
Abstract
In this article, we provide a feminist perspective on neonaticidal women while critically examining the mainstream literature. We analyze 26 cases reported between 2003 and 2013 in a Portuguese online newspaper. We conclude that neonaticide must be framed by two main lines of thought: Motherhood is a social construction that imposes difficult-to-achieve norms, and it is a complex experience, intercepted by age, social class, marital status, and having other children. This approach should encourage a shift from the present focus on palliative and punitive measures to a more preemptive one including new policies on sexual education and pregnancy termination.
Feminist approaches have made important theoretical contributions to describing the social and cultural dimensions of motherhood while deconstructing the biological perspective through which it is traditionally viewed (Badinter, 1981; de Beauvoir, 1949/1989; Irigaray, 1974/1985; Rich, 1995). However, few feminist studies have focused on the implications of these social constructions for neonaticidal mothers (for important exceptions, see, for example, Alder & Baker, 1997; Dougherty, 1993).
In this article, we offer a feminist approach to neonaticide and neonaticidal mothers and illustrate this approach with an analysis of real-life cases collected from a Portuguese newspaper. We do not claim that these cases are representative of the Portuguese reality. 1 Nevertheless, we believe that these cases allow different conclusions from those reached by the mainstream approach, and encourage new interpretations for future studies in Portugal and elsewhere.
Overall, we conclude that neonaticide must be framed by three main lines of thought: that motherhood is a social and cultural construction (e.g., Badinter, 1981; de Beauvoir, 1949/1989; Irigaray, 1974/1985; Rich, 1995) that imposes difficult-to-achieve norms, particularly for women of disadvantaged social and economic backgrounds; that motherhood is a complex, contradictory experience, particularly for those who do not fit the ideals of traditional femininity; and, finally, that the intersections of age, social class, marital status, and having previously been a mother are crucial in explaining this crime. 2
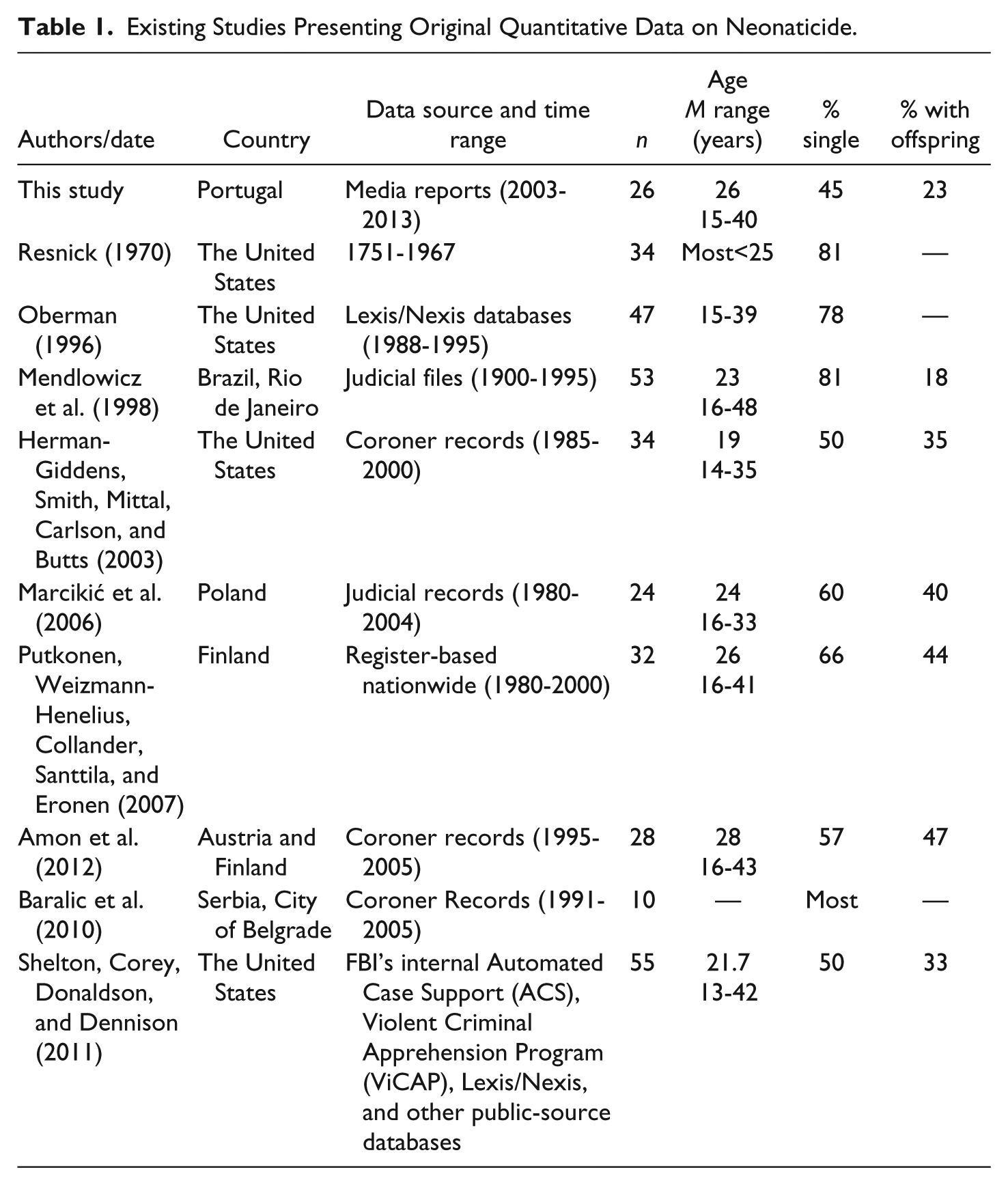
