
Abstract
Background:
Pregnancy in teenagers and emerging adults is associated with an increased risk of adverse outcomes. Similarly, pregnancies complicated by pregestational and gestational diabetes mellitus (GDM) carry a higher risk of complications. However, limited data exist on the intersection of these two high-risk conditions. Our objective was to establish the prevalence of teenage and emerging adult pregnancies complicated by diabetes in a population-based cohort and compare outcomes to pregnancies uncomplicated by diabetes, noting a background prevalence of GDM of 8.1% and pregestational diabetes of 1.2% across all age groups in the United States.
Methods:
This is a retrospective cohort study conducted in Olmsted County, Minnesota, USA. It includes female residents aged ≤21 years with a pregnancy ICD-10 code between January 1, 2013, and December 31, 2022. The main outcome measures assessed include maternal characteristics and maternal and fetal pregnancy outcomes.
Results:
A total of 1491 pregnancies in 1379 individuals were identified and included. In total, 68 (4.6%) pregnancies were complicated by diabetes: 51 (3.4%) with GDM and 17 (1.1%) with pregestational diabetes. In this study, pregnancies with diabetes had higher rates of adverse outcomes including cesarean delivery (GDM 29.4% vs. pregestational 60.0% vs. no diabetes 17.0%, P < 0.001), preeclampsia (GDM 15.7% vs. pregestational 40.0% vs. no diabetes 7.3%, P < 0.001), large-for-gestational-age neonates (GDM 13.7% vs. pre-existing 50.0% vs. no diabetes 5.8%, P < 0.001), and neonatal hypoglycemia (GDM 42.6% vs. pregestational 60.0% vs. no diabetes 13.3%, P < 0.001).
Conclusions:
The prevalence of pregestational diabetes in our teenage and emerging adult population is similar to that of the general pregnancy population; however, the prevalence of GDM is significantly lower. Overall, diabetes in teenage pregnancy is associated with an elevated risk of adverse maternal and neonatal outcomes. Future research should evaluate interventions aimed at reducing adverse pregnancy outcomes in this vulnerable population.
Keywords
Introduction
In 2022, 8.2 per 1000 births in Minnesota, USA, were to mothers <20 years of age, with an additional 43.0 per 1000 births to mothers aged 20–24 years. 1 Olmsted County, Minnesota, specifically reported that 2.0% of pregnancies from 2016 to 2020 were born to mothers aged 15–19 years, with an another 10.6% being born to mothers 20–24 years. 2 Teen pregnancy is associated with premature maternal mortality, and low maternal age is a unique risk factor for adverse pregnancy outcomes, including preterm birth, low birth weight, and preeclampsia.3–5 Pregnancies complicated by pregestational diabetes and gestational diabetes mellitus (GDM) impacted for 1.2% and 8.1%, respectively, of pregnancies in the United States in 2022. 1 Both pregestational diabetes and GDM are associated with increased risks for both mother and child, including, but not limited to, congenital anomalies, stillbirth, large-for-gestational age infants, birth trauma, and preeclampsia.6–9 Clinical guidelines for pregestational diabetes recommend optimal glycemic control prior to and during pregnancy to minimize the potential for obstetric and neonatal adverse events.10,11 However, achieving optimal glycemic control in teenagers and young adults is challenging, as only 21% of young individuals with type 1 diabetes meet their glycemic control targets.12–14 This is compounded by generally low rates of preconception care in reproductive-aged women with diabetes.15,16 Furthermore, teenagers and emerging adults have also been found to participate in higher rates of novelty-seeking and risky behaviors, 17 which may contribute to the risk of unplanned pregnancies and substance-related obstetric and neonatal complications.
Unfortunately, population-based data on the prevalence of and pregnancy outcomes among individuals with low maternal age and diabetes are scarce.13,18–20 Limited prevalence studies suggest that 0.2%–3.1% of teenage pregnancies are complicated by pregestational diabetes.13,18,19 These studies report an increased risk of preeclampsia, preterm delivery, and increasing neonatal birthweight among teenagers with pregestational diabetes compared to those without diabetes.13,18–20 There are no prior studies examining prevalence and clinical outcomes associated with GDM in this age group. In this context, it is clear that teenagers and emerging adults with diabetes likely represent a uniquely vulnerable group due to the intersecting challenges of diabetes and physiological immaturity. We aim to address a critical literature gap by providing data on disease prevalence and pregnancy outcomes in this understudied population.
