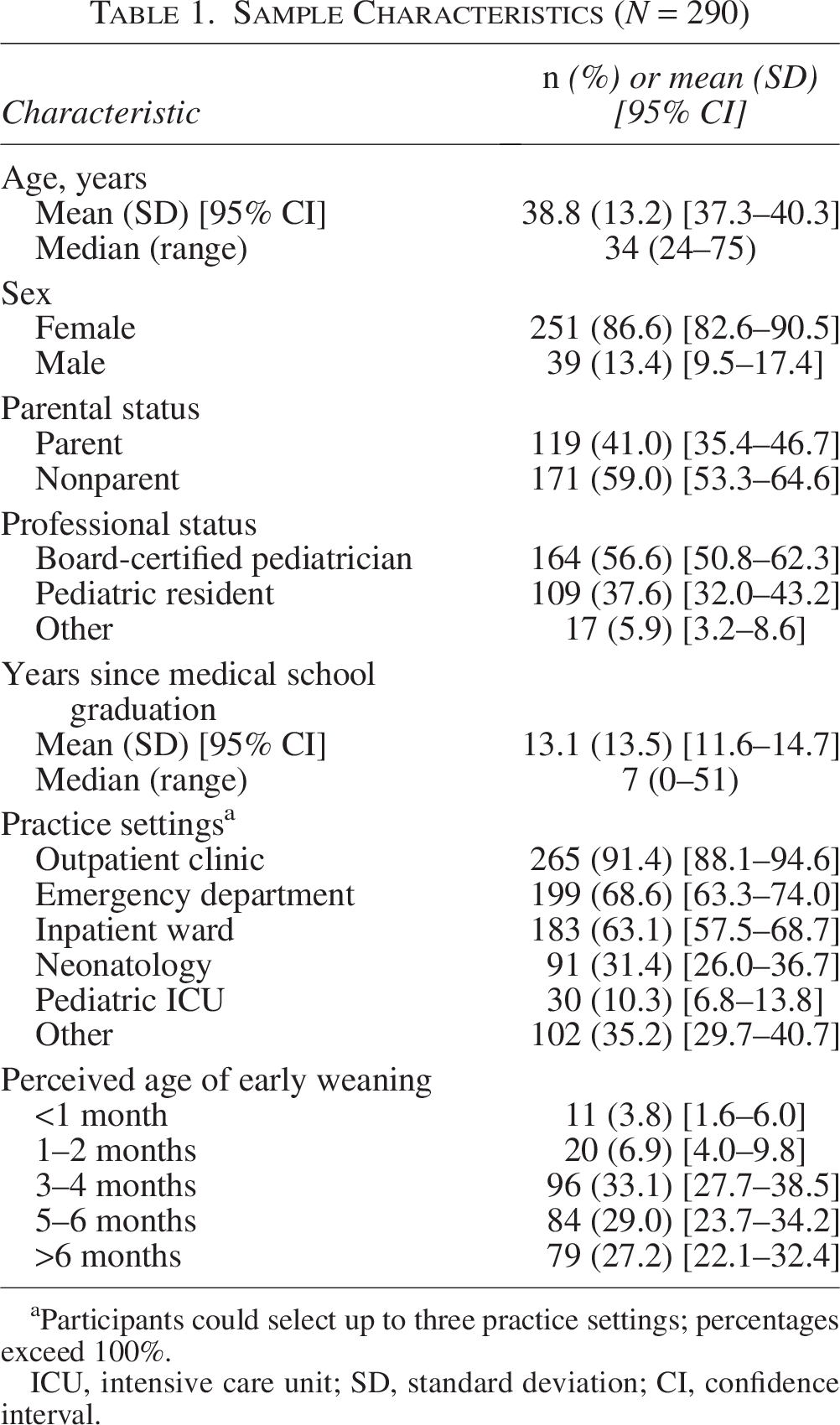
Participants could select up to three practice settings; percentages exceed 100%.
ICU, intensive care unit; SD, standard deviation; CI, confidence interval.
Data processing
Missing data handling
Although only the informed consent item was mandatory in the electronic form, all 290 participants who completed the survey provided responses to every closed-ended item. Therefore, no missing values were present in the variables used for the clustering algorithm. Nonresponse occurred only for the open-ended question on desired educational topics, which was answered by 200 of 290 participants (69.0%). Comparison of responders and nonresponders showed that nonresponse was systematically associated with younger age, more recent medical graduation, resident or noncertified professional status, and practice in emergency or inpatient settings (all p < 0.05, Kruskal–Wallis and chi-square tests). This pattern is consistent with a missing-at-random (MAR) rather than missing-completely-at-random mechanism. Because the clustering analysis relied exclusively on items with complete data, no imputation was required. For the educational topic analysis, complete-case analysis was used. The implications of the observed MAR pattern—particularly for Cluster 1 (early career profile)—are discussed in the section “Discussion.” The audit of missingness, including per-variable counts and the responder/nonresponder comparison, is available in the study repository.