We begin by introducing the underpinnings of the clinical/mainstream approach to neonaticide and proceed by describing the need for a coherent, comprehensive feminist approach to motherhood with respect to this crime. While searching scientific databases for previous studies on this subject, we concluded that the number of articles containing rigorous quantitative data on neonaticide was quite limited. Therefore, we decided to list them all followed by the features that were important to our own results (Table 1).
Existing Studies Presenting Original Quantitative Data on Neonaticide.
Neonaticidal Women: The Mainstream View
Research on neonaticidal mothers originated in the United States with a study by Resnick (1970) that distinguished these women from those who kill their older children. Resnick’s and subsequent studies concluded that unlike mothers who kill their older children, women who commit neonaticide do not typically present major psychological disorders (e.g., Ciani & Fontanesi, 2012; Herman-Giddens et al., 2003; Oberman, 1996; Riley, 2006; Shelton, Corey, Donaldson, & Dennison, 2011).
Neonaticidal women are also described as young, single, and poor. Nevertheless, recent European studies have increasingly reported a larger number of older women (e.g., Amon et al., 2012; Putkonen, Weizmann-Henelius, Collander, Santtila, and Eronen, 2007), most of whom are single (Baralic et al., 2010; Marcikić et al., 2006; Mendlowicz, Rapaport, Mecler, Golshan, & Moraes, 1998; Putkonen et al., 2007; Resnick, 1970; see Table 1). They are also typically described as either having denied their pregnancy or having concealed it from family and friends (e.g., Friedman, Cavney, & Resnick, 2012; Oberman, 1996; Resnick, 1970).
In these studies, one of the primary motives presented for maternal neonaticide is the mother’s lack of resources required to successfully raise a child (e.g., Oberman, 1996). Several authors also discuss the lack of social support from the families or partners of neonaticidal mothers and such mothers’ anticipation of the negative reactions or disapproval of others (e.g., Friedman et al., 2012; Riley, 2006). Other motives include strict religious backgrounds and taboos associated with premarital sex (Friedman & Resnick, 2009; Mendlowicz et al., 1998; Milner, 2000; Oberman, 1996; Riley, 2006; Wessel, Endrikat, & Ulrich, 2003).
