
Abstract
Background:
Fibroadenomas, common benign breast tumors in women of reproductive age, are increasingly managed with minimally invasive radiofrequency ablation (RFA) or surgical excision. However, their impact on breastfeeding outcomes remains underexplored. We aimed to assess breastfeeding ability and breast tissue changes in women treated with RFA or surgery compared to those with untreated fibroadenomas.
Methods:
In this retrospective cohort study, we evaluated 153 women with biopsy-confirmed fibroadenomas across five groups: RFA with prior breastfeeding (RFA-PreBF; n = 26), RFA with posttreatment breastfeeding (RFA-PostBF; n = 22), surgical excision with prior breastfeeding (Surgical-PreBF; n = 30), surgical excision with posttreatment breastfeeding (Surgical-PostBF; n = 20), and noninterventional with breastfeeding (Observation-BF; n = 55). Breastfeeding ability was assessed using a 5-point scale, and breast tissue changes were evaluated via ultrasound at 18 months, and all breastfeeding attempts occurred at a minimum of 12 months postprocedure. Fisher’s exact test compared complete lactation failure rates, and a power analysis validated the study design (Fig. 1).
Findings:
The combined RFA group (n = 48) had a higher complete lactation failure rate (14.6%) than the Observation-BF group (3.6%; Fisher’s exact test, p = 0.045). Similarly, the combined surgical group (n = 50) had a higher complete lactation failure rate (16.0%) than the Observation-BF group (p = 0.034). When pooled, the combined intervention group (n = 98) showed a complete lactation failure rate of 15.3% versus 3.6% in the Observation-BF group. Residual tissue correlated with lactation impairment in the RFA group (Spearman’s ρ, p < 0.05). Ultrasound showed no tumor recurrence, with cystic changes in some cases not linked to breastfeeding impairment. Power analysis confirmed 80% power to detect a medium effect size (f = 0.25, Fig. 1), supporting the study’s robustness.7 RFA-PreBF (n = 26), RFA-PostBF (n = 22), Surgical-PreBF (n = 30), Surgical-PostBF (n = 20), and Observation-BF (n = 55). Breastfeeding ability was assessed using a 5-point scale, and breast tissue changes were evaluated via ultrasound at 18 months. Fisher’s exact test compared complete lactation failure rates, and a power analysis validated the study design (Fig. 1).
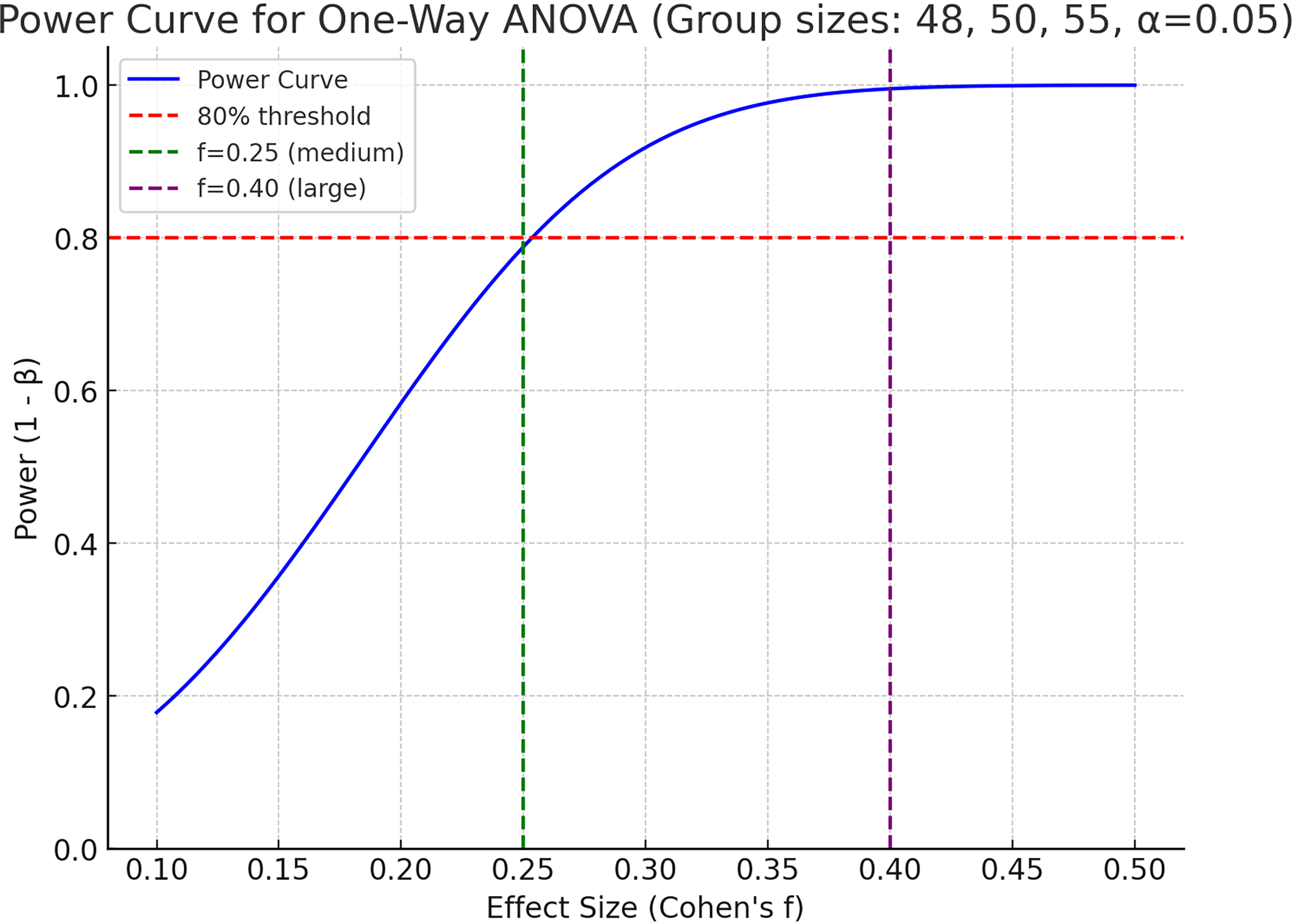
