
Abstract
Background:
Exclusive breastfeeding (EBF) provides health benefits, yet its continuation remains limited. Maternal endocrine disorders, including gestational hypothyroidism, may impair lactogenesis through hormonal dysregulation; however, evidence regarding the association between gestational hypothyroidism and breastfeeding outcomes remains limited.
Objective:
To investigate the association between maternal gestational hypothyroidism and breastfeeding outcomes in term infants, with a focus on EBF at the end of the first month and formula-free breast milk feeding at 6 months.
Methods:
This retrospective matched case–control study compared term infants of mothers with gestational hypothyroidism treated with levothyroxine (n = 103) and matched controls (n = 103). Feeding data were obtained from medical records and 6-month telephone follow-up, and factors associated with early formula supplementation were analyzed using multivariable logistic regression.
Results:
EBF rates were significantly lower in the case group at 1 month (58.3% versus 81.6%, p < 0.001). Formula supplementation within the first postnatal day was more frequent in the case group than in controls (46.6% versus 21.4%; χ2 = 14.63, p < 0.001). At 6 months, formula feeding—either alone or combined with breastfeeding and/or complementary foods—was significantly more frequent in the case group (45.6% versus 25.2%, p = 0.003). Among infants who ever received formula (n = 84), formula was initiated during the first postnatal month more frequently in the case group (82.7% versus 59.4%, p = 0.018), with earlier mean age at formula initiation (1.4 ± 0.97 versus 2.3 ± 1.51 months, p = 0.003). Multivariable logistic regression showed that higher maternal gravidity was independently associated with early formula supplementation (odds ratio = 3.16; 95% confidence interval: 1.09–9.10; p = 0.033).
Conclusions:
Gestational hypothyroidism was associated with lower EBF rates at 1 month and increased early formula supplementation. These findings underscore the need for targeted lactation support and careful postpartum follow-up in mothers with gestational hypothyroidism.
Keywords
Introduction
Breast milk is the natural source of nutrition for infants, and breastfeeding is a cornerstone of maternal and child health, conferring substantial short- and long-term benefits for both mother and infant.1,2 The World Health Organization, the United Nations Children’s Fund (UNICEF), and the American Academy of Pediatrics recommend exclusive breastfeeding (EBF) for the first 6 months of life, followed by continued breastfeeding alongside appropriate complementary foods.1,3,4 Despite these well-established benefits, global EBF rates remain suboptimal, and breastfeeding continuation declines over time due to multiple barriers, including perceived insufficient milk supply, maternal discomfort, return to work, and inadequate support.2,5
In Turkey, breastfeeding initiation is common; however, EBF declines substantially during the first months of life. According to UNICEF country data, early initiation of breastfeeding in Turkey is reported as 71%, and EBF among infants aged 0–5 months is reported as 41%. 6 Similarly, the 2018 Türkiye Demographic and Health Survey reported that approximately 40.7% of infants under 6 months of age were exclusively breastfed, with a decline from 59% among infants aged 0–1 months to 45% among those aged 2–3 months and 14% among those aged 4–5 months. 7 This early decline underscores the importance of identifying clinical factors that may contribute to early formula introduction.
Beyond sociodemographic and psychosocial factors, maternal health conditions also play an important role in breastfeeding success. Delayed lactogenesis, perceived insufficient milk supply, and maternal metabolic or endocrine conditions have been associated with early breastfeeding difficulties and shorter breastfeeding duration.5,8 Evidence from studies on diabetes in pregnancy further supports the concept that maternal endocrine disturbances may adversely affect milk production and breastfeeding continuation. 9
With a rising prevalence, gestational hypothyroidism (affecting 2–5% of pregnancies) constitutes a significant endocrine disorder with direct implications for lactation.10,11 The condition disrupts the endocrine milieu critical for mammogenesis and lactogenesis, wherein thyroid hormones are indispensable for mammary gland development, alveolar differentiation, and secretory activation.12,13 Dysregulation impairs prolactin signaling and mammary epithelial cell function, leading to a delayed onset of lactogenesis II.8,12,14 This physiological disruption extends to impaired neuroendocrine reflexes, such as oxytocin release, resulting in suboptimal milk ejection. 12 Furthermore, inadequately treated hypothyroidism may compound these challenges by contributing to maternal fatigue and depressive symptomatology, creating additional barriers to effective breastfeeding initiation and persistence.5,14
Although these biological and psychosocial mechanisms provide a plausible link between hypothyroidism and impaired lactation, controlled evidence specifically addressing EBF rates and formula supplementation patterns among mothers with gestational hypothyroidism remains limited. Therefore, this study aimed to investigate the association between maternal gestational hypothyroidism and breastfeeding outcomes in term infants, specifically EBF rates at 1 month and continued breast milk feeding without formula at 6 months postnatally.