Fear of the opinions of and rejection by others correlates with two of the most distinctive features of neonaticidal women: the concealment and denial of pregnancy (Wessel et al., 2003). Concealment describes an active, intentional process of hiding one’s pregnancy from others, whereas denial refers to an inner unawareness of the pregnancy (Wessel et al., 2003). However, even when they are conscious of the pregnancy (and simply conceal it from others), neonaticidal mothers rarely seek medical care. They also tend to deliver alone, increasing the risk of the newborn’s death (Shelton et al., 2011).
A key feature of this clinical-oriented research is its emphasis on the psychological states of the perpetrators and the psychological processes that drive them to commit the crime. For example, emotional isolation, low self-esteem, and negative self-image (Riley, 2006), together with a general apathy regarding the pregnancy (including a lack of birth plans and child care), are psychological states that are regularly observed in these women (Pitt & Bale, 1995; Stanton, Simpson, & Wouldes, 2000).
This psychiatric/clinical line of investigation must be credited with deconstructing the long medical and legal tradition (since the 19th century) that has considered all female offenders who kill their offspring to be either mentally ill or overwhelmed by hormonal shifts (e.g., Pitt & Bale, 1995; Schwartz & Isser, 2000; Shelton et al., 2011; Stangle, 2008; Stanton & Simpson, 2002; Stanton et al., 2000). However, this line of investigation has been unable to show that neonaticide is, not simply motivated by a set of clinical or psychological conditions, but also—and most importantly—a product of cultural norms aimed at controlling both women’s sexuality and motherhood. Therefore, below, we will frame this issue in terms of a transgression of normative motherhood and attempt to show how this normative construction is irreconcilable with many women’s life conditions.
A Feminist Approach to Neonaticide
The prevailing Western ideology of motherhood was established in the 18th century (Badinter, 1981; Giddens, 1992). Until then, children were accorded little social relevance, which made their killing permissible (Badinter, 1981; Thurer, 1994).
Under the influence of economic, political, and philosophical changes, the idea of the modern family (Badinter, 1981; Giddens, 1992; Thurer, 1994) and the institutionalization of motherhood (Rich, 1995) emerged based on three main pillars: the ideal of romantic (i.e., heterosexual) love, the creation of the home as a cellular familial space, and the modification of relationships between parents and children (Giddens, 1992). Simultaneously, a new institutional pedagogy of mothering developed—supported by the literature and science of the period, from Rousseau’s Emile (Badinter, 1981; Thurer, 1994) to Linnaeus’s concept of Mammalia (Schiebinger, 1993)—that advised women to breastfeed. The first example strongly advocated breastfeeding and the ideal of the good wife. The second emphasized breastfeeding—and therefore maternity—as part of the nature of all female mammals. In awarding women new domestic roles and parental power, this discourse confined women to the household, child care, and family circle in general (Badinter, 1981; Rich, 1995; Thurer, 1994).
During the 20th century, male psychologists and psychoanalysts played a leading role in the social construction of motherhood. Sigmund Freud contributed significantly to linking motherhood—particularly “bad mothering”—to psychopathology and considered the mother as the “great responsible [individual]” with respect to the happiness of her descendants (Badinter, 1981, p. 237). Bowlby (1951) claimed, “the infant and young child should experience a warm, intimate, and continuous relationship with his mother (or permanent mother substitute) in which both find satisfaction and enjoyment” (p. 13). For example, Winnicott (1952) introduced the concept of the “good enough mother,” who is able to provide physical and emotional care. As Badinter (1981) suggested, psychiatry and psychoanalysis had the ability to combine morality with psychopathology in such way that “bad mothering” was primarily equated with either “abnormal” femininity or psychopathology.
In the late 1940s, Simone de Beauvoir (1949/1989) refuted the biological determinism according to which motherhood is socially constructed as a woman’s “destiny.” Drawing on her groundbreaking research, second-wave feminists vigorously challenged generalized discourses on maternal instincts and the mother role and questioned the popular ideas that women have a biological compulsion to become mothers and that motherhood is a natural and desirable state for all women. According to this logic, the skills and capacities for caring for children are a natural result of being a woman (Nicolson, 2001).
