
Abstract
Introduction:
Supporting women during the perinatal period helps build confidence, strengthens early bonding between mother and baby, and encourages successful breastfeeding. Continuous midwifery care models are one of the ways that support women in this periods.
Objective:
This study aimed to evaluate the effect of integrated continuous team midwifery care (ICTMC) in enhancing breastfeeding success in the Iranian health system.
Methods:
In this randomized controlled trial, 200 low-risk primiparous women with a gestational age of less than 12 weeks were recruited from public health centers. Participants were randomly assigned to either the intervention group, which received continuous midwifery care throughout pregnancy, childbirth, and postnatal follow-up, or the control group, which received routine care. The primary outcomes were early skin-to-skin contact and breastfeeding success at the time of discharge and at 4–6 weeks postpartum. Data were analyzed using Stata, employing descriptive statistics, Chi-square, independent t-test, Phi/Cramer’s V, and Cohen’s d. The p < 0.05 is significant. Data were analyzed with SPSS 26.
Results:
ICTMC groups were significantly more likely to initiate skin-to-skin contactearly skin-to-skin contact immediately after birth (92% vs. 74%, p < 0.001) and achieve successful breastfeeding at the discharge time (88% vs. 70%, p = 0.002) compared to the control group. At 6 weeks postpartum, breastfeeding success remained higher in the intervention group (82% vs. 65%, p = 0.004).
Conclusion:
Women with ICTMC, effectively support skin-to-skin contactearly mother–infant bonding and enhance breastfeeding success among low-risk primiparous women. Integrating this model into routine maternal care may improve perinatal outcomes.
Introduction
Breastfeeding is acknowledged as a fundamental factor influencing both immediate and prolonged health outcomes for mothers and their infants. 1 The World Health Organization (WHO) recommends that infants should receive exclusive breastfeeding for the first 6 months of life, after accompanied by continued breastfeeding alongside the introduction of complementary food for 2 years or more. 2 However, despite these recommendations, the global rate of exclusive breastfeeding remains low worldwide. 3 According to the WHO Global Health Observatory, only 44% of infants aged 0–6 months are exclusively breastfed, which is still slightly below the target of 50% set by the World Health Assembly for 2025.4,5
These gaps reflect the complex interplay of multiple factors—including limited maternal knowledge, inadequate education, insufficient support, sociocultural barriers, and fragmented, noncontinuous maternity care systems—that collectively undermine breastfeeding success.6,7 These challenges highlight the need for evidence-based maternity care models capable of providing continuous support for women throughout pregnancy, childbirth, and the early postpartum period. 8
Evidence suggests that continuity care models, particularly those led by midwives who have received adequate lactation training, may effectively address these multifaceted barriers by providing increased informational, emotional, and practical support across the perinatal period, although the specific training requirements may differ across cultural contexts. 9 Continuity of midwifery care models involve the provision of antenatal, intrapartum, and postnatal care by a single midwife or a team of midwives familiar with the mother. In these models, sustained relationships between women and their care providers foster trust and effective communication, enabling early identification of breastfeeding challenges, timely counseling, and consistent reinforcement of education and confidence-building strategies. 10
A study conducted in a private maternity center in Iran demonstrated that a team-based continuum of midwifery care not only increases maternal satisfaction and reduces unnecessary interventions, but also significantly increases the rate of exclusive breastfeeding in the early postpartum period. 11 Moreover, a large retrospective cohort study from Sweden reported that women receiving midwifery continuity of care had a higher likelihood of exclusive breastfeeding at hospital discharge, highlighting the effectiveness of this model across diverse health-system contexts. 12 Evidence from systematic reviews further indicates that midwife-led continuity models support breastfeeding initiation and may extend breastfeeding duration, especially when combined with structured postpartum support interventions. 13 However, despite these positive findings, a Cochrane systematic review reported that although midwife-led continuity models offer benefits, such as reduced interventions and increased maternal satisfaction, there is insufficient and inconsistent evidence to conclude a clear effect on breastfeeding outcomes, particularly beyond hospital discharge. 14
Despite growing evidence supporting midwife-led continuity of care models, the impact of such models on breastfeeding outcomes remains inconsistent, particularly beyond hospital discharge. Moreover, there is a notable lack of randomized controlled trials evaluating integrated continuity of midwifery care within public health care systems in low- and middle-income countries, including Iran, where maternity care is largely fragmented across the antenatal, intrapartum, and postpartum periods. 15 To address these gaps, the present randomized controlled trial aimed to evaluate the effectiveness of an integrated continuous midwifery care model embedded within Iran’s existing health system on breastfeeding success during the postpartum period.