Methods
Study design and setting
This retrospective matched case–control study was conducted at Sancaktepe Şehit Prof. Dr. İlhan Varank Training and Research Hospital, Istanbul, Turkey, a tertiary-care training and research hospital serving a large urban population and providing obstetric and neonatal care. The clinical data analyzed in this study were routinely recorded during standard obstetric and neonatal care between June 1, 2024, and December 30, 2024, and were not collected for research purposes at the time of documentation. Ethical approval was obtained from the local institutional ethics committee before research-related data extraction and statistical analysis were performed (Approval No: 2025/309; September 10, 2025). The ethical approval covered the retrospective use and analysis of routinely collected clinical data, as well as follow-up telephone contacts conducted solely for data verification. Due to the retrospective and minimal-risk nature of the study, the requirement for informed consent was waived by the ethics committee.
Participants
The study comprised mother–infant dyads that included mothers with singleton, full-term infants (gestational age >37 weeks, birth weight between the 10th and 90th percentiles) born at the study center, with eligible infants defined as those without postnatal complications, an Apgar score >7 at 5 minutes, rooming-in with their mothers after birth, and otherwise healthy clinical status. Infants who required hospitalization for any reason during the first postnatal month were excluded from the study.
Infants were assigned to the case group based on a maternal diagnosis of isolated gestational hypothyroidism; those whose mothers had concomitant medical conditions were excluded. Control participants were selected using a 1:1 matching approach based on gestational age, birth weight, and mode of delivery to reduce perinatal confounding related to perinatal characteristics; their mothers had no medical conditions.
Definition of gestational hypothyroidism
This retrospective study employed a pragmatic, management-based definition of gestational hypothyroidism. Cases were identified as mothers who received a clinical diagnosis of isolated gestational hypothyroidism and were treated with levothyroxine during pregnancy according to institutional protocols aligned with the American Thyroid Association guidelines. 11 The cohort was restricted to mothers diagnosed during pregnancy; those with known pre-gestational thyroid disease were excluded. Antenatal thyroid function records were reviewed for all mothers in the case group, and all included mothers had documented thyroid-stimulating hormone (TSH) and free thyroxine (fT4) values within the trimester-specific reference ranges used in the institutional protocol during pregnancy. More granular antenatal thyroid characterization, including antibody status, thyroid ultrasonography findings, exact timing of diagnosis, and levothyroxine dose adjustments during pregnancy, was not systematically available in the retrospective records and was therefore considered a study limitation.
Data collection and feeding definitions
Prenatal variables, including maternal age, gravidity, parity, medical history, and gestational age, as well as neonatal characteristics such as birth weight, length, head circumference, infant sex, and mode of delivery, were obtained from electronic medical records. Postnatal feeding data at the end of the first postnatal month were retrieved from hospital databases.
At 6 months of age, families in both groups were contacted by telephone solely to verify infant feeding practices, with no intervention performed. EBF was defined according to WHO criteria as feeding with breast milk only, excluding all other foods or liquids except vitamins, minerals, or medications. 3 For infants who were not exclusively breastfed, detailed feeding histories—including the timing and reasons for formula supplementation and the introduction of complementary foods—were recorded. Data collection and follow-ups were conducted by the same experienced neonatal and pediatric team throughout the study.
In the study setting, all newborns undergo routine heel-prick screening for congenital hypothyroidism using TSH measurement. Additionally, venous TSH and fT4 levels are measured on or around the 7th and 30th postnatal days in infants born to mothers treated with levothyroxine for gestational hypothyroidism during pregnancy. None of the enrolled newborns were diagnosed with congenital hypothyroidism.
Statistical analysis
The required sample size was calculated to compare EBF rates between infants of mothers with gestational hypothyroidism (case group, p1 = 60%) and healthy mothers (control group, p2 = 80%). Using a two-proportion test with 80% power and a two-sided significance level of α = 0.05, a minimum of 82 infants per group was required. Allowing for an estimated 10% dropout rate, the target sample size increased to 91 infants per group (total N = 182). To enhance population representativeness, the final analysis included 206 participants.
Statistical analyses were performed using R software (version 4.3; R Foundation for Statistical Computing, Vienna, Austria). 15 Categorical variables were summarized as counts and percentages and compared using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were reported as mean ± standard deviation or median with interquartile range (IQR, 25th–75th percentile), depending on distribution assessed by the Shapiro–Wilk test, and compared using the independent samples t-test or Mann–Whitney U test, as appropriate.
Univariable logistic regression analyses were conducted to assess associations between maternal and neonatal factors (birth weight, gestational age, maternal age, maternal height, head circumference, parity, and gravidity) and formula supplementation during the first postnatal month. Variables with p < 0.20 were entered into a multivariable logistic regression model to identify factors independently associated with early formula supplementation. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, and statistical significance was defined as p < 0.05.