The aims of this study are to establish the prevalence of teenage and emerging adult pregnancies complicated by diabetes (pregestational and GDM) in a retrospective cohort from Olmsted County, Minnesota, USA, and to compare the outcomes of these pregnancies with those of teenage and emerging adult pregnancies not complicated by diabetes.
Methods
Study design and population
The Rochester Epidemiology Project (REP) is an electronic infrastructure that allows scientific access to medical records from healthcare providers across southeast Minnesota, including
Following approval from the
Demographic variables
Body mass index (BMI) was abstracted from the patients’ first presentation during the relevant pregnancy. Preconception contraception was based on any prescription, or implant, active within 6 months prior to the first obstetric presentation. Postpartum contraception was defined as any prescription made at or before the participant’s postpartum obstetric appointments in the case of a live birth, or within a 6-week window following a miscarriage or termination. The primary exposure was maternal diabetes. Women were categorized as having “type 1 diabetes” or “type 2 diabetes” or “GDM” based on their documented clinical diagnosis. Most prenatal care for this population was delivered at two institutions:
Outcome variables
Included outcomes were selected by the authors based on variables consistently available in the medical records, previous studies, and relevant core outcome sets.13,18,19,22 Outcome variable definitions were applied consistently throughout the study.
In keeping with local clinical practice, miscarriage was defined as the spontaneous loss of a fetus prior to 20 weeks’ gestation. Stillbirth was defined as pregnancy loss at or after 20 weeks’ gestation. Neonatal death was defined as death in the first 30 days of life. Early preterm birth was defined as delivery prior to 34 + 0 weeks’ gestation. Late preterm birth was defined as delivery between 34 + 0 and 36 + 6 weeks’ gestation.
GDM was diagnosed using a universal two-step approach at 24–28 weeks’ gestation, as outlined by the American Diabetes Association using Carpenter–Coustan thresholds. 10 Gestational hypertension was defined as a systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg on two separate occasions after 20 weeks’ gestation, with prior normal blood pressures. 23 Preeclampsia was defined as new-onset hypertension with proteinuria or, in the absence of proteinuria, new-onset thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema, or headache. 23
Neonates were categorized as small-for-gestational age (<10th percentile at birth) or large-for-gestational age (>90th percentile at birth) based on sex-specific growth charts. 24 Macrosomia was defined as a neonatal birth weight >4000 grams. Hypoglycemia was recorded if dextrose treatment was required within the first 24 h of life. Congenital anomalies were indexed using a joint World Health Organization, Centers for Disease Control and Prevention, and the International Clearinghouse for Birth Defects initial list of congenital anomalies. 25 Shoulder dystocia and jaundice were recorded based on clinical diagnosis following medical record review. Breastfeeding was recorded if patients reported breastfeeding at their initial postpartum visit. In patients with pregestational diabetes, preconception HbA1c was defined as the most recent HbA1c measured within 3 months of initial obstetric presentation.
Statistical analyses
Data were analyzed using BlueSky (Version 10.3.4; BlueSky Statistics, Chicago, IL, USA). Comparisons between groups were evaluated using the chi-square or Fisher’s exact test, as appropriate, for categorical variables. Comparisons between groups for continuous variables were evaluated using the Kruskal–Wallis and Mann–Whitney U tests (as the relevant variables were not normally distributed). Multivariable logistic regression was used to determine the relationship between maternal diabetes (yes/no) and binary clinically relevant adverse outcomes (preeclampsia, cesarean delivery, preterm delivery, neonatal hospitalization, neonatal hypoglycemia, macrosomia, and large-for-gestational age). Variables used as predictors in the regression analysis (maternal age, maternal BMI category, and gestational age) were selected based on known relationships between maternal diabetes/adverse outcomes. Results were deemed statistically significant at P < 0.05.
Results
A total of 1491 confirmed pregnancies were identified in 1379 individuals. The cohort had an age range of 13–21 years, a median age of 19.9 years, and a median BMI of 25.6 [interquartile range (IQR) 8.6] kg/m2 at the first prenatal presentation. Diabetes was present in 68 (4.6%) pregnancies. Type 1 diabetes was present in 10 (0.7%) pregnancies, type 2 diabetes in 7 (0.5%) pregnancies, and GDM in 51 (3.4%) pregnancies.
