
Abstract
Objective:
To evaluate the surgical outcomes of the modified right vertical infra-axillary thoracotomy (MRVIAT) technique for the treatment of various congenital heart diseases (CHDs) across all age groups.
Methods:
A retrospective analysis was performed on 1,513 patients with CHD who underwent surgery using the MRVIAT technique between January 2022 and June 2024. Incisions were 2 to 5 cm, and peripheral extracorporeal circulation was not used. Twelve primary surgical procedures were executed across all age groups.
Results:
All 1,513 patients successfully underwent surgery without the need for conversion to a median sternotomy or any in-hospital mortality. The median patient age was 1.1 years (range, 0.1 to 57 years), with 62 patients aged 18 years or older. The median weight was 9 kg (range, 1.8 to 101.6 kg), with 859 patients (56.8%) weighing ≤10 kg, 588 patients (39.9%) weighing between 10 kg and 50 kg, and 66 patients (4.4%) weighing ≥50 kg. Two patients (0.1%) required early reoperation: 1 (0.1%) due to third-degree atrioventricular block and 1 (0.1%) due to postoperative bleeding. Other postoperative complications included mild residual shunt in 20 patients (1.3%), pneumothorax in 2 patients (0.1%), wound infection in 3 patients (0.2%), and pulmonary infection in 4 patients (0.3%). The median follow-up period was 1.3 years (range, 0.3 to 2.5 years). During follow-up, no surgery-related thoracic deformities were noted.
Conclusions:
The MRVIAT technique is a safe and viable method for treating CHD patients across all age groups. This technique, which involves a smaller, less prominent incision, offers a promising alternative to median sternotomy methods.
This is a visual representation of the abstract.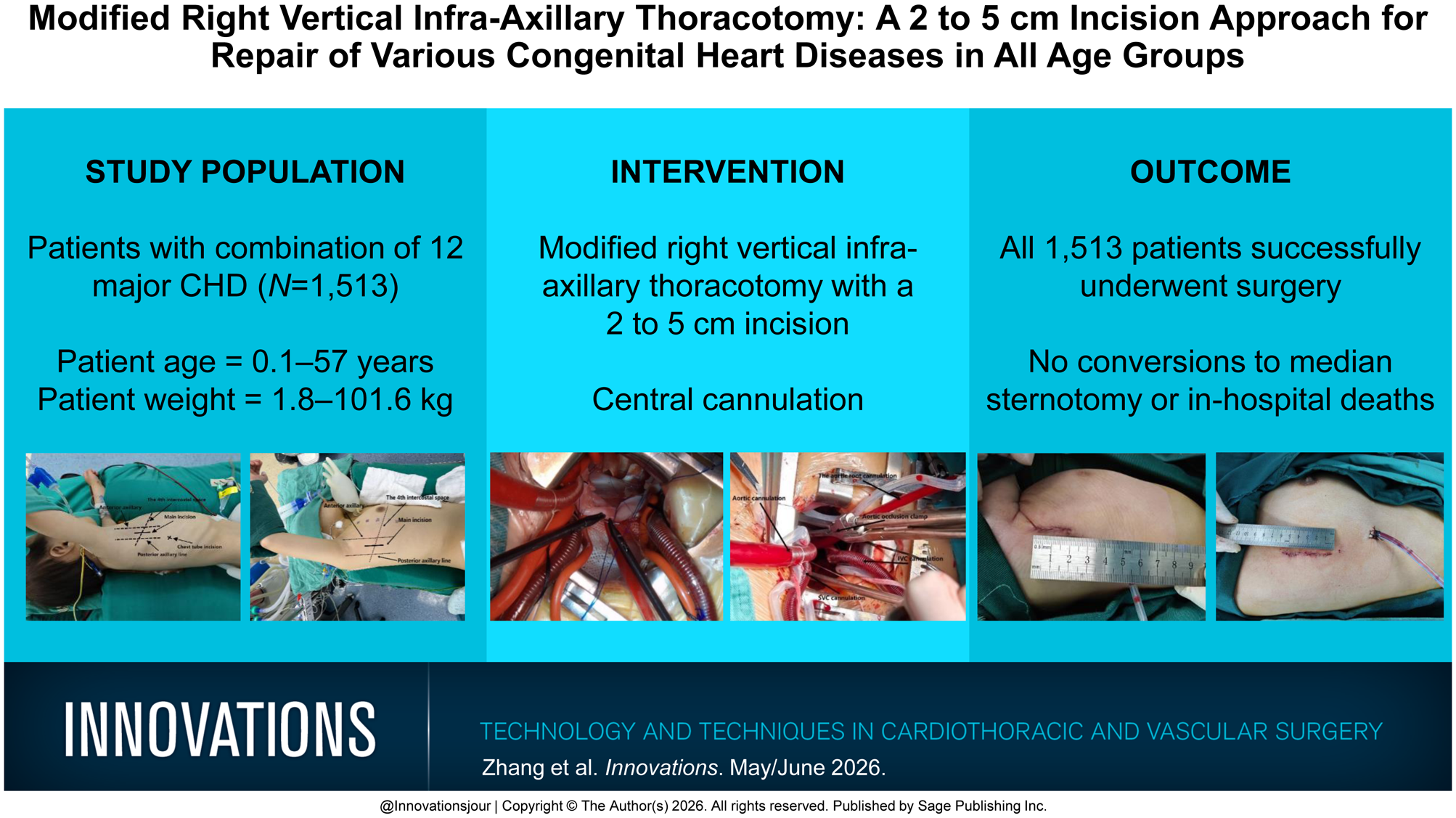
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.