
Abstract
Background:
Venous malformations can cause substantial morbidity and long-term complications. There are no Food and Drug Administration (FDA)-approved therapies for the treatment of venous malformations. However, off-label use of sirolimus has demonstrated clinical benefit in these patients. This systematic review evaluates the efficacy and safety of sirolimus in the management of venous malformations.
Methods and Results:
A systematic literature search identified 26 studies comprising 98 patients treated with sirolimus for venous malformations. Most studies were case reports or case series (77%), with 15% prospective trials and 8% retrospective analyses. Sirolimus, primarily administered orally, yielded some level of clinical improvement in 72% of reported patients, with consistent symptomatic relief observed in coagulopathy, bleeding, anemia, pain, and improved function. However, reduction in the size of the malformation varied and treatment-limiting side effects were observed.
Conclusions:
Oral sirolimus is a promising treatment option for venous malformations, especially for those with deep venous malformations. A direct, targeted topical treatment could provide clinical benefit for the cutaneous manifestation without the risk of off-target effects as occur with oral sirolimus. Further prospective, controlled studies are warranted to elucidate sirolimus’s role in managing venous malformations.
Keywords
Introduction
Venous malformations are the most common congenital slow-flow vascular anomaly with an estimated prevalence of 45 cases per 100,000 births. 1 They can result in substantial morbidity and severe long-term complications. Venous malformations typically manifest as collections of ectatic venous channels involving the head, neck, limbs, and trunk, often with a cutaneous manifestation, but lesions may also emerge in portions of the internal viscera including the gastrointestinal tract.2,3 There are no Food and Drug Administration (FDA) approved therapies for venous malformations.
With a highly variable clinical presentation, venous malformations usually manifest as isolated lesions, but may involve regional or multifocal lesions associated with segmental overgrowth syndromes, including blue rubber bleb nevus syndrome and Klippel–Trenaunay syndrome, among others.4,5
Venous malformations present with deformity, bleeding, infection, chronic pain, and functional limits. Interventional treatments—surgery, sclerotherapy, and laser therapy, for instance—may be inadequate, particularly in patients with extensive, cutaneous, or invasive disease, highlighting an unmet clinical need for pharmacologic options.2,6