To explore differences across gravidity strata, formula supplementation patterns were summarized according to gravidity category. Formal interaction testing was additionally performed using logistic regression models including gestational hypothyroidism × maternal gravidity interaction terms. Maternal gravidity was evaluated both as a continuous variable and as a categorical variable using the strata shown in Figure 1.
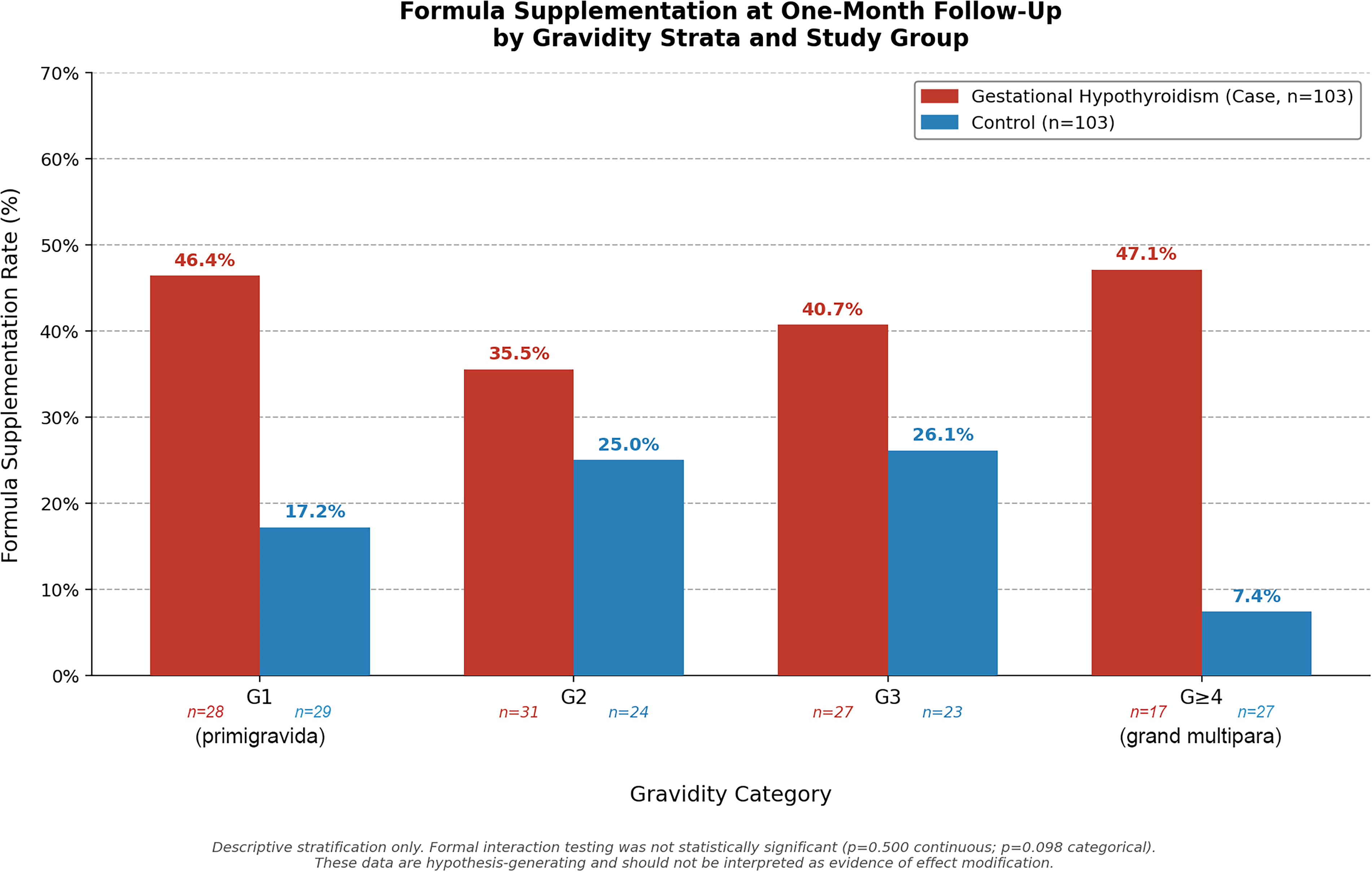
Descriptive stratification of formula supplementation rates at 1-month follow-up by maternal gravidity in the gestational hypothyroidism (case) and control groups. Gravidity strata: G1, primigravida (case n = 28, control n = 29); G2 (case n = 31, control n = 24); G3 (case n = 27, control n = 23); G ≥ 4, grand multipara (case n = 17, control n = 27). Data are presented for descriptive purposes only. Formal interaction testing using logistic regression with a group × gravidity interaction term did not demonstrate statistically significant effect modification (continuous gravidity: p = 0.500; categorical gravidity: p = 0.098). These findings are hypothesis-generating rather than confirmatory and should be interpreted with caution.