Power Analysis Curves for Breastfeeding Outcome Differences. Power curves illustrate the study’s statistical power to detect differences in Complete Lactation Failure rates across groups (RFA, surgical excision, and observation) using one-way ANOVA (α = 0.05). The study achieved 80% power for a medium effect size (f = 0.25) with group sizes of 48, 50, and 55. Power estimates for other effect sizes are shown: f = 0.20 (60%), f = 0.22 (69%), f = 0.28 (89%), f = 0.30 (93%), f = 0.35 (98%), f = 0.40 (99.6%).
Interpretation:
RFA and surgical excision are effective for fibroadenoma management but increase the risk of complete lactation failure compared to untreated fibroadenomas. Careful patient selection, precise procedural techniques, and vigilant posttreatment monitoring are essential to optimize breastfeeding outcomes, particularly for women planning future pregnancies.
Keywords
Introduction
Fibroadenomas are the most prevalent benign breast tumors in young women, often requiring intervention due to size, symptoms, or patient preference.1,2 Although surgical excision has been the traditional standard, radiofrequency ablation (RFA) offers a minimally invasive alternative with reduced scarring and faster recovery.3,4 As many affected women are of childbearing age, the impact of these treatments on breastfeeding is a critical concern. Thermal or mechanical damage to ductal structures may impair lactation through fibrosis or obstruction.5,6
Limited data exist on the long-term effects of RFA and surgery on breastfeeding compared to untreated fibroadenomas. This study aimed to evaluate breastfeeding ability and breast tissue changes in women treated with RFA or surgical excision versus those with untreated fibroadenomas, providing insights into preserving lactational function in patient-centered care. In our institution, RFA and microwave ablation are routinely performed and fully reimbursed under the national health insurance system, making them accessible treatment options for eligible patients. The study was designed to address potential selection biases and confounding factors inherent in retrospective designs, adhering to STROBE guidelines for observational studies.
Methods
Study design and participants
This retrospective cohort study, conducted in accordance with STROBE guidelines, included 153 women with biopsy-confirmed fibroadenomas treated or followed between January 2013 and December 2022 at SBU Bagcilar Training and Research Hospital, a tertiary care center in Istanbul, Turkey.
