
Abstract
Background:
Diabetes mellitus (DM) is a globally growing chronic disease and is associated with numerous complications. In recent years, its potential impact on cognitive functions has gained increasing attention. This study was conducted to investigate the relationship between cognitive performance and micronutrient status in non-geriatric individuals with type 2 DM (T2DM).
Material and Methods:
This case–control study included 120 patients with T2DM aged 18–65 years. Patients with cognitive impairment constituted the case group, while age-matched patients without cognitive impairment served as controls, based on Montreal Cognitive Assessment scores. Individuals with malabsorption syndromes, severe acute or chronic illnesses, prior gastrointestinal surgery, dementia, Parkinson’s disease, cerebrovascular events, psychiatric disorders, use of cognition-affecting medications, or micronutrient supplementation were excluded. Fasting blood glucose (FBG), HbA1c, renal and liver function tests, total protein, albumin, iron, zinc, magnesium, calcium, vitamin B12, folate, and vitamins A, C, D, and E were measured and compared between groups.
Results:
75 females and 45 males, a total of 120 patients were included in the study. The mean age was 53.0 ± 8.4 years. Cognitive dysfunction was present in 50% of the patients. There were no statistically significant differences in the levels of FBG, HbA1c, urea, creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total protein, folic acid, vitamin A, vitamin C, vitamin E according to age, gender, and cognitive dysfunction variables. Albumin, iron, zinc, magnesium, calcium, vitamin B12, vitamin D levels were significantly lower in the group with cognitive dysfunction than in the group without cognitive dysfunction. Albumin, iron, zinc, magnesium, calcium, vitamin B12, vitamin D levels in univariate model and iron, magnesium, calcium, vitamin B12 levels in multivariate model were effective in differentiating patients with and without cognitive dysfunction.
Conclusion:
This study shows that there is a significant relationship between cognitive functions and micronutrient levels in non-geriatric patients with DM. Screening of micronutrient levels and appropriate replacement of deficiencies during diabetes management is important for the protection and improvement of cognitive functions.
Introduction
Micronutrient deficiencies can significantly affect both physical and mental health throughout the lifespan, in healthy individuals as well as those with chronic diseases. 1 Type 2 diabetes mellitus (T2DM) is characterized by significant losses of key micronutrients due to the underlying metabolic disturbances and associated complications of the disease. 2
Deficiencies in trace elements such as selenium, zinc, copper, iron, chromium, and iodine have been associated with impaired glucose homeostasis and increased insulin resistance. 3 Similarly, vitamin D deficiency has been linked to decreased insulin secretion, insulin resistance, and the development of T2DM. 4
Cognitive functions can be affected at any age in patients with diabetes through multiple mechanisms, often in a gradual and subtle manner. However, preexisting cognitive impairments tend to progress more rapidly in the geriatric population. 5 Numerous studies have explored the relationship between micronutrient deficiencies and cognitive function.6–10 B-complex vitamins (B1, B2, B3, B5, B6, B8, B9, and B12), as well as vitamin C, iron, magnesium, and zinc, have been associated with cognitive and psychological processes at both the molecular and cellular levels. 11 Notably, these investigations have predominantly focused on older adults, with limited attention to other age groups, including pediatric populations.
Our study aimed to examine the association between micronutrient, mineral, and vitamin levels and cognitive function in non-geriatric patients with T2DM by comparing these parameters between patients with and without cognitive dysfunction, as assessed using the Montreal Cognitive Assessment (MoCA).
Material and Methods
Data collection
This study is a case–control study. The case group consisted of diabetic patients aged 18–65 with cognitive impairment, while the control group consisted of age-matched diabetic patients without cognitive impairment. This study was conducted at Istanbul Training and Research Hospital, in accordance with national regulations and institutional guidelines. The study adhered to the principles of Good Clinical Practice and Declaration of Helsinki, and patient confidentiality and privacy were strictly maintained. The protocol for this study was approved by the Ethical Committee of University of Health Sciences Turkey, İstanbul Training and Research Hospital (approval number: 341, date: November 11, 2022).
