
Abstract
Pregnant incarcerated women pose unique challenges in jails and prisons. Many states still require or permit the shackling of pregnant incarcerated women throughout the pregnancy and during labor, delivery, and recovery. This study includes a content analysis of shackling laws and policies currently in effect throughout the United States. The findings identify the range of shackling laws and policies at the state level and whether these laws and policies adhere to a female indifferent or gender-specific orientation. Finally, the implications are discussed to assist lawmakers and correctional administrators in understanding the effects and potential outcomes of certain types of laws and policies.
Introduction
On October 15, 2013, Juana Villegas received a US$490,000 settlement, because she was shackled to a hospital bed while giving birth in Nashville, Tennessee. A federal court found that the jail officers had shown deliberate indifference to the medical needs of Villegas by having cuffed her ankle to the hospital bed through most of her labor and recovery (Preston, 2013). Recently, there have been federal civil lawsuits filed against correctional facilities and staff members claiming that there was deliberate indifference demonstrated in the shackling or use of mechanical restraints on incarcerated women during pregnancy or during transportation to medical facilities for pregnancy-related care. This has led to an increase in media coverage regarding the practice of shackling pregnant incarcerated women.
Proponents report the laws and policies are necessary to protect correctional staff, judges, medical personnel, and members of the public from harm and to prevent flight. The proponents generally argue that the correctional staff should decide whether or not a pregnant incarcerated woman should be restrained, and the issue should be dealt with on a case-by-case basis (Harvard & Schwartzman, 2013). Conversely, critics argue that the shackling of pregnant incarcerated women is unnecessary and may constitute cruel and unusual punishment, violating the Eighth Amendment of the Constitution of the United States (Sichel, 2007; U.S. Const., Amend. VIII).
The current study includes a content analysis of the shackling laws and policies in effect in each state (as of December 22, 2015) to develop a typology of these laws and policies throughout the United States. The purpose of this study is to determine the degree of consonance between current shackling laws and policies and the viewpoints of proponents and critics. Specifically, this study examines whether current shackling laws and policies adopt a female indifferent or a gender-specific orientation. The study is anchored in Binion’s (1993) discussion regarding the impact of gender neutrality in the law. Proponents of broad shackling policies argue that giving discretion to correctional officers in determining whether restraints should be used is justified. In addition, proponents adopt a female indifferent stance relative to shackling laws and policies. In other words, in the pursuit of equal protection and in an attempt to treat all inmates equally, proponents may overlook certain legitimate gender differences, such as pregnancy. Critics believe that restraints are being used on pregnant incarcerated women as the default practice when shackling should be the rare exception. In addition, critics argue that shackling laws and policies should reflect a gender-specific orientation and should recognize the dangers of shackling incarcerated women who are pregnant. The findings are reported and the implications are discussed to inform lawmakers and correctional administrators about the issue of shackling pregnant incarcerated women.
Background
Pregnant Incarcerated Women: A Unique Subpopulation
Approximately 6% to 10% of the women entering the criminal justice system each year are pregnant and there are about 2,000 births per year to incarcerated women (Quinn, 2014). Pregnancies in correctional facilities are often considered high risk due to the prevalence of alcohol and substance abuse, smoking, and sexually transmitted diseases in this population (Hotelling, 2008). In addition, there is variation in access to prenatal and perinatal care in American prisons and jails, which further increases the incidence of high-risk pregnancies. Collectively, these factors lead miscarriages and cellblock births, which contribute to newborn deaths, to be commonplace (Roth, 2006). Incarcerated women and their fetuses are in danger of high-risk pregnancies without the proper treatment and care (Cardaci, 2013). According to Cardaci (2013), failure to provide adequate care costs society more than the provision of care, especially when the consequences could have been avoided.
The mechanical restraints used to shackle incarcerated people and limit movement include handcuffs or flex cuffs (i.e., zip ties), waist chains, and leg irons (Sichel, 2007). Handcuffs and zip ties are restraints that tether an inmate’s wrists together. Handcuffs can also be used to secure an incarcerated person to a hospital bed. A waist chain is a chain that is wrapped around an inmate’s torso and then the inmate’s cuffed hands are secured to the chain. Leg irons use a chain to closely tether an incarcerated person’s ankles, which impairs his or her ability to walk or run. In addition, leg irons can be used to secure an incarcerated person to a hospital bed. Historians believe that shackling pregnant incarcerated women became common in the 1970s and 1980s, a period subsequent to the initiation of the civil rights and women’s rights movements, both of which were focused on equality. Sexual equality was often interpreted to mean treating men and women equally in all circumstances. It was during this time that the criminal justice system returned to largely female indifferent laws and policies (Mastony, 2010); these are laws and policies initially developed for use with incarcerated men and were subsequently applied in the same way to incarcerated men and women. Female indifferent shackling laws and policies are the ones that require or permit that most incarcerated people, regardless of gender or condition, are to be restrained when transported off prison or jail grounds (Griggs, 2011; Mastony, 2010). In other words, female indifferent shackling laws and policies treat all prisoners equally and do not consider legitimate gender differences.
Proponents’ Arguments for Allowing the Shackling of Pregnant Incarcerated Women
American prisons and jails commonly utilize the practice of shackling for pregnant incarcerated women during their pregnancy, labor, delivery, and recovery (Allen, 2010). There are two justifications for shackling pregnant incarcerated women. The first justification is that it is necessary to protect correctional staff, judges, medical personnel, and members of the public from harm. The second justification is that it is necessary to prevent escape. Other than courthouses, medical facilities are the only publicly accessible places where incarcerated people are frequently transported (Mason, Burke, & Owen, 2013). Correctional staff members need to be aware of the possible dangers associated with transporting inmates to and from public places.
