
Abstract
Background:
Idiopathic intracranial hypertension (IIH) is commonly linked to obesity. Glucagon-like peptide-1 receptor agonists (GLP-1RAs) and bariatric surgery may improve outcomes beyond conventional therapy, but comparative evidence is limited.
Methods:
We systematically searched MEDLINE, EMBASE, and Cochrane from inception until June 2025. Eligible randomized and observational studies compared GLP-1RAs or bariatric surgery (each plus conventional care) against conventional management. Primary outcomes were the change in papilledema, visual acuity, and visual field. Secondary outcomes included body mass index (BMI), retinal nerve fiber layer (RNFL) thickness, monthly headache days, and risks of papilledema, visual disturbance, and headache. Pairwise random-effects meta-analyses and frequentist network meta-analysis (P-scores) were performed.
Results:
Out of 429 records, 8 studies were included. Versus conventional therapy, GLP-1RAs reduced BMI (mean difference −1.55 kg/m2; 95% confidence interval [CI]: −2.13 to −0.97) and lowered risks of papilledema (relative risk [RR]: 0.47; 95% CI: 0.34–0.65), visual disturbance (RR: 0.48; 95% CI: 0.24–0.98), and headache (RR: 0.78; 95% CI: 0.69–0.88). Changes in papilledema severity and RNFL thickness were not different; visual acuity favored GLP-1RAs at the end of follow-up, whereas visual field values were worse at some time points. In indirect comparisons with bariatric surgery, no significant differences were detected across outcomes.
Conclusions:
Adjunctive GLP-1RA therapy may be associated with weight loss and improved clinical/ophthalmic outcomes in IIH relative to conventional care, with a signal for worse visual fields at certain time points. Indirect comparisons suggest comparable efficacy to bariatric surgery. High-quality randomized trials are needed to define comparative effectiveness, safety, and optimal use.
Keywords
Introduction
Idiopathic intracranial hypertension (IIH), or pseudotumor cerebri, is defined by elevated intracranial pressure (ICP) in the absence of abnormal cerebrospinal fluid (CSF) composition, hydrocephalus or structural lesion, or another clear etiology. 1 It most commonly affects women of reproductive age with obesity.2,3 Clinical manifestations span from asymptomatic or mild headache with visual disturbances (e.g., transient visual obscurations, mild visual loss, tinnitus) to disabling chronic headache and, in some cases, permanent visual loss.4–6
Although IIH is relatively uncommon, its incidence has risen over recent decades. United States data indicate a 1.35-fold increase in prevalence (from 11.3 per 100,000 women in 2015 to 15.4 per 100,000 in 20223,7–9) likely paralleling the increase in obesity.10,11 The pathophysiology remains incompletely understood; however, obesity is considered a major contributor. 12 Accordingly, weight reduction is central to management, achievable through lifestyle intervention, bariatric surgery, or glucagon-like peptide-1 receptor agonists (GLP-1RAs). 13
Beyond promoting weight loss, GLP-1RAs have been shown to lower ICP in IIH even without substantial weight change, 14 potentially via direct CSF modulation, 12 suggesting both weight-dependent and weight-independent therapeutic effects. Bariatric surgery, particularly Roux-en-Y gastric bypass, also increases circulating GLP-1 levels. 15 Prior evaluations of IIH therapies have largely emphasized visual and ophthalmological outcomes (e.g., papilledema, visual fields) and headache within conventional treatment frameworks. 16 However, comparative evidence directly relating GLP-1RAs and bariatric surgery to conventional approaches remains limited.
Therefore, we conducted a network meta-analysis to compare GLP-1RAs and bariatric surgery with conventional therapies in IIH, focusing on visual outcomes and headache.
Methods
Data sources and search strategy
We systematically searched MEDLINE, EMBASE, and the Cochrane Library from inception to June 2025 with no language restrictions. Harmonized strategies were adapted to each database’s indexing (Supplementary Table S1). The protocol was prospectively registered in PROSPERO (CRD420251108771).
Eligibility criteria
We included randomized controlled trials, cohort studies, case–control studies, and cross-sectional studies evaluating either bariatric surgery or GLP-1RAs in combination with conventional therapy compared against conventional management (e.g., weight management strategies; medications such as acetazolamide, topiramate, or diuretics). Studies were required to report at least one prespecified clinical or ophthalmological outcome relevant to IIH.
Study selection and data extraction
Two reviewers (S.P. and N.S.) independently screened titles, abstracts, and full texts and extracted data using a piloted, structured form capturing study characteristics, diagnostic criteria, interventions, comparators, follow-up, and outcomes. Disagreements were resolved by consensus with a third reviewer (P.P.).
Outcomes
Primary outcomes were change from baseline to follow-up in ophthalmological measures: papilledema (Frisén scale), visual acuity (logMAR), and visual field (perimetric mean deviation, dB). Secondary outcomes were between-group differences at each time point for the above measures and additional endpoints: body mass index (BMI, kg/m2), retinal nerve fiber layer (RNFL) thickness (optical coherence tomography, µm), monthly headache days, risk of headache, risk of visual disturbance, and risk of papilledema. Visual disturbance was defined as symptoms of visual discomfort/defects or International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) H53 (visual disturbances) or H54 (blindness and low vision).
Risk-of-bias assessment
Risk of bias for cohort and case–control studies was assessed using the Newcastle–Ottawa Scale (Supplementary Fig. S1).
Statistical analysis
Analyses were conducted in R (v4.4.0) using meta (v8.1-0) for pairwise meta-analyses and netmeta (v3.2-0) for network meta-analysis. Adjusted study estimates were synthesized with the generic inverse-variance method (DerSimonian-Laird). Random-effects models were used; between-study heterogeneity was estimated with Paule–Mandel for binary outcomes and restricted maximum likelihood for continuous outcomes. Effect measures were relative risks (RRs) for dichotomous outcomes and mean differences (MDs) for continuous outcomes, each reported with 95% confidence intervals (CIs).
