
Abstract
Cataracts are the leading cause of blindness worldwide. Obesity, a key component of metabolic syndrome (MetS), may represent a modifiable risk factor for cataracts. However, the evidence regarding the association between MetS or its components and cataracts remains controversial. Therefore, our meta-analysis aims to clarify the relationship between MetS or its components and cataracts. A search was conducted until February 2024 via the MEDLINE, EMBASE, and Cochrane databases. The primary endpoint included the association between MetS or its components, including body mass index (BMI), diabetes mellitus (DM), hypertension (HT), and dyslipidemia (DLP), and cataracts. Secondary endpoints included the association between levels of blood pressure, blood sugar, and lipid profiles and cataracts. A total of 27 studies were included with a total of 1,010,014 patients (134,498 with cataracts and 875,516 without cataracts). Of these, there were 2 prospective cohort studies, 6 case–control studies, and 19 cross-sectional studies. The prevalence of cataracts was 13.3%. MetS was significantly associated with cataracts with an odds ratio (OR) of 1.60 (95% confidence interval [CI]: 1.44–1.77, I2 = 93%). Among MetS components, high BMI and being diagnosed with DM, HT, and DLP were associated with cataracts with ORs of 1.45 (95% CI: 1.33–1.58, I2 = 80%), 1.77 (95% CI: 1.69–1.85, I2 = 51%), 1.23 (95% CI: 1.19–1.28, I2 = 62%), and 1.38 (95% CI: 1.30–1.46, I2 = 0%). Among the metabolic parameters, high total cholesterol, high triglycerides, low high-density lipoprotein cholesterol, and high low-density lipoprotein cholesterol were associated with cataracts with ORs of 1.25 (95% CI: 1.04–1.49, I2 = 48%), 1.05 (95% CI: 1.04–1.06, I2 = 68%), 1.07 (95% CI: 1.01–1.13, I2 = 0%), and 1.30 (95% CI: 1.10–1.53, I2 = 71%), respectively. MetS, obesity, DM, HT, and DLP are associated with cataracts. Prevention or treatment of MetS or its components likely represent a modifiable risk factor in cataract development.
Keywords
Introduction
In the past three decades, the prevalence of blindness has increased by up to 50%. 1 The number of people with moderate-to-severe visual impairment is estimated to reach 474 million by 2050. Of these, 61 million people are expected to be blind. 1 Cataracts are the most common cause of blindness worldwide, and several risk factors contribute to cataract formation. 2 Among these, nonmodifiable risks include, but are not limited to, older age, female sex, genetics, and concurrent ocular diseases. 2 However, other factors related to cataracts are modifiable, such as ultraviolet exposure, 3 excessive alcohol consumption, 4 smoking, 5 and certain metabolic diseases, including diabetes mellitus (DM), hypertension (HT), and obesity. 6
Metabolic syndrome (MetS) is highly prevalent globally and is expected to increase up to 53% by 2035. 7 MetS is a constellation of abdominal obesity, DM, HT, and dyslipidemia (DLP).8,9 Obesity may be one of the modifiable risk factors for cataracts. According to a meta-analysis in 2014, 10 obesity is associated with all types of cataracts, including nuclear, cortical, and posterior subcapsular (PSC) cataracts. However, later Mendelian randomization studies have shown no association between obesity and cataracts.11,12 Furthermore, evidence gaps exist regarding the association between other components of MetS and cataracts. Therefore, we performed a meta-analysis to determine the association between MetS or its components and cataracts.
Methods
Our meta-analysis was registered with PROSPERO (CRD Number 420251001712). All processes were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Search strategy
A systematic search was conducted for studies published up to February 2024 via MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews, along with manual searching of the references. The search objective was to identify the association between MetS or its components and cataracts. Two authors (P.T. and S.P.) searched independently, and discrepancies were reviewed by the third author (P.P.) until reaching consensus. Search terms included “metabolic syndrome,” “cataracts,” “obesity,” “body mass index,” “waist circumference,” “diabetes mellitus,” “hypertension,” “hyperlipidemia,” and “dyslipidemia,” as shown in Supplementary Table S1.