Protecting correctional staff, judges, medical personnel, and members of the public from harm
The correctional staff have a duty to ensure the safety of their staff, judges, the medical staff, and members of the public from harm (Mason et al., 2013). This duty requires the correctional staff to be confident in their security measures and aware of any security and safety concerns. The security of incarcerated people is vitally important to the safety of the correctional staff, judges, medical personnel, and members of the public, especially as transporting them to medical facilities can be a risky endeavor (Mason et al., 2013; Schiffner, 2011). According to Schiffner (2011), correctional staff members may relax toward the end of a transport, because they are almost back inside correctional facilities and they know the transportation to the medical facilities went smoothly. However, incarcerated people often become agitated near the end of the transport, because they are also aware of their imminent return to their respective correctional facilities. Correctional officers are sometimes assaulted by incarcerated people immediately after the restraints are removed (Schiffner, 2011). Schiffner also reported that the end of a transport is when most escape attempts occur.
Preventing escape
Researchers who study inmate transport suggest that correctional staff should assume that all incarcerated people are flight risks and that they will seize an opportunity if there is a security breach (Mason et al., 2013; Schiffner, 2011). Other research suggests that incarcerated people will act on impulse rather than considering the consequences of an escape attempt (Culp & Bracco, 2005). Culp (2005) found that 92% of incarcerated people who escaped acted alone or in pairs and that most of them did not plan the escape in advance—Escape attempts were spur-of-the-moment decisions. Incarcerated people will use to their advantage inattentive staff or defective security technology (Culp, 2005). In addition, Culp and Bracco (2005) found that all incarcerated people, regardless of characteristics, are equally likely to attempt escape. This conclusion provides evidence to justify female indifferent shackling laws and policies. Accordingly, proponents support the shackling of pregnant incarcerated women and believe the decision to use restraints on pregnant women should be made by the staff members on duty on a case-by-case basis (Harvard & Schwartzman, 2013).
Critics’ Arguments Against Shackling Pregnant Incarcerated Women
Various national medical and advocacy organizations, including the American Medical Association (AMA), the American Congress of Obstetricians and Gynecologists (ACOG), the American College of Nurse-Midwives (ACNM), the American Public Health Association (APHA), and the American Civil Liberties Union (ACLU), oppose shackling pregnant incarcerated women for multiple reasons. These organizations adopt a gender-specific orientation that distinguishes pregnancy from other medical conditions. In addition, these organizations recognize that there are gender differences that need to be taken into consideration. In this instance, the gender difference that needs to be considered is that women can become pregnant and men cannot. Furthermore, it needs to be considered that pregnancy carries with it a set of specific medical and safety needs. The American Correctional Association (ACA) also recommends substantial restrictions on the use of restraints with pregnant incarcerated women.
Unacceptable risk to the women’s health
All five medical and advocacy organizations argue that a pregnant woman should not be shackled when she goes into labor. The woman needs to be able to freely move, because she will be more prone to injury if movement is impaired by shackles (ACLU, n.d.-a; ACNM, 2012; APHA, 2013). Research has shown that the use of abdominal and leg shackles while the woman is in labor can lead to bruising and leg shackles can cause severe cuts, because of the strain childbirth can put on the woman’s body (Sichel, 2007). In addition, shackling a woman during labor and delivery can interfere with the medical staff’s ability to assist during the process (ACNM, 2012; ACOG, 2011). Shackling during the postpartum period increases the risk for thromboembolic disease (i.e., blood clots) and postpartum hemorrhage, because a woman’s movement is restricted (ACLU, n.d.-a).
Unacceptable risk to the health of the fetus
A woman’s center of balance is altered when she is pregnant. If she is shackled, then her likelihood of falling is increased and her ability to break her fall is decreased, which leads to the increased risk of personal and fetal injuries (ACNM, 2012; Ehrlich & Paltrow, 2006). If an emergency cesarean delivery (C-section) is necessary, then the delay associated with restraint removal can pose a threat to the fetus (ACNM, 2012). Even a delay of 5 min is enough to cause permanent brain damage to the child (Amnesty International, 2000). When the child is born, mother and child bonding is important to a child’s development (Cassidy et al., 2010; Goshin, Byrne, & Blanchard-Lewis, 2014), and this process is impaired if the mother is shackled (ACOG, 2011). In addition, if a mother is shackled, then her ability to breast-feed is impaired, which further impedes the bonding process between her and her child (Padmavathi, Jayadeepa, & Babu, 2014).
Violation of the Eighth Amendment right
The five medical and advocacy organizations argue that shackling women during their pregnancies represents deliberate indifference to the women’s medical needs. This deliberate indifference violates Eighth Amendment protections from cruel and unusual punishment (Estelle v. Gamble, 1976; U.S. Const., Amend. VIII). The U.S. Supreme Court declared it an obligation for American correctional facilities to provide adequate medical care, because incarcerated people rely on correctional staff to address their medical needs. It constitutes cruel and unusual punishment when staff members know of a prisoner’s medical needs, but do not arrange for adequate medical care (Thompson, 2010). The medical and advocacy organizations argue that there is no evidence to support the justifications utilized for shackling, because most incarcerated women are nonviolent offenders without any history of escape. The evidence marshaled by critics counters the case-by-case standard advocated by proponents and suggests that shackling these women may constitute deliberate indifference to their medical needs.