A total of 120 patients, aged 18–65 years, who were admitted to the internal medicine and diabetes outpatient clinics and who met the inclusion and exclusion criteria were enrolled in the study.
Age between 18 and 65 years Confirmed diagnosis of T2DM No history of malabsorption syndromes (inflammatory bowel disease, celiac disease, pernicious anemia, Zollinger–Ellison syndrome, or chronic pancreatitis) No acute or severe chronic illness (including malignancy, end-stage liver cirrhosis, end-stage renal disease, or severe infection) No history of gastrointestinal surgery
Age <18 years or >65 years Diagnosis of dementia or Parkinson’s disease History of cerebrovascular accident Presence of any diagnosed psychiatric disorder Use of medications known to affect cognitive function Use of supplements containing the micronutrients investigated in the study
Clinical and laboratory data were obtained from patient files, the hospital information management system, and the Ministry of Health’s MEDULLA system. Patients were categorized into two groups based on cognitive function status (normal vs. impaired), and comparisons were made in terms of micronutrient levels between these groups.
Biochemical and micronutrient analysis
After an overnight fast of at least 12 h, venous blood samples were collected from all participants in the morning. Fasting conditions were applied primarily for the assessment of fasting glucose and selected trace elements; however, uniform preanalytical conditions were maintained for all laboratory parameters to ensure consistency across measurements. Participants were allowed to drink water during the fasting period. The following laboratory parameters were assessed: fasting blood glucose (FBG), hemoglobin A1c (HbA1c), urea, creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total protein, albumin, iron, zinc, magnesium, calcium, vitamin B12, folic acid, and vitamins A, C, D, and E.
For the interpretation of laboratory results, reference intervals recommended by the assay manufacturers were applied. The reference intervals were as follows: FBG, 82–115 mg/dL; urea, 21–43 mg/dL; creatinine, 0.50–0.90 mg/dL; AST, 0–32 U/L; ALT, 0–33 U/L; total protein, 64–83g/L; albumin, 35–52g/L; iron, 37–145 µg/dL; zinc, 70–114 µg/dL; magnesium, 1.6–2.4 mg/dL; calcium, 8.8–10.2 mg/dL; vitamin B12, 197–771 ng/L; folic acid, 3.89–26.8 µg/L; vitamin A (retinol), 300–1000 ng/mL; vitamin E (α-tocopherol), 5.5–18 µg/mL; and vitamin C (ascorbic acid), 4–20 mg/L. Glycated hemoglobin (HbA1c) results were interpreted according to established clinical decision limits: <5.7% (normal), 5.7–6.4% (prediabetes), and ≥6.5% (diabetes). Vitamin D status was defined based on laboratory reference limits as follows: deficiency, <12 µg/L; insufficiency, 12–20 µg/L; and sufficiency, >20 µg/L. All reference intervals and decision limits were specific to the analytical methods and instrumentation used in this study.
All analyses were performed using an automated clinical chemistry analyzer operated, calibrated, and maintained in accordance with the manufacturer’s instructions using original Beckman Coulter® reagents and materials. Internal quality control was conducted daily for all analytical parameters using two-level control materials (low and high) supplied by the manufacturer. Analytical stability was continuously monitored and evaluated according to Westgard rules, and external quality assessment schemes were applied to verify analytical accuracy. Throughout the study period, both internal and external quality control results consistently fulfilled the predefined desirable analytical performance specifications
HbA1c was measured using high-performance liquid chromatography (HPLC)-based cation exchange chromatography on the ADAMS HA-8180V analyzer (Arkray Inc., Japan) using whole blood samples collected in K3-EDTA–containing Sarstedt S-Monovette® tubes (Lot No. 3032622). Biochemical analyses were performed on serum samples obtained from gel-containing Sarstedt S-Monovette® tubes (Lot No. 3033021). Serum glucose, urea, creatinine, AST, ALT, iron, and calcium levels were measured using photometric methods on the Roche Cobas 8000 analyzer (Roche Diagnostics Ltd., Switzerland). Total protein and albumin concentrations were determined by colorimetric assays on the same platform. Vitamin B12 and folic acid levels were measured using electrochemiluminescence immunoassay, while vitamin D was assessed by chemiluminescence immunoassay, both on the Roche Cobas 8000 system. Vitamins A and E were analyzed by HPLC using a Shimadzu analytical system (Shimadzu Corporation, Kyoto, Japan). Vitamin C concentrations were determined using a microplate-based photometric method on the SYNERGY HT analyzer (BioTek Instruments, USA). Serum zinc levels were measured photometrically on the Roche Cobas 8000 analyzer using blood samples collected in trace-element Sarstedt S-Monovette® tubes containing lithium heparin (Lot No. 3030821).