Depending on data availability, we (1) compared the change from baseline to each follow-up between interventions; (2) compared observed values at each follow-up between interventions; and (3) performed a frequentist network meta-analysis to indirectly compare GLP-1RAs with bariatric surgery. End-of-study outcomes were also pooled across studies to enable cross-study comparisons. Treatment ranking in the network meta-analysis was summarized using P-scores.
When change scores were not reported, we imputed pre–post differences following the Cochrane Handbook guidance. 17 If the correlation between pre- and post-treatment measures could not be derived, we assumed zero correlation and conducted sensitivity analyses varying the correlation coefficients (0.3, 0.5, 0.7) irrespective of imputation feasibility.
Small-study effects/publication bias were assessed by funnel-plot inspection and Egger’s test. Heterogeneity was interpreted as follows: I2 0–25% (insignificant), 26–50% (low), 51–75% (moderate), and >75% (high).
Results
Study selection
Across databases, 429 records were identified after deduplication. Titles and abstracts screening excluded 315 studies due to a lack of comparison between interventions or a lack of intervention of interest. 114 studies remained for full-text screening, 108 of which were excluded for not reporting outcomes of interest or for being duplicate reports. Eight studies were ultimately included in the quantitative synthesis18–25 (Fig. 1). An overview of the main findings is provided in Figure 2.
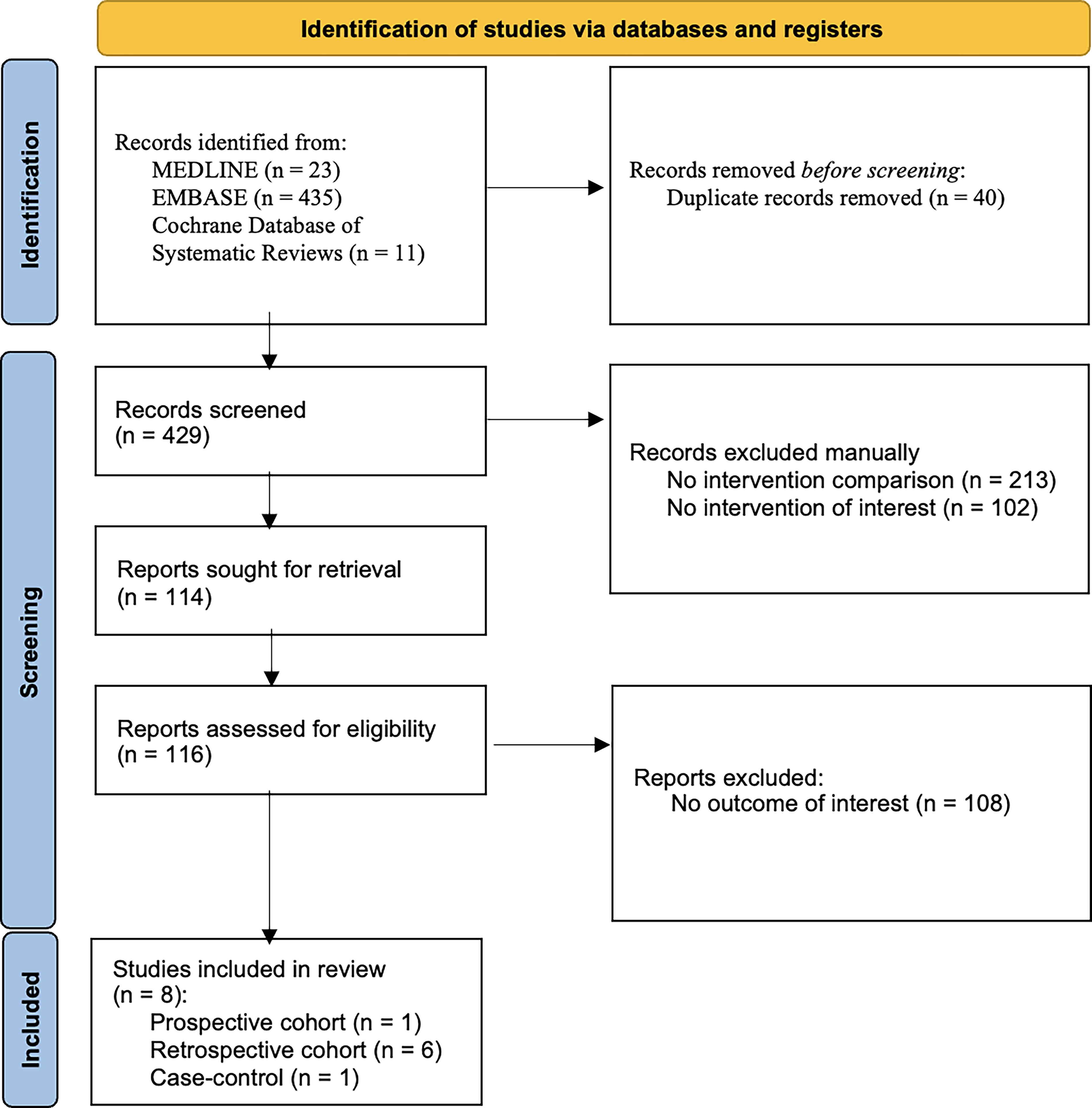
PRISMA 2020 flow diagram.