Shackling should be an exception
There have been no reported escape attempts by pregnant incarcerated women who were not shackled during their childbirth processes (ACLU, n.d.-a; ACOG, 2011). ACNM and AMA argue that restraints are only appropriate when a legitimate need to protect the woman, her baby, or staff arises, and that being a flight risk is not a realistic justification (ACNM, 2012; AMA, 2010). If restraints are necessary, then the restraints should be the least restrictive option appropriate for the situation. This means that the restraints used should restrict the woman’s movement as little as possible and should never include shackles that impair leg movement or impair a woman’s ability to break her fall (ACOG, 2011). Furthermore, a report explaining the reasons for the use of restraints should be filed and reviewed by a third party. The third party should be an external body that is not associated with the respective department of corrections (ACOG, 2011).
Views of the ACA
The ACA supports restrictions on the use of restraints on pregnant incarcerated women. The ACA Delegate Assembly unanimously ratified the Public Correctional Policy on Use of Restraints With Pregnant Offenders (2012-1) in January 2012. This policy indicates that female offenders should be restrained in the least restrictive method possible when it is reasonably known they are pregnant to provide for [the] safety of the unborn fetus/child and offender during arrest situations, transport, labor, delivery, and the postpartum hospital stay. (ACA, 2012, p. 99)
The use of restraints should be based on correctional or medical staff’s determination that the incarcerated woman poses an immediate and serious risk of harm to herself, the fetus, staff, or the public; the determination of the medical staff that restraints are necessary to facilitate a safe delivery; or the determination of the chief correctional administrator or designee that the woman poses a significant risk of escape that “cannot be reasonably managed with other methods” (ACA, 2012, p. 99). Furthermore, the ACA (2012) indicates that waist chains should not be used at any point during pregnancy; electronic restraints should not be used during pregnancy, labor, or delivery; and that leg irons should only be used during transport under extreme circumstances and should never be used during labor or delivery.
Theoretical Framework
The shackling of pregnant incarcerated women is at the intersection of gender, law, and policy. The rich body of research guided by feminist theory demonstrates that the intersection of gender, law, and policy is not a new topic. Binion (1993) explained the evolution of women’s equality starting in the 1970s with a critique of classifications based on sex. These gender-specific laws and policies assigned privileges and punishments according to gender or sex (McCorkel, Schmitt, & Hans, 2001). The initial reform focus was on shifting the focus from sex differences to achieving gender neutrality in the law. Gender neutral laws and policies afford men and women identical consideration (McCorkel et al., 2001; Williams, 1989). By the late 1970s, feminist theorists began to recognize that gender neutrality or blindness was not the route to sexual equality, because the effect of neutral laws is not always equal treatment and they may “not effectively incorporate women’s experiences into public and organizational policy” (Binion, 1993, p. 141; see also Golden, 1991; Littleton, 1987; Rhode, 1990). Specifically, female indifferent law fails to consider situations in which men and women are not similarly situated, such as the unique condition of pregnancy (Dworkin, 1981; Hatcher, 2003; McCorkel et al., 2001; Scales, 1986; West, 1988). However, this theoretical approach has not been applied to discussions of the shackling of pregnant incarcerated women. The discussion of gender neutrality or indifference to legitimate differences related to sex (e.g., pregnancy) and gender specificity in law and policy will frame this study and represents a new avenue of inquiry in feminist theory.
Current Study
Overview of the Study
This study includes a content analysis of the shackling laws and policies currently in effect throughout the United States, which is used to produce a typology. The typology classifies shackling laws and policies on a continuum from entirely female indifferent (which tend to ignore medical evidence and policy positions of national medical and advocacy associations) to entirely gender-specific (which acknowledge medical evidence and the different needs of pregnant women, and comply with all recommendations) orientation. The following two research questions are explored in the study:
Method
Procedure
A content analysis was conducted to produce a typology that was used to answer the two research questions. The study 1 includes data on all state law and state departments of corrections policy regarding the shackling of pregnant inmates. In addition, there is an examination of whether the laws and policies adhere more to a female indifferent or a gender-specific orientation. The content analysis method was chosen, because it is a useful method for analyzing documents for trends and patterns to better understand the phenomena under study (Elo & Kyngas, 2008). In addition, it is a research method that allows researchers to make valid and replicable inferences from data (Krippendorff, 1989; Weber, 1990). This method was used to identify patterns in the content of laws or policies to determine whether the laws or policies adhere more to a female indifferent or gender-specific orientation.
Materials
Westlaw, LexisNexis, and government websites were used to locate each state’s statutes and departments of corrections policies. Westlaw is a database that provides access to statutes, federal regulations, court cases, and law reviews. LexisNexis is a database that provides access to legislation and case law, as well as articles from national and international newspapers. One site sponsored by the ACLU (n.d.-b) titled “State Standards for Pregnancy-Related Health Care and Abortion for Women in Prison—Map” was used as a supplemental source in locating laws and policies.