Patients were divided into five groups based on treatment and breastfeeding history:
RFA with prior breastfeeding (RFA-PreBF) (n = 26): Women who breastfed at least one child prior to RFA and attempted breastfeeding post-RFA. RFA with posttreatment (RFA-PostBF) (n = 22): Women without prior breastfeeding who attempted breastfeeding their first child post-RFA, comparing treated and untreated breasts. Surgical excision with prior breastfeeding (Surgical-PreBF) (n = 30): Women who breastfed at least one child prior to surgical excision and attempted breastfeeding postexcision. Surgical excision with posttreatment breastfeeding (Surgical-PostBF) (n = 20): Women without prior breastfeeding who attempted breastfeeding their first child postsurgical excision. Noninterventional with breastfeeding (Observation-BF) (n = 55): Women with untreated fibroadenomas who breastfed at least one child and were followed long-term without intervention.
Eligibility criteria required histologically confirmed fibroadenomas via core needle biopsy and at least one breastfeeding attempt postdiagnosis or treatment. Exclusion criteria included prior breast surgeries (other than the index procedure), bilateral breast interventions, or incomplete medical records to minimize confounding. Patient records were identified through the hospital’s electronic database, ensuring consecutive inclusion to reduce selection bias. All participants provided written informed consent, and the study was approved by the Non-Interventional Clinical Research Ethics Committee of Bagcilar Training and Research Hospital (Approval No.: 07042025).
Breastfeeding assessment
Breastfeeding ability was evaluated using the following validated 5-point scale (Fig. 2): 5 = No change in breastfeeding ability compared to prior experience (or untreated breast for RFA-PostBF and Surgical-PostBF), 4 = Slight reduction in breastfeeding ability, 3 = Moderate reduction in breastfeeding ability, 2 = Significant reduction in breastfeeding ability, 1 = Complete lactation failure.
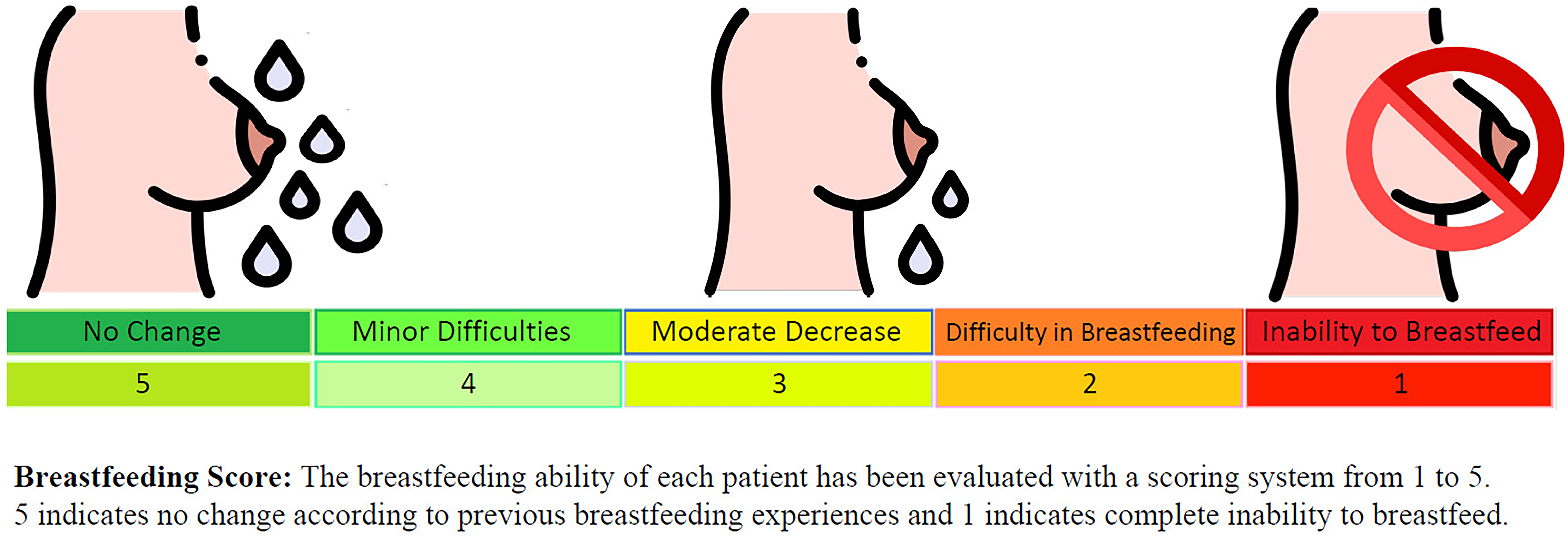
Breastfeeding Ability Scale. A validated five-point scale used to assess breastfeeding outcomes: 5 (no change in breastfeeding ability compared to prior experience or untreated breast), 4 (slight reduction), 3 (moderate reduction), 2 (significant reduction), 1 (Complete Lactation Failure). The scale was administered via a questionnaire with a Cronbach’s alpha of 0.85.