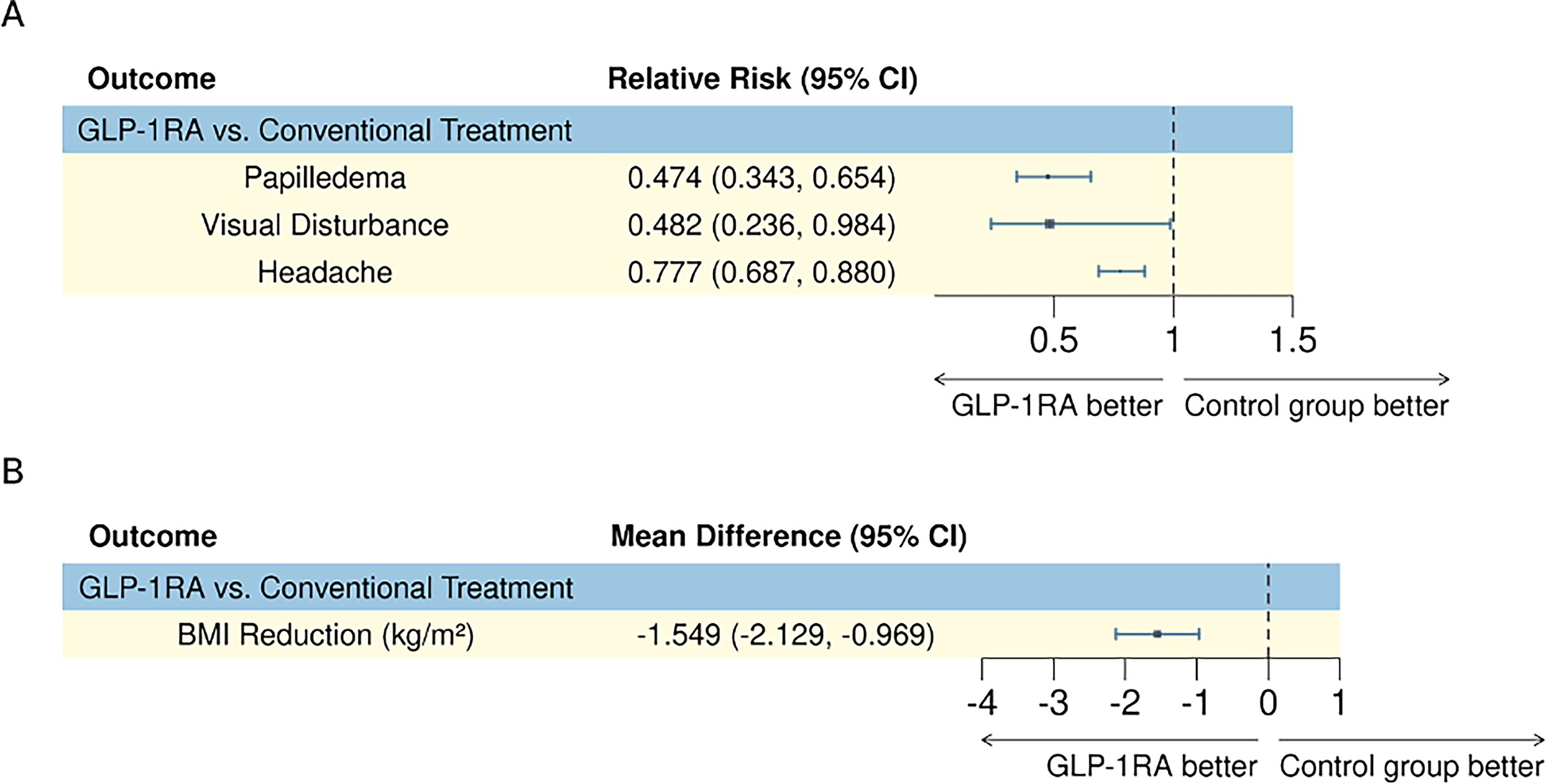
Summary forest plots for significant differences in treatment efficacy of GLP-1RAs compared to conventional management. Forest plots are shown for
Study characteristics
Six studies compared GLP-1 receptor agonists (oral tirzepatide, semaglutide, liraglutide, exenatide, lixisenatide, dulaglutide) with conventional management, and two compared bariatric surgery (Roux-en-Y gastric bypass, gastric banding, sleeve gastrectomy) with conventional management. Study designs included one prospective cohort, six retrospective cohorts, and one case–control study. Conventional management strategies varied from acetazolamide monotherapy to combination regimens (acetazolamide, topiramate, and diuretics including furosemide) with lifestyle-based weight reduction approaches. The reported acetazolamide dosage range varied within each study from 0 to 1500 mg with no fixed dose within any group21,22,24 No dosage range for other medications was reported. Detailed characteristics are presented in Table 1.
Baseline Characteristics of Studies Included in the Network Meta-Analysis
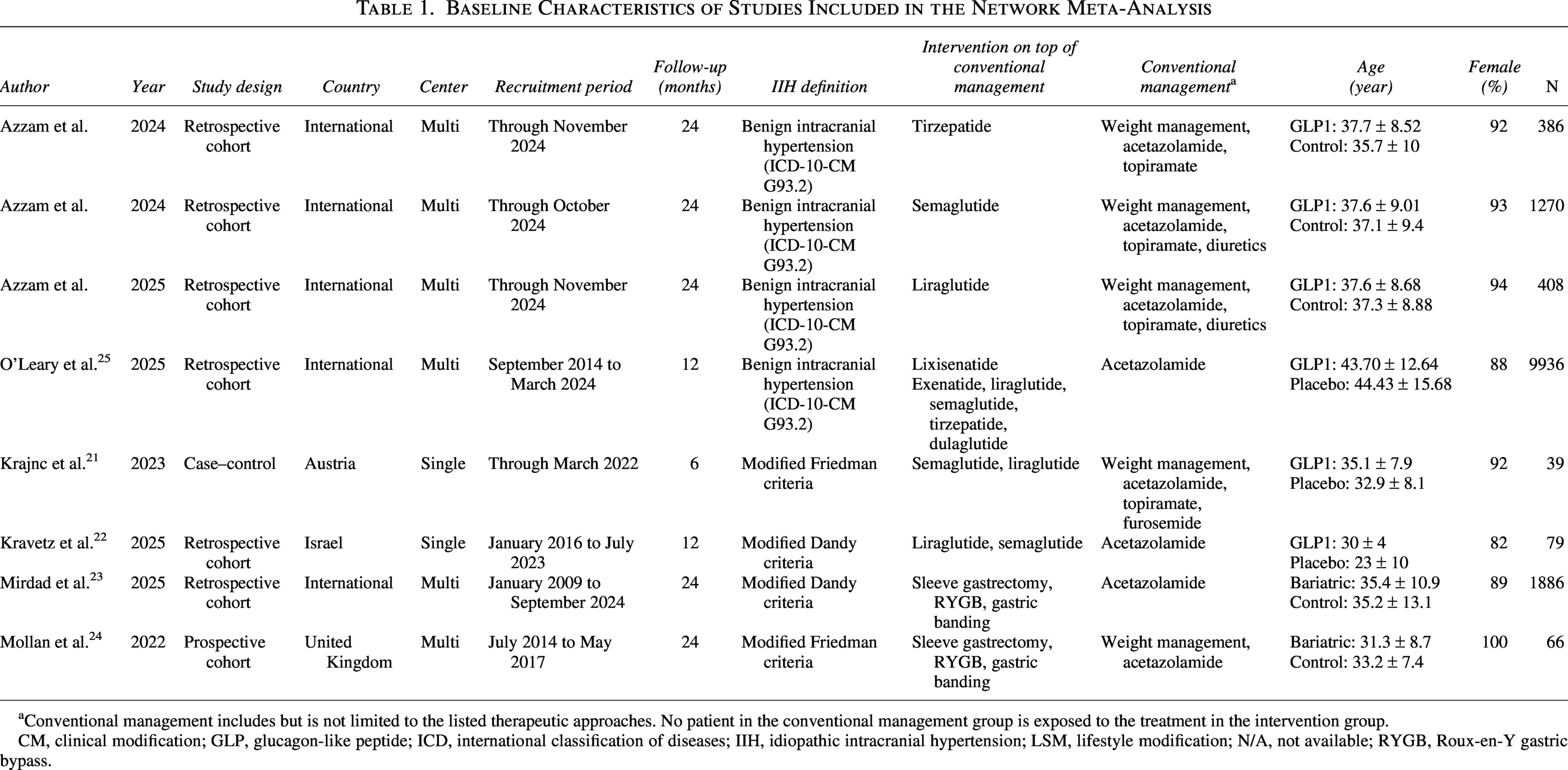
