
Abstract
Introduction:
Traditional biomarkers like creatinine and estimated glomerular filtration rate (eGFR) often fail to detect early diabetic nephropathy. Proenkephalin A (PENK-A), a stable, kidney-specific peptide, has emerged as a potential alternative biomarker. This study aimed to evaluate serum PENK-A levels in diabetic nephropathy and their association with renal and clinical parameters.
Methods:
In this prospective cross-sectional study, PENK-A levels were compared between patients with type 2 diabetes and healthy controls. Biochemical variables were assessed, and receiver operating characteristic (ROC) analysis was used to determine diagnostic performance. Binary logistic regression was conducted to identify independent predictors of elevated PENK-A levels.
Results:
A total of 120 participants (90 patients, 30 controls) were included. PENK-A levels were significantly higher in patients and correlated with lower eGFR, higher urea, and microalbuminuria. At a cut-off value of 2.25 pmol/L, PENK-A demonstrated moderate diagnostic accuracy (AUC = 0.702, p = 0.001), with high specificity (83.3%) and positive predictive value (90.6%). Logistic regression revealed an independent inverse association between PENK-A and HbA1c, while eGFR showed a borderline relationship.
Conclusion:
Serum PENK-A may serve as a supportive biomarker for renal dysfunction in diabetic nephropathy. Its relationship with HbA1c suggests possible links to metabolic stress. PENK-A could complement traditional markers, particularly in early detection or high-risk patients. Further longitudinal studies are warranted to confirm its prognostic value.
Introduction
According to the 11th edition of the IDF Diabetes Atlas (2025), approximately 589 million adults (aged 20–79 years) are currently living with diabetes mellitus (DM) worldwide, and this number is projected to rise to 853 million by 2050.1,2 DM is indeed a multisystem disease with the potential to cause significant complications across multiple organ systems including the kidney, nervous system, cardiovascular system, especially the eye, and can lead to loss of functions.
Diabetic nephropathy is one of the most common microvascular complications of diabetes and is associated with the loss of kidney function. 3 It is also a condition with high mortality and morbidity and is seen in 40% of patients with diabetes.4,5 Diabetic nephropathy is characterized by glomerular hyperfiltration and albuminuria in the initial stages, subsequently followed by a progressive decline in renal function. In the context of diabetic kidney disease (DKD), the risk of end-stage renal disease is determined by albuminuria and estimated glomerular filtration rate (eGFR) measurement.
The assessment of renal function through creatinine levels is subject to various confounding factors, including muscular composition, metabolic rate, dietary intake, and pharmaceutical agents, which may complicate its interpretation. 5 Additionally, creatinine is actively secreted within the renal tubules, and its serum levels demonstrate a delayed elevation compared to the reduction in eGFR. 6 Despite extensive research involving various biomarkers, including neutrophil gelatinase-associated lipocalin, kidney injury molecule 1, inulin, and Cystatin C, their clinical utility in assessing real-time kidney function remains limited.7–12 These limitations have necessitated the exploration of alternative biomarkers capable of providing more accurate and sensitive assessments of renal function for various clinical contexts.
Enkephalins, classified as endogenous opioid peptides, primarily interact with delta opioid receptors. These receptors exhibit the highest concentration in cerebral tissues, with renal tissues demonstrating the second highest concentration. 13 The PENK gene is expressed in non-neuronal organs and systems such as the kidney, heart and muscle tissue, as well as the central nervous system. 14 Through proteolytic cleavage of PENK, the initial translation product, Preproenkephalin A is generated including a sequence of 267 amino acids. Various bioactive peptides are generated by the cleavage of Preproenkephalin A. Proenkephalin A (PENK-A), a larger and more stable molecule than these active peptides, exhibits a prolonged half-life and remains unaffected by age and gender. 15
While the exact function of PENK-A in renal physiology remains incompletely characterized, experimental studies in animal models have illuminated its participation in regulatory mechanisms, including diuresis, natriuresis, and the inhibition of antidiuretic hormone.16,17 It is considered to be more sensitive in assessing renal function due to its ability to circulate freely in plasma without binding to proteins, undergo glomerular filtration, and remain stable in plasma for 48 h.18,19 In addition, studies have shown that PENK-A is associated with acute renal failure developing in some clinical conditions such as acute and chronic heart failure and sepsis and is considered a prognostic marker.19–25
The objective of this research was to investigate the serum concentration of PENK-A, a potential novel indicator of renal function, and its correlation with select clinical and laboratory variables in individuals diagnosed with diabetic nephropathy. The study focused on patients who had not yet developed end-stage renal disease or severe kidney dysfunction.