Selection criteria
We included studies reporting a head-to-head comparison regarding cataracts between patients who had MetS or its components and those without. MetS components included body mass index (BMI), waist circumference (WC), DM, HT, and DLP. We also included studies comparing different levels of blood pressure (BP), both systolic BP (SBP) and diastolic BP (DBP), and metabolic parameters, including total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and fasting blood sugar (FBS). Eligible study designs included randomized controlled trials, cohort, case–control, and cross-sectional studies. There were no limitations regarding language or settings.
Quality assessment
We used multiple assessment criteria based on study designs. For cohort and case–control studies, quality was assessed using the Newcastle–Ottawa scale (NOS). 13 Meanwhile, cross-sectional studies were assessed using the modified NOS.
Statistical analyses
The primary analysis included the odds ratio (OR) between MetS or its components and the presence of any cataract in at least one eye. Secondary analyses were performed by stratifying continuous data into high and low groups, categorized by the cutoff value used in each study. Since there was heterogeneity in the cutoff values, further analysis was conducted to select only studies that used the same cutoff values, including BMI at 25 kg/m2, SBP at 140 mm Hg, DBP at 90 mm Hg, TC at 200 mg/dL, and TG at 150 mg/dL.
Weighted treatment estimates and 95% confidence intervals (95% CIs) were computed using arcsine transformation. Cochrane Q test and I2 statistics were used to define statistical heterogeneity, using cutoff values of 50% and 75% for considerable and substantial heterogeneity, respectively. Publication bias was assessed by visualizing the symmetry of funnel plots. All analyses were performed using the “meta” package in R software version 4.4.3 (Vienna, Austria).
Results
Study selection and characteristics