Feature engineering
Multiple-choice variables related to clinical practice context and perceived causes of early weaning were transformed into binary indicators (0 = not selected; 1 = selected) for the clustering analysis. Practice areas were represented by six binary variables (outpatient clinic, emergency department, inpatient ward, neonatology, pediatric intensive care unit, and other). Perceived causes of early weaning were represented by eight binary variables (maternal perception of low milk production, return to work or studies, lack of support network, breastfeeding technique or management issues, nipple fissures or breast complications, lack of knowledge about breastfeeding benefits, concerns about breast aesthetics, and other causes).
Variables reflecting demographic characteristics or career stage (e.g., age, years since graduation, parental status) were intentionally excluded from the clustering algorithm and reserved exclusively for postclustering characterization. This design choice ensured that any observed association between clusters and career stage emerged from the data rather than being imposed by variable selection. Variables included in the clustering analysis were selected a priori based on their relevance to clinical practice context and perceived determinants of early weaning rather than demographic characteristics.
Dimensionality reduction
Multiple correspondence analysis (MCA) was applied to the 14 binary variables to reduce dimensionality while preserving the categorical structure of the data, 10 following previously described methodological approaches for categorical data in health research. 11
Clustering analysis
Sample size justification
As this was an exploratory, hypothesis-generating study using unsupervised clustering, conventional sample size calculations based on hypothesis testing and statistical power were not applicable, as there was no prespecified effect size, null hypothesis, or primary comparison to power. Sample size adequacy for the analytical approach was instead considered in relation to established methodological guidance for the techniques used. For MCA, the sample of 290 participants substantially exceeded common rules of thumb (n ≥ 5 times the number of active variables; here, 14 × 5 = 70). 12 For K-means clustering, the sample met recommendations for stability-based validation of clustering solutions with categorical data. 13 The adequacy of the resulting solution was confirmed post hoc through internal validity indices and bootstrap stability metrics (section “Cluster validation and selection”), which served as the equivalent of power assessment in a confirmatory testing framework. Post hoc statistical power was not computed for the descriptive between-cluster comparisons, as retrospective power analysis is considered uninformative and potentially misleading in contemporary biostatistical literature. 14
K-means clustering and selection of the number of clusters
K-means clustering was performed on the MCA coordinates, testing solutions with K = 2, 3, 4, and 5 clusters. The optimal number of clusters was selected based on statistical performance, stability, parsimony, and clinical interpretability.
Cluster validity was assessed using the following metrics:
Calinski–Harabasz index: measuring between-cluster variance versus within-cluster variance. Silhouette score: evaluating cluster cohesion and separation. Jaccard bootstrap stability: assessing cluster reproducibility across 100 bootstrap resamples. Adjusted Rand Index (ARI): measuring agreement between reference and bootstrap cluster solutions.
The three-cluster solution (K = 3) was selected based on the highest Calinski–Harabasz index, greater stability metrics (Jaccard and ARI), and superior clinical interpretability.
Cluster characterization
After cluster assignment, clusters were characterized using variables not included in the clustering algorithm, including age, sex, parental status, years since graduation, and the perceived age of early weaning in clinical practice. Descriptive statistics were calculated for each cluster.
Statistical comparisons across clusters were performed using the Kruskal–Wallis test for continuous variables and the chi-square test for categorical variables. We acknowledge that formal hypothesis testing of cluster differences has inherent circularity when applied to algorithmically derived groups; therefore, these tests are presented for descriptive completeness rather than confirmatory inference.
Educational topics analysis
Open-ended responses classification
Of the 290 respondents, 200 (69.0%) provided a response to the open-ended question on desired educational topics. Thirteen responses (n = 13) were excluded as noninformative based on prespecified criteria applied independently by both classifiers: (1) empty after whitespace trimming (e.g., “.,” “.,” and “-”); (2) single-word filler responses without any thematic content (e.g., “tudo,” “todos,” and “nada”); or (3) responses explicitly indicating “all topics” without specifying themes. A final set of 187 valid responses was included in the thematic analysis.
Responses were independently classified into 16 thematic categories by two researchers (M.C.S. and F.C.S.). As responses could address multiple topics, each response could be assigned to more than one category. Inter-rater reliability, computed across all 200 classified responses, yielded a Cohen’s kappa of 0.957 (96.0% exact-match agreement; with 8 of 200 responses showing disagreement), indicating near-perfect agreement. All disagreements were resolved by consensus, and the consensus classification was used for the final analysis. The complete annotation dataset (both raters’ independent classifications, consensus decisions, and per-category disagreement details) and the kappa computation script are publicly available in the study repository, enabling independent verification of the classification process.