Conventional management includes but is not limited to the listed therapeutic approaches. No patient in the conventional management group is exposed to the treatment in the intervention group.
CM, clinical modification; GLP, glucagon-like peptide; ICD, international classification of diseases; IIH, idiopathic intracranial hypertension; LSM, lifestyle modification; N/A, not available; RYGB, Roux-en-Y gastric bypass.
Papilledema (six studies; five GLP-1RA vs. conventional18–22; one bariatric vs. conventional 23 ).
Change from baseline—GLP-1RA versus conventional (Table 2, Supplementary Table S2, Supplementary Fig. S2): There was no significant change in papilledema from baseline to end of follow-up (MD 0.538; 95% CI: −2.441 to 3.516; I2 = 0.0%), nor at 3 months (MD −0.023; 95% CI: −0.182 to 0.135; I2 = 0.0%) or 6 months (MD 0.093; 95% CI: −0.414 to 0.600; I2 = 0.0%). Sensitivity analyses were concordant. Between-group comparisons at baseline and follow-up were similarly nonsignificant.
Pooled Mean Differences for GLP-1-RAs Versus Conventional Treatment in Pairwise Meta-Analysis
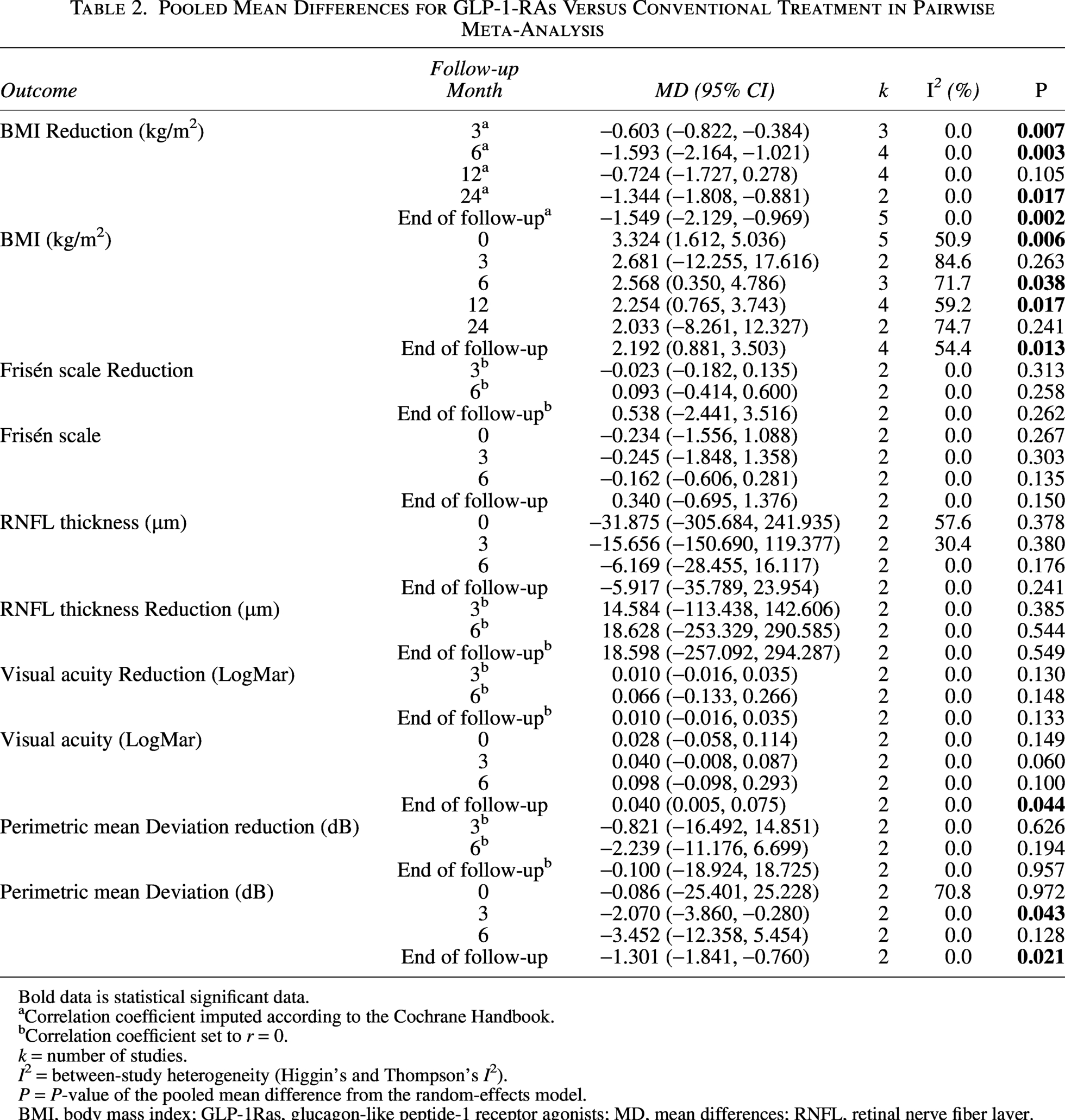
Bold data is statistical significant data.