Results
During the study period, 231 eligible mother–infant dyads were screened. Seventeen infants were excluded because of hospitalization for any reason during the first postnatal month, including respiratory distress, suspected sepsis, or hyperbilirubinemia requiring phototherapy, and eight were excluded because of incomplete data. The final analysis included 206 mother–infant dyads, with 103 infants in the case group and 103 in the control group.
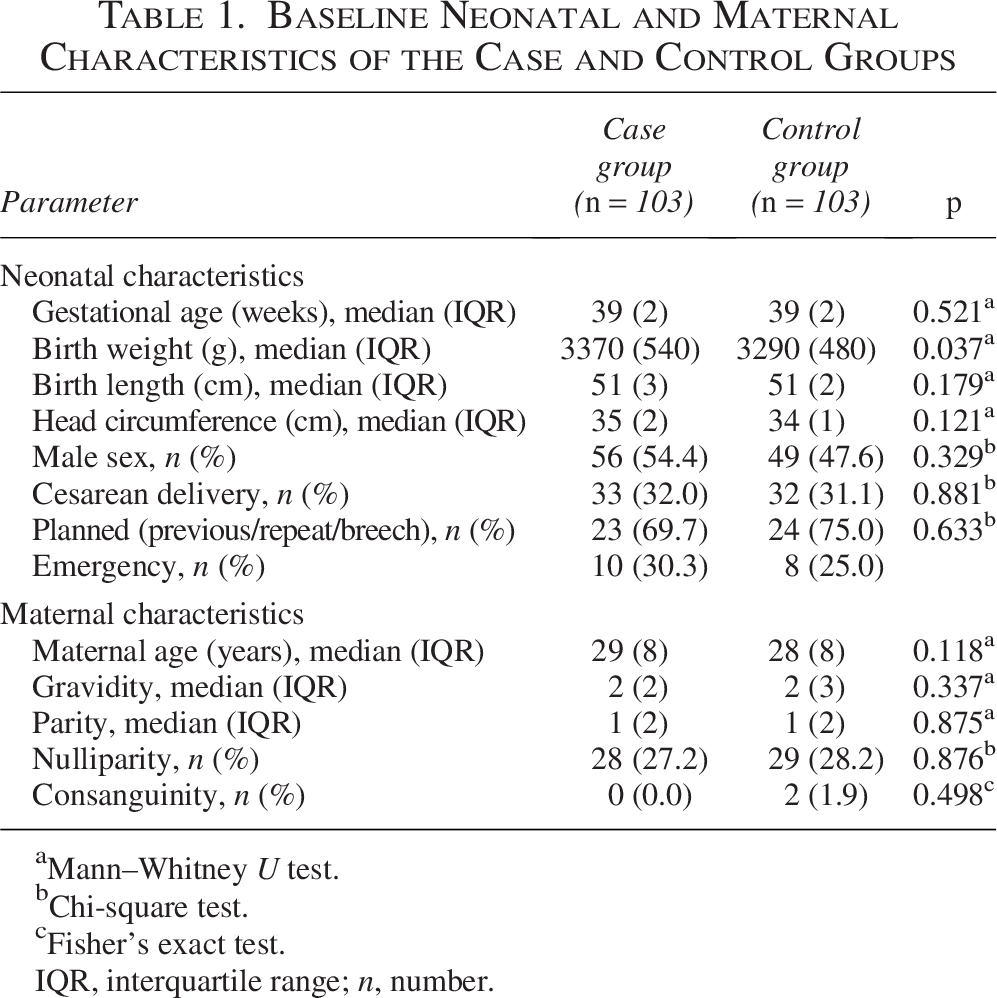
Baseline maternal and neonatal characteristics are presented in Table 1. The two groups were comparable regarding gestational age, infant length, head circumference, sex, mode of delivery, cesarean section indications, maternal age, gravidity, parity, nulliparity, and consanguinity. Birth weight was slightly higher in the case group compared with the control group (median 3370 g [IQR: 540] versus 3290 g [IQR: 480]; p = 0.037).
Baseline Neonatal and Maternal Characteristics of the Case and Control Groups
Mann–Whitney U test.
Chi-square test.
Fisher’s exact test.
IQR, interquartile range; n, number.
Antenatal thyroid function records confirmed that all mothers in the case group had documented TSH and fT4 values within the trimester-specific reference ranges used in the institutional protocol during pregnancy.