Materials and Methods
Between January 2024 and June 2024, participants were prospectively and consecutively recruited from individuals attending the diabetes outpatient clinic. The diagnosis of diabetic nephropathy was established according to eGFR measurement and amount of albumin measured in 24-h urine. The assessment of albuminuria was performed using 24-h urine collections to measure urinary albumin excretion. The eGFR was calculated using the chronic kidney disease (CKD)–EPI equation. Patients with diabetic nephropathy were included if they had an eGFR between 40 and 60 mL/min/1.73 m2, regardless of albuminuria status, or if they had micro- or macroalbuminuria with eGFR ≥60 mL/min/1.73 m2. Patients with eGFR <40 mL/min/1.73 m2 or clinical evidence of advanced kidney disease were excluded. Although the standard CKD staging groups use eGFR thresholds of 45 and 30 mL/min/1.73 m2 (representing G3b and G4), we adopted a more conservative inclusion threshold of ≥40 mL/min to capture moderate CKD (G3a–G3b) while excluding advanced disease, consistent with age-adapted approaches in the literature. The control group consisted of individuals attending routine outpatient visits who had normal renal function (eGFR > 90 mL/min/1.73 m2), no albuminuria, and no history of diabetes, hypertension, or cardiovascular disease.
Both patients and controls were prospectively and consecutively enrolled during the study period based on predefined inclusion and exclusion criteria. Written and verbal consent was obtained from all patients. Approval for the study was obtained from the local ethics committee.
Demographic and clinical data, including age, sex, comorbid conditions (such as hypertension, ischemic heart disease, and peripheral vascular disease), and use of sodium-glucose co-transporter 2 (SGLT-2) inhibitors, were obtained through patient medical records and standardized data collection forms during initial clinical evaluation. Venous blood samples were taken from all patients included in the study following an 8-h fasting at the time of admission. Fasting glucose, HbA1c %, estimated average glucose (EAG), urea, creatinine, eGFR, total cholesterol, high-density lipoprotein (HDL)-cholesterol, low-density lipoprotein (LDL)-cholesterol, triglyceride, and PENK A levels were measured in the venous blood samples.
For serum PENK-A, blood samples from patients and controls were collected in Sarstedt S-Monovette® vacutainer tubes (Sarstedt AG & Co. Germany, Lot no: 2034725) and centrifuged at 1500g for 10 min. The serum was then stored at −20°C until the laboratory analysis.
Human PENK-A levels (ng/mL) were measured by sandwich Enzyme-Linked Immunosorbent Assay method using the human PENK-A kit (Shanghai Sunred Biological Technology Co., Ltd, China, Catalog No: 201-12-2342).
Statistics
Statistical methods: Mean ± SD for normally distributed variables and median [IQR] for non-normally distributed variables were used. The distribution of variables was checked with Kolmogorov–Smirnov test. Independent samples T test and Mann–Whitney U test were used for the comparison of quantitative data. Chi-square test was used for the comparison of the qualitative data. Receiver operating characteristic (ROC) curve analysis was performed to determine the discriminatory power and diagnostic threshold (cut-off) of serum PENK-A levels for identifying diabetic nephropathy. Subgroup analysis was conducted by stratifying patients based on a serum PENK-A cut-off value of 2.25 pmol/L, which was determined through ROC analysis. SPSS 27.0 was used for statistical analyses.
Before the study began, a sample size calculation was performed to detect a medium effect size (Cohen’s d equals 0.5) with 80% power at a 5% significance level. This analysis indicated that each group should include at least 64 participants. However, due to the number of eligible individuals available during the study period, a total of 120 participants were enrolled, including 90 patients and 30 healthy controls. Although the group sizes were not equal, the relatively high number of patients allowed for meaningful evaluation of biomarker distributions and associations. This sample structure enabled subgroup analyses, ROC curve evaluation, and regression modeling within the patient group, supporting the generation of novel and clinically relevant findings.
Results
A total of 120 patients including 90 patients and 30 healthy controls, were included in the study. We compared their clinical and laboratory findings to evaluate whether serum PENK-A levels differed between the two groups. Clinical and demographic characteristics of the patients are presented in Table 1.