Evaluation of cognitive function
Cognitive function was evaluated using the MoCA tool. Patients scoring ≥21 points were classified as cognitively normal, while those scoring <21 points were considered to have cognitive impairment.
Statistical analysis
The sample size was calculated using a standard power analysis formula for categorical data. Assuming a 5% margin of error, 80% statistical power, and a standard effect size of 0.63, it was determined that a minimum of 40 participants per group would be sufficient. Mean, standard deviation, median, minimum, maximum value frequency and percentage were used for descriptive statistics. The distribution of variables was checked with Kolmogorov–Simirnov test. Mann–Whitney U test were used for the comparison of quantitative data. Chi-square test was used for the comparison of the comparison of qualitative data. The effect level was tested with logistic regression (Univariate and Multivariate Model). All variables were included in the univariate logistic regression model. In the multivariate logistic regression model, only the variables with P < 0.05 in the univariate model were included. The multivariate model was evaluated using the Forward LR method, and the independent variables were identified. SPSS 22.0 was used for statistical analyses.
Results
A total of 120 patients were included in the study, comprising 75 women (62.5%) and 45 men (37.5%). The mean age of the participants was 53.0 ± 8.4 years.
Patients were divided into two groups of 60 individuals each, based on the presence or absence of cognitive impairment. The results of laboratory parameters of these two groups are summarized in Table 1.
Comparison of Laboratory Parameters of Case and Control Groups
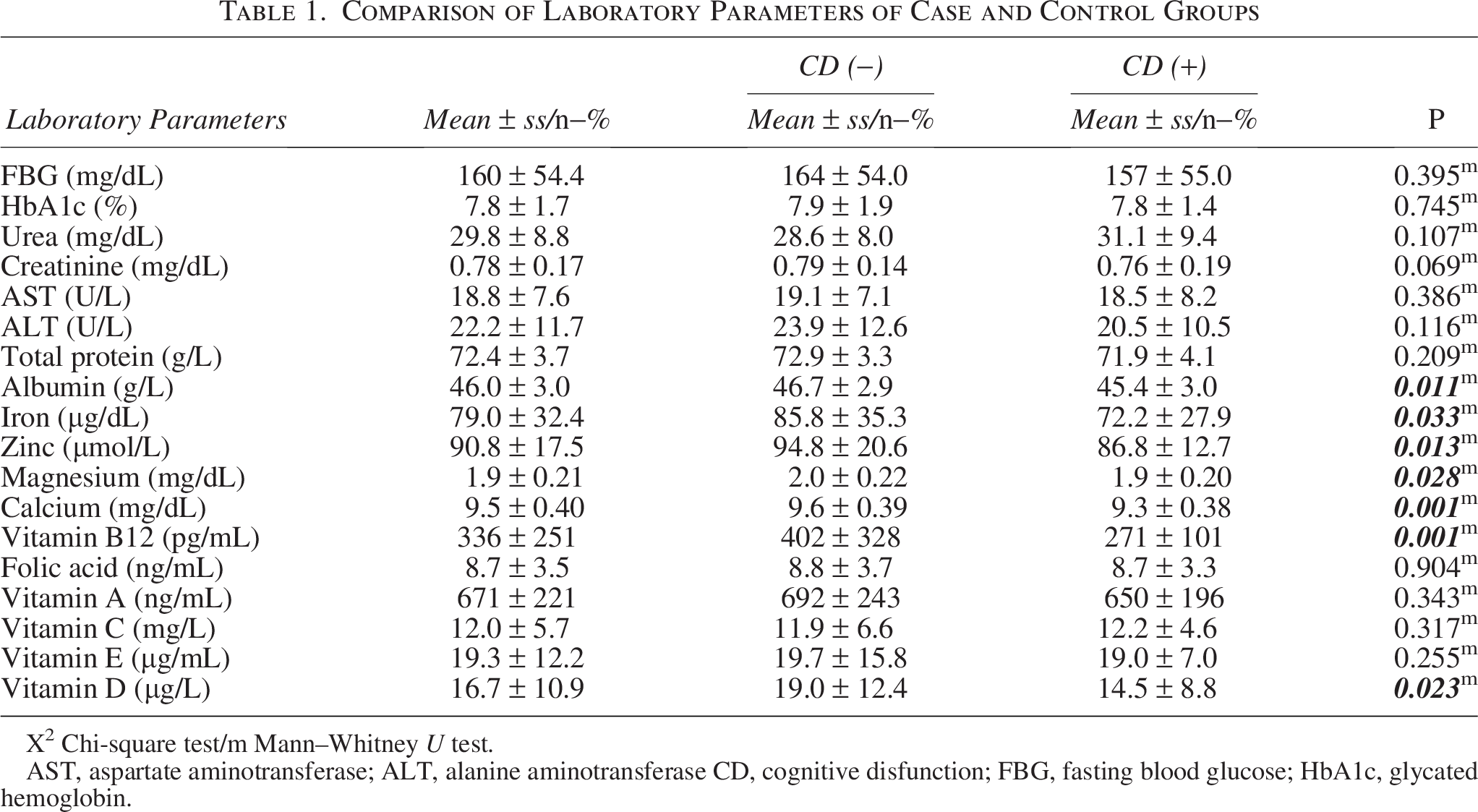
X² Chi-square test/m Mann–Whitney U test.
AST, aspartate aminotransferase; ALT, alanine aminotransferase CD, cognitive disfunction; FBG, fasting blood glucose; HbA1c, glycated hemoglobin.
There were no statistically significant differences between the groups with and without cognitive impairment in terms of age (P > 0.05), gender distribution (P > 0.05), or the levels of FPG, HbA1c, urea, creatinine, AST, ALT, total protein, folic acid, vitamin A, vitamin C, and vitamin E (P > 0.05) (Table 1).
In the group with cognitive impairment, the levels of albumin, iron, zinc, magnesium, calcium, vitamin B12, and vitamin D were significantly lower compared to the group without cognitive impairment (P < 0.05) (Table 1).
In the univariate model, age, gender, HbA1c, fasting plasma glucose, urea, creatinine, AST, ALT, total protein, folic acid, vitamin A, vitamin C, and vitamin E were not found to have a statistically significant effect (P > 0.05) in distinguishing patients with and without cognitive impairment. However, albumin, iron, zinc, magnesium, calcium, vitamin B12, and vitamin D levels showed a significant effect (P < 0.05) in differentiating between the two groups in the univariate model (Table 2).