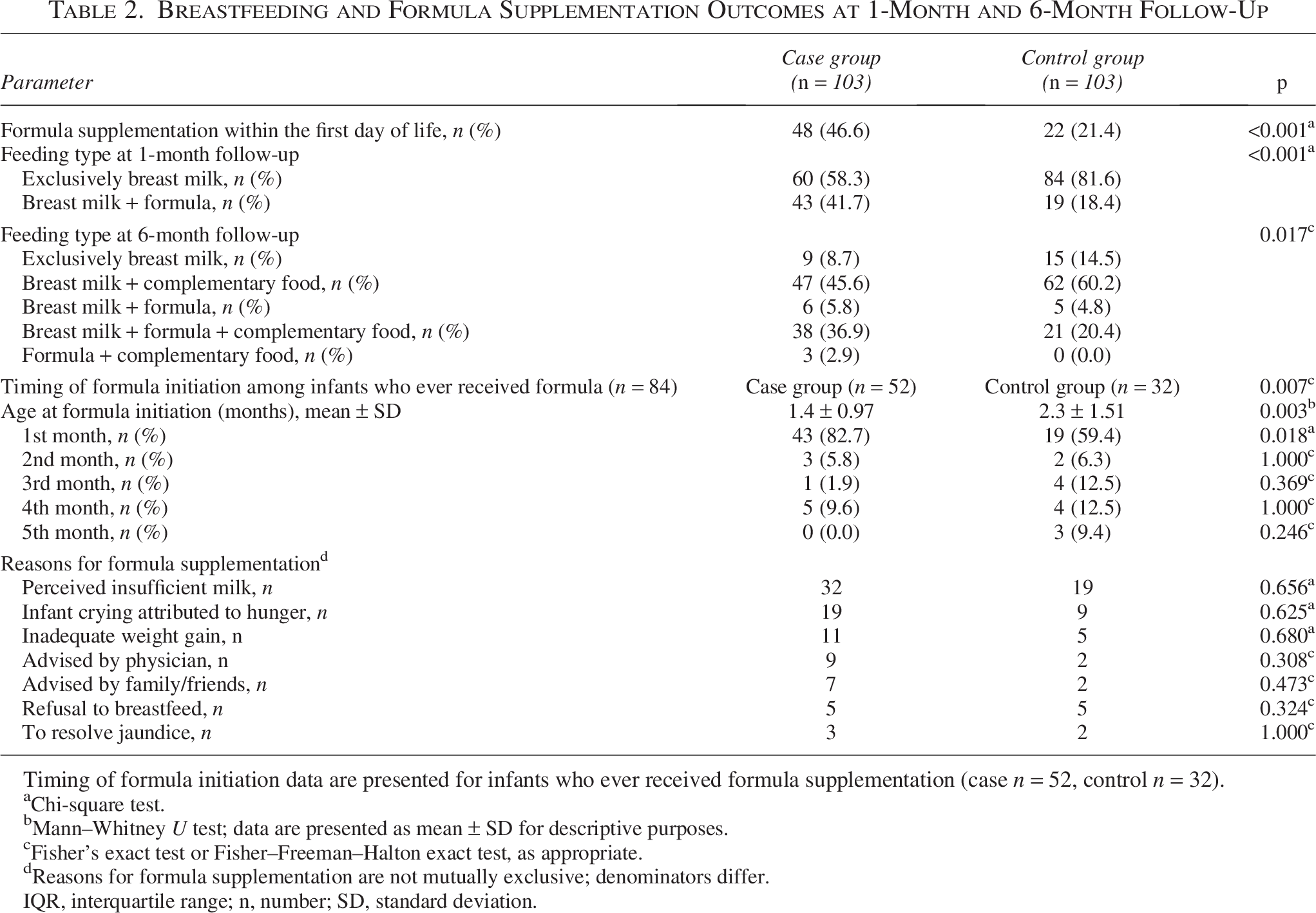
Infants in the case group exhibited a significantly lower rate of EBF at 1-month follow-up than those in the control group (58.3% versus 81.6%, p < 0.001; Table 2). At 6-month follow-up, EBF rates remained lower among cases compared with controls (8.7% versus 14.5%). When broader feeding patterns at this time point were examined, the overall distribution of feeding types differed significantly between groups (p = 0.017; Table 2). Formula feeding—either alone or combined with breastfeeding and/or complementary foods—was significantly more frequent in the case group than in the control group (45.6% versus 25.2%, p = 0.003).
Breastfeeding and Formula Supplementation Outcomes at 1-Month and 6-Month Follow-Up
Timing of formula initiation data are presented for infants who ever received formula supplementation (case n = 52, control n = 32).
Chi-square test.
Mann–Whitney U test; data are presented as mean ± SD for descriptive purposes.
Fisher’s exact test or Fisher–Freeman–Halton exact test, as appropriate.
Reasons for formula supplementation are not mutually exclusive; denominators differ.
IQR, interquartile range; n, number; SD, standard deviation.