Normalization for cluster comparison
To allow comparison across clusters with different sample sizes, category frequencies were normalized within each cluster using the following formula:

This normalization ensured that the distribution of educational topics within each cluster summed to 100%, enabling direct comparison regardless of cluster size.
Visualization
Radar (spider) charts were used to visually compare educational topic distributions across clusters. Each axis represented a thematic category, and the distance from the center corresponded to the normalized percentage.
Statistical analysis
All analyses were performed using Python (version 3.x). Data manipulation was conducted using pandas, MCA was performed using the prince library, and K-means clustering and validation metrics were computed using scikit-learn. Visualizations were generated using matplotlib. The complete analytical pipeline, including all scripts and processed data, is publicly available at https://github.com/marcelosilva2604/clusteringeducation. All analyses were exploratory, and no causal inferences were intended.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki. Participation was anonymous and voluntary. Electronic informed consent was obtained from all participants prior to questionnaire completion. The study protocol was approved by the Research Ethics Committee of University of Santo Amaro (CAAE protocol number: 7.067.249).
Results
Sample characteristics
A total of 290 physicians providing pediatric care completed the survey: 164 (56.6%) board-certified pediatricians, 109 (37.6%) pediatric residents, and 17 (5.9%) physicians without pediatric specialty certification. The sample was predominantly female (86.6%, n = 251), with a mean age of 38.8 years (SD = 13.2). Approximately 41.0% of participants (n = 119) reported being parents. The mean year of medical graduation was 2011 (SD = 13.5). Detailed demographic characteristics are presented in Table 1.
Cluster validation and selection
Cluster solutions ranging from K = 2 to K = 5 were evaluated using internal validation and stability metrics. The three-cluster solution presented the highest Calinski–Harabasz Index (71.81) and showed a favorable balance between cluster cohesion and stability (Silhouette score = 0.238; Jaccard bootstrap = 0.801; Adjusted Rand Index = 0.771). The observed Silhouette score is consistent with expected values for clustering of binary survey data, as categorical variables typically yield lower cohesion metrics than continuous measures.13,15
Although slightly higher Silhouette values were observed for K = 4, this solution showed reduced stability and lower parsimony. Considering statistical performance, cluster stability, and clinical interpretability, the three-cluster solution (K = 3) was selected for subsequent analyses. Validation metrics for all tested solutions are summarized in Table 2.
Internal Validation and Stability Metrics for Cluster Solutions (K = 2–5)
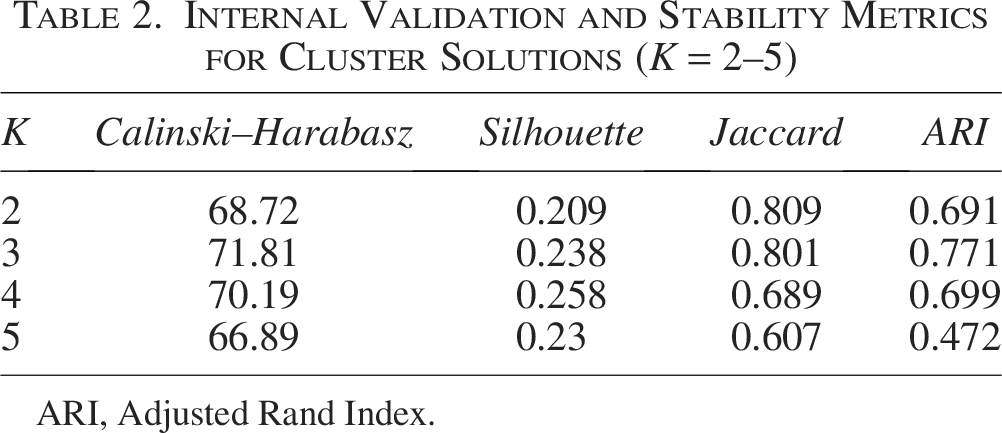
ARI, Adjusted Rand Index.
Cluster characteristics
The three-cluster solution resulted in distinct groups differing in demographic and professional characteristics (Table 3).