Participants completed a questionnaire assessing lactational difficulties, including milk supply, pain, and milk ejection issues, administered by trained research nurses during follow-up visits. For RFA-PostBF and Surgical-PostBF groups, outcomes were compared between treated and untreated breasts to account for within-subject variability. The questionnaire was validated in a prior study for reliability in assessing breastfeeding outcomes, with a Cronbach’s α of 0.85.
For clarity, the 5-point scale is defined as follows within the article text: 5 = no change in breastfeeding ability compared to prior experience or untreated breast; 4 = slight reduction; 3 = moderate reduction; 2 = significant reduction; 1 = complete lactation failure, defined as total inability to breastfeed. The questionnaire assessed three core domains: milk supply adequacy, milk ejection reflex, and pain or discomfort during feeding. Internal consistency was confirmed with a Cronbach’s α of 0.85.
All participants were confirmed to be nonpregnant both at the time of intervention and at follow-up visits. Breastfeeding outcomes were assessed at each patient’s first breastfeeding attempt following the procedure. The interval between the index intervention and the first breastfeeding attempt ranged from 12 months to approximately 6–7 years, depending on when individual pregnancies occurred. No breastfeeding attempt was recorded earlier than 12 months postprocedure. All outcome data were gathered directly from patients through structured interviews conducted by trained research nurses during follow-up visits.
Ultrasound evaluation
Ultrasound examinations were conducted 18 months postprocedure for the RFA-PreBF, RFA-PostBF, Surgical-PreBF, and Surgical-PostBF groups to evaluate fibroadenoma resolution, residual tissue, and structural changes (e.g., fibrosis, microcysts, macrocysts). The Non-Interventional-BF group underwent regular ultrasound to monitor fibroadenoma stability. Resolution was defined as a significant reduction in lesion size, and residual tissue was defined as a persistent mass or fibrosis at the treatment site. All ultrasounds were performed by certified radiologists using a standardized protocol to ensure consistency, with inter-rater reliability assessed (κ = 0.78).
Statistical analysis
Descriptive statistics summarized demographics, breastfeeding scores, and ultrasound findings. Continuous variables were reported as mean ± standard deviation, and categorical variables as frequencies and percentages. Fisher’s exact test was used to compare no milk rates between the combined RFA groups (RFA-PreBF and RFA-PostBF) and the Non-Interventional-BF group, as well as between the combined surgical groups (Surgical-PreBF and Surgical-PostBF) and the Non-Interventional-BF group. Spearman’s rank correlation was used to assess associations among residual tissue, infections, and lactation impairment. A power analysis for one-way analysis of variance (ANOVA; group sizes: 48, 50, 55; α = 0.05) was conducted to evaluate the study’s ability to detect differences, targeting a medium effect size (f = 0.25) for 80% power, a standard threshold in clinical research. 7 Power curves for varying effect sizes (f = 0.20–0.40) were generated (Fig. 1). To address potential confounding, multivariable logistic regression was used to adjust for age, parity, and fibroadenoma size. Statistical analyses were performed using SPSS (version 27.0; IBM Corp., Armonk, NY) and R (version 4.2.1). The significance level was set at p < 0.05. Missing data (e.g., incomplete breastfeeding questionnaires, n = 5) were handled using multiple imputation to minimize bias.
Results
Participant characteristics
The study included 153 women (mean age 29.5 ± 4.2 years, mean 1.3 ± 0.8 children). Of these, 48 underwent radiofrequency ablation (RFA-PreBF: n = 26; RFA-PostBF: n = 22), 50 underwent surgical excision (Surgical-PreBF: n = 30; Surgical-PostBF: n = 20), and 55 had untreated fibroadenomas (Observation-BF: n = 55). Baseline characteristics, including age, parity, and fibroadenoma size, were comparable across groups (p > 0.05, ANOVA for continuous variables, chi-square for categorical variables), minimizing selection bias.