Formula supplementation within the first day of life was significantly more frequent in the case group (48/103, 46.6%) than in the control group (22/103, 21.4%). This between-group difference was statistically significant (χ2 = 14.63, p < 0.001, chi-square test). At the 1-month follow-up, breast milk plus formula was reported in 43 infants (41.7%) in the case group versus 19 infants (18.4%) in the control group. At 6 months, formula-containing feeding patterns were more frequent in the case group than in the control group, as shown in Table 2.
Among infants who ever received formula, initiation during the first postnatal month was more frequent in the case group than in the control group (82.7% versus 59.4%, p = 0.018; Table 2).
Perceived insufficient milk supply was the most common reason for formula supplementation in both groups, with no significant between-group differences in reported reasons (Table 2). Complementary feeding was introduced before 6 months in most infants in both groups.
In univariable analyses, head circumference and gravidity met the prespecified criterion for inclusion in the multivariable model (p < 0.20) and were entered into the model (Table 3).
Factors Associated with Early Formula Supplementation During the First Postnatal Month: Results of Logistic Regression Analysis

Variables included in the multivariable model were selected based on univariable p < 0.20 (gravidity and head circumference).
Gestational hypothyroidism status was not included as a covariate because it defines the study groups (case versus control). Bold values indicate statistical significance (p < 0.05).
CI, confidence interval; OR, odds ratio.
Multivariable logistic regression showed that higher maternal gravidity was independently associated with early formula supplementation during the first postnatal month (odds ratio = 3.16; 95% confidence interval: 1.09–9.10; p = 0.033). Complete regression results are presented in Table 3.
Descriptive stratification by gravidity suggested variation in formula supplementation patterns across gravidity strata (Fig. 1). Formal interaction testing was performed using logistic regression models with gestational hypothyroidism × maternal gravidity interaction terms. The interaction was not statistically significant when gravidity was modeled as a continuous variable (p = 0.500). When gravidity was modeled categorically, the overall likelihood-ratio test for the interaction block did not reach conventional statistical significance (p = 0.098). Therefore, these stratified findings should be interpreted as descriptive and hypothesis-generating rather than evidence of formal effect modification.
Due to substantial heterogeneity in 6-month feeding patterns and a low prevalence of the EBF reference group, regression modeling was not conducted for 6-month outcomes.
Discussion
This study demonstrates that gestational hypothyroidism is associated with an early shift away from EBF, characterized by lower EBF rates at 1 month, earlier initiation of formula supplementation, and a higher frequency of formula-containing feeding patterns during follow-up. Maternal gravidity was independently associated with early formula supplementation in the multivariable model; however, formal interaction testing did not demonstrate statistically significant effect modification by gravidity. Therefore, the gravidity-stratified findings should be interpreted as descriptive and hypothesis-generating rather than confirmatory.
Breastfeeding duration and effectiveness are shaped by a complex interplay of sociodemographic, psychological, and clinical determinants.1,2,5 Among these, early initiation of breastfeeding, skin-to-skin contact, and appropriate feeding techniques represent key modifiable determinants, whereas maternal reproductive history and infant-related characteristics—such as prematurity, mode of delivery, and early neonatal hospitalization—are largely non-modifiable. In the present study, the case and control groups were well balanced with respect to baseline maternal demographics, age, and obstetric characteristics. Although infants born to mothers with gestational hypothyroidism had a slightly higher birth weight, this difference was small and unlikely to confound feeding outcomes. Notably, despite this baseline comparability, gestational hypothyroidism was associated with suboptimal breastfeeding outcomes, underscoring the potential impact of maternal endocrine dysregulation on early lactation success.
One of the most consistently reported predictors of early breastfeeding cessation in the literature is perceived insufficient milk supply.5,14 Early initiation of breastfeeding within the first postpartum hours provides a critical physiological stimulus for lactogenesis and has been shown to support both the establishment and duration of EBF.1,3 Despite routine initiation of breastfeeding within the first 30 minutes after birth in accordance with Baby-Friendly Hospital Initiative policies, our study revealed a clinically meaningful increase in formula supplementation on the first postnatal day among mothers with gestational hypothyroidism. This finding suggests an association between gestational hypothyroidism and delayed or inadequate lactogenesis, which may manifest clinically as perceived or actual insufficient milk production.
Early formula supplementation may also have contributed to the persistence of formula use beyond the first days of life. Formula introduction during the immediate postpartum period can reduce infant suckling frequency and breast stimulation, thereby disrupting the supply-demand cycle during the period when milk production is being established.16,17 In this context, the higher rate of day-one formula supplementation in the case group may have amplified the initial lactation difficulty and contributed to continued formula use at later follow-up points. Consistently, perceived insufficient milk supply was the most frequently reported reason for formula use in both groups.