Recent advances in our understanding of the pathogenesis of venous malformations have implicated abnormal activation of the phosphatidylinositol 3-kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin (mTOR) signaling pathway, a critical intercellular pathway that plays a central role in venous malformation expansion and proliferation.6,7 The PI3K/AKT/mTOR signaling pathway overactivation that underlies the pathogenesis of venous malformations mostly results from somatic over activating mutations in Tyrosine Kinase with Immunoglobulin and EGF Homology Domains-2 (TIE2)/TEK gene and from PIK3CA gene hyperactivating variants. In the first murine model of a human venous malformation, researchers induced endothelial cell tyrosine kinase receptor TIE2 mutations in mice. 8 These mutations triggered venous malformations with ectatic blood-filled channels that enlarged over time. Using this model, daily intraperitoneal sirolimus injections over 7 days prevented venous malformation growth and attenuated mutant TIE2-induced signaling. Sirolimus, an mTOR inhibitor, dampens PI3K/AKT/mTOR signaling, thus garnering increasing attention as a potential therapeutic option for venous malformations.7–9 This systematic review examines clinical study findings related to the role of sirolimus in the treatment of children and adults with venous malformations.
Methods
Search strategy
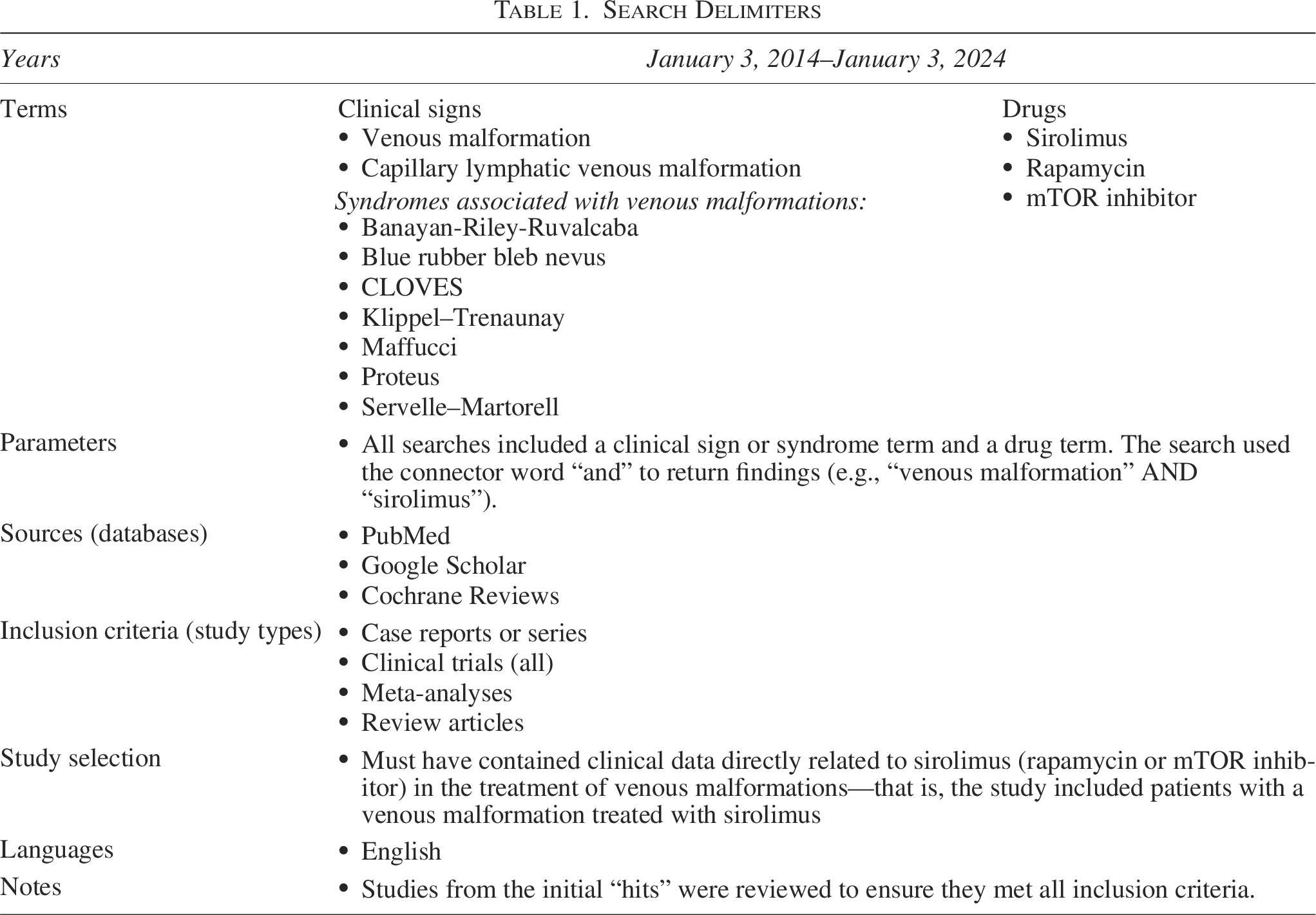
The primary objective of the search was to identify and assess clinical studies published within a 10-year period (January 2014–January 2024), specifically focusing on the role of sirolimus in the treatment of venous malformations. The search was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 10 All studies were assessed to ensure they contained clinical data on patients treated with sirolimus for venous malformations. The search terms included several syndromes commonly associated with the development of venous malformations to maximize the number of patients identified who received sirolimus for venous malformations. 4
Search criteria
All searches included clinical signs and syndromes and a drug term with the connector “AND” (Table 1). For example, the search format was as follows: “venous malformation” AND “sirolimus” OR “rapamycin” OR “mTOR inhibitor.” Only studies published in English with titles and/or abstracts indicating clinical data directly related to sirolimus in the treatment of patients with venous malformations were included.
Search Delimiters
Data extraction
From each relevant study, pertinent details were extracted and compiled into a comprehensive table (Table 2). The extracted information captured study type, demographic characteristics, prior treatments for venous malformation, diagnosis and affected anatomical sites, major symptoms, sirolimus dosing and treatment duration, sirolimus efficacy, and sirolimus-related adverse events (AEs).