Correlation coefficient imputed according to the Cochrane Handbook.
Correlation coefficient set to r = 0.
k = number of studies.
I2 = between-study heterogeneity (Higgin’s and Thompson’s I2).
P = P-value of the pooled mean difference from the random-effects model.
BMI, body mass index; GLP-1Ras, glucagon-like peptide-1 receptor agonists; MD, mean differences; RNFL, retinal nerve fiber layer.
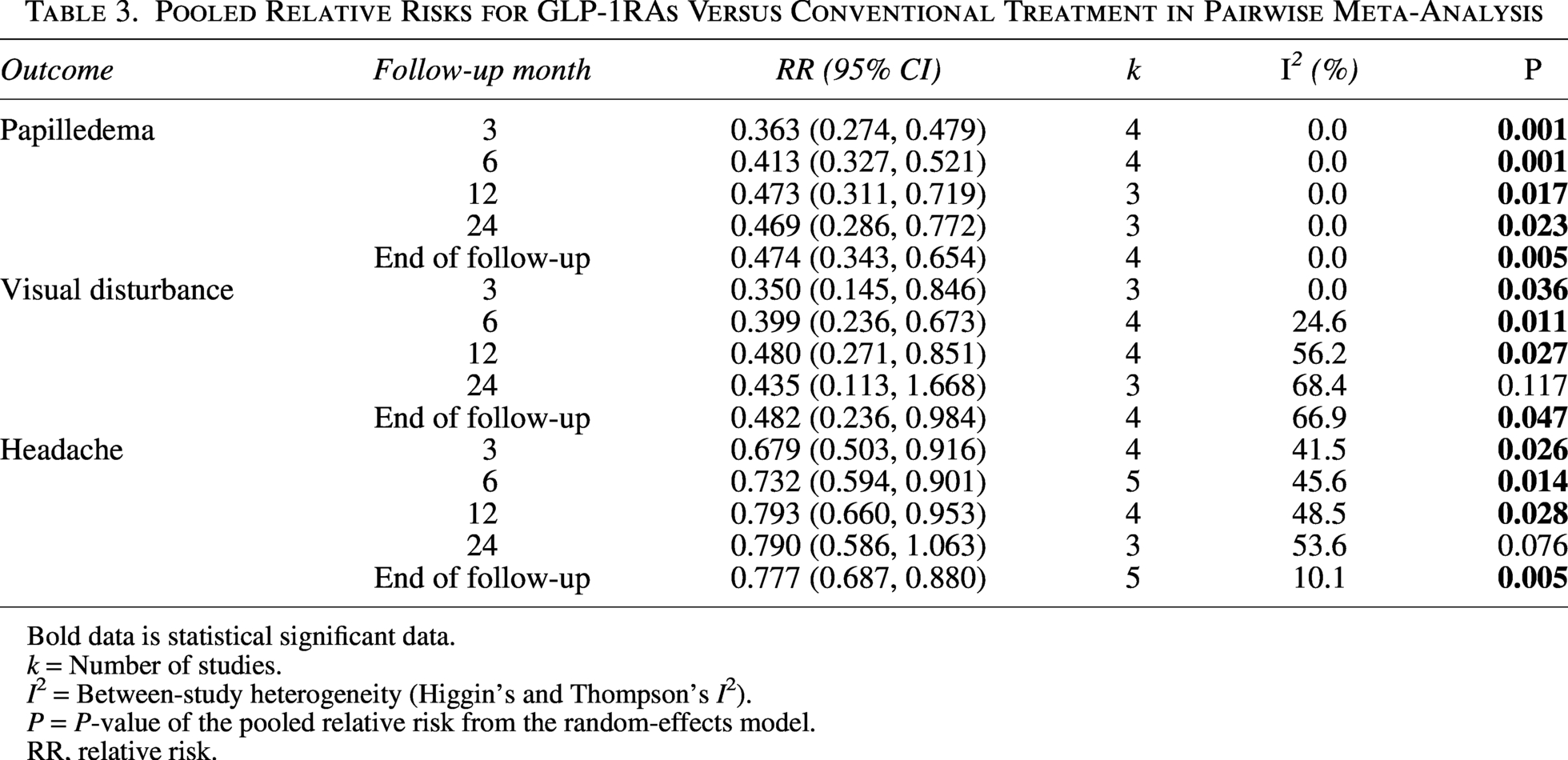
Risk of any papilledema—GLP-1RA versus conventional (Table 3, Supplementary Fig. S2): The risk was lower with GLP-1RAs at end of follow-up (RR 0.474; 95% CI: 0.343–0.654; I2 = 0.0%) and consistently at 3 months (RR 0.363; 95% CI: 0.274–0.479; I2 = 0.0%), 6 months (RR 0.413; 95% CI: 0.327–0.521; I2 = 0.0%), 12 months (RR 0.473; 95% CI: 0.311–0.719; I2 = 0.0%), and 24 months (RR 0.469; 95% CI: 0.286–0.772; I2 = 0.0%).