Baseline Demographic, Clinical, and Laboratory Characteristics of Study Population
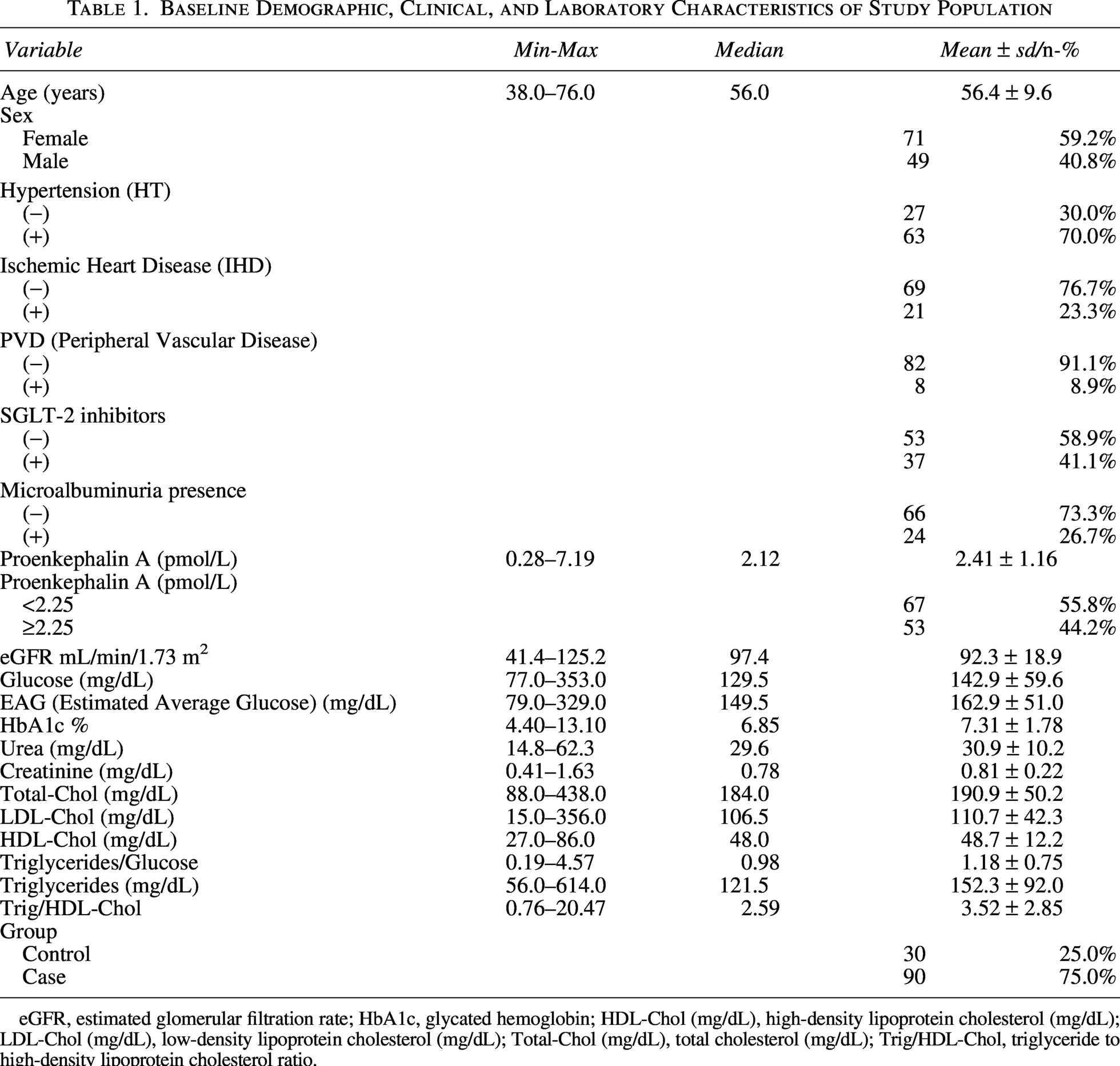
eGFR, estimated glomerular filtration rate; HbA1c, glycated hemoglobin; HDL-Chol (mg/dL), high-density lipoprotein cholesterol (mg/dL); LDL-Chol (mg/dL), low-density lipoprotein cholesterol (mg/dL); Total-Chol (mg/dL), total cholesterol (mg/dL); Trig/HDL-Chol, triglyceride to high-density lipoprotein cholesterol ratio.
There was no significant difference (p > 0.05) in the age and gender distribution of the patients between the case and control groups. PENK-A, glucose, estimated average glucose, HbA1c, urea, and creatinine values were significantly (p < 0.05) higher in the case group than in the control group. eGFR and triglycerides/glucose values were significantly (p < 0.05) lower in the case group than in the control group. Total-cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides and triglycerides/HDL-cholesterol values did not differ significantly (p > 0.05) between the case and control groups. (Table 2)
Comparison of Clinical and Laboratory Data of Groups

mMann–Whitney U test.
χ²Chi-square test (Fischer test).