Cluster Characteristics
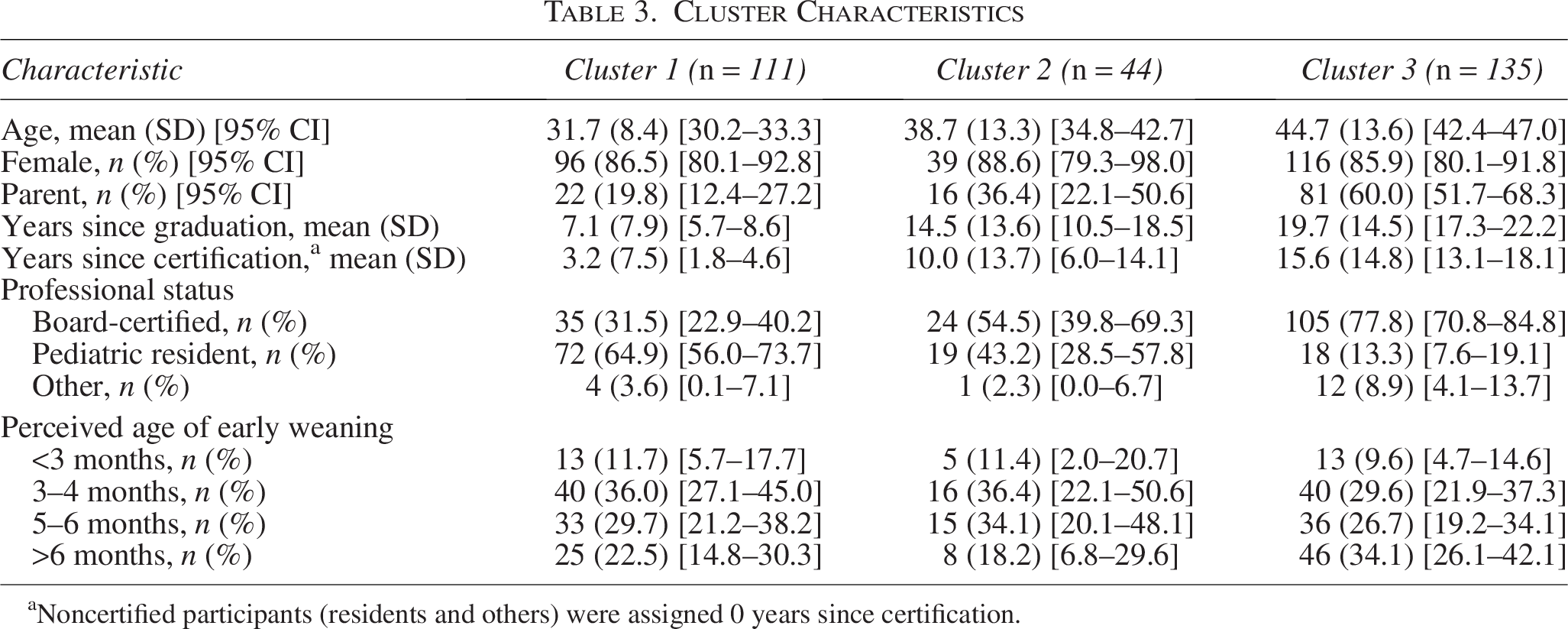
Noncertified participants (residents and others) were assigned 0 years since certification.
Cluster 1 (early-career profile) included 111 participants (38.3%) and was characterized by the lowest mean age (31.7 years, SD = 8.4), the fewest years since graduation (mean = 7.1, SD = 7.9), and the lowest proportion of participants reporting parental status (19.8%, 95% confidence interval [CI]: 12.4–27.2). This cluster had the highest proportion of pediatric residents (64.9%, 95% CI: 56.0–73.7).
Cluster 2 (intermediate profile) comprised 44 participants (15.2%) and presented intermediate values for age (mean = 38.7 years, SD = 13.3), years since graduation (mean = 14.5, SD = 13.6), and parental status (36.4%, 95% CI: 22.1–50.6). Professional status was evenly distributed between board-certified pediatricians (54.5%) and pediatric residents (43.2%).
Cluster 3 (senior profile) included 135 participants (46.6%) and was characterized by the highest mean age (44.7 years, SD = 13.6), the most years since graduation (mean = 19.7, SD = 14.5), and the highest proportion of participants reporting parental status (60.0%, 95% CI: 51.7–68.3). This cluster had the highest proportion of board-certified pediatricians (77.8%, 95% CI: 70.8–84.8).
Clusters differed significantly in age, years since graduation, years since certification, parental status, and professional status (all p < 0.001). Sex distribution and perceived age of early weaning did not differ significantly across clusters (p = 0.900 and p = 0.576, respectively).
Although perceived age of early weaning did not differ significantly across clusters (p = 0.576), descriptive patterns were observed: Cluster 3 showed the highest proportion of participants reporting weaning after 6 months of age (34.1%, 95% CI: 26.1–42.1), compared with Cluster 1 (22.5%, 95% CI: 14.8–30.3) and Cluster 2 (18.2%, 95% CI: 6.8–29.6).