In the face of these normative conditions of motherhood (i.e., the natural state and the natural skills of motherhood), most of today’s mothers are confronted with the arduous task of being confident and effective 24 hr a day, 7 days a week. Caught between an idealization of motherhood as a natural state and the actual challenges of motherhood, many women feel guilty for being improper, bad mothers (Nicolson, 2001), whereas others “convey positive aspects alongside with some downsides” (Ambrosini & Stanghellini, 2012, p. 279).
As previously stated, the mainstream literature emphasizes, as motives for neonaticide, the mother’s lack of social support from her family, the anticipation of negative reactions or disapproval (e.g., Friedman et al., 2012; Riley, 2006), strict religious backgrounds, and taboos associated with premarital sex (Friedman & Resnick, 2009; Mendlowicz et al., 1998; Milner, 2000; Oberman, 1996; Riley, 2006; Wessel et al., 2003). However, this view of neonaticidal women can be best interpreted through Linda McClain’s (1996) compelling concept of “irresponsible” reproduction, which she used to demonstrate how the popular discourse bestows “individual responsibility” for reproduction upon women. The discourse of “irresponsible reproduction” includes cases of illegitimacy, teenage motherhood, single mothering, and motherhood coupled with economic difficulties, that is, all the situations presented by the traditional literature plus others revealed by our study, as we describe below.
Indeed, “irresponsible” reproduction is attributed to those women who fit the designation of “bad” mother because they transgress traditional norms of sexual morality (e.g., adolescent motherhood or illegitimate sexuality) and the structure of the traditional family (i.e., being single or finding themselves in disadvantageous economic conditions). One can conjecture that the internalization of this discourse by potential neonaticidal women and the resultant guilt regarding their “misbehavior” can contribute to explaining their crime. Subjugated by these mighty discourses, neonaticidal mothers become powerless, unable to define themselves as agents in their own lives, and overwhelmed by contradictory emotions regarding whether to have the child or to seek an abortion. In addition, abortion remains stigmatized not only because it causes the death of the fetus but also because the woman who terminates a pregnancy is, at the same time, rejecting her “natural” mothering role (Abrams, 2014).
Thus, neonaticidal women are trapped in a “double bind” (Bateson, 1972) that prevents them from making a decision. The first injunction asserts that they are unable to be good mothers; the second asserts that if they have an abortion, they will also be bad mothers. Unsurprisingly, given such societal norms and discourses, women may feel divided regarding having an abortion, expressing “both positive and painful feelings such as anxiety, relief, grief, guilt, anguish, emptiness and responsibility, [even if] one-third expressed only painful feelings” (Kero, Hogberg, Jacobsson, & Lalos, 2001, p. 1481). During this period of reflecting on and muddling through dilemmas, the time limit for a legal abortion can elapse, resulting in neonaticidal behavior.
The clinical/mainstream approach neglects the power of motherhood normativity and the conflicts, ambiguities, and ambivalences that derive from the discrepancies between the idealized construction of motherhood and the complexities of real-life experiences:
Having a baby brings about a change in one’s own priorities. It influences preexisting relationships and redefines roles formerly played. While all this happens, mothers are called to handle a new set of tasks, including feeding, nurturing and caring for the baby, playing with him, putting him to sleep and beginning to love him. Mothers will have to redirect their previous mental organization and their previous set of values and needs and cope with the duties and responsibilities of motherhood. (Ambrosini & Stanghellini, 2012, p. 280)
The clinical/mainstream tradition also neglects not only gender’s intersection with several other social categories (including race, ethnicity, age, and social class) but also how these intersections construct a particular position in society that facilitates understanding differences and inequalities among women (Crenshaw, 1991). This approach is particularly relevant in understanding “gender, crime, and justice” (Burgess-Proctor, 2006, p. 27; Chesney-Lind, 2006), as Amanda Burgess-Proctor (2006, p. 28) advocated,
Contemporary feminist criminologists bear the responsibility of advancing an inclusive feminism, one that simultaneously attends to issues of race, class, gender, sexuality, age, nationality, religion, physical ability, and other locations of inequality as they relate to crime and deviance.