Pooled Relative Risks for GLP-1RAs Versus Conventional Treatment in Pairwise Meta-Analysis
Bold data is statistical significant data.
k = Number of studies.
I2 = Between-study heterogeneity (Higgin’s and Thompson’s I2).
P = P-value of the pooled relative risk from the random-effects model.
RR, relative risk.
Network meta-analysis (Supplementary Table S3, Supplementary Fig. S3): When comparing GLP-1RAs to bariatric surgery, P-scores at 3, 6, 12, and 24 months and end of follow-up were 0.947 versus 0.552; 0.935 versus 0.547; 0.928 versus 0.572; 0.954 versus 0.546; 0.949 versus 0.550, respectively. However, no significant difference in risk (RR 0.802; 95% CI: 0.571 to 1.126) was noted.
RNFL thickness (three studies; two GLP-1RA vs. conventional21,22; one bariatric vs. conventional 24 ).
GLP-1RA versus conventional (Table 2, Supplementary Table S2, Supplementary Fig. S4): No significant difference in RNFL thickness at end of follow-up (MD 18.598 µm; 95% CI: −257.092 to 294.287; I2 = 0.0%) or at 3 months (MD 14.584 µm; 95% CI: −113.438 to 142.606; I2 = 0.0%) and 6 months (MD 18.628 µm; 95% CI: −253.329 to 290.585; I2 = 0.0%). Baseline and follow-up between-group comparisons were also nonsignificant. Sensitivity analyses replicated these findings.
Network meta-analysis (Supplementary Table S4, Supplementary Fig. S5): P-scores between GLP-1RAs and bariatric surgery were 0.404 versus 0.366 at 12 months and 0.390 versus 0.237 at 12 months. However, no significant differences at 12 months (MD 1.100; 95% CI: −19.721 to 21.921) or at the end of follow-up (MD 4.483; 95% CI: −16.519 to 25.485) were noted.
Visual acuity (two studies; GLP-1RA vs. conventional21,22).
Change from baseline (Table 2, Supplementary Table S2, Supplementary Fig. S6): No significant differences at end of follow-up (MD 0.010 LogMAR; 95% CI: −0.016 to 0.035; I2 = 0.0%) or at 3 months (MD 0.010 LogMAR; 95% CI: −0.016 to 0.035; I2 = 0.0%) and 6 months (MD 0.066 LogMAR; 95% CI: −0.133 to 0.266; I2 = 0.0%) were noted. Sensitivity analyses were consistent.
Between-group comparisons (Table 2, Supplementary Fig. S6): Baseline, 3-month, and 6-month estimates showed no differences, whereas visual acuity favored GLP-1RAs at the end of follow-up (MD 0.040 LogMAR; 95% CI: 0.005 to 0.075; I2 = 0.0%).
Visual field (three studies; two GLP-1RA vs. conventional21,22; one bariatric vs. conventional 24 ).
Change from baseline—GLP-1RA versus conventional (Table 2, Supplementary Table S2, Supplementary Fig. S7): No significant differences in perimetric mean deviation at end of follow-up (MD −0.100 dB; 95% CI: −18.924 to 18.725; I2 = 0.0%) or at 3 months (MD −0.821 dB; 95% CI: −16.492 to 14.851; I2 = 0.0%) and 6 months (MD −2.239 dB; 95% CI: −11.176 to 6.699; I2 = 0.0%) were observed. Sensitivity analyses were consistent.
Between-group comparisons (Table 2, Supplementary Fig. S7): Baseline and 6-month values were similar; however, the GLP-1RA group had worse measurements at 3 months (MD −2.070 dB; 95% CI: −3.860 to −0.280; I2 = 0.0%) and at end of follow-up (MD −1.301 dB; 95% CI: −1.841 to −0.760; I2 = 0.0%) (Table 2, Supplementary Fig. S12).
Network meta-analysis (Supplementary Tables S4, and S5, Supplementary Fig. S8): P-scores for GLP-1RAs versus bariatric surgery were 0.515 versus 0.448 at end follow-up. However, no significant difference between these interventions was observed (MD 0.600; 95% CI: −10.411 to 11.611). Sensitivity analyses were concordant (Supplementary Table S5).
Visual disturbance (five studies; four GLP-1RA vs. conventional18–20,25; one bariatric vs. conventional 24 ).
(Defined as visual discomfort/defects or ICD-10 H53–H54).
GLP-1RA versus conventional (Table 3, Supplementary Fig. S9): Lower risk with GLP-1RAs at end of follow-up (RR 0.482; 95% CI: 0.236 to 0.984; I2 = 66.9%) and at 3 months (RR 0.350; 95% CI: 0.145–0.846; I2 = 0.0%), 6 months (RR 0.399; 95% CI: 0.236–0.673; I2 = 24.6%), and 12 months (RR 0.480; 95% CI: 0.271–0.851; I2 = 56.2%) were noted.
Network meta-analysis (Supplementary Table S3, Supplementary Fig. S10): P-scores for GLP-1RAs versus bariatric surgery at 3, 6, 12, and 24 months and end of follow-up were 0.950 versus 0.474, 0.910 versus 0.555, 0.832 versus 0.634, 0.837 versus 0.588, 0.822 versus 0.625, respectively. However, no significant difference between these interventions was observed (RR 0.832; 95% CI: 0.314–2.207).
Headache (seven studies; five GLP-1RA vs. conventional18–21,25; two bariatric vs. conventional23,24).
GLP-1RA versus conventional (Table 3, Supplementary Fig. S11): Lower risk of headache at end of follow-up (RR 0.777; 95% CI: 0.687–0.880; I2 = 10.1%), consistent at 3 months (RR 0.679; 95% CI: 0.503–0.916; I2 = 41.5%), 6 months (RR 0.732; 95% CI: 0.594–0.901; I2 = 45.6%), and 12 months (RR 0.793; 95% CI: 0.660–0.953; I2 = 48.5%).