Educational topics identified
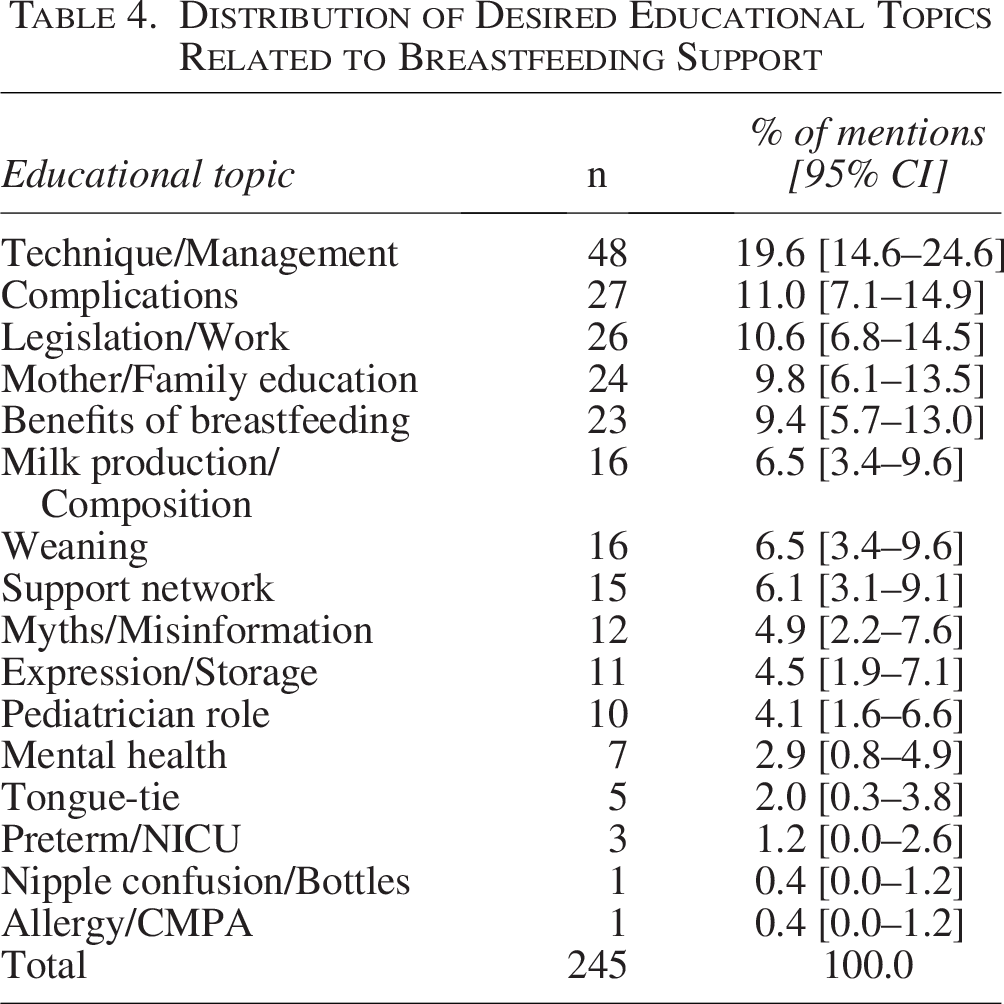
Among the 290 participants, 200 (69.0%) provided responses to the open-ended question regarding desired educational topics related to breastfeeding support. After excluding 13 responses (6.5%) that met prespecified exclusion criteria for noninformativeness (empty or whitespace-only responses; single-word filler such as “tudo,” “todos,” and “nada”; or responses indicating “all topics” without specifying themes), 187 responses were included in the analysis. The identifiers and full text of the 13 excluded responses are available in the study repository. Since responses were open-ended and could address multiple topics, each response was assigned to one or more of 16 thematic categories. A total of 245 category assignments were made across the 187 valid responses (mean = 1.3 categories per response).
The most frequently assigned categories were technique/management (n = 48 mentions, 19.6%), complications related to breastfeeding (n = 27, 11.0%), legislation and work-related issues (n = 26, 10.6%), mother and family education (n = 24, 9.8%), and benefits of breastfeeding (n = 23, 9.4%). Less frequently mentioned topics included mental health (n = 7, 2.9%), tongue-tie (n = 5, 2.0%), preterm/Neonatal Intensive Care Unit (NICU) care (n = 3, 1.2%), nipple confusion/bottle use (n = 1, 0.4%), and allergy/cow's milk protein allergy (CMPA) (n = 1, 0.4%). The complete distribution of educational topics is presented in Table 4.