The theoretical issues that we have discussed in relation to the social and cultural construction of motherhood, namely, the complexities of the motherhood experience at the societal and individual level, and the relevance of intersectionality for deconstructing the homogeneity of neonaticidal women, frame the analysis that follows.
Study
We used the online version of the Portuguese newspaper Correio da Manhã (Morning Mail), a popular daily newspaper with national coverage, to collect our cases. 3 Cases that occurred between January 2003 (when the newspaper started publishing online news) and December 2013 were selected using the following keywords: “dead baby,” “infanticide,” “murder of baby,” and “fetus.” In addition to clear murder cases, we decided to include cases of suspected murder. In these cases, no evidence could prove whether the child was murdered after delivery or whether it was born dead. However, in those cases, there were strong suspicions that the mother had murderous intentions. The decision to include these suspected murders was made in light of limitations caused by the scarcity of information (Alder, & Baker, 1997). After applying these selection criteria, our final corpus for analysis consisted of 26 cases (17 identified and nine unidentified—the last three rows of Table 2). Although this number might be considered small for the purposes of inquiry, in fact, they are all the population of neonaticidal women between 2003 and 2013 and it resembles the data in other studies (Table 1). Also, we must bear in mind that Portugal is a small country with a population of approximately 10 million.
Offender, Motives, and Crime Characteristics.

Note. Y = yes; — = not mentioned by the news; C = confirmed murder; SN = suspected neonaticide.
Using manifest content analysis (Bardin, 1977) and following the aspects generally focused on by mainstream studies, we coded 26 cases based on three dimensions: (a) offender and pregnancy characteristics (17 identified cases), (b) offender motives (for only nine of the 17 identified cases), and (c) crime characteristics (for 11 cases; see Table 2).
Results and Discussion
Offender and Pregnancy: Diversity and the Double Bind
Instead of trying to find commonalities and patterns of regularities as in mainstream studies, our interpretation of the data emphasizes the diversity of the women in this population and the intersection of age with marital status, social class, and being (or not being) a mother prior to the crime. In this section, we focus on these women’s demographic characteristics and the strategies they used to conceal pregnancy.
Regarding demographic characteristics, the mean age of the 17 offenders was 26.48 years (SD = 7.31). As shown above, although these ages differ widely from those of studies conducted in the United States (Table 1), they resemble those found in studies conducted in European countries and Brazil. This difference between the United States and Europe is likely explainable by differences in their respective political, social, and economic environments resulting in distinct types of motherhood and transgression.
The ages of the perpetrators ranged from 15 to 40 years, indicating that this crime is committed not only by young girls but also by older women. The substantial diversity in this demographic characteristic encourages us to consider different motives for the crime, as discussed in the “Motives: Intersectionality and ‘Irresponsible’ Reproduction” section.
The results also indicated that 45% of the women reported their marital status as single, which is clearly lower than the percentages reported in other studies. It is noteworthy that this sample included more women with partners, indicating that being single might not be a primary condition for this crime (e.g., Oberman, 1996, Table 1). Four of the women had other offspring, which is a lower number than that found in most of the studies considered.
Thus, we believe it is worth emphasizing the heterogeneity of these women in terms of their ages (there were both adolescents and women nearing their 40s), marital status (there were both married and single women), and whether they had other offspring. Such diversity prevents the reduction of the present sample either to a simple profile or to a fixed identity or behavior.
The data also show that there was concealment of pregnancy in most of the cases suggesting that these women thought coldly on the possibility of making their newborns “disappear,” that is, either by killing or by abandoning them. However, the data also reveal the difficult social and economic conditions that these women had to bear with respect to the idealistic norms of motherhood (e.g., Badinter, 1981; de Beauvoir, 1949/1989; Irigaray, 1974/1985; Rich, 1995). We might suppose that the frequently used strategy of concealment reflects the double bind (Bateson, 1972) in which these women become trapped and that forces them to “choose” between two ways of being “bad” mothers: either by having the child under questionable conditions (i.e., being single, having other children, and being under economic limitations) or by having an abortion and suffering the associated social stigma (Abrams, 2014).