Materials and Methods
This randomized controlled trial was conducted as part of a comprehensive and in-depth PhD research program. This was a parallel, two-arm randomized controlled trial with a 1:1 allocation ratio. A total of 200 pregnant women from Government health centers Kashan, Iran, were enrolled and randomly assigned to two comparable groups, following CONSORT guidelines. Data collection occurred between April 30, 2023, and January 20, 2024. Written informed consent was obtained from all participants, and study procedures adhered to the ethical standards of the institutional review board and the Declaration of Helsinki, with strict confidentiality and anonymity.
Participants were recruited from 15 governmental primary health care centers affiliated with Kashan University of Medical Sciences. Eligible participants were married Iranian women aged 18–35 years, primiparous, with a low-risk singleton pregnancy at ≤12 weeks’ gestation and basic literacy. Exclusion criteria included medical complications or a history of abortion.
Following the methodology of study Shahinfar et al., 11 the sample size was calculated with a power of 80% and a two-sided α of 0.05. The required sample size was determined to be 100 participants per group.
Participants were allocated to either the intervention or control group using block randomization with block sizes of 4 and 6, maintaining an allocation ratio of 1:1. The randomization sequence was generated using a computer-based random number generator. Allocation concealment was ensured through sequentially numbered, opaque, sealed envelopes prepared by an independent third party who was not involved in recruitment, data collection, or aware of the study objectives. Envelopes were opened only after obtaining written informed consent, preventing any prior knowledge of group assignment during enrollment.
Due to the nature of the intervention, blinding of participants and care providers was not possible. Nevertheless, the data analyst remained blinded to group allocation throughout the study.
The intervention components were categorized into the Core Components of the Integrated Continuous Midwifery Care (ICTM) and the Additional Supportive ICTM elements. The ICTM Core Components comprised “continuous access” and “multidimensional continuity of care.”
To ensure continuous access, women were provided with a 24/7 contact number from their first prenatal visit for timely support. Structured daily educational program was delivered through a dedicated Eitaa messaging-platform (commonly used in Iran) group. In addition to general pregnancy and childbirth content, the program placed a strong and continuous emphasis on breastfeeding education and support, beginning early in pregnancy and continuing through the postpartum period.
In the case of multidimensional continuity of care, temporal continuity and relational continuity of care were prioritized. To avoid disruption of care (temporal continuity), care was maintained continuously throughout pregnancy, labor, and the postpartum period (up to 6 weeks). To maintain relational continuity of care, women received continuous midwifery care by a dedicated team consisting of two primary health care-based midwives, two hospital-based midwives, and the principal investigator (F.N.).
One designated lead midwife in each health center was responsible for providing antenatal and postnatal care, while an assigned hospital midwife managed intrapartum care, with backup coverage available when required. In the event of complications, the team collaborated, regular communication was maintained among team members, and referrals and follow-up were conducted in a coordinated manner. In the event of complications, the team collaborated with obstetricians and other relevant specialists.
Additional supportive ICTM components were integrated to strengthen the sustainability of the main pillars. These included educational empowerment and health literacy, where training was tailored to various stakeholders, including the pregnant women and the care team itself, utilizing a variety of pedagogical methods. During the childbirth preparation classes delivered by the midwifery team, women received training on lactation physiology, early initiation of breastfeeding, the importance of exclusive breastfeeding, prevention and management of common breastfeeding problems, maternal nutrition, positioning and latch techniques, and the role of immediate skin-to-skin contact. Midwives provided individualized counseling on breastfeeding initiation within the first hour, proper latch, management of engorgement, prevention of nipple trauma, recognition of infant feeding cues, and ensuring adequate milk transfer. Practical skill-building (including breast massage, hand expression, and relaxation techniques) was included. All breastfeeding support adhered to woman-centered care principles and evidence-based lactation guidelines.