Maternal comorbidities represent important upstream risk factors for early breastfeeding cessation and are frequently mediated through pathways including maternal fatigue, psychosocial distress, non-elective cesarean delivery, and suboptimal feeding practices.5,9 Among medical conditions, maternal endocrine disorders—particularly gestational diabetes mellitus—have been extensively studied and consistently linked to delayed lactogenesis and shorter breastfeeding duration.8,9 These findings support the concept that endocrine dysregulation during pregnancy can have persistent postpartum effects on lactation physiology and breastfeeding continuation. In parallel, epidemiological data indicate a rising prevalence of hypothyroidism among women of reproductive age, accompanied by a corresponding increase in gestational hypothyroidism, highlighting its growing clinical relevance for breastfeeding outcomes.10,11
An important consideration in interpreting our findings is that all mothers in the case group received levothyroxine during pregnancy and had documented antenatal thyroid control within institutional reference ranges. Nevertheless, breastfeeding outcomes were worse in this group. This observation suggests that antenatal biochemical control may not fully eliminate the risk of lactation difficulties, particularly if delayed lactogenesis, early formula supplementation, or unmeasured postpartum thyroid dysfunction contribute to breastfeeding trajectories. Despite increasing recognition of gestational hypothyroidism as an important endocrine disorder of pregnancy, its impact on breastfeeding outcomes has received relatively limited attention compared with other endocrine conditions. Our findings contribute to this gap by demonstrating an association between gestational hypothyroidism and increased early formula supplementation in a well-matched cohort of term infants without major perinatal complications.
Gestational hypothyroidism is increasingly recognized as an endocrine condition that may contribute to high-risk pregnancy status, particularly when thyroid dysfunction is inadequately controlled.10,11 Women with high-risk pregnancies have been reported to show lower rates of breastfeeding initiation and continuation. In a recent cohort study by Salama et al., 18 initiation of breastfeeding within the first hour postpartum was significantly lower among women with high-risk pregnancies compared with those with uncomplicated pregnancies, and EBF rates at 6 months were also reduced. 18 In line with these findings, our matched analysis showed that gestational hypothyroidism was associated with increased formula use and reduced EBF, including differences observed at 6 months postpartum.
Available data specifically addressing EBF prevalence and early breastfeeding cessation among infants born to mothers with gestational hypothyroidism remain limited. Pisoni et al. 19 prospectively investigated breastfeeding outcomes among women who conceived via assisted reproductive technologies and reported lower EBF rates at 6 months among those with thyroid dysfunction; however, these associations did not remain statistically significant after full multivariable adjustment. 19 In contrast, our findings showed an association between gestational hypothyroidism and early formula supplementation in a well-matched cohort of term infants, thereby extending the limited evidence on thyroid dysfunction and breastfeeding outcomes.
Maternal gravidity was independently associated with early formula supplementation during the first postnatal month. Previous pregnancy and breastfeeding experience may support breastfeeding confidence and continuation, and increasing parity has been associated with more favorable breastfeeding outcomes in some studies. 8 However, in our cohort, gravidity-stratified findings suggested variation in formula supplementation patterns across gravidity strata. Formal interaction testing did not demonstrate a statistically significant gestational hypothyroidism × gravidity interaction. Therefore, these findings should be interpreted as descriptive and hypothesis-generating rather than evidence of formal effect modification.
Several biologically plausible mechanisms may help explain the observed association between gravidity and early formula supplementation, although formal interaction testing did not confirm statistically significant effect modification. Pregnancy represents a substantial physiological stressor that increases thyroid hormone requirements, and repeated pregnancies may progressively deplete thyroidal reserve in susceptible individuals.10,20 In women with limited thyroid reserve, successive pregnancies may therefore unmask or exacerbate thyroid dysfunction, even when overt hypothyroidism is not clinically apparent before pregnancy.11,20 This concept is supported by epidemiological data demonstrating a higher prevalence of thyroid dysfunction among multigravid women compared with primigravid women. 21
In addition to thyroid reserve depletion, autoimmune mechanisms may further contribute to this association. Repeated pregnancies have been hypothesized to increase immune system activation and the persistence of fetal microchimerism, which may play a role in the development or progression of autoimmune thyroid disease during the postpartum period. 22 These autoimmune processes may adversely affect both thyroid function and lactation physiology, potentially compounding the risk of delayed lactogenesis and early breastfeeding cessation in multigravid women with gestational hypothyroidism.
A further consideration is that postpartum thyroid function was not assessed in this retrospective study. Postpartum thyroiditis and persistent or recurrent hypothyroidism may occur during the same period in which breastfeeding continuation was evaluated, and hypothyroid phases during lactation could contribute to reduced milk production, maternal fatigue, or difficulty maintaining breastfeeding.11,23 Therefore, we cannot determine whether the observed feeding differences were related solely to gestational thyroid dysfunction, early lactogenesis difficulties, or ongoing postpartum thyroid dysfunction. This uncertainty should be considered when interpreting the persistence of formula use at later follow-up points.