In nine cases considered in this study, the perpetrator concealed her pregnancy from friends, family, and colleagues. In the cases under study, concealment occurred among single women, those who lived with a partner, women who had children, women without children, and women of all ages. This outcome again emphasizes the heterogeneity of the women who commit this crime. The media describe concealment in diverse ways, indicating that women use different strategies to hide their pregnancies. Several women were even able to conceal their pregnancies from their partners. For example, a 36-year-old woman (Case 4) told her family and friends that she had a fibroma that caused stomach distension. She told them that she had visited a doctor who promised that surgery would solve the problem (Laranjo, 2008). An 18-year-old female (Case 1) hid her pregnancy, even from her boyfriend, by wearing baggy clothes. Near the end of her pregnancy, she told friends in Internet chat forums that “the nightmare was ending” (Laranjo, Oliveira, & Pereira, 2010). Finally, a 37-year-old woman (Case 17) hid her pregnancy by telling relatives and friends that she had fibromas. Ultimately, a doctor who treated her for a hemorrhage in the hospital emergency room alerted the authorities.
These details from news reports document the intentions of the offenders to make their newborns disappear, dismissing the obsolete assumptions that the women were influenced by hormonal or other biological triggers and confirming current beliefs regarding their conscious execution of these acts. In terms of determining a profile for neonaticidal women, as traditional approaches often attempt to do, this heterogeneous group of women—in terms of age, marital status, and parental status—again reveals how such attempts are somewhat artificial. For instance, although most of the women in our sample were from socially and economically disadvantaged backgrounds, students and members of the military were also included.
Motives: Intersectionality and “Irresponsible” Reproduction
To understand the complexities that surround “irresponsible” reproduction (McClain, 1996), it is important to comprehend the motives of this crime and how these motives intersect with the demographic characteristics of the neonaticidal mothers. Although we only have nine cases in which motives were declared, given their consistency, we can infer that information regarding the motives in the remaining cases, if available, would not indicate a radically different pattern, as occurs when qualitative data are theoretically saturated (i.e., when no new data emerge; see Glaser, 1978).
As shown in Table 2, we grouped the motives into three categories: psychological/cognitive difficulties, fear of parental or societal reactions, and economic difficulties. Typically, given the complexities of motherhood in these women’s lives, these categories overlap, indicating the existence of two or more motives for the crime. For instance, five cases indicate economic difficulties as a motive. However, such difficulties were only identified as the sole motive in one case (Case 4). In two cases (Cases 5 and 11), the offenders’ disabilities and economic difficulties were mentioned. In Case 6, depression and economic difficulties were mentioned, and in Case 10, fear of societal reactions and economic difficulties were mentioned. Four cases mentioned fear of societal reactions as the motive. However, fear of the reactions of parents or the community was cited as the sole motive in only three cases. Case 2 was the only case in which depression was mentioned without reference to economic problems or fear. The existence of multiple motives in most of the cases reveals the close interrelations between these motives and indicates the complexities and hardships of many of the offenders’ lives, which might be considered capable of transforming motherhood for these women into a much more difficult condition than usual (Abrams, 2014; Alder & Baker, 1997; Ambrosini, & Stanghellini, 2012; Dougherty, 1993).
By considering the intersections among the women’s demographic characteristics, we can observe that older offenders were involved in most of the cases in which the media mentioned economic difficulties. A 36-year-old woman with three children (Case 4) claimed that constant quarreling with her husband over the lack of money caused her to conceal her pregnancy and eventually murder her newborn. A 33-year-old woman and a 38-year-old woman (Cases 11 and 5, respectively) experienced precarious economic situations, and the latter was additionally challenged by borderline intellectual disability. A 40-year-old woman (Case 6) with a 20-year-old daughter also reported being unemployed and suffering from depression.
A younger woman in our sample (Case 12) served in the military and hid the postpartum fetus in the trunk of her car. In terms of motive, “fear of disappointing the family might have been another reason for this woman to hide what happened. [She] also feared destroying the [military] career she had dreamed of all her life” (Fonseca, Laranjo, & Pinto, 2012). Indeed, it seems that most of these women generally commit neonaticide for one of two reasons (if not both): It is not the right time to have a child or they do not have the right partner. As a case in point, these are also the two main justifications Kero and collaborators (2001) have identified among women who decide to abort.