Moreover, management and support were provided by the first investigator. The first investigator supervised all stages of care to ensure adherence to the study protocol.
Women in the control group received routine antenatal, intrapartum, and postpartum care in accordance with the national maternity care protocol of Iran, delivered by multiple health care providers without continuity of care. Breastfeeding education, when provided, was unstructured and inconsistent, and was typically limited to brief advice during routine antenatal visits or after birth, rather than being delivered through a standardized or systematic program. No ongoing follow-up or continuous support for breastfeeding or postpartum care beyond standard practice was ensured.
The primary outcome of the study was exclusive breastfeeding at 4–6 weeks postpartum. This outcome was assessed through structured maternal interviews conducted by trained midwives at the 4–6-week postpartum follow-up.
Secondary outcomes included early breastfeeding practices and breastfeeding-related maternal complications during the first 6 weeks postpartum. These outcomes were immediate skin-to-skin contact at birth, defined as uninterrupted skin-to-skin contact between mother and newborn initiated within the first 5 minutes after birth (yes/no). Time to first breastfeeding, defined as the time interval (in minutes) from birth to the initiation of the first breastfeeding session. Duration of the first breastfeeding session, measured in minutes. Infant feeding modality at 72 hours, 2 weeks, and 4–6 weeks postpartum, categorized as exclusive breastfeeding, mixed feeding (breast milk plus formula or other liquids), and formula feeding. Incidence of nipple fissure within the first 6 weeks postpartum, defined as the presence of visible cracks, bleeding, or pain in the nipple area during breastfeeding, as reported by the mother. Incidence of mastitis within the first 6 weeks postpartum, defined as localized breast pain, redness, swelling, and systemic symptoms (e.g., fever), diagnosed or reported during follow-up. Outcomes were assessed by trained midwives using structured follow-up interviews based on a standardized maternal well-being assessment checklist. The content validity of the checklist was assessed through expert review by 10 faculty members in midwifery.
All statistical analyses were conducted using a per-protocol approach. Chi-square for categorical variables, independent t-test for continuous. Effect sizes: Phi/Cramer’s V (categorical), Cohen’s d (continuous). p < 0.05 is significant. Data were analyzed with SPSS 26.
Results
Of the 200 randomized participants, 190 completed the study and were included in the per-protocol analysis. The remaining 10 participants (4 from the intervention group and 6 from the control group) did not complete the study because they developed high-risk conditions during the perinatal period that required medical management beyond the scope of the trial protocol. Baseline demographic and obstetric characteristics of participants were comparable between the intervention and control groups and have been previously reported. 16 At 4–6 weeks postpartum, the rate of exclusive breastfeeding was significantly higher in the ICTMC group compared to the control group (76% vs. 46%, p < 0.001, Φ = 0.32).
Table 1 presents a comparison of breastfeeding-related complications between the intervention and control groups. The prevalence of nipple fissure was lower in the ICTMC (10.42%) compared to control group (15.96%), although the difference was not statistically significant (p = 0.259). Similarly, the incidence of mastitis was low in both groups, and there was no significant difference between the two groups in terms of this variable (p = 1.000).