Research Questions, Methods, and Analyses
Research Question 1
First, all shackling laws or policies were examined to determine whether each state had a law or policy addressing the shackling of pregnant incarcerated women. The differences between a law and a policy include how they are developed, how they are enforced, and how the consequences of noncompliance are handled. Laws are the set of rules or norms of conduct for the public or governments to follow (Gupta, 2001). A legislative body can enact a law. A policy consists of a regulatory measure, a plan to ensure compliance with law or to provide guidance if a law does not exist, and funding priorities that concern a certain topic (Kilpatrick, 2000). Agencies such as departments of corrections will have policies authorized under law.
Information was collated from the following 13 nominal items:
Can handcuffs be used on a pregnant incarcerated woman at any time in her pregnancy?
Can a waist chain be used on a pregnant incarcerated woman at any time in her pregnancy?
Can leg irons be used on a pregnant incarcerated woman at any time in her pregnancy?
Can a pregnant incarcerated woman be shackled if she is a safety concern?
Can a pregnant incarcerated woman be shackled if she is a flight risk?
Can a pregnant incarcerated woman be shackled with any form of restraint during her first trimester?
Can a pregnant incarcerated woman be shackled with any form of restraint during her second trimester?
Can a pregnant incarcerated woman be shackled with any form of restraint during her third trimester?
Can a pregnant incarcerated woman be shackled during labor?
If a medical emergency arises, can the restraints be removed?
Can a pregnant incarcerated woman be shackled during delivery?
Can a pregnant incarcerated woman be shackled during recovery after childbirth?
If a pregnant incarcerated woman is shackled, then is a report required from the correctional staff member on duty?
Each nominal item is worth 1 point. The first 12 items use reverse codes. For the first 12 items, if the response is “yes,” then the state received 0 points, and if the response is “no,” then the state received 1 point. The last nominal item is a standard code where the answer of “yes” meant the state received 1 point and the answer of “no” meant the state received 0 points. The nominal items were aggregated to produce the typology. Fewer points received from the nominal items indicated a higher adherence to the female indifferent orientation. A higher number of points indicated a greater adherence to the gender-specific orientation. In other words, laws or policies with a greater focus on or acknowledgment of the gender differences associated with pregnancy received more points. If no law or policy were found, then research was conducted to gather supporting evidence that the state does not have a law or policy in place. In addition, an attempt to contact the state’s department of corrections was made to determine whether a state did or did not have a law or policy. Interrater reliability for the nominal items was assessed using Cohen’s kappa. This statistic was selected, because there are two raters, the data are nominal, each variable is dichotomous, and the response categories are mutually exclusive (Kvålseth, 2015).
Research Question 2
Second, the content analysis was used to create a typology to determine where each state’s law or policy fell on a continuum from an entirely female indifferent orientation to an entirely gender-specific orientation. The typology was created using cluster analysis in SPSS. The two-step cluster analysis was used to identify clusters of states that adhere to female indifferent or gender-specific orientations.
The distribution of states’ shackling laws and policies on this continuum will provide insight into how legislators and correctional administrators approach pregnancy during incarceration. It can be suggested that more of the states’ legislatures and correctional institutions place greater emphasis on inmates being safety and flight risks if a higher percentage of states adhere to a female indifferent orientation. This is defined as the combination of states that entirely adhere to a female indifferent stance and states whose laws and policies reflect a combination of female indifferent and gender-specific elements. Conversely, if there is a higher percentage of states that entirely or primarily adhere to the gender-specific orientation, then it can be suggested that more of the states’ legislatures and correctional institutions place greater emphasis on recognizing that legitimate gender differences exist.
Results
The content analysis revealed variation in laws and policies and yielded several patterns. The typology and the number of states in each category suggest that shackling laws and policies reflect a primarily female indifferent orientation.
Research Question 1
A content analysis was conducted on the current state shackling laws and policies throughout the United States to answer the first research question. Information on laws or policies was found for 48 states. Michigan and New Jersey were classified as “unknown,” because information was not found. In addition, the state departments of corrections provided no information or inadequate information regarding the shackling laws or policies that specifically involve pregnant incarcerated women. The Michigan Department of Corrections declined to share the department policy. The New Jersey Department of Corrections provided a statement via email, but it did not include the exact state statute or policy documentation.
Interrater agreement is excellent. Cohen’s kappa is 1.0 (p < .000), indicating 100% agreement between the raters (McHugh, 2012). This degree of agreement is likely attributable to the nature of each item. Specifically, each item assesses whether or not a law or policy permits or prohibits an action at a specific time; raters were not required to make subjective determinations.
Types of shackles
A few patterns regarding the types of restraints required or permitted by law or policy were identified in the data. Thirty-eight states (76%) were found to allow the standard use of handcuffs on pregnant incarcerated women at some point in their pregnancies. Furthermore, it was found that 29 states (58%) allow the standard use of leg irons and 26 states (52%) allow the standard use of waist chains on pregnant incarcerated women at some point in their pregnancies. These data indicate that most states require or permit the standard use of some form of restraint on women who are pregnant while incarcerated during some stage in the pregnancy. Most states authorize the use of handcuffs while comparatively fewer states permit the use of leg irons and waist chains on pregnant women. A possible reason for handcuffs being the most common form of permissible shackling is that handcuffs may be considered the least restrictive and least harmful type of restraint to use on pregnant incarcerated women. Handcuffs may also be the most common form of shackling used with pregnant women, because they are the most common form of shackling used for all inmates, regardless of sex or condition.