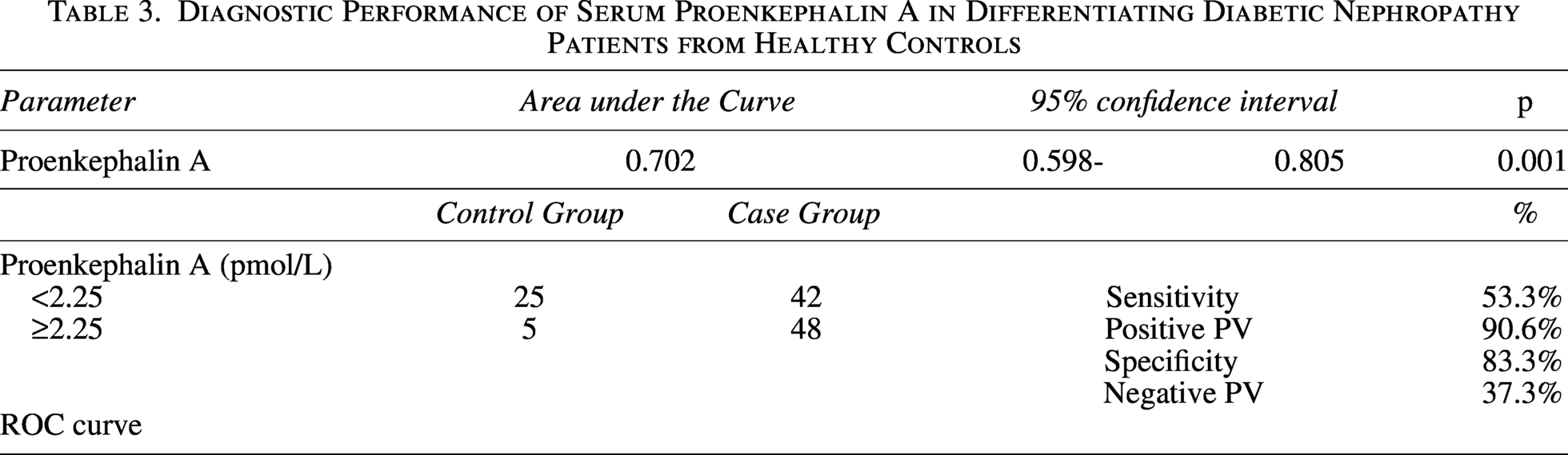
We observed that PENK-A differentiated between the case and control groups with an area under the curve (AUC) of 0.702 (95% CI: 0.598–0.805). The PENK-A 2.25 pmol/L cut-off value exhibited varying degrees of diagnostic accuracy in differentiating between case and control group patients. Specifically, it demonstrated a sensitivity of 53.3%, a positive predictive value of 90.6%, a specificity of 83.3%, and a negative predictive value of 37.3% (Table 3, Fig. 1). These values should be interpreted with caution, as predictive values are influenced by group distribution.
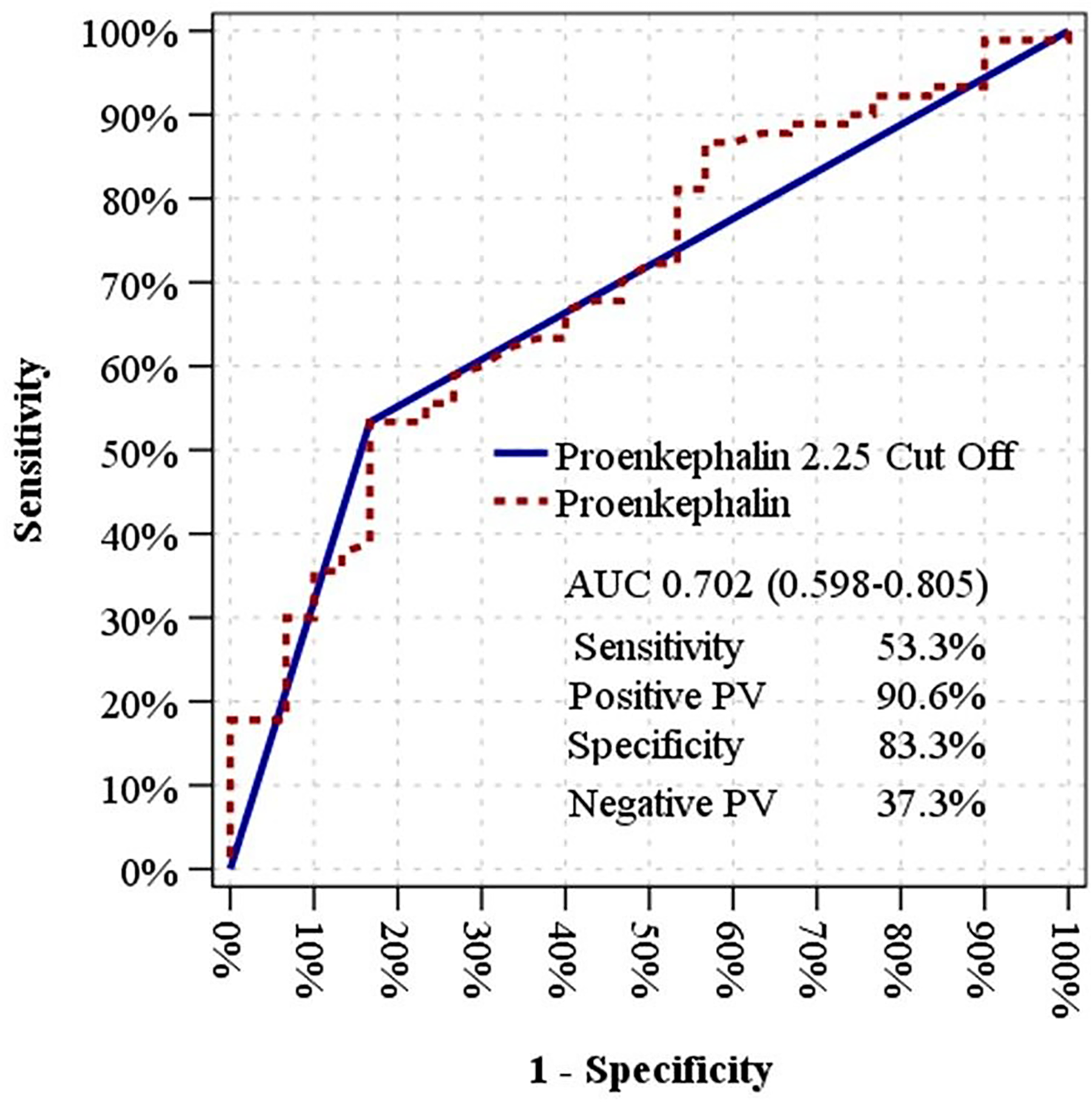
Receiver operating characteristic (ROC) curve demonstrating the diagnostic performance of serum proenkephalin A in differentiating patients with diabetic nephropathy from healthy controls. The area under the curve (AUC) was 0.702 (95% CI: 0.598–0.805), indicating moderate discriminative ability. At the optimal cut-off value of 2.25 pmol/L, sensitivity was 53.3%, and specificity was 83.3%. The ROC curve was generated using continuous PENK-A values with standard axis scaling.