Network meta-analysis (Supplementary Tables S4, S5, Supplementary Fig. S12): P-scores for risk of headache when comparing GLP-1RAs versus bariatric surgery at 3, 6, 12, and 24 months and end of follow-up were 0.932 versus 0.465, 0.933 versus 0.442, 0.900 versus 0.539, 0.913 versus 0.503, and 0.945 versus 0.496, respectively. However, no significant difference in risk was noted (RR 0.881; 95% CI: 0.718–1.080). For monthly headache days, P-score was 0.764 for GLP-1RA and 0.514 for bariatric surgery, though there was no significant difference (MD −1.5 days; 95% CI: −29.131 to 26.131). Sensitivity analyses were consistent.
BMI (seven studies; five GLP-1RA vs. conventional18,20–22,25; two bariatric vs. conventional23,24).
GLP-1RA versus conventional—change over time (Table 2, Supplementary Table S2, Supplementary Fig. S13): GLP-1RAs produced greater BMI reduction overall (MD −1.549 kg/m2; 95% CI: −2.129 to −0.969), consistent at 3 months (MD −0.603 kg/m2; 95% CI: −0.822 to −0.384; I2 = 0.0%), 6 months (MD −1.593 kg/m2; 95% CI: −2.164 to −0.021; I2 = 0.0%), and 24 months (MD −1.344 kg/m2; 95% CI: −1.808 to −0.881; I2 = 0.0%). Sensitivity analyses were concordant.
GLP-1RA versus conventional—absolute BMI at time points (Table 2, Supplementary Fig. S13): The GLP-1RA cohort started heavier and often remained heavier, with between-group MDs of baseline MD 3.324 (95% CI: 1.612 to 5.036; I2 = 50.9%); 3 months MD 2.681 (95% CI: −12.255 to 17.616; I2 = 84.6%); 6 months MD 2.568 (95% CI: 0.350–4.786; I2 = 71.7%); 12 months MD 2.254 (95% CI: 0.765–3.743; I2 = 59.2%); 24 months MD 2.033 (95% CI: −8.261 to 12.327; I2 = 74.7%); and end of follow-up MD 2.192 (95% CI: 0.881–3.503; I2 = 54.4%). The magnitude of this difference generally decreased with longer follow-up.
Bariatric surgery versus conventional (Supplementary Table S6, Supplementary Fig. S13): Individual studies consistently showed lower BMI with surgery across follow-up; however, the pooled estimate was imprecise and not statistically significant (MD −6.472 kg/m2; 95% CI: −45.631 to 32.687; I2 = 72.1%).
Network meta-analysis (Supplementary Table S4, S5, Supplementary Fig. S14): No significant difference in BMI reduction between GLP-1RAs and bariatric surgery (MD 10.213 kg/m2; 95% CI: −11.873 to 32.298; P-scores 0.395 vs. 0.812) (Supplementary Table S4); sensitivity analyses were concordant (Supplementary Table S5). In absolute terms, BMI was higher in the GLP-1RA group at end of study (MD 7.201 kg/m2; 95% CI: 4.909–9.493) and at 6 months (MD 4.763 kg/m2; 95% CI: 2.653–6.873), 12 months (MD 6.561 kg/m2; 95% CI: 4.453–8.668), and 24 months (MD 8.148 kg/m2; 95% CI: 3.123–13.173), with P-scores 0.000 versus 0.995–1.000 at these time points (Supplementary Table S4).
Publication bias
Visual inspection of funnel plots and Egger’s test indicated small-study effects for 6-month BMI reduction. No outliers were identified; given the small number of studies, no adjustments were applied. Other time points did not suggest publication bias, and effect directions remained consistent.
Discussion
This meta-analysis is the first to compare GLP-1RAs, bariatric surgery, and conventional treatment in IIH. Adjunctive GLP-1RA therapy, versus conventional management alone, was associated with greater BMI reduction and lower risks of papilledema, visual disturbances, and headache, whereas changes in papilledema severity (Frisén scale) and RNFL thickness did not differ. Visual efficacy signals were mixed: end-of-follow-up visual acuity favored GLP-1RAs, while visual field values were worse at some time points. In indirect comparisons with bariatric surgery, despite higher P-score rankings for GLP-1RAs among several outcomes including papilledema, visual outcomes, and headache, no statistically significant differences between these interventions emerged.
Biologically, these observations are plausible. Glucagon-like peptide-1 (GLP-1) is a multifunctional incretin that enhances insulin sensitivity without hypoglycemia risk, increases satiety, and delays gastric emptying. It also modulates adipose depots (including reductions in centripetal fat), supporting weight loss and metabolic improvement. 26 Beyond weight effects, GLP-1RA activity within the central nervous system (CNS) aligns with IIH pathophysiology. 27 Choroid plexus GLP-1 receptors reduce Na+/K+-ATPase activity and CSF secretion, thereby lowering ICP21. GLP-1 signaling can improve glymphatic function and paravascular exchange.28,29 It also attenuates neuroinflammation via reduced expression of TNF, IL-6, IL-1β, and Nos2 in microglia. 30
The spectrum of IIH-related visual outcomes includes transient obscurations, acuity loss, field defects, and papilledema. 31 These manifestations derive largely from pressure transmission to the optic nerve head, causing axoplasmic stasis, intra-axonal swelling, microvascular compression, and ischemic injury. 32 Prior trials (e.g., Idiopathic Intracranial Hypertension Treatment Trial (IIHTT)) show that weight loss and acetazolamide with dietary measures improve visual endpoints. 33 Consistent with this, our synthesis found lower risks of papilledema and visual disturbances with GLP-1RAs and greater BMI reductions versus conventional therapy.