Safety and flight risk
States are nearly universal in their provisions for the use of shackles on pregnant incarcerated women who are viewed as safety or flight concerns. Forty-eight states (96%), or all of the states for which information was available, allow the use of shackles if pregnant incarcerated women pose a physical threat to correctional staff, judges, medical staff, and public. In addition, all 48 states (96%) for which information was available allow the use of shackles if pregnant incarcerated women represent a flight risk. The results from these two items were expected, because all departments of corrections have standard operating procedures that permit the shackling of incarcerated people if they are considered safety or flight risks. There are standard criteria that are used by departments of corrections to determine whether an incarcerated person constitutes a safety or flight risk. These criteria include determining whether an incarcerated person is likely to assault correctional or medical staff, assault a member of the public, execute self-injurious behavior, engage in behavior that may injure a fetus, cause damage to property, or attempt escape. In the case of pregnant incarcerated women, 38 states specify that the threat to safety or flight must be imminent. However, the language in a majority of laws and policies is vague (e.g., “An inmate is likely to . . .”), which allows maximum discretion.
Shackling and stages of pregnancy
Thirty-nine states (78%) were found to allow the use of shackles on pregnant incarcerated women during the first trimester, 38 states (76%) allow the use of shackles on pregnant incarcerated women during the second trimester, and 34 states (68%) were found to allow the use of shackles on pregnant incarcerated women during the third trimester. A pattern emerged from these data. A pregnant incarcerated woman is less likely to be shackled the closer she is to giving birth. In other words, a pregnant incarcerated woman is most likely to be shackled during her first trimester and least likely to be shackled during her third trimester.
Nine states (18%) allow the use of restraints on pregnant incarcerated women during labor, during medical emergencies, and during deliveries, and 28 states (56%) allow the use of restraints on incarcerated women during postbirth recovery. Finally, 20 states (40%) require reports to be completed when restraints are used on pregnant incarcerated women at any point during gestation, labor, delivery, or recovery. There are a few patterns that emerge from the data collected on the use of restraints during and immediately after childbirth. Only nine states allow the use of shackles on pregnant incarcerated women during labor, medical emergencies, and delivery. Legislators and correctional administrators may recognize the importance of not shackling pregnant women during these stages in pregnancies, and laws and policies are more likely to adhere to the gender-specific orientation during the birthing process. More states allow the use of shackles on incarcerated women during recoveries after childbirth. The three most obvious explanations for this phenomenon are the change in medical status, political palatability or viability, and oversight in the law and policy development process. The first possible explanation is that once an incarcerated woman has given birth, her ability to harm others or attempt escape may seem to increase, because her immediate medical condition (i.e., pregnancy) has ended. The second possible explanation is that it is more palatable or viable from a political perspective to argue that an incarcerated woman who is in labor, experiencing a medical emergency, or delivering a baby ought not be restrained than it is to argue that an incarcerated woman who happens to be pregnant or who recently gave birth ought not be restrained, given the ideological and social views of incarcerated people that are espoused by many politicians and their constituents. The third possible explanation is that when the shackling laws or policies were developed, the shackling of incarcerated women during postbirth recoveries may have been left inadvertently unaddressed. The last pattern is that less than half of the states require reports to be completed when restraints are used on pregnant incarcerated women. Results indicate that the more stages of pregnancy that are addressed in shackling laws or policies, the more likely the laws or policies are to include a requirement for reports to be completed when restraints are used. This pattern suggests these states may be more focused on the discrete use of restraints and require reports as a part of an accountability process.
Total item scores
The scores from all 13 items were added to produce the total number of points for each state (Figure 1). Results demonstrate that nine states (18%) received 0 points from the items, meaning there are no restrictions on the use of restraints on pregnant incarcerated women. Five states (10%) received 11 points from the items, indicating that the use of restraints on pregnant incarcerated women is subject to significant restrictions and monitored. All other states earned 1 to 10 points. The distribution includes five states (10%) that received 3 points, nine states (18%) that received 4 points, seven states (14%) that received 5 points, two states (4%) that received 6 points, four states (8%) that received 7 points, three states (6%) that received 8 points, three states (6%) that received 9 points, and one state (2%) that received 10 points from the items. Finally, none of the states received all 13 points, because all states for which laws or policies were available provide that pregnant incarcerated women may be shackled if they pose a safety concern or flight risk.