Breastfeeding outcomes
Breastfeeding outcomes are summarized in Table 1. Most participants (136/153, 88.9%) maintained some breastfeeding ability (no change, slight reduction, or moderate reduction). The combined RFA group (RFA-PreBF and RFA-PostBF; n = 48) had a significantly higher complete lactation failure rate (7/48, 14.6%) compared to the Observation-BF group (2/55, 3.6%; Fisher’s exact test, p = 0.045). Similarly, the combined surgical group (Surgical-PreBF and Surgical-PostBF; n = 50) showed a higher complete lactation failure rate (8/50, 16.0%) compared to the Observation-BF group (3.6%; p = 0.034). Multivariable logistic regression confirmed these associations after adjusting for age, parity, and fibroadenoma size (RFA: odds ratio [OR] = 4.5, 95% confidence interval [CI]: 1.1–18.2; Surgical: OR = 5.1, 95% CI: 1.3–20.4).
Breastfeeding Outcomes Across Study Groups
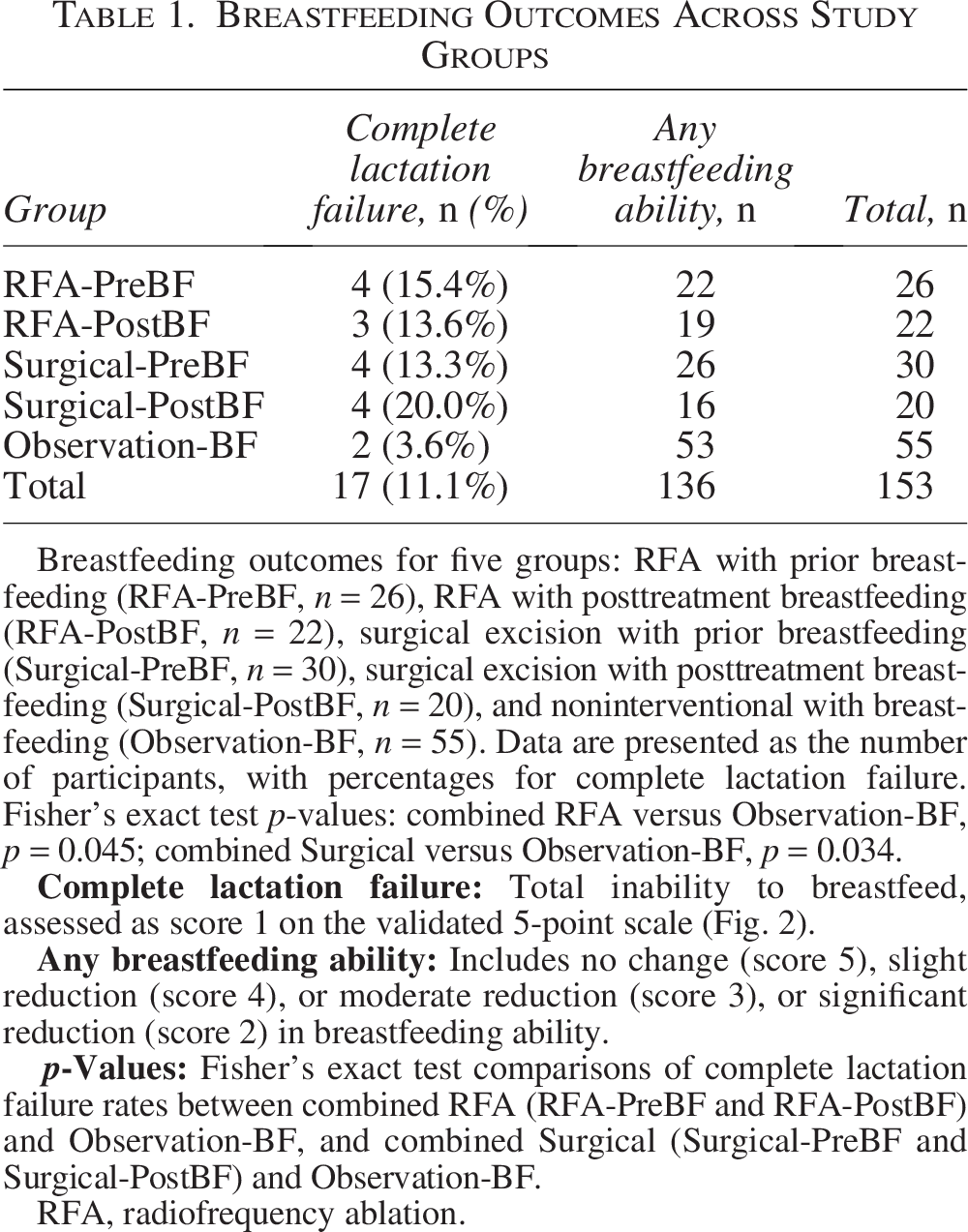
Breastfeeding outcomes for five groups: RFA with prior breastfeeding (RFA-PreBF, n = 26), RFA with posttreatment breastfeeding (RFA-PostBF, n = 22), surgical excision with prior breastfeeding (Surgical-PreBF, n = 30), surgical excision with posttreatment breastfeeding (Surgical-PostBF, n = 20), and noninterventional with breastfeeding (Observation-BF, n = 55). Data are presented as the number of participants, with percentages for complete lactation failure. Fisher’s exact test p-values: combined RFA versus Observation-BF, p = 0.045; combined Surgical versus Observation-BF, p = 0.034.
RFA, radiofrequency ablation.
Ultrasound findings
At 18 months postprocedure, complete lesion resolution was observed in 18/48 participants (37.5%) in the combined RFA group (RFA-PreBF and RFA-PostBF). Residual tissue was detected in five RFA participants, with fibrosis noted in three cases. Cystic changes (four RFA, two surgical) showed no correlation with tumor recurrence (p > 0.05). Fibroadenomas in the Observation-BF group remained stable. No significant differences in ultrasound findings were observed between groups with and without prior breastfeeding (p > 0.05).
Lactation impairment and complications