Diagnostic Performance of Serum Proenkephalin A in Differentiating Diabetic Nephropathy Patients from Healthy Controls
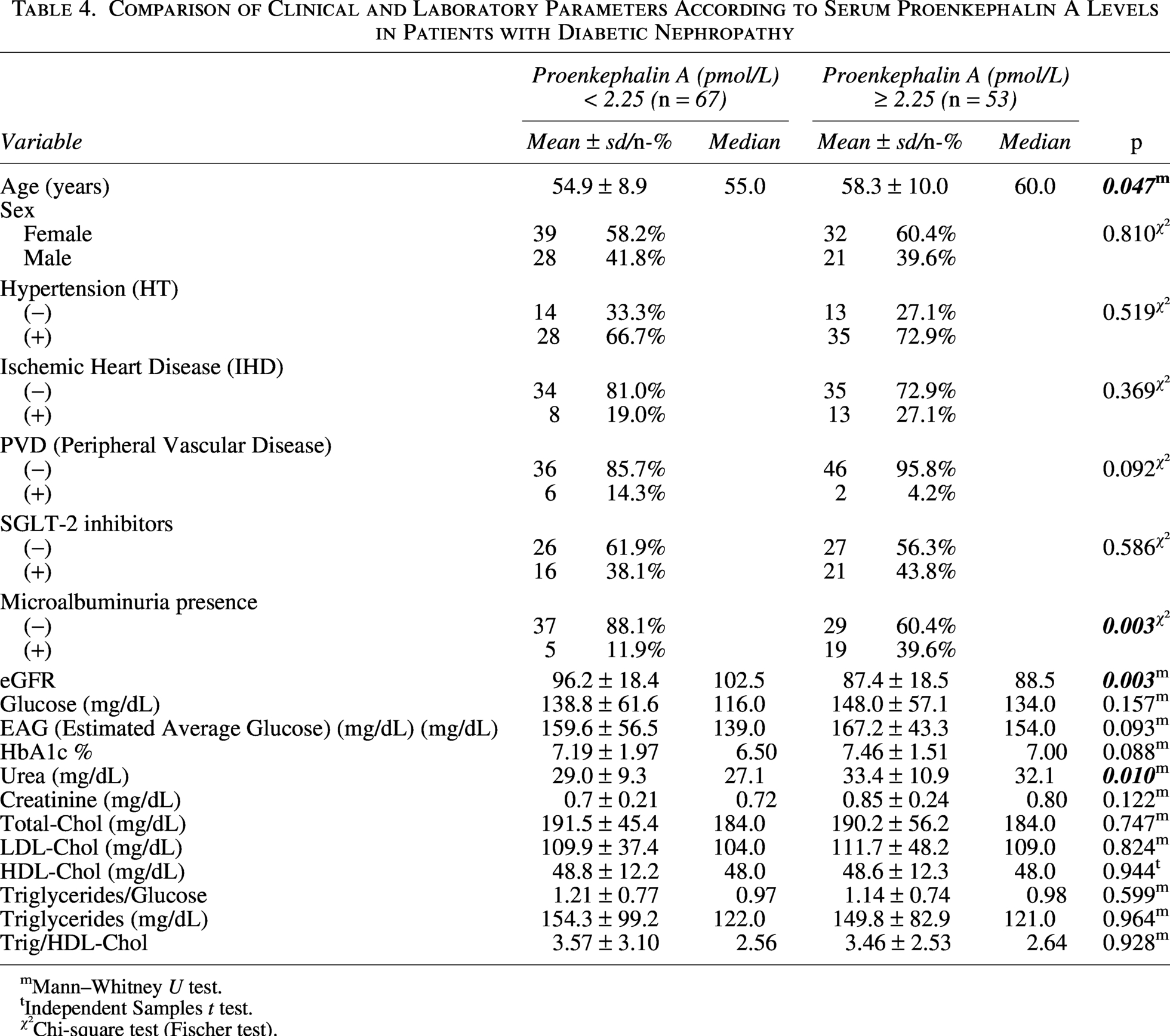
The age of the patients was significantly (p < 0.05) higher in the PENK-A ≥ 2.25 pmol/L group than the PENK-A < 2.25 pmol/L group. There was no significant difference in gender distribution between the PENK-A < 2.25 pmol/L and ≥2.25 pmol/L groups (p > 0.05). There was no significant difference (p > 0.05) in the presence of hypertension, ischemic heart disease and peripheral vascular disease, and the percentage of patients using SGLT-2 inhibitors between the PENK-A < 2.25 pmol/L and ≥2.25 pmol/L groups. The amount of microalbumin was significantly (p < 0.05) higher in the PENK-A ≥ 2.25 pmol/L group than in the PENK-A < 2.25 pmol/L group. The eGFR value was significantly (p < 0.05) lower in the PENK-A ≥ 2.25 pmol/L group than in the PENK-A < 2.25 pmol/L group. Glucose, EAG, HbA1c, creatinine, total-cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides/glucose, triglycerides and trig/HDL-cholesterol values did not differ significantly (p > 0.05) between the PENK-A < 2.25 pmol/L and ≥2.25 pmol/L groups. The urea value was significantly (p < 0.05) higher in the PENK-A ≥ 2.25 pmol/L group than in the PENK-A < 2.25 pmol/L group (Table 4).
Comparison of Clinical and Laboratory Parameters According to Serum Proenkephalin A Levels in Patients with Diabetic Nephropathy
mMann–Whitney U test.
tIndependent Samples t test.
χ²Chi-square test (Fischer test).
In patients with diabetes, only HbA1c (%) was significantly associated with elevated proenkephalin levels (p = 0.005), indicating a protective effect (OR = 0.707, 95% CI: 0.555–0.901). eGFR showed a borderline significant association (p = 0.067), while other variables including age, sex, and triglyceride/glucose ratio, were not significantly associated (Table 5).