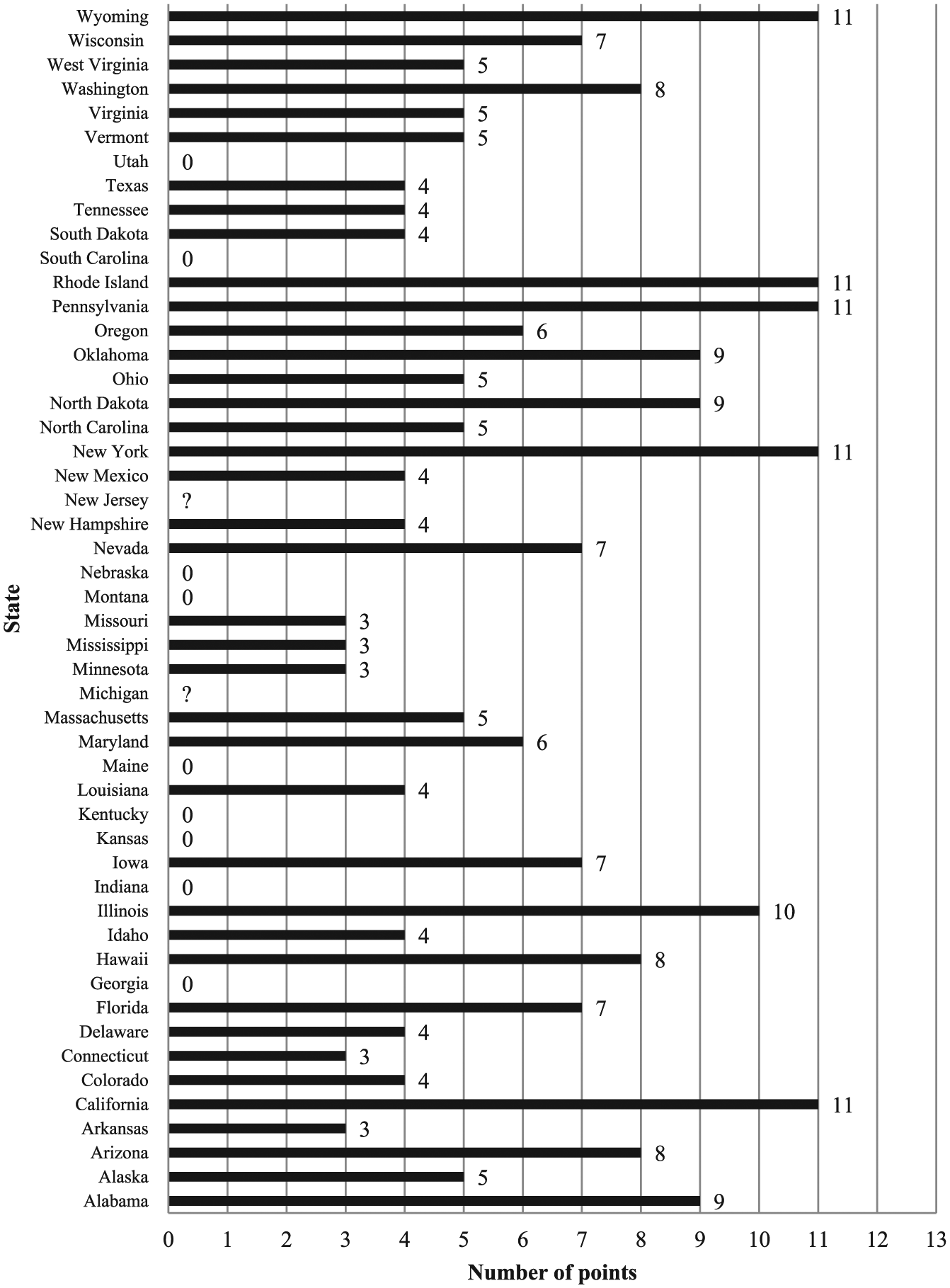
Total nominal item points for each state (n = 50).
Research Question 2
Cluster analysis was used to create a typology to determine where the state-level shackling laws or policies fell on a continuum from an entirely female indifferent to an entirely gender-specific orientation. The analysis revealed three clusters or categories of laws and policies in the dataset. The three categories include states that entirely adhere to the female indifferent orientation (0 points), states that adhere to a combination of female indifferent and gender-specific orientations (1-10 points), and states that almost entirely adhere to the gender-specific orientation (11-12 points). A state that entirely adheres to the female indifferent orientation is a state that does not have a law or policy in place that addresses the shackling of pregnant incarcerated women or does not place any restrictions on the use of restraints. A state is classified as adhering to a combination of the female indifferent and gender-specific orientations if the law or policy in place permits the shackling of pregnant incarcerated women at many points throughout the pregnancy. For example, a law or policy that allows shackling during the first, second, and third trimesters, prohibits shackling during labor and delivery, and allows shackling during recovery would be classified as adhering to a combination of female indifferent and gender-specific orientations. A state is classified as adhering to an almost entirely gender-specific orientation if the law or policy permits shackling of a pregnant incarcerated woman only if she is a safety or flight risk.
The distribution of state-level law and policy orientation is displayed in Table 1. None of the states for which data were available adopt an entirely gender-specific position that prohibits the use of restraints under all circumstances. Rather, these findings reflect the fail-safe position to permit correctional staff members to restrain a pregnant incarcerated woman if she is determined to be a safety or a flight risk, often based on vague criteria.
States’ Adherence to the Female Indifferent and Gender-Specific Orientations (n = 50).

The laws or policies for nine states (18%) were classified as entirely adhering to the female indifferent orientation. Thirty-four states (68%) have laws or policies in effect that prohibit the use of restraints during some of the stages of pregnancy or birthing process. These states are classified as adhering to a combination of the female indifferent and gender-specific orientations. Five states (10%) have laws or policies that restrict the use of shackles throughout the pregnancy and the birthing process. These states are classified as almost entirely adhering to the gender-specific orientation. In other words, these are the states that will only permit the use of restraints on a pregnant incarcerated woman if she is a safety or escape risk. The laws or policies for two states, Michigan and New Jersey (4%), were classified as unknown.
Combination states
A second cluster analysis was performed on the states that were classified as adhering to a combination of female indifferent and gender-specific orientations (n = 34). The cluster analysis was performed, because there was considerable variation in these state laws and policies. This cluster analysis was conducted to determine whether the states that adhere to a combination of female indifferent and gender-specific orientations adhere more to either the female indifferent or the gender-specific orientation. The analysis concluded that the laws and policies of these states fall into one of four clusters.