Breastfeeding-Related Complications during the First 6 Weeks Postpartum (Per-Protocol Analysis)
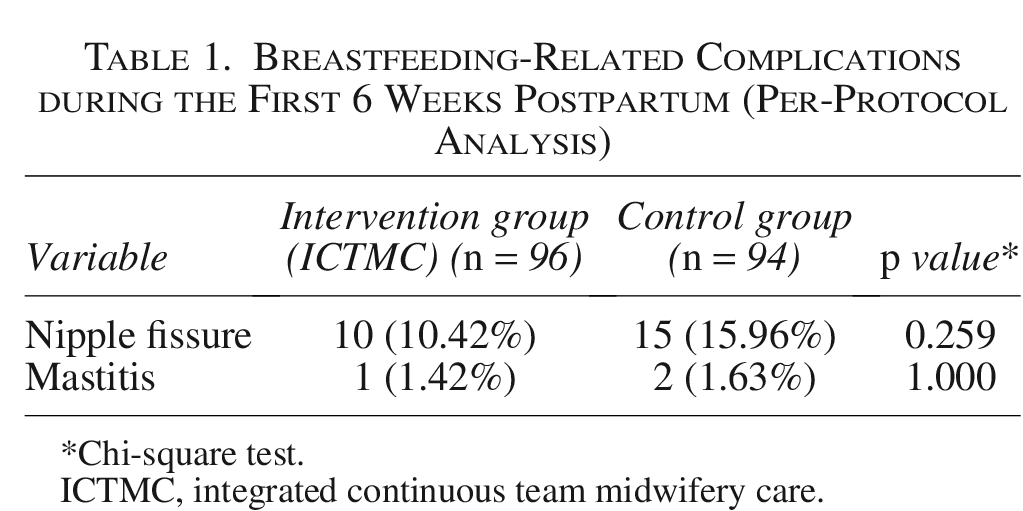
Chi-square test.
ICTMC, integrated continuous team midwifery care.
Table 2 summarizes early postpartum breastfeeding outcomes and infant feeding methods in the intervention and control groups. Skin-to-skin contact immediately after delivery was more frequent in women with ICTMC compared to control group (p = 0.006). The mean time from birth to first mother–infant contact was significantly shorter in Women with ICTMC compared to control group (p < 0.001, Cohen’s d = 0.41). Similarly, the time to first breastfeeding was reduced in women with ICTMC (p < 0.001, Cohen’s d = 0.67), and the duration of the first breastfeeding session was longer (p < 0.001, Cohen’s d = 1.19). Exclusive breastfeeding rates were consistently higher among women with ICTMC. Also, the prevalence of formula feeding or mixed feeding during 2 and 4–6 weeks postpartum was lower in women with ICTMC compared to control group.
Early Postpartum Breastfeeding Outcomes and Infant Feeding Methods in the Study Groups (Per-Protocol Analysis)
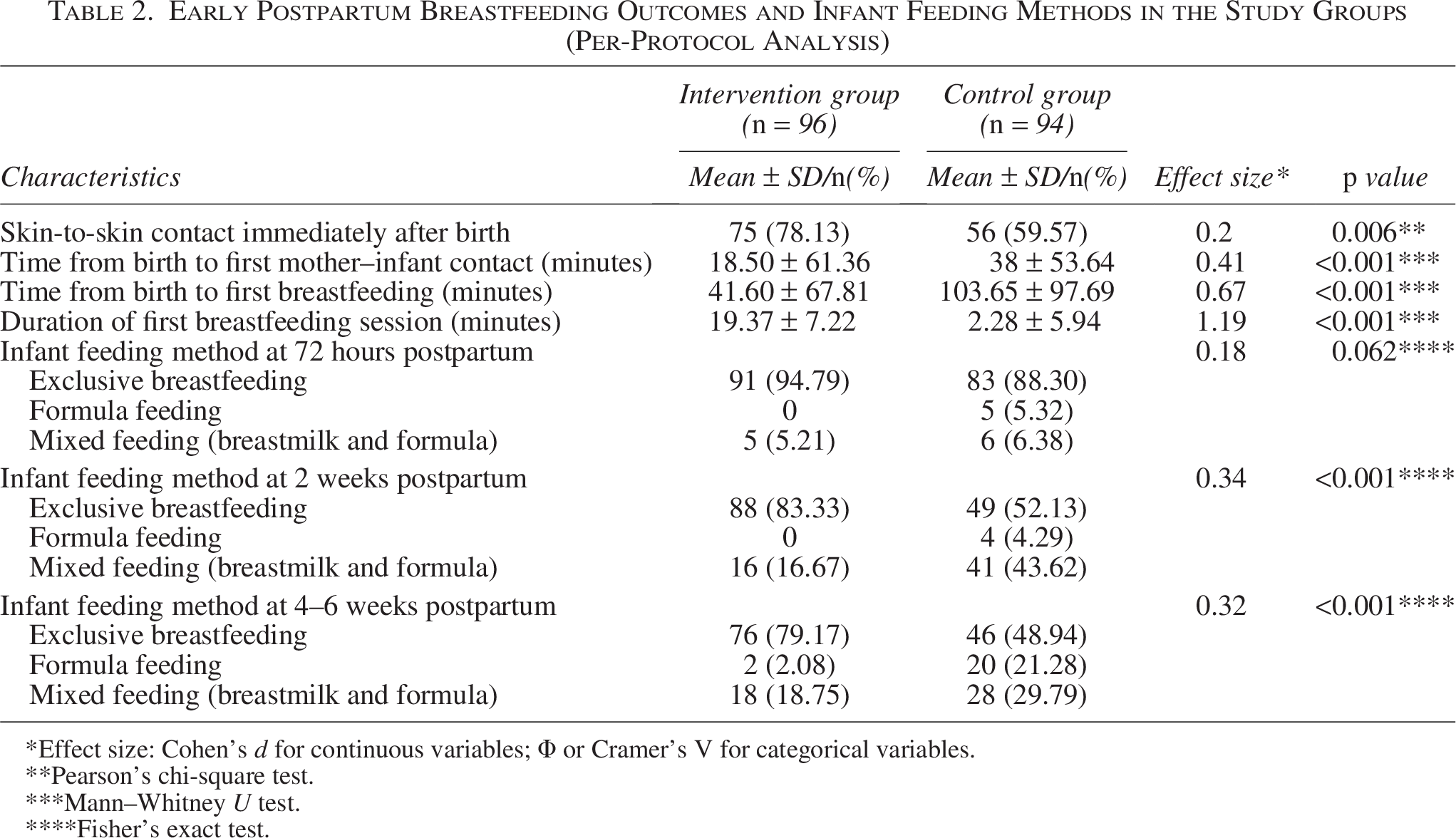
Effect size: Cohen’s d for continuous variables; Φ or Cramer’s V for categorical variables.
Pearson’s chi-square test.
Mann–Whitney U test.
Fisher’s exact test.
Discussion