Distribution of Desired Educational Topics Related to Breastfeeding Support
Educational priorities by cluster
Normalized distributions of educational topics differed across clusters (Fig. 1).
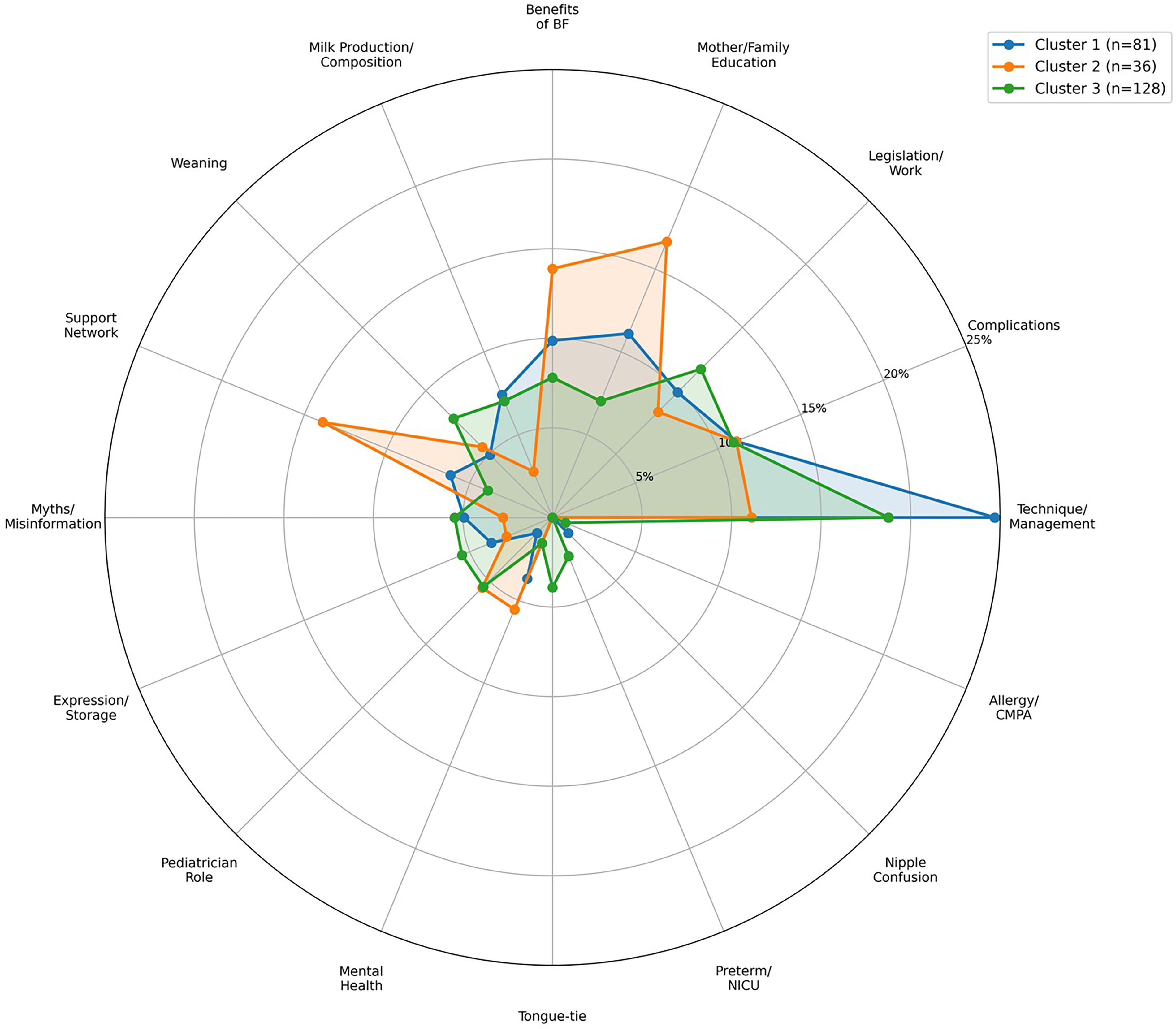
Radar chart comparing normalized distribution of desired educational topics across clusters (% of mentions per cluster).
Cluster 1 (early-career) showed the highest proportion of mentions related to technique/management, with lower relative emphasis on legislation/work and the pediatrician’s role. This pattern suggests that early-career professionals prioritize mastery of fundamental clinical skills.
Cluster 2 (intermediate) showed higher proportions of mentions related to mother/family education and support network compared with the other clusters. This may reflect a transitional phase in which professionals begin integrating clinical skills with broader counseling responsibilities.