A total of 18,130 studies were identified from our search strategy. After removing duplicates, 17,287 studies remained for screening. Another 17,216 studies were excluded after abstract screening, leaving 71 studies that underwent full-text review. Finally, 27 studies were included in the data collection and analysis. The selection process is summarized in the PRISMA flow diagram (Fig. 1).

The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Of the final 27 studies,14–40 2 were prospective cohort studies, 6 were case–control studies, and 19 were cross-sectional studies. A total of 1,010,014 patients were included, comprising 134,498 patients with cataracts and 875,516 patients without cataracts. The prevalence of cataracts was 13.3%. The baseline characteristics and quality assessment of all studies are presented in Table 1.
Baseline Characteristics of the Studies Included in the Meta-Analysis
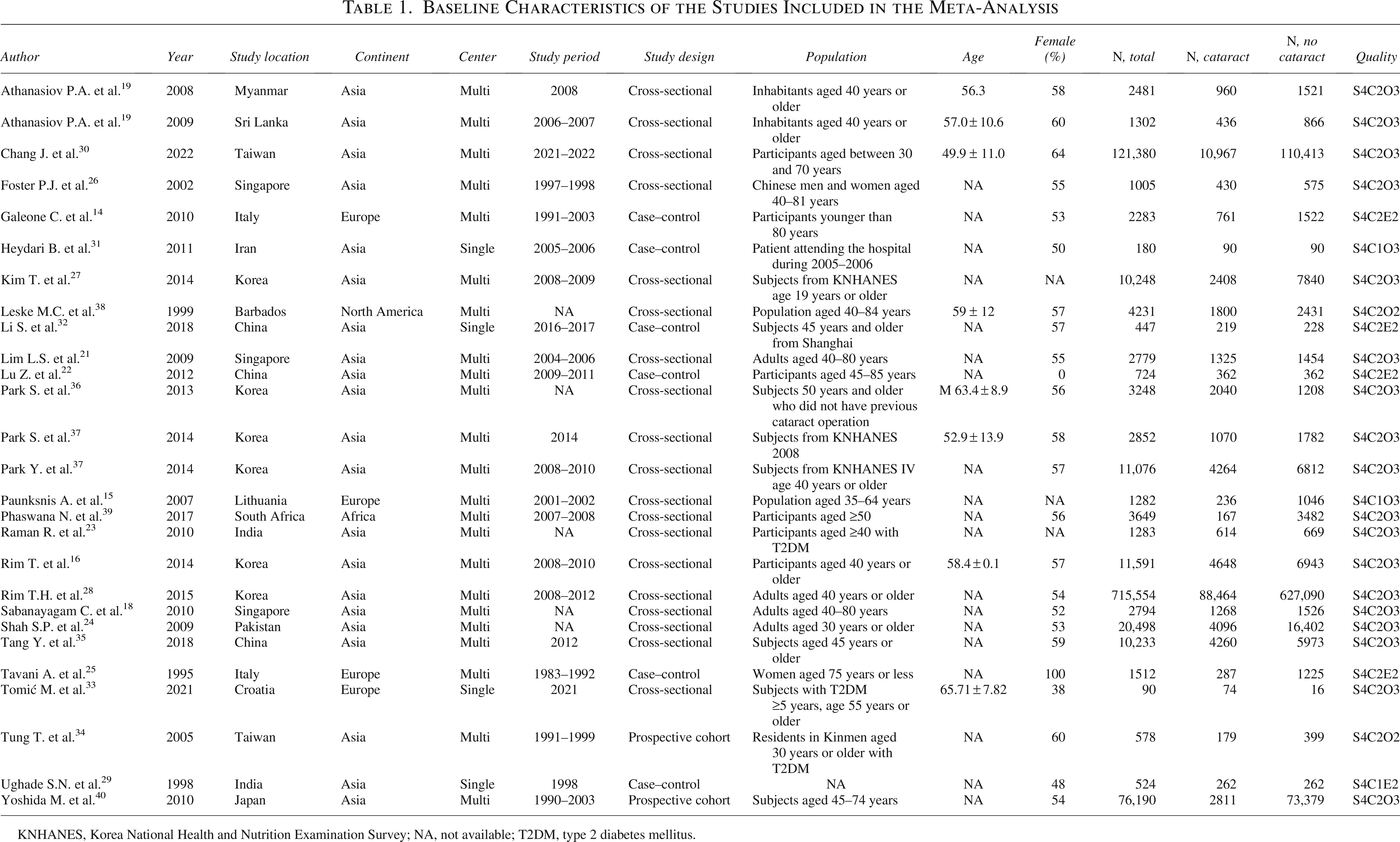
KNHANES, Korea National Health and Nutrition Examination Survey; NA, not available; T2DM, type 2 diabetes mellitus.
MetS and cataracts
A total of five studies14–18 evaluated data on MetS and cataracts. MetS is significantly associated with cataracts, with an OR of 1.60 (95% CI: 1.44–1.77, I2 = 93%). Among the components of MetS, pooled results from nine studies18–26 showed that high BMI was associated with cataracts, with an OR of 1.45 (95% CI: 1.33–1.58, I2 = 80%). Pooled results from two studies36,40 reported that BMI >25 kg/m2 was associated with cataracts, with an OR of 1.23 (95% CI: 1.10–1.37, I2 = 0%). Pooled results from eight studies14,16,18,25–29 showed that DM was associated with cataracts, with an OR of 1.77 (95% CI: 1.69–1.85, I2 = 51%). Pooled results from 10 studies14,16,18,23–29 showed that HT was associated with cataracts, with an OR of 1.23 (95% CI: 1.19–1.28, I2 = 62%). Pooled results from three studies14,25,28 showed that DLP was associated with cataracts, with an OR of 1.38 (95% CI: 1.30–1.46, I2 = 0%). However, pooled results from three studies14,30,39 showed no association between WC and cataracts with an OR of 1.03 (95% CI: 0.98–1.09, I2 = 75%). All analyses on MetS or its components and cataracts are shown in Table 2.