The present study shows improved rates of early skin-;to-skin contact, shorter time to first breastfeeding, longer initial feeding sessions, and higher exclusive breastfeeding rates in the ICTMC group. Importantly, the observed effects were not only statistically significant but also clinically meaningful, with large effect sizes for duration of first breastfeeding session and time to initiation. The results of this study are consistent with findings from previous studies highlighting the advantages of continuous midwifery-led care. For example, Cai et al. (2025) reported midwife-led continuity of care increased exclusive breastfeeding rates at 48 hours postpartum, along with improved lactation function and milk volume. 17 Moreover, evidence suggests that continuous midwifery care models enhance maternal satisfaction, improve care experience, and increase the likelihood of continued exclusive breastfeeding. Mortensen et al. (2019) showed women receiving a midwife-led continuity model had significantly higher satisfaction scores and a greater proportion of exclusive breastfeeding at the postpartum follow-up compared to those receiving standard care. 18 Previous systematic evidence also highlights that components such as early skin-to-skin contact, consistent education, and postpartum support often integral parts of continuity-of-care models are associated with better breastfeeding initiation and continuation. 19 In the present study, continuous education and support of the mother by the continuous care team during pregnancy, labor, and postpartum played a significant role in breastfeeding success, as did continued education in childbirth preparation classes and the use of an educational platform in this regard.