These four clusters represent states that adhere more to a female indifferent than a gender-specific orientation (1-3 points), states that adhere slightly more to a female indifferent than a gender-specific orientation (4-5 points), states that adhere slightly more to a gender-specific than a female indifferent orientation (6-7 points), and states that adhere more to a gender-specific than female indifferent orientation (8-10 points). A state with a law or policy that adheres more to a female indifferent than a gender-specific orientation is a state that permits the shackling of incarcerated women through a majority of the pregnancy. For example, a law or policy that allows shackling during the first, second, and third trimesters, prohibits shackling during labor and delivery, and allows shackling during recovery would be classified as adhering more to a female indifferent than a gender-specific orientation. A state is classified as adhering slightly more to a female indifferent than a gender-specific orientation if the law or policy in effect permits the shackling of incarcerated women at many points throughout the pregnancy. For example, a law or policy that allows the use of restraints during the first and second trimesters; prohibits shackling during the third trimester, labor, and delivery; and allows shackling during recovery would be classified as adhering slightly more to a female indifferent than a gender-specific orientation. A state is classified as adhering slightly more to a gender-specific orientation if the law or policy prohibits shackling of incarcerated women at many points throughout the pregnancy. For example, a law or policy that allows shackling during the first trimester; prohibits the use of restraints during the second and third trimesters, as well as labor and delivery; and allows shackling during recovery would be classified as adhering slightly more to a gender-specific orientation. Finally, a state will be classified as adhering more to a gender-specific orientation than a female indifferent orientation if the law or policy prohibits the shackling of incarcerated women through a majority of the pregnancy. For example, a law or policy that prohibits the use of restraints throughout the pregnancy, labor, and delivery, but allows shackling during recovery, would be classified as adhering more to a gender-specific orientation than a female indifferent orientation. The results from the second cluster analysis are displayed in Table 2. The data suggest that states with laws and policies reflecting a combination of female indifferent and gender-specific orientations are still more likely to adhere more to a female indifferent orientation when responding to a gender-specific condition.
States With Laws or Policies That Adhere to a Combination of Female Indifferent and Gender-Specific Orientations and the Level of Adherence to the Orientations (n = 34).

Percentages total more than 100% due to rounding.
Discussion
This research further educates readers on the issue of shackling pregnant incarcerated women through a national analysis, which highlights variation in laws and policies and demonstrates that most state-level laws and policies reflect a female indifferent orientation. The implications of this approach to shackling are discussed. Finally, areas for future research are presented.
Implications of the Results
The results demonstrate variation in current law and policy regarding the shackling of pregnant incarcerated women in the United States. In addition, there are a few patterns that emerge from the analyses. The first pattern is that it is more likely for a pregnant incarcerated woman to be shackled during her first trimester compared with her third trimester. State laws and department of corrections policies were written to allow the shackling of pregnant women during the first trimester to occur more frequently. It could be argued that during the first trimester, the pregnant incarcerated woman does not have the visible signs of pregnancy, and legislators and correctional administrators, as well as correctional staff who may be permitted to exercise discretion, could easily ignore any harm that shackling could pose to the inmate and her fetus. The second pattern is that handcuffs are the most common shackling method used on pregnant incarcerated women at some point during their pregnancies. This could be because handcuffs are considered the least restrictive restraint, are viewed as the type of restraint least likely to harm the incarcerated woman and her fetus, or are the most common restraint used with all incarcerated people.
A majority of states (n = 34) have laws or policies that adhere to a combination of female indifferent and gender-specific orientations and nine states do not have laws or policies that restrict the shackling of pregnant incarcerated women. Only five states almost entirely adhere to the gender-specific orientation, which means that very few states place extensive restrictions on the use of restraints with pregnant incarcerated women. This suggests that a majority of the laws or policies at the state level adopt a more female indifferent orientation; in most states, the use of restraints on a pregnant incarcerated woman is at the discretion of the correctional staff on duty with little guidance. In total, 43 states either have laws or policies that do not restrict the shackling of pregnant incarcerated women or adhere to a combination of female indifferent and gender-specific orientations. This means that 86% of the sample has laws or policies that are inconsistent with the policy positions of medical and advocacy organizations (e.g., AMA, ACOG, ACNM, APHA, ACLU) and the ACA.
The same conclusion was reached when the cluster analysis was completed on the laws and policies that adhere to a combination of female indifferent and gender-specific orientations; approximately 62% of the states in this subsample (21 of 34) adhere more to the female indifferent orientation. There are significant implications related to most state legislatures and correctional systems adopting a primarily female indifferent orientation with respect to the use of restraints. The growth of the female inmate population creates the potential for a higher incidence of pregnancy during incarceration. Pregnant incarcerated women have different medical and safety needs than incarcerated women who are not pregnant and incarcerated men. The incarcerated woman is carrying a fetus, so the institution in which she is confined is responsible for not only her safety but for that of her fetus. This further underscores the need to adequately respond to biological changes associated with pregnancy.
These results support the work of many scholars who argued that gender neutrality in law and policy does not always result in equitable treatment (Binion, 1993; Golden, 1991; Littleton, 1987; Rhode, 1990), particularly in situations wherein men and women are not similarly situated, such as pregnancy (Dworkin, 1981; Hatcher, 2003; McCorkel et al., 2001; Scales, 1986; West, 1988). Generally, shackling laws and policies have their foundations in the lives of men—people who cannot become pregnant—and do not effectively incorporate or account for women’s experiences. If states do not implement laws or policies that provide sufficient guidance on the use of restraints to correctional staff members so that they may adequately and reasonably respond to pregnant incarcerated women, then states are faced with the increased risk of an incident and the liability that comes with the failure to adequately address the medical and safety needs of the pregnant incarcerated women in their custody.