Association Between Metabolic Syndrome or Its Components and Cataracts
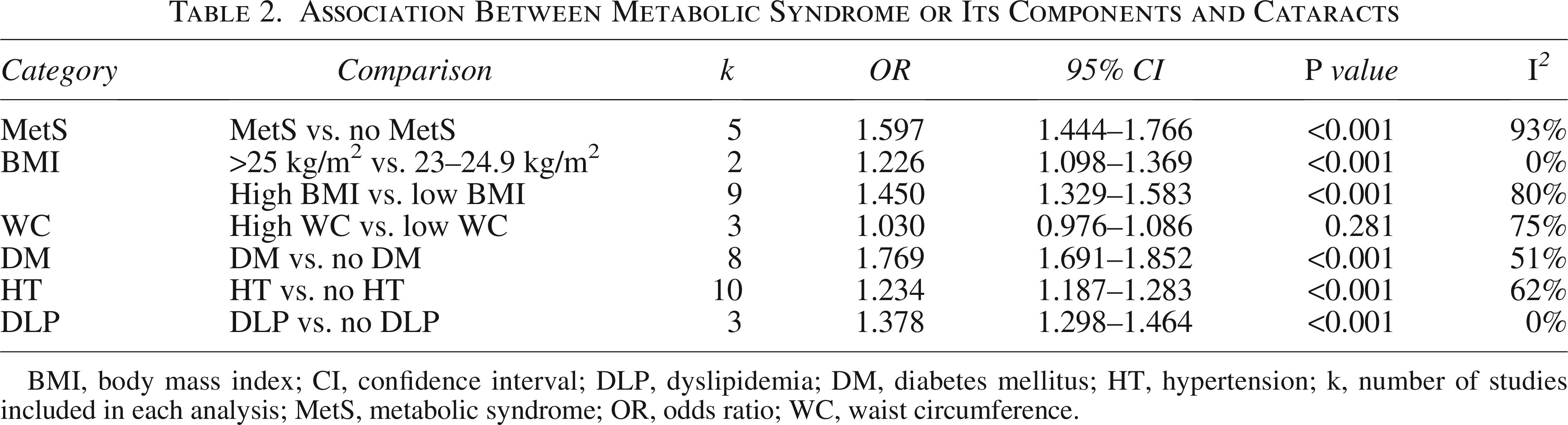
BMI, body mass index; CI, confidence interval; DLP, dyslipidemia; DM, diabetes mellitus; HT, hypertension; k, number of studies included in each analysis; MetS, metabolic syndrome; OR, odds ratio; WC, waist circumference.
BP and cataracts
A total of four studies15,18,30,37 evaluated data on BP level and cataracts. High BP was associated with cataracts with an OR of 1.06 (95% CI: 1.00–1.12, I2 = 72%). Among BP components, pooled results from four studies18,34,35,38 showed that high SBP was associated with cataracts with an OR of 1.35 (95% CI: 1.23–1.49, I2 = 59%), of which two studies34,35 showed that SBP >140 mm Hg was associated with cataracts with an OR of 1.34 (95% CI: 1.20–1.49, I2 = 0%). Pooled results from five studies18,33–35,38 showed that high DBP was associated with cataracts with an OR of 1.08 (95% CI: 1.01–1.14, I2 = 52%), while pooled results from two studies34,35 showed that DBP >90 mm Hg was not associated with cataracts with an OR of 1.19 (95% CI: 0.96–1.49, I2 = 84%). All analyses on BP and cataracts are presented in Table 3.
Association Between Blood Pressure and Cataracts

BP, blood pressure; CI, confidence interval; DBP, diastolic blood pressure; k, number of studies included in each analysis; OR, odds ratio; SBP, systolic blood pressure.
Metabolic parameters and cataracts
A total of 10 studies15,16,18,23,30–35 evaluated data on metabolic parameters and cataracts. Among lipid profiles, pooled results from four studies16,31,33,34 showed that high TC was associated with cataracts with an OR of 1.25 (95% CI: 1.04–1.49, I2 = 48%), of which two studies31,34 showed no association between TC >200 mg/dL and cataracts with an OR of 1.36 (95% CI: 0.88–2.08, I2 = 80%). Pooled results from eight studies15,18,23,30–34 showed that high TG was associated with cataracts with an OR of 1.05 (95% CI: 1.04–1.06, I2 = 68%), of which five studies15,18,30–32 showed no association between TG >150 mg/dL and cataracts with an OR of 1.05 (95% CI: 1.04–1.06, I2 = 78%). Pooled results from five studies15,18,30,31,35 showed that low HDL-C was associated with cataracts with an OR of 1.07 (95% CI: 1.01–1.13, I2 = 0%). Pooled results from five studies23,31–33,35 showed that high LDL-C was associated with cataracts with an OR of 1.30 (95% CI: 1.10–1.53, I2 = 71%). Among glycemic profiles, pooled results from four studies15,30,31,34 showed that high FBS was associated with cataracts with an OR of 1.16 (95% CI: 1.10–1.23, I2 = 77%). All analyses on metabolic parameters and cataracts are shown in Table 4.