In Iranian culture, childbirth is an important family-centered event; however, maternal practices can often be influenced by traditional beliefs that may differ from evidence-based guidelines. As noted by Olang et al. (2009), various sociocultural factors and traditional practices in Iran may influence the duration and method of feeding, creating significant challenges in achieving exclusive breastfeeding. 20
Our intervention reduced these barriers through ongoing education and continuous access to information. Rather than relying on sporadic education, the ICTM model ensured that mothers received ongoing guidance through a structured communication channel. Importantly, continuity of care from a familiar midwifery team fostered trust and allowed the team to provide evidence-based breastfeeding support and clinical guidance in a timely manner. By ensuring that care was not sporadic but an ongoing process of engagement and follow-up, the intervention helped mothers to breastfeed successfully and effectively bridged the gap between cultural practices and best clinical practice to the extent possible.
A plausible mechanism underlying the improved breastfeeding outcomes observed in the ICTMC group involves both behavioral and physiological pathways. Continuous midwifery-led care promotes early and uninterrupted mother–infant contact, which is strongly associated with earlier breastfeeding initiation and longer first feeding sessions. 8 Immediate skin-to-skin contact enhances neonatal reflexes and maternal oxytocin release, facilitating effective latch and early milk transfer, 21 and has also been shown to increase maternal breastfeeding self-efficacy. 22 Within continuity models, repeated contact with a known midwife strengthens maternal autonomy and confidence through ongoing education, hands-on support, and individualized feedback, helping to address common early challenges such as poor latch and positioning. 23 Clinically, these mechanisms translate into higher early exclusive breastfeeding rates and improved initiation practices by optimizing lactation physiology and reducing psychosocial barriers, particularly in settings with limited postpartum support or high cesarean section rates. 8 Nevertheless, while many studies showed beneficial results, not all research demonstrates a sustained long-term benefit of antenatal continuity of care alone on breastfeeding duration. A recent systematic review found no clear, consistent association between midwife-led antenatal care continuity and breastfeeding duration beyond hospital discharge, due to methodological heterogeneity and limited quality of evidence studies. 13 These mixed findings underscore that while midwifery continuity of care due to continued support and structured breastfeeding education, skin-to-skin contact can significantly improve early breastfeeding practices, its impact on long-term breastfeeding maintenance may depend on additional factors, such as family support, maternal context, and health system infrastructure. Therefore, there is a pressing need for public health care centers to have continuous and long-term support.
Clinically, even a modest 20–25-minute reduction in time to breastfeeding initiation can have meaningful neonatal benefits. Early initiation of breastfeeding is associated with reduced neonatal morbidity and up to a 44% lower risk of neonatal mortality, largely through timely transfer of colostrum rich in immune-protective factors.24,25 Early initiation also increases the likelihood of sustained exclusive breastfeeding; infants who breastfeed within the first hour are approximately twice as likely to remain exclusively breastfed at 6 weeks. 26 Exclusive breastfeeding at 2 and 6 weeks is clinically important, as it is linked to lower rates of respiratory and gastrointestinal infections, improved nutritional status, and reduced risk of early childhood stunting. 27
Another result of this study was that although the rates of nipple fissure and mastitis were lower in Women with ICTMC compared to women without an ICTMC, the differences were not statistically significant. This lack of significance may be partly explained by the overall low incidence of these complications, which reduces statistical power to detect between-group differences, particularly within the relatively short postpartum follow-up period. In addition, nipple fissure and mastitis are multifactorial conditions influenced with suboptimal infant positioning, poor latch, and delayed management of breastfeeding challenges, which are preventable with early and skilled support.28,29
Evidence suggests that structured breastfeeding education and timely support reduce the incidence of breast problems, including nipple trauma and subsequent mastitis. 30 Vieira et al. demonstrated that early lactation counseling significantly decreased the risk of nipple injury and improved latch technique among primiparous women. 31 Similarly, systematic reviews addressing mastitis prevention report that specialist breastfeeding advice, early assessment of latch, and proactive management of engorgement and milk removal are plausible strategies to reduce the risk and severity of lactational mastitis, although the certainty of evidence is variable and in some cases low. 32
Findings from Kulsum et al. (2023) indicate that implementing a continuity midwifery care model during the postpartum period can effectively address early breastfeeding problems, as continuous assessment and timely interventions such as management of breast engorgement resulted in smoother milk flow and reduced breast discomfort among mothers. 33
Overall, while our study did not find statistically significant reductions in nipple fissure or mastitis, the direction of effect aligns with evidence that continuity of midwifery care—which integrates repeated lactation counseling, skilled hands-on support, and rapid access to professional help—can plausibly reduce breastfeeding-related complications. 32 However, further high-quality trials with standardized outcome definitions are needed to confirm these findings. Taken together, these findings reinforce the growing body of evidence suggesting that in Women with ICTMC compared to routine maternal services may be a promising strategy to enhance breastfeeding outcomes and minimize early lactation problems, underscoring the need for future multicenter trials to evaluate its broader clinical applicability and long-term benefits.