Evaluation of Patients with Variable Model
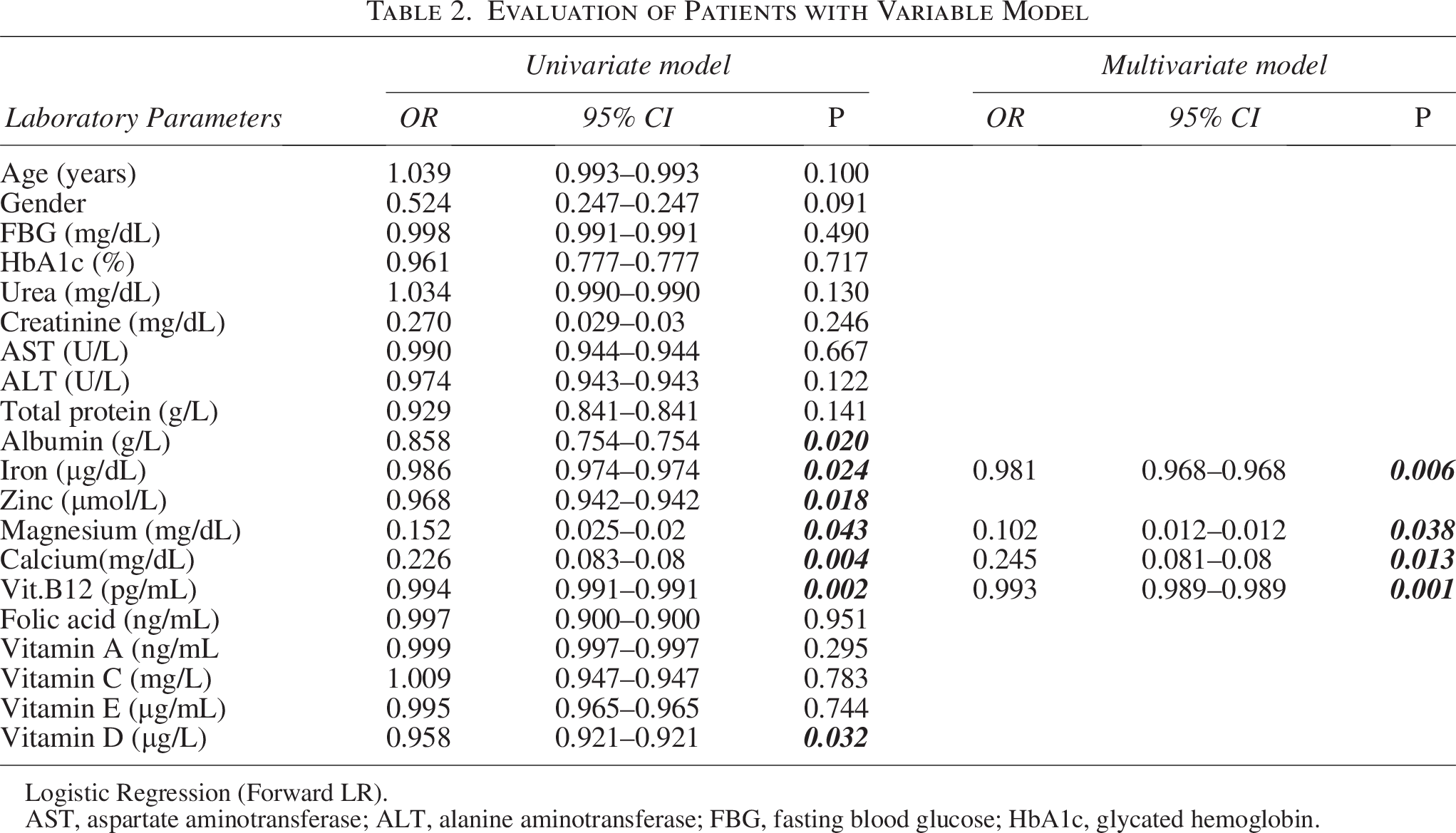
Logistic Regression (Forward LR).
AST, aspartate aminotransferase; ALT, alanine aminotransferase; FBG, fasting blood glucose; HbA1c, glycated hemoglobin.
In the multivariate reduced model, iron, magnesium, calcium, and vitamin B12 levels were found to have a statistically significant and independent effect (P < 0.05) in distinguishing patients with and without cognitive impairment (Table 2).