Maternal characteristics and pregnancy outcomes for pregnancies with GDM, pregestational diabetes, and without diabetes are presented in Table 1 (with between-group analyses presented in Supplementary Table S1). Maternal age and BMI were different between groups (P < 0.001, Table 1). Women with diabetes (both pregestational and GDM) were older than women without diabetes [pregestational: 21.2 (2.0) vs. no diabetes 19.9 (2.3) years, P = 0.02; GDM: 20.9 (1.3) vs. no diabetes 19.9 (2.3) years, P = 0.001]. Women with GDM had a higher BMI compared to those without diabetes [30.3 (9.2) vs. 25.5 (8.3) kg/m2, P < 0.001]. Live birth rates were different between all groups and lowest in those with pregestational diabetes (GDM: 98.0% vs. pregestational: 58.8%, no diabetes: 84.7%; P < 0.001).
Maternal Demographics and Pregnancy Outcomes for Included Pregnancies

Data are presented as median (interquartile range) or n (%).
BMI, body mass index.
Maternal and neonatal outcomes for pregnancies delivered after 20 weeks’ gestation are presented in Table 2 (with between-group analyses presented in Supplementary Table S2). There were significant differences between groups in the rate of cesarean delivery (P < 0.001), gestational age at delivery (P < 0.001), and late preterm birth (P < 0.001). Compared to pregnancies not complicated by diabetes, those with GDM had a higher rate of cesarean delivery (29.4% vs. 17.0%; P = 0.02), delivered at an earlier gestational age (39.0 (2.3) vs. 39.6 (1.9) weeks; P < 0.001), and had a higher frequency of late preterm birth (21.6% vs. 7.3%; P < 0.001). Pregnancies affected by pregestational diabetes also had a higher frequency of cesarean delivery (60.0% vs. 17.0%; P < 0.001), delivered at an earlier gestational age [37.1 (2.1) vs. 39.6 (1.9) weeks; P = 0.003)], and had a higher frequency of late preterm birth (30.0% vs. 7.3%; P = 0.04). The frequency of gestational hypertension and preeclampsia differed between groups (P < 0.001). Compared to pregnancies without diabetes, pregnancies with pregestational (40.0% vs. 11.4%; P = 0.005) and GDM (23.5% vs. 11.4%; P = 0.009) had higher occurrence of gestational hypertension. Similarly, preeclampsia was more frequent in pregnancies with pregestational (40.0% vs. 7.3%; P < 0.001) and GDM (15.7% vs. 7.3%; P = 0.03) compared to pregnancies without diabetes. While absolute birth weight did not differ between groups (P = 0.54, Table 2), the frequency of large-for-gestational age was different between all groups (GDM 13.7% vs. pregestational 50.0% vs. no diabetes 5.8%; P < 0.001). Infants born to women with diabetes had higher rates of neonatal hypoglycemia (P < 0.001). Specifically, compared to infants born to women without diabetes, those born to women with both GDM (42.6% vs. 13.3%; P < 0.001) and pregestational diabetes (60.0% vs. 13.3%; P < 0.001) had higher rates of hypoglycemia. Admission to the neonatal intensive care unit was higher in neonates born to women with GDM compared to those without diabetes (14.9% vs. 6.2%; P = 0.02).