Within routine public health services, particularly in resource-limited settings, several components of ICTM appear feasible to scale. One such component involves the use of lay messengers and telephone-based support: a low-cost strategy that circumvents the need for physical infrastructure while enabling ongoing education and follow-up, thereby reducing the financial and logistical burden of frequent travel for mothers. Another component is a midwife-centered model that draws on existing community health workers; integrating this approach into the established community health system can reduce dependence on specialists for routine care.
Regarding the linguistic framework of this study, it is important to acknowledge the intersection between international standards of inclusivity and local cultural contexts. While we recognize the importance of gender-inclusive language in the global breastfeeding discourse, the term “mother” holds a central and essential place in Iranian sociocultural identity. In the context of childbirth and breastfeeding practices in Iran, “motherhood” is not simply a biological status, but a fundamental social role that determines family dynamics and support systems. Therefore, in this study, the use of gender-specific terms such as “mothers” in parts of the article is intended to reflect the specific cultural reality and core identities of participants in the Iranian health and social care structure.
Conclusion
This study showed that continuity of midwifery care significantly improved exclusive breastfeeding rates among low-risk primiparous women. Continuous and coordinated support enhanced maternal confidence, reduced early breastfeeding difficulties, and promoted sustained breastfeeding during the early postpartum period. The findings highlight the value of relationship-based, woman-centered care in achieving optimal breastfeeding outcomes. Integrating continuity models into routine maternity services may be a feasible strategy to strengthen maternal–infant health. Further research is recommended to evaluate long-term outcomes and implementation across diverse settings.
Strengths and Limitations: This study, the first conducted in Iran’s public health system, used a rigorous randomized controlled trial design and followed women across pregnancy, birth, and postpartum, providing comprehensive and context-specific evidence. Incorporating qualitative insights helped explain how continuous, team-based midwifery care improved breastfeeding outcomes. Limitations include its single-center design, short follow-up of 6 weeks, reliance on self-reported measures, and the need for adequate staffing and organizational support for broader implementation.
Authors’ Contributions
N.F.: Writing—original draft, visualization, validation, resources, project administration, methodology, investigation, funding acquisition, formal analysis, data curation, conceptualization. B.A.: Writing—review and editing, visualization, supervision, project administration, methodology, investigation, formal analysis, conceptualization. M.D.: Writing—review and editing, validation, software, methodology, formal analysis, conceptualization. S.K.: Writing—review and editing, visualization, supervision, project administration, methodology, investigation, conceptualization. Z.A.: Writing—review and editing, visualization, validation, supervision, resources, project administration, methodology, investigation, formal analysis, conceptualization.
Ethical Approval
This study received ethical approval from the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences, under the ID IR.AJUMS.REC.1402.010.
Informed Consent
Written informed consent was obtained from all participants prior to enrollment in the study.
Footnotes
Acknowledgments
This work originated from Farzaneh Nasiri’s PhD thesis. The authors are grateful to the faculty members of the School of Nursing of Ahvaz Jundishapur University and the midwives of the university and health centers. Special thanks to all participants who willingly participated in this study.
The authors used ChatGPT AI for language editing, text refinement, and translation assistance during the preparation of this article.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This study was supported by Ahvaz Jundishapur University of Medical Sciences, Ahvaz (Grant ID: 330101336).