From a clinical standpoint, these findings suggest that maternal gestational hypothyroidism should be recognized as a potential risk marker for breastfeeding difficulties. Neonatologists, obstetricians, and lactation consultants should be aware that mothers with gestational hypothyroidism—even when treated during pregnancy—may require closer monitoring for delayed lactogenesis and early feeding difficulties. Early identification of this risk profile may allow timely lactation counseling, reinforcement of breastfeeding techniques, and prevention of unnecessary formula supplementation during the first days of life, when the supply-demand cycle is being established. Given the possible contribution of postpartum thyroid dysfunction, structured postpartum follow-up that integrates thyroid management and lactation support may also be beneficial. Integration of thyroid status into breastfeeding risk assessment may therefore support more individualized postpartum care.
Future prospective studies should include serial maternal thyroid function assessment during pregnancy and the postpartum period, together with detailed information on levothyroxine dose adjustments, antibody status, and timing of diagnosis. Larger multicenter cohorts are also needed to clarify whether maternal gravidity modifies the association between gestational hypothyroidism and breastfeeding outcomes, using predefined interaction analyses with adequate statistical power. In addition, studies incorporating objective lactation measures and structured assessment of lactation support may help determine whether targeted postpartum interventions can reduce unnecessary early formula supplementation in this population.
Limitations
This study is subject to several inherent limitations of its retrospective design. First, the absence of granular data on the timing of diagnosis, levothyroxine therapy details, antibody status, thyroid ultrasonography findings, and parity-specific thyroid history limited the precision of disease stratification and introduced potential for unmeasured confounding. Second, key psychosocial and socioeconomic determinants of breastfeeding (e.g., maternal education, breastfeeding self-efficacy, depressive symptoms, and access to lactation support) could not be systematically analyzed. Third, while 6-month outcomes were captured via follow-up, reliance on maternal recall may have introduced recall bias.
In addition, substantial heterogeneity and the low prevalence of EBF at this timepoint precluded adjusted multivariable analysis for 6-month outcomes. Nonetheless, the observed persistence of altered feeding patterns at 6 months suggests a potential protracted association between gestational hypothyroidism and breastfeeding outcomes, although this interpretation should be made cautiously because adjusted regression modeling was not feasible. Finally, postpartum thyroid management variables, which could directly modulate lactation, including maternal thyroid function and levothyroxine dose adjustments during follow-up, could not be assessed.
Strengths
A major strength of this study is its matched case–control design, which minimized confounding by key perinatal factors such as gestational age, birth weight, and mode of delivery. The inclusion of only healthy term infants without neonatal hospitalization during the first postnatal month further reduced confounding from neonatal morbidity. Antenatal thyroid control was documented in all mothers in the case group, supporting the consistency of the gestational hypothyroidism exposure definition. The use of both short-term and longer-term breastfeeding outcomes allowed evaluation of temporal patterns in feeding practices. Additionally, the relatively large sample size and standardized follow-up methods enhance the internal validity of the findings.
Conclusion
In this retrospective matched case–control study, gestational hypothyroidism was associated with lower rates of EBF at 1 month, earlier initiation of formula supplementation, and altered feeding patterns through the 6-month follow-up. Maternal gravidity was independently associated with early formula use; however, formal interaction testing did not demonstrate statistically significant effect modification by gravidity. These findings suggest that mothers with gestational hypothyroidism may benefit from targeted lactation support beginning in the early postpartum period, together with careful postpartum follow-up. Further prospective studies with serial thyroid function assessment and adequate power for interaction analyses are warranted to clarify the mechanisms linking thyroid dysfunction, gravidity, and breastfeeding outcomes.
Statement of Adherence to Preprint Policy
The authors declare that this article has not been published as a preprint and is not under consideration elsewhere.
Authors’ Contributions
T.I. conceptualized and designed the study, coordinated data collection, performed the statistical analyses, and drafted the initial article. B.G. and A.O.G. contributed to data collection and interpretation and critically reviewed the article for important intellectual content. S.C. participated in data acquisition and contributed to data interpretation. E.A. and S.G. provided overall supervision, contributed to study design and interpretation of the results, and critically revised the article. All authors approved the final version of the article and agree to be accountable for all aspects of the work.
Ethics Approval Statement
This study was approved by the Scientific Research Ethics Committee of Sancaktepe Şehit Prof. Dr. İlhan Varank Training and Research Hospital (Approval No: 2025/309; Date: September 10, 2025). The ethical approval covered the retrospective use and analysis of routinely collected clinical data as well as follow-up telephone contacts conducted solely for data verification.
Footnotes
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Disclosure Statement
The authors declare no conflicts of interest in relation to this study.
Funding Information
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.