Independent Factors Associated with Proenkephalin Levels in Diabetic Patients
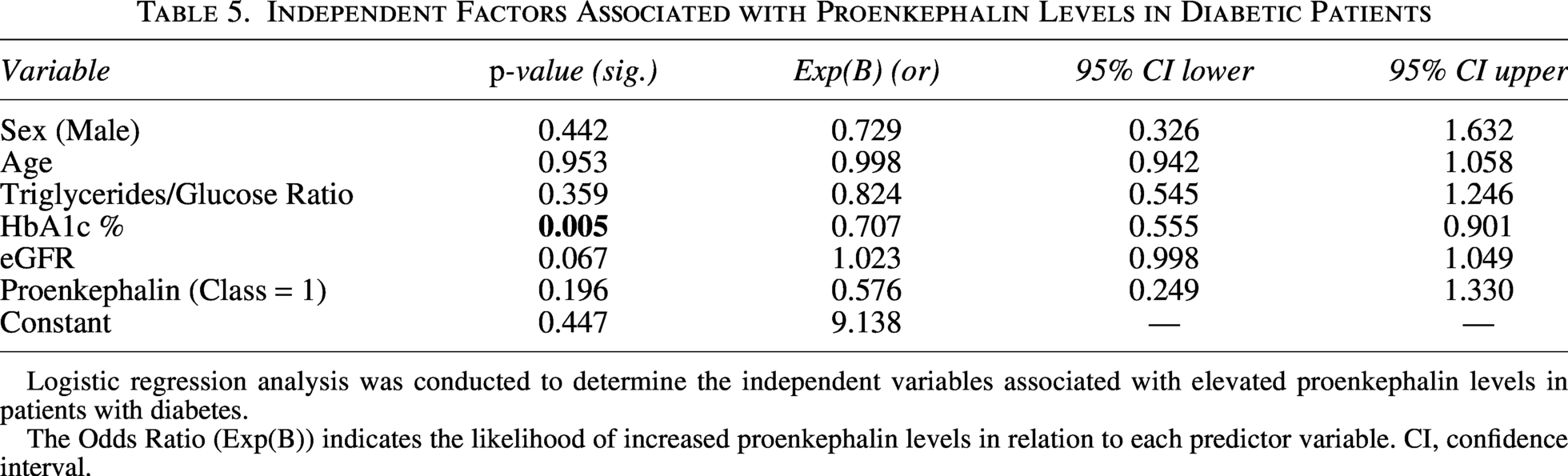
Logistic regression analysis was conducted to determine the independent variables associated with elevated proenkephalin levels in patients with diabetes.
The Odds Ratio (Exp(B)) indicates the likelihood of increased proenkephalin levels in relation to each predictor variable. CI, confidence interval.
Discussion
There remains a clear unmet need for early and sensitive biomarkers to aid in the diagnosis and monitoring of diabetic nephropathy, which was the primary rationale behind the present study.1,3,5,26 We compared PENK-A levels and selected clinical parameters between diabetic patients and healthy individuals. Among patients, elevated PENK-A levels were observed alongside markers of impaired glucose metabolism and reduced kidney function, while eGFR and the triglyceride/glucose ratio were lower. These findings are in line with previous studies suggesting that PENK-A may reflect glomerular filtration dynamics and early renal stress.12,19,21,25 Patients with PENK-A concentrations ≥2.25 pmol/L tended to be older and had higher urea and microalbumin levels, as well as lower eGFR. In our study, logistic regression analysis showed that HbA1c was independently associated with PENK-A levels, indicating a potential link between glycemic control and this biomarker. Although other variables did not reach statistical significance, eGFR showed a borderline association with PENK-A, supporting its biological plausibility. 25 These findings highlight the clinical value of PENK-A as a candidate biomarker in DKD and underscore the need for further prospective studies to confirm its diagnostic and prognostic potential.25,27
These findings are consistent with the expected profile of diabetic nephropathy, including impaired glycemic control and reduced renal function. These findings support the internal validity of our dataset and align with previously reported disease patterns.3,5
Serum creatinine is known to be insensitive to early declines in eGFR, and approximately 75% of patients with stage 3 CKD do not present with albuminuria.28,29 In contrast, PENK-A, widely studied in the context of acute kidney injury, has emerged as a promising functional biomarker. It offers several advantages, including real-time tracking of kidney function, stability against inflammation and comorbidities, kidney-specific excretion, absence of protein binding, and filtration that is not affected by serum protein levels.16,30 Rising PENK-A levels are thought to reflect glomerular injury and impaired renal function. Multiple studies support its value as an early and reliable indicator of kidney dysfunction across various clinical settings.12,18,19,21,30 Schulz et al. found that elevated fasting PENK-A levels were associated with declining renal function and increased CKD risk in diabetic patients. 25 Similarly, Beunders et al. and Caffrey et al. emphasized its responsiveness to subtle changes in glomerular filtration and tubular integrity.19,27,30
Although we observed an association between PENK-A levels and microalbuminuria in our study, this relationship does not fully account for its clinical significance. Albuminuria primarily reflects alterations in glomerular permeability, whereas PENK-A more directly reflects overall renal function, particularly glomerular filtration. Moreover, many patients with early-stage CKD do not exhibit albuminuria.28,29 Therefore, PENK-A may provide additional value in detecting renal dysfunction, especially in cases where albuminuria is absent. Beyond its diagnostic role, elevated PENK-A concentrations have been associated with poor outcomes in patients with heart failure and kidney transplantation, supporting its broader prognostic potential. Taken together, our results are consistent with growing evidence that serum PENK-A may serve not only as a diagnostic marker in diabetic nephropathy but also as a tool for monitoring disease progression and long-term risk.31–33
Among patients with diabetic nephropathy, those with higher PENK-A levels (≥2.25 pmol/L) were older, had lower eGFR, higher urea, and more frequent microalbuminuria, consistent with previous findings linking elevated PENK-A to impaired renal function and glomerular damage.12,19,25,27,30 No associations were found between PENK-A levels and comorbidities, SGLT-2 inhibitor use, fasting glucose, or lipid parameters. However, although HbA1c did not differ significantly between PENK-A subgroups in univariate analysis, logistic regression revealed a significant independent association, with lower HbA1c linked to higher PENK-A levels. This may reflect the underlying metabolic stress or compensatory pathways related to poor glycemic control. A significant correlation with age was also observed at PENK-A levels ≥ 2.5 pmol/L (AUC = 2.5, p < 0.001). The ZODIAC study reported that elevated PENK-A was not independently predictive of cardiovascular mortality in type 2 diabetes over 14 years. Yet, when adjusted for traditional risk factors, high PENK-A levels were associated with increased mortality risk. 33 Other studies have linked PENK-A to future renal decline in general populations. In a 16-year follow-up of 2568 individuals without kidney disease, higher PENK-A levels predicted chronic renal failure, though not albuminuria. 34 Additionally, cross-sectional data showed a relationship between PENK-A and albumin excretion in kidney transplant recipients. 26 However, current evidence does not support its use in predicting end-stage renal disease in diabetic nephropathy. Larger, long-term studies are needed to better define the prognostic role of PENK-A and its potential utility in monitoring renal function in diabetic nephropathy.