Discussion
T2DM has become a global pandemic, with an expected worldwide prevalence of approximately 366 million individuals by 2030. 12 Beyond its well-established microvascular and macrovascular complications, T2DM has also been associated with an increased risk of cognitive impairment.13,14 Studies have reported that individuals with diabetes are up to 2.5 times more likely to develop dementia compared to individuals without diabetes.15,16 Cognitive decline related to diabetes has become a substantial burden on healthcare systems and economies, particularly in aging societies such as Japan. 17
Although hyperglycemia and insulin resistance are thought to be key contributors to this relationship, 18 the evidence remains mixed. Some studies suggest that chronic hyperglycemia, through mechanisms involving oxidative stress and the accumulation of advanced glycation end products, may contribute to neurovascular damage and impaired cognition. 19 In contrast, other research has found minimal or no association between hyperglycemia and cognitive dysfunction in T2DM. 20 In our study, cognitive impairment was identified in 50% of the patients with T2DM, underscoring the need for early screening and intervention.
Sebastian et al. emphasized the cerebral reliance on glucose and described how abnormalities in glucose metabolism can affect multiple domains of cognition and executive function. Diabetes may impair cognition via cerebrovascular hypoperfusion, alterations in glucose transport, regional brain hypometabolism, or recurrent hypoglycemia induced by pharmacotherapy. Furthermore, cognitive decline in patients with diabetes may compromise self-management of the disease itself. 21 Similar findings were echoed in a meta-analysis by Sharma et al., who identified cognitive decline as a modifiable risk factor in the early stages of disease progression, including dementia and Alzheimer’s disease. Lifestyle factors, such as poor diet, sedentary behavior, and alcohol consumption, have also been shown to contribute to cognitive deficits in individuals with diabetes. 22
Our study supports these findings and further identifies micronutrient deficiencies specifically albumin, iron, zinc, magnesium, calcium, vitamin B12, and vitamin D as potentially modifiable contributors to cognitive impairment in non-geriatric T2DM patients. In our multivariate model, lower levels of albumin, iron, magnesium, calcium, and vitamin B12 were independently associated with cognitive dysfunction. These findings are consistent with previous research highlighting the link between micronutrient status and neurocognitive performance.23–25
Although glucose and HbA1c are critical markers in the management of diabetes, our study did not observe a statistically significant association between these parameters and cognitive function. This may be attributable to the relatively limited sample size, as previously noted in the literature.26–28 However, earlier studies have reported a dose-dependent relationship between elevated glucose levels and dementia risk, even among individuals without diabetes.28–30
Vitamin D has received considerable attention due to its neuroprotective properties. Its receptors are widely expressed in the central nervous system, and it is believed to modulate neurogenesis, calcium signaling, and the expression of neurotrophic factors.31–33 Although some studies did not find a significant association between vitamin D status and cognitive function,34–38 other research including ours has found significantly lower vitamin D levels in cognitively impaired diabetic patients.35,36 The variability in findings across studies may be attributed to differences in population characteristics, genetic background, dietary habits, sun exposure, and socioeconomic factors.39,40
Emerging dietary patterns such as the Mediterranean, DASH, and MIND diets have been associated with improved cognitive outcomes, primarily due to their anti-inflammatory and antioxidant profiles.41–49 Our findings highlight the importance of integrating dietary counseling and micronutrient supplementation in the management of cognitive health in patients with T2DM.
Finally, systemic inflammation, as measured by dietary inflammatory indices and inflammatory biomarkers, has been implicated in the pathogenesis of both diabetes and cognitive impairment.50,51 Magnesium and other anti-inflammatory nutrients may offer dual benefits in glycemic control and neuroprotection.
In line with our findings, previous studies have also identified low serum albumin as a risk factor for mild cognitive impairment, particularly in elderly populations. 51 In our younger diabetes mellitus cohort, lower albumin levels were likewise significantly associated with cognitive decline.
Vitamin B12 plays a key role in maintaining neuronal integrity, and its deficiency has been linked to cognitive deficits. While some studies have found that B12 supplementation may be ineffective in improving cognition in the absence of overt deficiency or neurologic disease, 52 other research suggest that metformin use may contribute to B12 deficiency in patients with diabetes. 53 In our study, we observed significantly lower B12 levels in patients with cognitive impairment, independent of medication use, while folic acid levels were not significantly different between groups.