Maternal and Neonatal Outcomes for Pregnancies After 20 Weeks’ Gestation
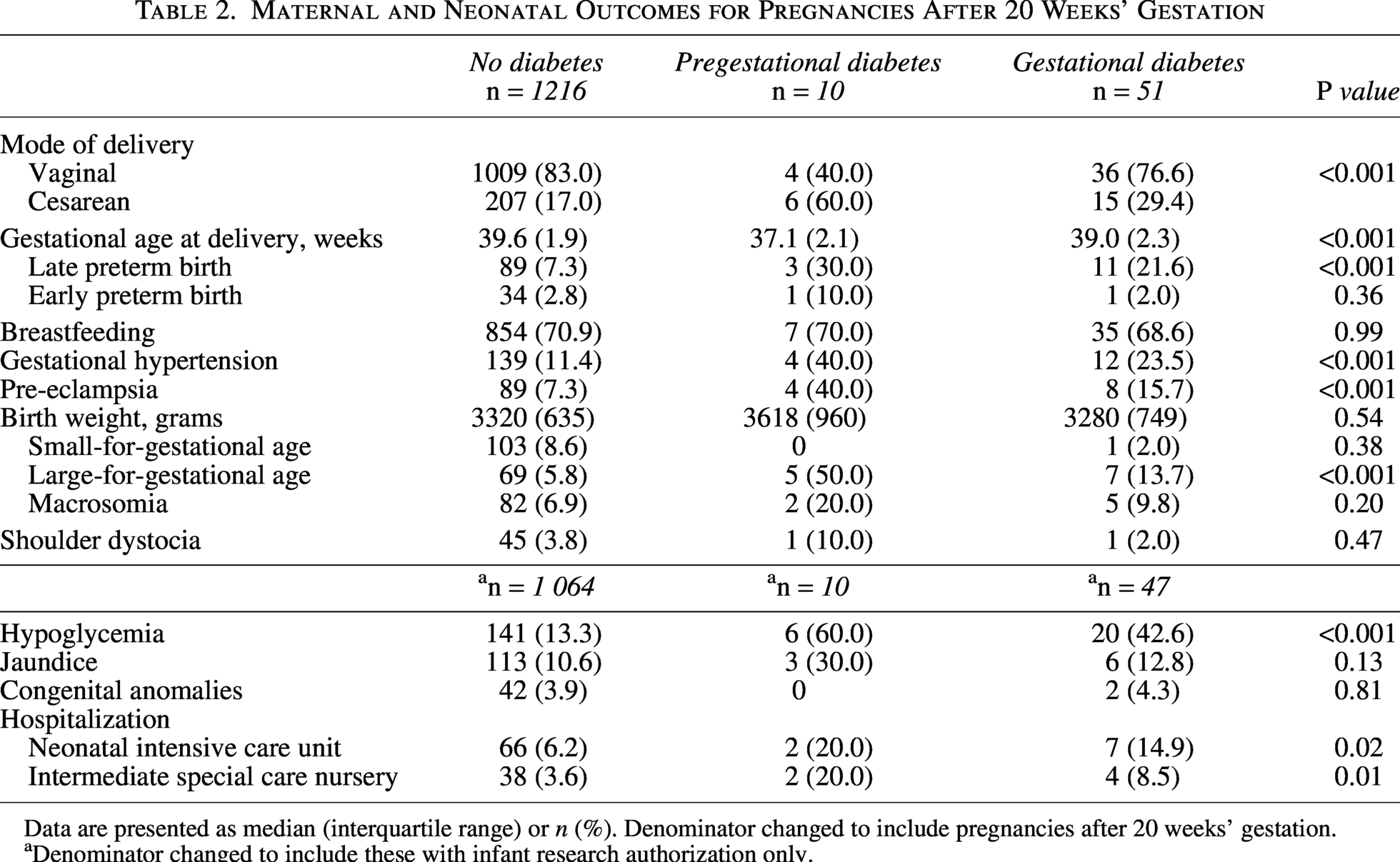
Data are presented as median (interquartile range) or n (%). Denominator changed to include pregnancies after 20 weeks’ gestation.
Denominator changed to include these with infant research authorization only.
Women with pregestational diabetes had increased rates of large-for-gestational-age neonates compared to women with GDM (50.0% vs. 13.7%, P = 0.02). The mean pre-pregnancy HbA1c for patients with pregestational diabetes was 77 ± 11 mmol/mol, range 39–119 mmol/mol (9.2 ± 3.2%; range 5.7%–13.0%).
Data pertaining to GDM screening, treatment, and postpartum follow-up are outlined in Table 3. Of the patients who did not have pregestational diabetes mellitus, 91.1% (1148/1260) completed their 50 gram oral glucose challenge test. In patients diagnosed with GDM, 60.8% were diet-controlled, and 39.2% were managed with medications (17.6% glyburide, 15.7% insulin, and 5.9% metformin). Overall, 27.5% (14/51) completed the 75 gram postpartum oral glucose tolerance test (OGTT); among these patients, four (28.6%) were diagnosed with prediabetes based on their results.