Although the news reports only explicitly identified economic difficulties as a motive in five cases, most of the reports described the women as having low socioeconomic status. This finding supports the hypothesis that poverty and unemployment are closely related to a higher incidence of child homicide (Alder & Baker, 1997; Gauthier, Chaudoir, & Forsyth, 2003), likely because economic difficulties cause the offender to anticipate insufficient resources to raise the child. In cases of mental disease, such as intellectual disability or depression, poverty also decreases the likelihood of obtaining effective health care or assistance in preventing or addressing unwanted pregnancy.
In this regard, it is important to emphasize that Portuguese woman generally participate in the labor market at higher rates (85.6%) than other women in the EU-27 (European Union-27 Member States; 76.6%) and endure more segregation and unsatisfactory working conditions (European Institute for Gender Equality, 2013). These circumstances have indirectly affected the national birthrate, which is extremely low. 4 In contrast, the birthrate among adolescents (i.e., the annual number of births per 1,000 women ages 15 to 19 years) is extremely high (15.6% in 2012) compared with that of other countries 5 (see United Nations, 2015). This phenomenon may be partially attributable to inadequate sex education and the perception among lower class adolescents that having a child is the only way to escape the parental home (Granja, Cunha, & Machado, 2012).
As might be expected, given these characteristics of Portuguese culture, young adults or adults who live with their parents reported pregnancy concealment because they feared their parents’ reactions. In three cases, this fear was the only reason mentioned. In Case 9, a 26-year-old woman hid her pregnancy from her parents, with whom she lived, out of shame and because a married man had possibly fathered the child (Gomes, 2005). Again, this woman did not have “the right partner” with whom to have a child (Kero et al., 2001). In Case 12, the woman wanted to find a way to abort her child. However, it was too late. Her mother helped her conceal the pregnancy until the end “because she was afraid of the father” (Lopes, 2008). These cases illustrate the pressure exerted by traditional values in Portuguese society through the family and the surrounding community. In addition, they reveal that the bureaucratization of legal abortion in Portugal may compromise access to this procedure 6 and that the period during which an abortion is legal in Portugal may be too short for women who realize that they are pregnant relatively late. 7 If the absence of physiological symptoms is combined with the previously described “double bind”—“irresponsible” reproduction (McClain, 1996) combined with stigmas associated with abortion (Abrams, 2014)—we realize that young, poorly educated women who are vulnerable because of personal or economic conditions encounter a highly complex set of circumstances when confronted with an unwanted pregnancy.
Finally, in a single case, psychological problems were mentioned as the only reason for neonaticide (Case 2): A young student who resisted everyone opposed to her pregnancy (because they feared the baby would have birth defects). She badly wanted to have the child. However, she suddenly disappeared for a week. When she returned, she was no longer pregnant and refused to state what had happened to the baby (Laranjo, 2013). This case is the only case out of eight with declared motives that can be considered primarily driven by the offender’s psychological disturbances.
Although mainstream research simply lists perpetrator demographics such as age, marital status, and parental status without discussing them (see Table 1), we believe that demographic information is a crucial aspect to consider if we are to obtain a full understanding of the criminal behaviors of these women. For instance, older women who have other children occupy a seemingly contradictory position regarding motherhood, highlighting the contextual and transitory nature of their behavior. These women are paradigmatic in terms of deconstructing motherhood as something intrinsic to women that inevitably guides their behavior regardless of their circumstances. Indeed, these cases reveal that women who have always adhered to the “correct” standards of motherhood may violate these standards when constrained by their social or economic context. Thus, the “good” or “bad” mother identities—“once a good mother, always a good mother” (e.g., Saavedra, Cameira, Rebelo, & Sebastião, 2017)—are not fixed, rather they strongly depend on their contextual backgrounds and the discourses on motherhood and abortion that circulate in society. Instead of assuming these criminal women exhibit essentialist characteristics (which results in the profiling of neonaticidal women), this crime should be framed by a social constructionist perspective of motherhood. Motherhood should be viewed as a choice that is shaped not only by certain social categories (e.g., age, marital status, religion, and race) but also by contextual factors, as occurs in voluntary terminations of pregnancy (Kero et al., 2001).