Trace elements such as zinc and iron are essential for cognitive function. Zinc deficiency has been shown to impair antioxidant defense, promote oxidative stress, and contribute to neurodegenerative processes. 54 Similarly, iron deficiency, especially in pediatric populations with diabetes, has been associated with reduced non-verbal intelligence scores. 55 Our findings support the role of these deficiencies in cognitive impairment, even in non-geriatric adults with diabetes.
Magnesium, an essential mineral for neuronal activity, has demonstrated potential cognitive benefits in interventional studies, particularly when administered as magnesium L-threonate. 56 Our results also indicate significantly lower magnesium levels in cognitively impaired diabetic patients. Although our result is statistically significant, the absolute difference is small, indicating a subtle effect. This finding might indicate an association rather than causation, and residual confounding or unmeasured factors may contribute. Nevertheless, the results indicate that magnesium supplementation may have a potential role in this population.
Calcium has been linked to cognitive function in elderly populations, and our findings extend this association to younger individuals with diabetes. 57 On the other hand, we did not observe significant differences in vitamins A, C, and E levels between cognitively impaired and unimpaired groups, consistent with previous studies indicating inconclusive or weak associations. 58
Although the overall findings are favorable, the nature and severity of cognitive impairment in individuals with diabetes are likely influenced by diabetes duration and the level of glycemic control. Previous studies have shown that individuals with worse cognitive function tend to be older, have lower educational and socioeconomic status, longer diabetes duration, and a higher burden of comorbidities, including depressive symptoms and diabetic complications. 59
In addition, poorer cognitive performance has been associated with advanced age, male sex, nonprivate health insurance, neuropathy, and longer duration of diabetes in both univariate and multivariate analyses. 60 Furthermore, better glycemic control and fewer diabetic complications have been linked to less cognitive impairment. 61 Therefore, the findings should be interpreted cautiously, and future studies that include diabetes duration, metabolic control, and complication burden may help to further clarify their relationship with cognitive outcomes.
Conclusion
This study demonstrates that lower levels of specific micronutrients, minerals, and vitamins are associated with cognitive impairment in non-geriatric patients with T2DM. Among the evaluated parameters, serum albumin, iron, zinc, magnesium, calcium, vitamin B12, and vitamin D levels were significantly lower in patients with cognitive dysfunction, suggesting their potential value as discriminative or associated markers rather than causal factors.
These findings highlight the multifaceted nature of diabetes, which may be accompanied by neurocognitive alterations in addition to metabolic disturbances. Cognitive health represents an important aspect of overall well-being in patients with diabetes and may influence quality of life and daily functioning.
Given the cross-sectional nature of the study, causality cannot be inferred; however, the observed associations suggest that micronutrient status may be a relevant and potentially modifiable factor related to cognitive function in this population. Routine assessment of micronutrient levels, particularly in patients reporting cognitive complaints, may be considered within a holistic approach to diabetes care, while prospective and interventional studies are needed to clarify causal relationships and therapeutic implications.
Study Limitations
Although some findings reached statistical significance, the absolute differences were small, suggesting modest effect sizes. Therefore, these results should be interpreted as associations rather than evidence of causality, as residual confounding or unmeasured factors may have influenced the outcomes. Cognitive function was assessed using a validated international instrument; however, no formal evaluation by a psychiatrist or neurology specialist was performed. Therefore, factors such as intelligence level or educational background may have influenced the test results. Potential confounding factors, such as diabetes duration and glycemic control, were not assessed in this study.
Informed Consent
All included patients provided written informed consent for the publication of their medical details.
Authors’ Contributions
E.C.G.: Conceptualization, design, data collection or processing, analysis or interpretation, literature search, writing, and final review. F.A.: Conceptualization, design, data collection or processing, analysis or interpretation, literature search, writing, and final review. T.A.: Data collection or processing, design, and final review. All authors listed have contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline. To the best of our knowledge, no conflict of interest, financial or other, exists.
Footnotes
Author Disclosure Statement
No conflict of interest was declared by the authors.
Funding Information
The authors declared that this study received no financial support.