Gestational Diabetes Mellitus Screening and Management of Pregnancies After 20 Weeks’ Gestation
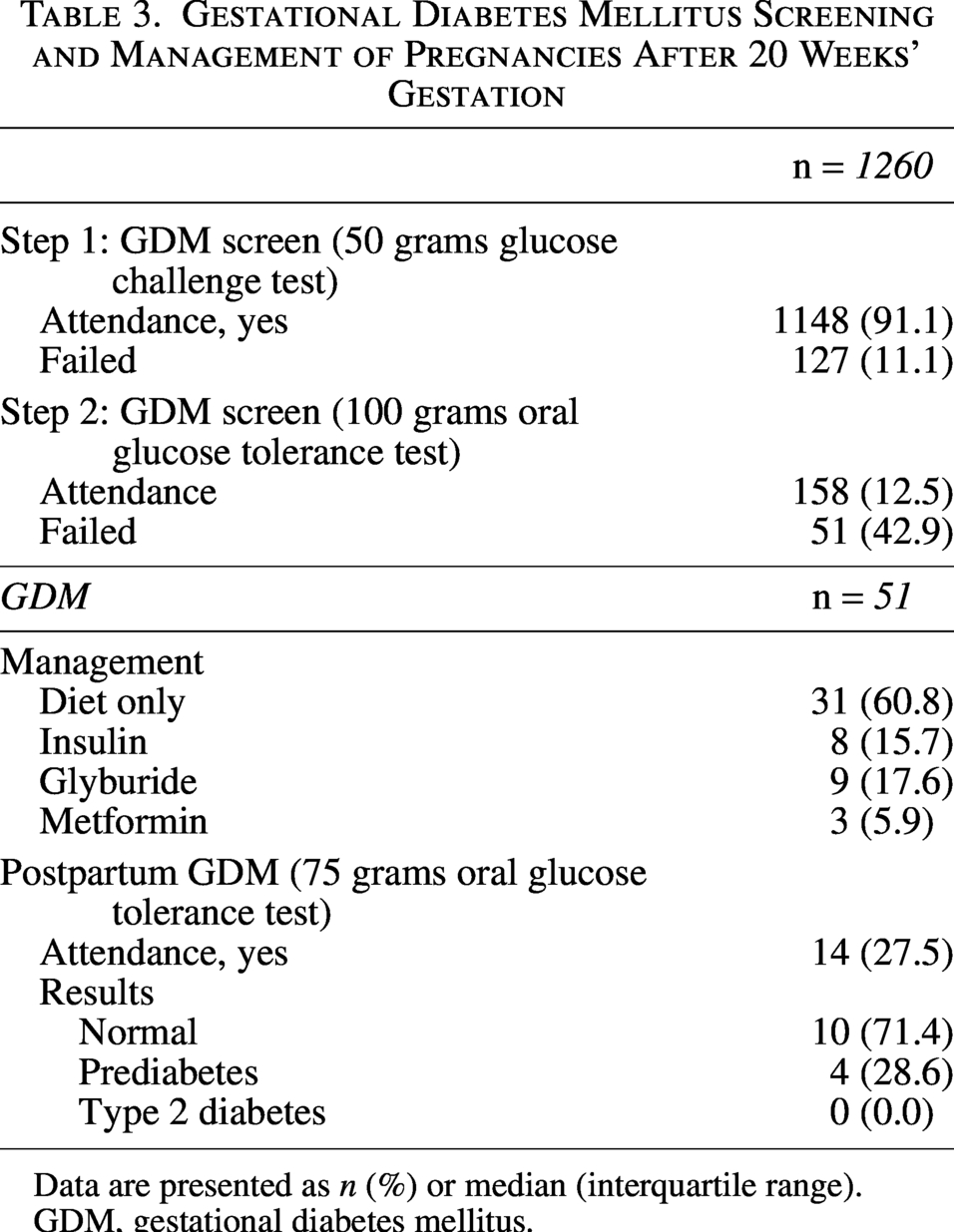
Data are presented as n (%) or median (interquartile range).
GDM, gestational diabetes mellitus.