Model for Replication
The laws and accompanying policies guiding the shackling of pregnant incarcerated women in Pennsylvania earned a total of 11 points, the highest point total earned in this study (California, New York, Rhode Island, and Wyoming also earned 11 points). Collectively, these laws and policies almost entirely adhere to a gender-specific orientation and create a model that states should consider for adoption. In Pennsylvania, correctional staff are not permitted to use restraints of any type at any stage of pregnancy, the birthing process, postbirth recovery, or during medical emergencies unless the woman poses an imminent safety or flight risk (see County Recording System for Application of Restraints to Pregnant Prisoners or Detainees, 2010; Healthy Birth for Incarcerated Women, 2010; Hospital Posts, 2009; State Recording System for Application of Restraints to Pregnant Prisoners or Detainees, 2010; Transport of a Pregnant Inmate, 2004; Use of Restraints for Pregnant Inmates, 2004). Pennsylvania has a state recording system that requires all correctional staff members to file reports every time restraints are used on pregnant incarcerated women and the reports are reviewed by an external body (State Recording System for Application of Restraints to Pregnant Prisoners or Detainees, 2010). The individual reports of restraint use are compiled into annual reports that are sent to the Governor and then are made publicly available (Pennsylvania Department of Corrections, 2013, 2014). These laws and policies collectively create a model that is responsive to general medical recommendations regarding the safety of pregnant incarcerated women and fetuses, includes an external accountability process, and makes the reports available to the public as an additional layer of surveillance. For these reasons, states should consider replicating this robust model for regulating and monitoring the use of restraints on pregnant women who are incarcerated to avoid unnecessary risk of harm to the women in their custody and their fetuses, and the legal liability attached to failing to adequately address legitimate medical and safety issues.
Limitations
The primary limitation associated with the methods chosen for this study is related to interpretation. The results of the content analysis may not be objective, because a different researcher may have categorized and interpreted the data in a different way. However, the involvement of a second researcher, the evaluation of interrater reliability, and the use of a two-step cluster analysis with automatic cluster determination minimize potential researcher bias.
Conclusion
The issue of shackling pregnant incarcerated women is a timely topic, because women are the fastest growing population in the criminal justice system (Cardaci, 2013; Thomas, 2014). In addition, approximately 6% to 10% of women entering prisons each year are pregnant and there are approximately 2,000 births per year to incarcerated women (Quinn, 2014). Some of these women are filing lawsuits seeking remedy for shackling-related harms, and some are prevailing in court. The findings from this study provide data to advance recommendations for lawmakers and correctional administrators.
The content analysis provided evidence that there is variation among the states’ laws and policies regarding the shackling of incarcerated women. Patterns emerged from the data, and it was found that incarcerated women who are pregnant were most likely to be shackled during the first trimester and handcuffs are the most common method of shackling used on pregnant incarcerated women. This raises the question as to why these patterns exist. The typology demonstrates that a majority of states have laws or policies that demonstrate ignorance or indifference regarding gender differences in medical needs, fail to recognize the importance of providing additional or specific treatment for pregnant incarcerated women, and generally fail to follow the recommendations of medical and advocacy organizations, as well as the ACA, on these issues. This suggests that lawmakers and correctional administrators should invest more time in developing more nuanced laws and policies to account for medical issues and conditions. In addition, gender differences in medical needs and associated safety concerns should be taken into consideration. It is important for lawmakers and correctional administrators to adhere to a more gender-specific orientation when it comes to incarcerated women who are pregnant—a legitimate medical condition that carries with it unique needs and concerns. The issue of pregnant incarcerated women is arising more frequently in prisons, jails, and media outlets as the size of the female correctional population increases. Lawmakers and correctional administrators should be more mindful of this growing population in the criminal justice system when developing or altering laws and policies. In addition, correctional administrators should ensure that all correctional staff members are properly trained on how to appropriately respond to gender differences in medical needs and related safety concerns experienced by incarcerated women.
Future Research
There are several possible avenues of future research involving the shackling of incarcerated women. There are very limited data on pregnant incarcerated women, and more research needs to be conducted to shed light on the subject. The following is a discussion of five possible follow-up studies. The first study explores the underlying motives for the observed patterns, including research on the reasons states neglect or choose to not address the issue of shackling incarcerated women. A second study includes an examination of potential racial and ethnic stereotyping that may influence decisions to shackle incarcerated women who are pregnant. One way to examine this issue is to research lawsuits involving the shackling of incarcerated women to determine whether the plaintiff is more likely to be a woman of color than White. A third possible study could examine whether or not local jurisdictions (i.e., jails) are implementing policies that align with state laws. A fourth possible study examines cases in which correctional officers did not follow laws or policies in states that restrict the use of shackles on pregnant incarcerated women to understand the reasons for noncompliance to increase the likelihood of compliance with restrictive laws and policies. A fifth possible study includes an examination of the relationship between state-level political climate and whether laws and policies reflect a female indifferent or gender-specific orientation with respect to shackling pregnant incarcerated women. These five studies would provide the opportunity to further investigate issues related to the shackling of pregnant incarcerated women and provide additional information to legislators and correctional administrators to facilitate informed law and policy development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.