Crime Characteristics: Deconstructing the Kind Mother
The manner in which a neonaticide is perpetrated, with more or less recourse to violence, deconstructs the established patriarchal characterization of motherhood and femininity based on kindness and delicacy (e.g., Neroni, 2005; Stangle, 2008), particularly because these women are not considered mentally disturbed (e.g., Oberman, 1996; Resnick, 1970). The methods used to accomplish these crimes are important aspects of news coverage because violent behavior such as strangulation with the umbilical cord (Case 1) or drowning in a toilet (Case 14) clearly challenges the widely shared stereotype of the caring mother, attracting public attention. There was a case in which a nonidentified woman killed her newborn by injuring its head; in another, a member of the military (Case 12) incinerated her dead newborn to conceal the corpse. We also found cases characterized by behavior that was less violent, such as the woman (Case 9) who abandoned her newborn in a bandstand. Regardless of their level of violence, we think that these behaviors support the idea that women are not instinctively or biologically predisposed to conform to an idealized discourse of motherhood (e.g., Badinter, 1981; de Beauvoir, 1949/1989; Irigaray, 1974/1985; Rich, 1995). We agree with Dougherty (1993), in that this type of crime shows that whereas these women may be victims of societal rules under which they feel powerless, they can become agents of their own “decisions,” even if these decisions are permeated by conflict and ambivalence and occasionally by confused psychological states.
Concluding Statement
As we conclude this article, there are several main ideas that seem important to restate. First, we consider the clinical/mainstream approach insufficient to provide a comprehensive explanation of neonaticide, primarily because it neglects the role of society in defining the norms of motherhood. In this literature, women are perceived as gender-neutral entities. In addition, such an approach fails to persuasively explain why only women perpetrate this crime and do not try to clarify why these women do not choose abortion.
By avoiding the issues involved in normative motherhood, mainstream literature emphasizes the personal disposition of the perpetrator. For us, more than a theoretical debate is at stake. More important is the type of intervention that these approaches encourage. That is, whereas the feminist approaches tend to support public policies that can improve the lives of disadvantaged women—in fact of all women—to prevent these crimes, the clinical approach tends to uphold palliative interventions and retributive measures (e.g., imprisonment) for female offenders, which are implemented after the crime is committed.
Public policies are not easy to change, particularly when a country, such as Portugal, is experiencing a severe economic crisis. However, a first step could be to create a national database with information on neonaticide and filicide of older children, both to monitor the extent of this criminal reality in Portugal and to develop policies accordingly.
Ideally, we believe that there are two important areas of intervention. First, the state should invest more in education, particularly sex education, including parental education, which should better equip parents to more directly address their children’s sexuality. Second, given the low birthrate, the state should promote a realistic policy on childhood and childbirth and create better conditions for parents to support their children. In addition, as an immediate response to neonaticide, the state should consider lengthening the period during which abortions can be legally performed and promoting access to anonymous deliveries (i.e., services that deliver babies without requiring women to be identified by name and that place the newborns with adoptive families). Such services safeguard women’s health and children’s lives; studies in Austria have demonstrated that their implementation has substantially reduced neonaticide (Klier et al., 2013).
Above all, conditions should be created for women to be truly free from traditional norms of sexuality and motherhood so that they can choose to be mothers when they want (independently from their age) and how they want (independently from their economic and marital status), without external conditions and social norms that constrain their wishes. The same could be said concerning fatherhood as men who assume this role could also benefit from such changes in traditional norms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted at Psychology Research Centre (UID/PSI/01662/2013), University of Minho, and supported by the Portuguese Foundation for Science and Technology and the Portuguese Ministry of Science, Technology and Higher Education through national funds and co-financed by FEDER through COMPETE2020 under the PT2020 Partnership Agreement (POCI-01-0145-FEDER-007653).