
Abstract
Objective:
As alternatives to conventional coronary artery bypass grafting (CABG), robot-assisted CABG (R-CABG) and percutaneous coronary intervention (PCI) offer less invasive treatments for coronary artery disease (CAD). However, data comparing outcomes of R-CABG versus PCI are limited.
Methods:
Databases were systematically searched for studies comparing R-CABG versus PCI. Random-effects models were used to calculate pooled odds ratios (ORs) with 95% confidence intervals (CIs), both overall and stratified by left main or multivessel (LM+MV) or isolated left anterior descending artery (LAD) disease. Kaplan–Meier curves were digitally extracted to reconstruct individual participant data (IPD), from which hazard ratios (HRs) were estimated for survival analyses.
Results:
Six retrospective studies, including 1,896 patients (R-CABG: 894, 47.1%), were analyzed. The mean age was 63.8 ± 11.3 years, and 78.7% were male patients. Follow-up ranged from 2 to 8 years. Overall, R-CABG was associated with a lower odds of target vessel revascularization (TVR; OR = 0.50, 95% CI: 0.27 to 0.93, P = 0.03) and myocardial infarction (MI; OR = 0.44, 95% CI: 0.26 to 0.76, P < 0.01), with no significant difference in all-cause mortality. Among patients with LM+MV disease, R-CABG reduced TVR and MI. In LAD lesions, R-CABG significantly lowered the likelihood of MI (OR = 0.18, 95% CI: 0.04 to 0.71) as well as major adverse cardiovascular events (MACE; OR = 0.51, 95% CI: 0.28 to 0.93). Time-to-event analysis from reconstructed IPD demonstrated significantly improved freedom from reintervention (HR = 0.31, 95% CI: 0.16 to 0.60) and MACE (HR = 0.24, 95% CI: 0.15 to 0.60) with R-CABG, whereas no significant difference was found for all-cause mortality.
Conclusions:
R-CABG was associated with less TVR and MI compared with PCI in CAD patients, with no difference in all-cause mortality.
This is a visual representation of the abstract.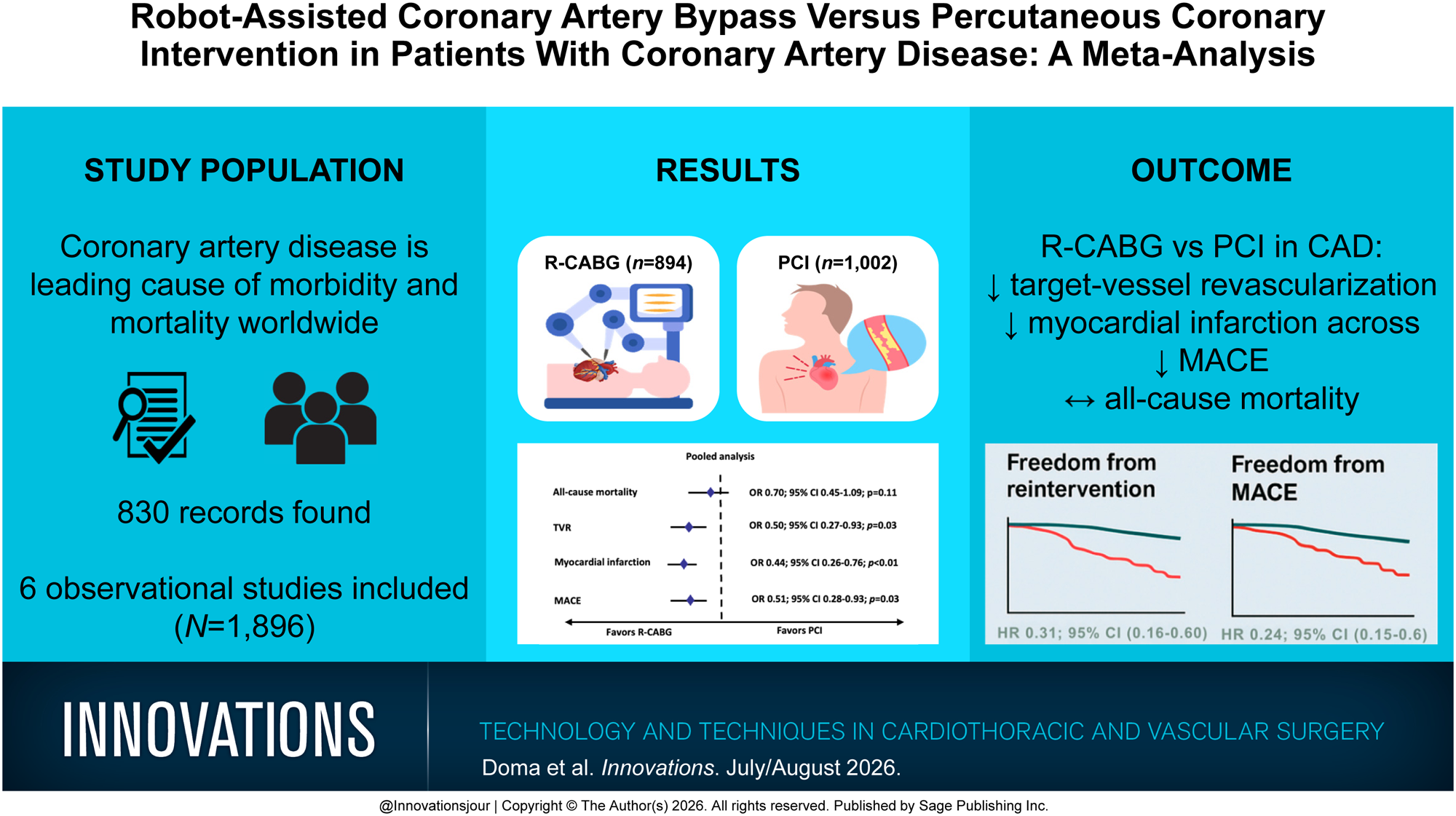
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.