In an adjusted model, a diabetes diagnosis (pregestational or GDM) was associated with an increased risk of preeclampsia [odds ratio (OR) = 2.79, 95% confidence interval (CI): 1.36–5.34, P = 0.003], cesarean delivery (OR = 2.30; 95% CI: 1.29–3.99, P = 0.004), and preterm delivery (OR = 3.23, 95% CI: 1.65–5.97, P < 0.001) (Table 4). Similarly, neonates born to mothers with diabetes were at increased risk of neonatal hypoglycemia (OR = 4.31; 95% CI: 2.41–7.64, P < 0.001) and large-for-gestational age (OR = 3.92; 95% CI: 1.90–7.57) (Table 4).
Logistic Regression for Adverse Outcome Risk with a Diabetes Diagnosis

Adjusted for maternal age and BMI.
Adjusted for maternal age, BMI, and gestational age at delivery.
BMI, body mass index; CI, confidence interval.
Discussion
Diabetes complicates 4.6% of teenage and emerging adult pregnancies in Olmsted County, Minnesota, USA. This includes pregestational diabetes, which affects 1.2% of this population, and GDM, which affects 3.4%. Teenage and emerging adult pregnancies affected by diabetes had higher BMI and maternal age at the establishment of their antenatal care compared to those without diabetes. They also had an increased risk for multiple adverse maternal and neonatal outcomes including cesarean delivery, late preterm birth, gestational hypertension, preeclampsia, large-for-gestational-age neonates, neonatal hypoglycemia, and neonatal hospitalization.
Our rates of pregestational type 1 and type 2 diabetes are consistent with prior studies in this field.13,18,19 Within our population of patients without pregestational diabetes, systematic early pregnancy screening for undiagnosed diabetes using HbA1c or fasting glucose was not performed. This reflects local institutional guidelines, which recommend selective screening for at-risk patients, as well as the fact that many patients presented for their first prenatal visit in the second trimester of pregnancy. Despite this, although the observed population had over 90% adherence to GDM screening with a glucose challenge test, we observed a relatively low rate of GDM at 3.4% compared to 8.5% within the general pregnant population in Minnesota, 26 suggesting that age may be a protective factor. These findings are inconsistent with prior work in a cohort of New York City adolescents and young adults, which reported a preconception prediabetes prevalence of 20.2% with a GDM incidence of 6.6%. 20 They are also inconsistent with a study using a dataset from the National Health and Nutritional Examination Survey, which reported that in a sample of US teenagers, 29% had prediabetes or diabetes. 27 This discrepancy is likely due to the majority of patients in the referenced studies being Hispanic or Black and therefore having a higher background risk of glucose intolerance 28 compared to the predominantly non-Hispanic White population of Olmsted County, Minnesota, USA. It is also noteworthy that only 27.5% of our patients with GDM completed a postpartum OGTT, and of those, 28.6% were diagnosed with prediabetes. This compares to a completion rate of 40.9% in a prior study examining our entire population with GDM. 29 This limits our understanding of the metabolic sequelae of GDM in teens and emerging adults and illustrates a need for effective strategies to identify and overcome unique barriers to attendance at postpartum glucose testing among women of younger age.
There was evidence of poor pregnancy preparation within our entire study population, and this was more pronounced among those with diabetes. For example, regardless of the presence of diabetes, there were high rates of smoking, recreational drug use, depression, and elevated BMI. These factors can increase the risk for unplanned pregnancies, GDM diagnosis, and other adverse pregnancy outcomes.30,31 In those with pregestational diabetes, the association between a high preconception HbA1c and adverse pregnancy outcomes is well established. 32 In order to minimize this risk, a glycemic threshold of HbA1c <48 mmol/mol (6.5%), and a consideration for prescription contraceptives from puberty, has been recommended by the American Diabetes Association.10,33 However, in our cohort, only 52.9% of teens and emerging adults with pregestational diabetes were prescribed contraceptive prior to conception, and only 11.8% had a preconception HbA1c below 48 mmol/mol (6.5%). This highlights the importance of reproductive and contraceptive counseling and potential missed opportunities for education and interventions to improve future health and pregnancy outcomes.
Several adverse pregnancy outcomes were higher in our teenage and emerging adults with diabetes in pregnancy compared to their counterparts without diabetes. This illustrates the additive adverse effect of diabetes in addition to the baseline risk conferred by their young age. Furthermore, in our study, teenage and emerging adults without diabetes experienced significantly higher rates of preeclampsia (7.3% vs. 3.3%) and gestational hypertension (11.4% vs. 3.0%) compared to a prior study in Olmsted County that included pregnant individuals of all ages.