Moreover, the control group did not include individuals with diabetes; thus, some differences may stem from diabetes itself, obesity, or medication use rather than nephropathy alone. Future studies comparing diabetic patients with and without nephropathy, while adjusting for these factors, are needed to clarify these associations. Finally, multivariate logistic regression identified HbA1c as the only variable independently associated with PENK-A levels. The inverse relationship suggests a possible link between glucose metabolism and proenkephalin dynamics in DKD. Although eGFR did not reach statistical significance, it showed a borderline association, consistent with previous findings on PENK-A’s sensitivity to glomerular filtration changes. 25 These findings support the potential role of PENK-A as a clinically relevant biomarker when interpreted alongside established renal and metabolic indicators.
This study has several limitations. Due to its cross-sectional design, causal relationships between PENK-A levels and clinical variables cannot be established. The relatively small sample size and single-center nature may limit the generalizability of our results. Additionally, the absence of histological confirmation restricted our ability to exclude other contributors to renal impairment, such as undiagnosed hypertensive nephrosclerosis. We also did not evaluate the impact of medications such as angiotensin converting enzyme inhibitors, nonsteroidal anti-inflammatory drugs, or diuretics, which may influence renal markers, particularly eGFR. Lastly, although logistic regression identified an independent association between PENK-A and HbA1c, the limited number of covariates included and the absence of a longitudinal design preclude conclusions about directionality or underlying mechanisms.
In conclusion, serum PENK-A levels were elevated in patients with diabetic nephropathy and associated with impaired renal function, as evidenced by lower eGFR, higher urea, and increased microalbuminuria. Logistic regression analysis revealed that HbA1c was independently associated with PENK-A levels, suggesting a potential link between glycemic control and this emerging biomarker. Although PENK-A demonstrated moderate diagnostic accuracy, its value may lie in complementing traditional renal markers for early detection and monitoring. Prospective, multicenter studies with longitudinal follow-up are needed to validate these findings and better define the clinical role of PENK-A in DKD.
Authors’ Contributions
F.S., H.U.A., and C.U.A. contributed to the design and implementation of the research; F.S. and Z.A.: Recruiting subjects and studying blood samples taken from subjects; F.S., H.U.A., O.Y., M.A.B., and C.U.A. to the analysis of the results and to the writing of the article. H.U.S. and C.U.A. conceived the original and supervised the project.
Financial Disclosure
The authors received no financial support for the research, authorship, or publication of this article.
Availability of Data and Materials
The datasets generated and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The authors obtained approval from the Ethics Committee of Sağlık Bilimleri University Istanbul Training and Research Hospital on May 7, 2024 (reference number: 05/07/2024-27). The authors conducted all procedures involving human participants in accordance with the ethical standards of the institutional research committee and the Declaration of Helsinki. The authors obtained informed consent from all participants included in the study.
Footnotes
Acknowledgments
This study was previously presented as an abstract at the IV. National Internal Medicine Congress (IV. Ulusal Dahiliye Kongresi), held on May 22–25, 2025, in Antalya, Türkiye. The abstract was published in the congress proceedings book and is available online at: ![]() . The current article includes expanded analyses and full results that have not been published elsewhere.
. The current article includes expanded analyses and full results that have not been published elsewhere.
Author Disclosure Statement
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the article. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. The authors declare that they have NO affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this article.
Funding Information
The author(s) reported there is no funding associated with the work featured in this article. The study received no funding.