Association Between Metabolic Parameters and Cataracts
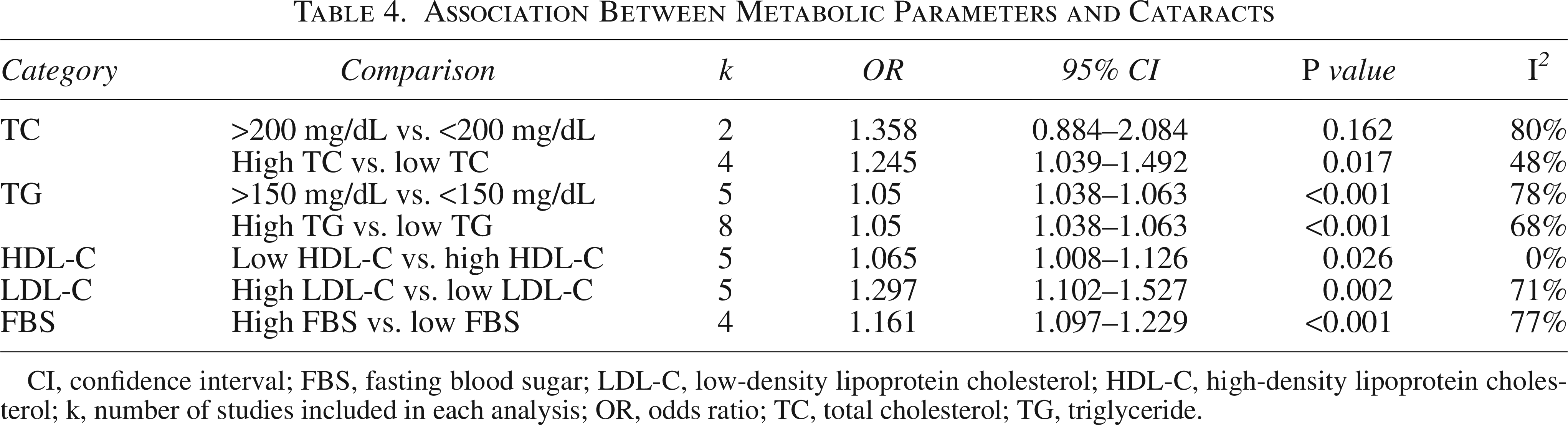
CI, confidence interval; FBS, fasting blood sugar; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; k, number of studies included in each analysis; OR, odds ratio; TC, total cholesterol; TG, triglyceride.
Publication bias
Since all funnel plots were symmetrical, no publication bias was detected for any outcome. The forest and funnel plots are presented in Supplementary Figs. S1 and Figs. S2, respectively.
Discussion
Our meta-analysis highlights MetS as a significant risk factor for cataract development. Among its individual components, HT, elevated TG levels, low HDL levels, and high FBS levels were all associated with cataract risk. However, increased WC did not show a statistically significant association. A long-standing question in research has been whether MetS contributes to cataract risk beyond the sum of its individual components. 41 While this notion has gained increasing acceptance, our study further supports the idea that MetS itself is an independent risk factor for cataract.