Cluster 3 (senior) demonstrated a more distributed pattern of educational priorities, with higher relative proportions of mentions related to legislation/work, myths/misinformation, and the pediatrician’s role. Mentions of preterm/NICU and allergy/CMPA topics were observed exclusively in Cluster 3, potentially reflecting subspecialty interests or accumulated clinical experience with complex cases.
Discussion
This study identified systematic variation in educational priorities regarding breastfeeding support among physicians providing pediatric care, with these priorities aligning with career stage and professional experience. Three distinct profiles emerged, forming a gradient from practical clinical skills among early-career professionals to broader contextual competencies—including advocacy, legislation, and combating misinformation—among senior pediatricians. The emphasis on the pediatrician’s role among senior professionals may reflect a perceived need to reassert the pediatrician as the central coordinator of the breastfeeding support team. The practical applicability of these findings is reinforced by the alignment between the identified profiles and the Scientific Department of Breastfeeding of the Brazilian Society of Pediatrics’ need for evidence-based continuing education planning. Indeed, structured educational programs targeting breastfeeding support have been shown to improve knowledge, self-efficacy, and action competence among health professionals, 16 supporting the rationale for tailored interventions based on identified professional profiles.
Of the participants, 91.4% reported outpatient settings among their practice areas—each respondent could select up to three—where breastfeeding counseling is most frequently delivered, reinforcing the clinical relevance of the educational priorities identified. Within this career-stage gradient, early-career professionals (Cluster 1) prioritized technique and management—the most frequently mentioned educational topic overall—consistent with a training phase focused on acquiring fundamental clinical skills such as latch assessment and positioning. Intermediate-career professionals (Cluster 2) shifted toward mother and family education and support networks, suggesting a transitional stage in which clinical skills begin to integrate with broader counseling responsibilities. Senior pediatricians (Cluster 3) emphasized themes external to immediate clinical practice, including legislation, workplace policies, combating misinformation, and reflection on the pediatrician’s role. Perceived age of early weaning did not differ significantly across clusters (p = 0.576), suggesting that professionals at all career stages observe similar patterns of breastfeeding discontinuation in clinical practice, despite differing in their educational priorities for addressing it. This gradient emerged despite demographic variables being intentionally excluded from the clustering algorithm, indicating that clinical practice context and perceived determinants of early weaning naturally covary with professional experience.
The educational priorities identified across clusters are consistent with existing evidence on gaps in breastfeeding training. The emphasis on technique and management among early-career professionals aligns with evidence that modifiable clinical factors—particularly bottle and pacifier exposure—are strongly associated with EBF discontinuation in Brazilian infants. 4 However, despite this evidence, nipple confusion and bottle use was mentioned by only one participant as desired educational topics, highlighting a discrepancy between the strength of the epidemiological association and the low demand for education on this topic among surveyed professionals. This finding is particularly relevant given that surveys show pediatric residents receive a median of only 9 hours of breastfeeding education over 3 years of residency, with most program directors considering this insufficient. 17 Residents also report low confidence in fundamental skills such as latch assessment and the management of common complications. 18 A national survey of primary care professionals in Ireland similarly found inadequate preparation for breastfeeding support, with 94.2% expressing interest in further education. 19 The shift toward counseling and family education observed in Cluster 2 reflects the broader scope of breastfeeding support increasingly recommended for pediatricians, including behavioral counseling interventions delivered across multiple contacts and tailored to individual family needs. 20 The emphasis on the central pediatrician’s role and legislation among senior professionals in Cluster 3 is consistent with the International Pediatric Association’s position that all pediatricians should acquire competencies beyond clinical management, encompassing policy engagement and the protection of breastfeeding at the societal level. 7
Our findings are consistent with a broader evidence base highlighting persistent gaps in physician breastfeeding education across multiple healthcare systems. A landscape analysis of breastfeeding-related physician education in the United States documented that training remains inadequate despite previous efforts, with physicians expressing a desire for more education, particularly in clinical skills. 21 Similar learning needs have been reported among family physicians, pediatricians, and obstetricians in Canada, where respondents identified clinical management of breastfeeding problems and communication skills as priority areas. 22 The differentiation of educational needs by career stage observed in our study suggests that standardized, one-size-fits-all curricula may inadequately address the spectrum of practitioner priorities. This is consistent with the framework proposed by Taylor and Bell, which emphasizes that breastfeeding education should be multifaceted, combining didactic curricula with clinical experiences and nonclinical opportunities in teaching, research, and advocacy across the professional lifespan. 23 Tailoring educational content accordingly—incorporating interactive, skills-based modules for trainees alongside broader policy, counseling, and advocacy competencies for experienced clinicians—could strengthen the quality of breastfeeding support and align with current recommendations for comprehensive physician training in this area.5,7 Although conducted in Brazil, the observed career-stage gradient likely reflects broader patterns in physician professional development, given that similar educational gaps have been documented across diverse healthcare systems.21,22
These findings suggest a framework for career-stage-tailored breastfeeding education. Residency programs could prioritize hands-on, skills-based training in latch assessment, positioning, and the management of common complications. Continuing education for mid-career pediatricians could incorporate counseling techniques and strategies for engaging families and support networks. For senior practitioners, educational offerings could expand beyond clinical content to include breastfeeding legislation, workplace policy advocacy, and the management of breastfeeding in medically complex populations such as preterm infants and children with cow’s milk protein allergy. The recent recognition of breastfeeding and lactation medicine as an emerging subspecialty, with providers acting as clinicians, advocates, researchers, and educators, further supports the need for comprehensive training that extends beyond clinical skills at every career stage. 24 Given the impact of breastfeeding on public health outcomes, increasing the overall exposure of health professionals to breastfeeding education across all career stages is essential. However, beyond expanding training broadly, our findings indicate that educational strategies should also address the specific needs identified at each stage of professional development, thereby maximizing the relevance and effectiveness of continuing education initiatives.