The discordant finding of reduced papilledema risk without significant improvement in papilledema grading demonstrates fundamental differences in what these metrics measure. Binary outcomes assess the risk associated with the development or resolution of papilledema, while continuous outcomes provide insight into the magnitude of progression or improvement associated with each intervention. All included studies that reported papilledema grading documented low baseline grades.21,22 In this context, small changes in severity scores can result in clinically meaningful transitions between papilledema being present or absent. Additionally, the Frisén scale’s ordinal nature limits its interpretability when treated as a continuous variable, as reported in most studies.
The discrepancy between favorable acuity at study end but worse visual fields at interim time points requires careful interpretation. This finding could reflect differences in visual acuity assessment methods, with one study analyzing both eyes 22 while another used the worse eye only, 21 or the varied exclusion criteria, with one study excluding patients with fulminant IIH or severe papilledema with visual compromise. 22 Nevertheless, this signal warrants caution given reported ophthalmical adverse events with GLP-1RAs: associations with nonarteritic anterior ischemic optic neuropathy34,35 (possibly via sympathetic effects on optic nerve head perfusion or rapid glycemic correction causing swelling/infarction), 36 and diabetic retinopathy complications with rapid glycemic improvement.37–39
Headache outcomes favored GLP-1RAs versus conventional therapy at multiple time points. Headache is prevalent in IIH (often migraine-like) and can persist as “post-IIH headache,” frequently uncoupled from opening pressure or papilledema severity.5,40,41 Mechanistically, IIH headache likely shares migraine pathways—trigeminovascular activation and central sensitization. 16 Obesity models demonstrate increased photophobia, allodynia, and calcitonin gene-related peptide (CGRP) signaling with higher cortical spreading depression rates. 42 GLP-1 receptor expression in microglia within the trigeminocervical complex and liraglutide’s suppression of nitroglycerin-induced sensitization, inflammatory mediators, and nociceptive proteins (CGRP, c-Fos) provide a biologically coherent basis for headache improvement beyond weight reduction. 43
Compared with GLP-1RAs, bariatric surgery produced larger BMI decreases, consistent with real-world data (−24.2% vs. −7.5%) 44 yet GLP-1RAs tended to rank better for ophthalmical and headache outcomes. Pharmacology may explain this: surgery elevates endogenous GLP-1, which has a 1-2-minute half-life and rises mainly postprandially, 45 whereas GLP-1RAs have extended half-lives (hours to days), higher receptor potency, and additional neuroglial effects that may mitigate neuroinflammation. 46
Our study is limited by the predominance of nonrandomized designs (especially retrospective cohorts), which are vulnerable to confounding by indication and selection bias despite adjusted estimates. Patients in these cohorts may have different disease severity, treatment eligibility, and contraindications compared to typical IIH patients. While matched control groups exist, they were artificially constructed with potential residual confounding. Clinical heterogeneity was substantial with inconsistently reported disease severity, timing of intervention, varying doses and agents used for GLP-1RA, different types of bariatric procedures, and differences in experience between each center. Additionally, the distinct weight loss trajectories for each intervention mean that standardized follow-up time points may favor one treatment over another. Without head-to-head trials comparing GLP-1RA to bariatric surgery, our network meta-analysis relied on indirect comparisons and the transitivity assumption. This assumption may be challenged by several differences between included studies. Baseline imbalances existed, including differences in baseline BMI, which is a disease-modifying factor. Disease severity was inconsistently reported and heterogenous across nodes, with some studies excluding severe cases. 22 Disease definitions and diagnostic criteria varied between studies. Background conventional treatment ranged from acetazolamide monotherapy to combination regimens with nonpharmacologic approaches. Treatment eras also differed across studies. Outcome definitions and measurements were not uniform—visual disturbance (ICD-10 codes vs. symptom-based), papilledema grading (Frisén inter-rater variability), visual-field platforms/algorithms, and RNFL segmentation protocols—limiting comparability. We relied on aggregate (study-level) data, precluding individual–participant adjustments or effect-modifier analyses; change scores were occasionally imputed using assumed pre–post correlations, introducing uncertainty. We partially addressed these through change-from-baseline analyses, when possible, sensitivity analyses, and random-effects models, but residual confounding remains. Consequently, our findings should be interpreted as hypothesis-generating, identifying potential areas for future trials rather than establishing definitive treatment guidelines.
Future work should prioritize adequately powered randomized and prospective comparative studies that harmonize outcome definitions, adjust for baseline imbalances, and specify control regimens. Comparative effectiveness across GLP-1RA classes and doses, bariatric procedures, and nonpharmacologic weight strategies is needed. Given differential weight-loss efficacy among agents (e.g., ∼5.4% with liraglutide vs. ∼12.5% with semaglutide), 47 studies should disentangle weight-mediated from drug-specific neurological effects. Agents with dual incretin activity (e.g., tirzepatide) merit investigation in IIH. Durability studies after GLP-1RA discontinuation are also needed to inform long-term care.
In conclusion, GLP-1RA therapy as an adjunct to conventional IIH management may be associated with weight loss and improved clinical outcomes, with a signal for possible worsening of visual fields at certain time points that warrants vigilance. Given the unmet need in IIH and limitations of current evidence, prospective randomized controlled trials are needed to establish GLP-1RAs’ efficacy, safety, and optimal use as an adjunct to IIH treatment.
Authors’ Contributions
S.P., N.S., P.P., and P.A. designed the meta-analysis and searched for relevant studies. S.P., N.S., and P.P. selected the studies and extracted the relevant information. S.P., N.S., and P.A. drafted the first article for intellectual content, created the tables and figures, analyzed data, and interpreted the data. All authors revised the article and approved the final article as submitted and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgment
The authors appreciate Auranee Trisataya for providing the concept about the GLP-1 receptor mechanism for the draft discussion section of the article.
Data Availability
The original data were kept with the first and corresponding author. Data could be shared upon request.
Author Disclosure Statement
S.P., N.P., P.P., A.V., and G.W.R. do not have any financial or nonfinancial potential conflicts of interest. P.A. and S.T. have received speaker and advisory board honoraria from BL HUA, DKSH, Lundbeck, Pfizer, and ZP Therapeutics.
Funding Information
The authors received no funding for this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.