Although obesity and higher BMI are not formally included in the diagnostic criteria for MetS, they have been linked to various ophthalmological conditions, including age-related macular degeneration, diabetic retinopathy, and cataract. 42 A previous study demonstrated a dose–response relationship between BMI and cataract risk. 43 Our findings, which show that BMI >25 kg/m2 is associated with an increased risk of cataracts, further reinforce this relationship. However, conflicting evidence exists, as some studies suggest that while high BMI is a risk factor for cataract onset, it may not necessarily contribute to cataract progression. 44
While DM is a well-established risk factor for cataracts, emerging evidence suggests that insulin resistance itself may contribute to various ophthalmological conditions, even in nondiabetic individuals. 44 Insulin resistance is a hallmark of MetS, which can alter lens metabolism by activating the sorbitol pathway, leading to the accumulation of advanced glycation end products.45,46 Our findings, which show an association between elevated FBS levels and cataract risk, further support the role of glucose dysregulation and insulin resistance in lens opacification. While the presence of diabetes increases cataract risk, these findings suggest that even prediabetic states associated with MetS may elevate cataract risk.
Dyslipidemia has been linked to cataract development, with low HDL and high LDL levels contributing to oxidative stress and lipid peroxidation in the lens. While previous studies suggested a role for high TC, low HDL, and high LDL in various ocular diseases, including cataracts,33,47 our findings indicate that low HDL and high LDL, rather than TC, are more strongly associated with cataract risk. Given that low HDL and high TGs are key components of MetS, our results further support a connection between lipid imbalance and cataract formation.
We also observed an association between high SBP and cataract risk. While routine preoperative testing is often unnecessary in low-risk surgeries such as cataract extraction, 48 the presence of HT may warrant closer evaluation due to its association with increased surgical risk. 49 In addition, unnecessary preoperative investigations can contribute to higher health care costs without a clear clinical benefit. 50 Further studies are needed to assess the impact of HT on cataract surgery outcomes.
Most cataracts develop as a result of aging, primarily due to oxidative stress and metabolic dysfunction, which compromise the structural integrity of the lens. MetS is characterized by adipocyte tissue dysfunction and insulin resistance, conditions closely linked to chronic inflammation and oxidative stress. These processes involve the NLRP3 inflammasome, which plays a key role in inflammatory responses within adipose tissue.51,52 Elevated levels of inflammatory markers such as C-reactive protein, interleukin-1, interleukin-6, and plasminogen activator inhibitor-1 have been reported in individuals with MetS, 53 further supporting the role of systemic inflammation in cataract development. While the precise mechanisms linking MetS to cataract formation remain unclear, chronic low-grade inflammation and oxidative stress likely contribute to the pathophysiology.
Our study has a few limitations. Most of the included studies are cross-sectional or case–control, with only a limited number of prospective cohort studies, which may impact the ability to establish causality. In addition, most studies did not indicate whether cataract in each eye was counted separately for each patient, which may affect the comparability across studies and the reliability of our findings. Furthermore, our choice of cutoff for obesity with a BMI of 25 or greater may limit generalizability to more developed countries. The choice of BMI cutoff was limited partly due to the inconsistent BMI cutoffs and stratification used across the included studies. Similarly, when assessing the risk of cataract in diabetes, diabetes severity, duration, and presence of diabetes-related complications were not considered in our analysis, as few studies reported these parameters. In addition, high heterogeneity was observed across studies. This variability likely arises from differences in study designs, patient populations, methodologies, and diagnostic criteria, which could influence the consistency and generalizability of our findings. To mitigate this, we performed meta-regression analyses, allowing us to explore potential sources of heterogeneity and improve the robustness of our findings. However, this variability is expected given the large number of studies included, making this one of the largest and most current meta-analyses to date. Future well-designed, large-scale prospective studies are needed to further elucidate the underlying mechanisms and associations.
Given the significant impact of cataracts on quality of life and health care costs, our findings suggest that effective management and prevention of MetS may help reduce cataract burden at a population level. Patients with MetS may require more extensive preoperative evaluations, potentially increasing costs and affecting surgical outcomes. This underscores the need for proactive strategies to address MetS as part of comprehensive eye health and cataract management.
Authors’ Contributions
All the authors had access to the data and a role in writing the article.
Footnotes
Author Disclosure Statement
The authors do not have any potential financial or nonfinancial conflicts of interest.
Funding Information
No funding was received for this article.
Acknowledgement
We gratefully acknowledge TERMAURA HEALTH AND WELLNESS CO., LTD., a healthcare provider company from Thailand, for their extensive and expert support during the development and implementation of this research, which substantially strengthened the rigor, progress, and successful completion of the study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.