Strengths of this study include: (1) a nationally relevant sample collected during a major pediatric congress attended by professionals from all 27 Brazilian federative units, broadening the geographic scope of the analysis beyond a single institution; (2) a deliberate analytical design that excluded demographic variables from the clustering algorithm, ensuring that the observed career-stage gradient emerged from the data rather than being imposed by variable selection; (3) independent dual manual classification of open-ended responses with near-perfect inter-rater agreement (Cohen’s κ = 0.957), reducing subjective bias in thematic assignment; and (4) a fully reproducible analytical pipeline, with all scripts, processed datasets, and validation artifacts publicly available in the study repository for independent verification.
Limitations should also be acknowledged. The sample was recruited by convenience at a professional congress through a passively advertised QR code. Participants who visited the SBP booth may differ systematically from nonattendees or from congress participants who did not visit the booth, potentially overrepresenting professionals already engaged in breastfeeding advocacy. Eligibility was verified through verbal triage at the booth and through self-identification within the questionnaire; no programmatic filter prevented enrollment of physicians from other specialties, and this reliance on self-report is a source of residual misclassification risk. Nonresponse to the open-ended question (31.0%) was associated with younger age, more recent graduation, resident or noncertified professional status, and practice in emergency or inpatient settings—a missing-at-random pattern that, while consistent with and reinforcing the main career-stage gradient, may attenuate the capture of early-career perspectives and should temper interpretation of Cluster 1 educational priorities. The cross-sectional design precludes causal inferences, and the observed cluster differences may reflect career-stage effects, cohort effects, or unmeasured confounding. The relatively small size of Cluster 2 (n = 44) warrants caution when interpreting the intermediate profile. Moderate Silhouette scores indicate some overlap between clusters, which is expected in survey-based behavioral data; however, bootstrap stability metrics (Jaccard = 0.801; ARI = 0.771) demonstrated adequate reproducibility. Finally, classification of open-ended responses, while conducted independently by two researchers and reconciled by consensus, retains an element of subjective judgment.
Conclusion
Three distinct professional profiles with differing educational priorities in breastfeeding support were identified among physicians providing pediatric care at the Brazilian Congress of Pediatrics. Educational needs followed a career-stage gradient, ranging from practical clinical skills among early-career professionals to leadership, coordination, and policy competencies among senior pediatricians. The emphasis on the pediatrician’s role among senior professionals underscores a perceived need to reassert the pediatrician as the central coordinator of the breastfeeding support team. These findings support the development of career-stage-tailored educational strategies to maximize the relevance and effectiveness of continuing education initiatives. Future research could evaluate whether targeted interventions based on these profiles improve clinical competence and breastfeeding outcomes.
Authors’ Contributions
M.C.S.: Methodology, software, data curation, investigation, formal analysis, validation, visualization, and writing—original draft and review and editing. L.C.G.: Conceptualization, data curation, formal analysis, investigation, resources, supervision, project administration, and writing—original draft and review and editing. D.D.W.: Data curation and writing—review and editing. R.P., E.F.P., I.M.D.L., L.M.N., L.M.O.R., D.F.F., R.S.S., S.S.R., and V.M.S.F.: Investigation and writing—review and editing. P.L.C.S. and F.C.S.: Data curation, methodology, and writing—review and editing. All authors reviewed and approved the final article.
Footnotes
Acknowledgments
The authors thank all physicians who voluntarily participated in this study during the Brazilian Congress of Pediatrics.
Data Availability Statement
Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.