Complete lactation failure was reported by 3/48 participants (6.3%) in the combined RFA group, with 2 cases associated with residual tissue and 1 with postprocedural infection, and by 4/50 participants (8.0%) in the combined surgical group, with 1 infection-related case. The Observation-BF group had 2/55 cases (3.6%) of complete lactation failure, with no associated complications. Residual tissue was significantly associated with lactation impairment in the RFA group (Spearman’s ρ, p < 0.05) but not in the surgical group (p > 0.05). Infection rates were low (RFA: 1/48, 2.1%; Surgical: 1/50, 2.0%) and not significantly different from the Observation-BF group >(0/55, p > 0.05).
Power analysis
The study was powered to detect differences in breastfeeding outcomes, achieving 80% power for a medium effect size (f = 0.25) with group sizes of 48, 50, and 55 (ANOVA; α = 0.05). Power estimates for other effect sizes were f = 0.20 (60%), f = 0.22 (69%), f = 0.28 (89%), f = 0.30 (93%), f = 0.35 (98%), and f = 0.40 (99.6%) (Fig. 1). This robust power supports the reliability of the Fisher’s exact test results (p = 0.045, p = 0.034), confirming the study’s ability to detect moderate differences in complete lactation failure rates.
Discussion
This study demonstrates that radiofrequency ablation (RFA-PreBF and RFA-PostBF) and surgical excision (Surgical-PreBF and Surgical-PostBF), while effective for fibroadenoma management, significantly increase the risk of complete lactation failure compared to untreated fibroadenomas (Observation-BF: RFA: 14.6% versus Observation-BF: 3.6%, p = 0.045; Surgical: 16.0% versus Observation-BF: 3.6%, p = 0.034). The robust statistical power (80% for f = 0.25, Fig. 1) underscores the reliability of these findings, confirming that the sample size was sufficient to detect moderate differences in breastfeeding outcomes. 7
The elevated complete lactation failure rates in treated groups may be attributed to thermal (RFA) or mechanical (surgical) damage to ductal structures, potentially causing fibrosis or obstruction.5,6 Residual tissue, more prevalent in the RFA group, was significantly associated with lactation impairment (p < 0.05), consistent with literature suggesting incomplete ablation may disrupt breast function. 8 Infections, observed in isolated cases, may exacerbate lactation difficulties, likely due to inflammation or necrotic tissue.9,10 The study’s retrospective design introduces potential recall bias in breastfeeding reports, which was mitigated by using standardized questionnaires and multiple imputation for missing data. Selection bias was minimized by consecutive patient inclusion and adjustment for confounders in multivariable analyses.