34
Compounding these risks is a diabetes diagnosis, which was associated with a further increased risk of hypertensive disorders of pregnancy within our study. Among the subset with GDM in our study, we observed a higher prevalence of hypertensive disorders of pregnancy compared to a cohort of women with GDM seen at
Strengths of this study include its population-based design and the use of a comprehensive medical record linkage system for initial electronic identification of the cohort, followed by manual abstraction of detailed, participant-level variables with cross-checking of all data for accuracy. This approach provides us with granular data on each subject with <5% missing data across most endpoints collected, which would not be possible with higher-level surveillance databases. However, our study also has limitations. Due to the retrospective, observational design, confounding may affect our results. While the study contains all identified, eligible participants, subjects without Minnesota research authorization were not retrieved in the initial search. However, according to previous studies, 98% of individuals gave authorization to use their data for research. 21 Our overall number of cases with diabetes is limited, which is an important finding from an epidemiological standpoint, but precludes detailed outcome analyses according to diabetes subcategory or adjustment for factors such as glycemic control during pregnancy. Because of this smaller number of cases, our ability to detect differences in rarer outcomes is limited, and the wider confidence intervals around adjusted odds ratios indicate reduced precision of the estimates. Some patients had multiple pregnancies during the study period, and as such, independence of observation is likely impacted. Furthermore, while the racial and ethnic characteristics of residents of Olmsted County are like those of individuals from the state of Minnesota and the Upper Midwest, USA, Olmsted County is less racially and ethnically diverse, and more highly educated than the overall U.S. population. 21 This limits the external validity of the study but may be addressed in future multicenter studies comparing our findings to those of more diverse populations. Finally, while we provide detailed information on common mental health disorders and social history, we do not have details on lifestyle factors, dietary habits, and socioeconomic status, all of which may contribute to diabetes prevalence in this age group and help us understand how to better prevent GDM and postpartum type 2 diabetes in this population.
These data define our prevalence of pregestational diabetes and GDM in teenage and emerging adult pregnancies and demonstrate that the presence of diabetes is associated with a higher risk of adverse outcomes in this already vulnerable group. These teenagers and young adults may benefit from tailored preconception and obstetric care to reach optimal glycemic targets and minimize the risk of adverse events. Future research should evaluate interventions aimed at supporting this at-risk population before, during, and after pregnancy.
Authors’ Contributions
H.E.C. and A.M.E. contributed to study design, collected, synthesized, and interpreted data and drafted the article. A.Z., S.M., and L.P-.E. contributed to data collection and interpretation. K.A.P., K.C., A.V., and A.L.C. contributed to study design and data interpretation. All authors critically reviewed and approved the final article.
Footnotes
Acknowledgments
The authors thank Barbara A. Abbott and colleagues of the Rochester Epidemiology Project, Mayo Clinic, Rochester, Minnesota, USA, for their assistance in identifying the cohort.
Data Availability
Anonymized data are available upon reasonable request and following research protocol approval.
Author Disclosure Statement
Dr. A.V. reported receiving grants from Novo Nordisk and personal fees from the Rezolute Advisory Board (and Boehringer-Ingelheim), outside the submitted work.
Funding Information
This research was supported by the Rochester Epidemiology Project Scholarship Program (H.E.C.), the National Institutes of Health USA under award numbers DK092721 and DK134767 (A.M.E.), the Mayo Clinic Robert and Elizabeth Strickland Career Development Award in Endocrinology, Metabolism, Diabetes and Nutrition (A.M.E.), and the National Institutes of Health USA under award numbers DK78646, DK116231, and DK126206 (A.V.). The research was completed using the Rochester Epidemiology Project medical record linkage system, which is supported by the National Institute on Aging of the National Institutes of Health under award numbers AG034676 and AG052425. This publication was supported through consultation with the Biostatistics, Epidemiology, and Research Design resource of Mayo Clinic’s Center for Clinical and Translational Science. Funding for the consultation came from grant number UL1 TR002377 from the National Center for Advancing Translational Sciences. The contents of this article and the views expressed are those of the authors and not necessarily reflect those of the study funders.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.