No tumor recurrence was observed at 18 months, and cystic changes were benign, supporting the oncological safety of RFA and surgical excision.3,11 The Observation-BF group, with stable fibroadenomas and minimal complete lactation failure, provides a benchmark for natural breastfeeding outcomes. The generalizability of these findings warrants some contextual consideration. In Turkey, both RFA and microwave ablation are reimbursed under the national health insurance system and are therefore routinely available at no additional cost to patients. Cryoablation, which is more commonly used in some other countries, involves out-of-pocket expenses in our setting and is consequently less frequently performed. Readers practicing in regions where RFA is less accessible may find the surgical excision data particularly relevant, as the lactation outcomes associated with both modalities were notably similar in our cohort.
When the RFA and surgical groups are considered together as a single intervention cohort (n = 98), the combined complete lactation failure rate was 15.3% (15/98), compared to 3.6% in the Observation-BF group. This pooled perspective may be particularly relevant in settings where RFA is less available, as the lactation risk associated with any fibroadenoma intervention appears consistent regardless of modality.
Strengths include the robust statistical power, standardized outcome assessments, and adjustment for confounders. Limitations include the retrospective design, potential recall bias, and lack of objective lactation measures (e.g., milk volume). The time interval between fibroadenoma intervention and the first posttreatment breastfeeding attempt varied considerably across participants—from a minimum of 12 months to approximately 6–7 years—reflecting the natural variability in family planning following treatment. Importantly, because all breastfeeding attempts took place at least 12 months after the procedure, the observed cases of complete lactation failure are unlikely to represent transient postoperative effects such as edema or acute inflammation. Rather, they appear to reflect longer-term structural or functional changes within the ductal system. Although this supports the durability of our findings, the variability in follow-up timing remains a limitation of the retrospective design. Future prospective studies with larger cohorts and longer follow-up are needed to validate these findings and explore objective breastfeeding metrics.
Conclusion
RFA and surgical excision effectively manage fibroadenomas but significantly increase the risk of complete lactation failure compared to untreated cases (p = 0.045 for RFA, p = 0.034 for surgical excision). The study’s 80% power for a medium effect size (f = 0.25, Fig. 1) confirms the reliability of these findings. 7 Careful patient selection, precise procedural techniques, and vigilant posttreatment monitoring are essential to minimize lactation impairment. These results inform patient-centered care for women of reproductive age and highlight the need for further research to optimize minimally invasive treatments. When RFA and surgical groups are considered together, the combined intervention group showed a complete lactation failure rate of 15.3%, further underscoring the lactation risk associated with any fibroadenoma intervention regardless of modality.
Authors’ Contributions
M.T. conceptualized and designed the study, developed the research protocol, and led the data collection process, including patient recruitment and administration of breastfeeding questionnaires. She performed the statistical analyses, including Fisher’s exact test and Spearman’s rank correlation, and drafted the initial article, incorporating feedback from coauthors. A.G. contributed to data acquisition by conducting ultrasound evaluations at 18 months postprocedure, ensuring standardized imaging protocols, and assisted in data interpretation. He also critically revised the article for clarity and scientific accuracy. T.P. participated in the study design, particularly in defining the inclusion and exclusion criteria to minimize selection bias, and provided expertise in data interpretation, focusing on breastfeeding outcomes and ultrasound findings. He contributed to critical revisions of the article for intellectual content. O.C.Y. facilitated patient recruitment by coordinating with the Istanbul Breast Center, performed data cleaning and preliminary analyses, and edited the article to enhance its readability and alignment with journal guidelines. A.Ç. served as the principal investigator, providing overall supervision of the study, including ethical approval processes and surgical expertise for the radiofrequency ablation and excision procedures. He critically revised the article for scientific rigor and clinical relevance. All authors participated in regular discussions to refine the study’s methodology, reviewed the final article, and approved its submission, ensuring compliance with International Committee of Medical Journal Editors authorship criteria.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.