Study Summaries
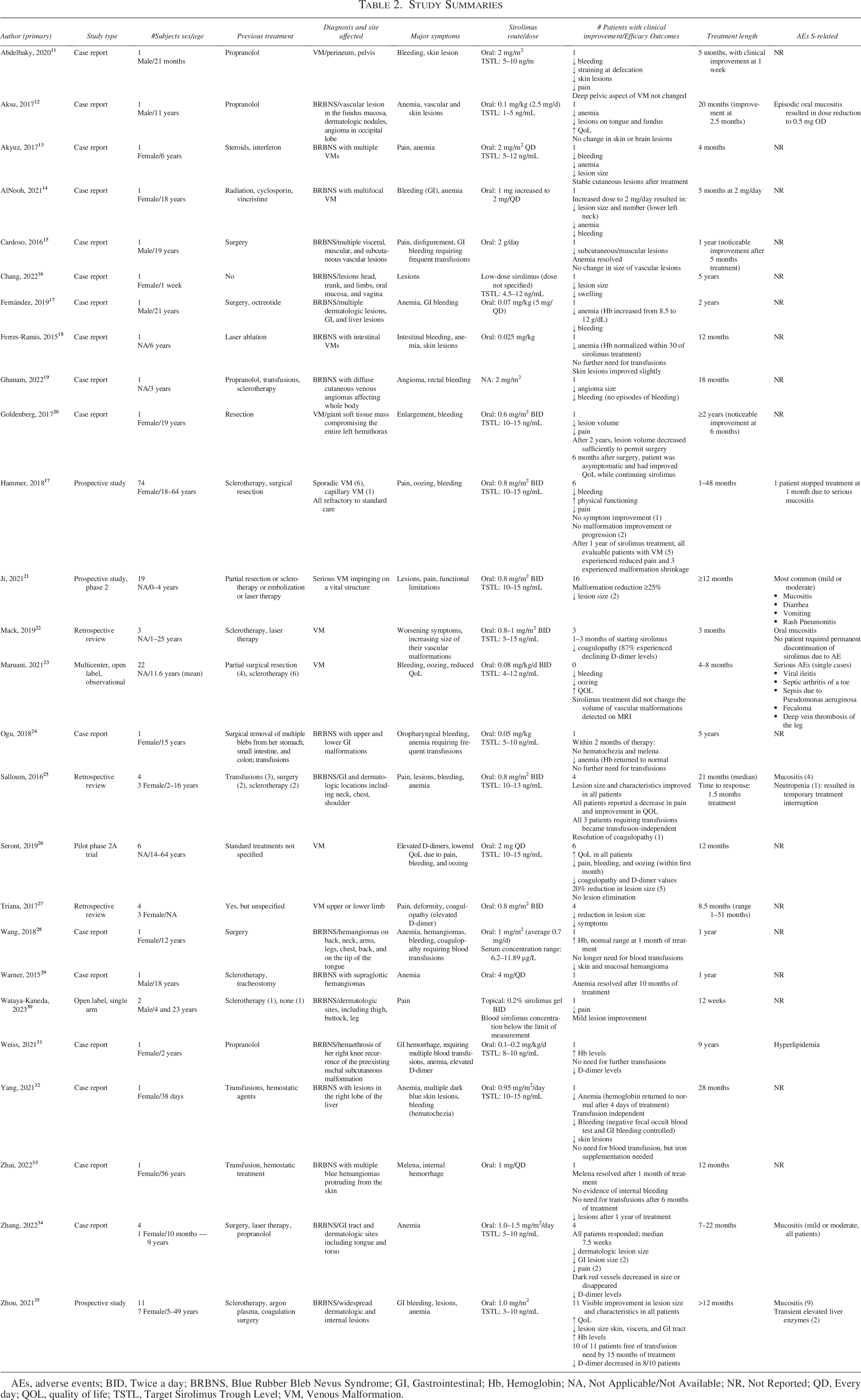
AEs, adverse events; BID, Twice a day; BRBNS, Blue Rubber Bleb Nevus Syndrome; GI, Gastrointestinal; Hb, Hemoglobin; NA, Not Applicable/Not Available; NR, Not Reported; QD, Every day; QOL, quality of life; TSTL, Target Sirolimus Trough Level; VM, Venous Malformation.
Statistical analyses
Given the inherent heterogeneity in outcome measures and subject selection criteria across the studies, formal statistical analyses were not conducted. Instead, descriptive statistical analyses were completed when necessary to enhance clarity in data presentation.
Institutional review board approval
As a retrospective review of existing literature, this study did not require formal institutional review board approval.
Results
This search strategy yielded 90 initial findings, the contents of which were scrutinized against the search delimiters. After excluding citations that did not meet the search delimiters criteria, the search yielded 26 studies that included 98 patients (Table 2).
The majority of the studies (77%, 20/26) were case reports or case series. Prospective clinical trials accounted for 15% (4/26), of which 2 were open-label, while retrospective chart analyses constituted 8% (2/26).
Demographics
The analysis included a total of 98 patients, with 2 studies (Ji, 21 Maurani 23 ) accounting for 41 patients. Most studies included patients with venous malformations with cutaneous involvement, especially those studies with patients diagnosed with blue rubber bleb nevus syndrome.12–19,24,25,28–35 The overall age range was wide, from newborn 16 to 64 years. 26 In studies that reported patient sex, the distribution skewed toward women, with 27 female vs 19 male patients.
Treatment
Virtually all patients had received and failed previous treatments, including surgery, sclerotherapy, and supportive transfusions. Sirolimus, primarily administered orally except for one small study using a topical formulation in two patients, 30 was typically administered once or twice daily to achieve target serum trough levels of 5–15 ng/mL. Treatment duration with sirolimus varied considerably, ranging from 1 month 7 to 5 years.16,24
Sirolimus efficacy overview
Most of the studies (69%, 18/26) were observational and did not use standardized efficacy assessment; 19% (5/26) were baseline controlled, and the remaining 12% (3/26) were retrospective.
Overall, sirolimus demonstrated some level of efficacy in the majority of reported patients, with 72% (71/98) showing evidence of clinical improvement. Sirolimus yielded consistent improvement in symptoms such as bleeding, oozing, pain, and anemia, although evidence of malformation size reduction was inconsistent.21,23,26,35 Across the studies, there was no difference in efficacy based on mutation subtype, although not all studies reported on mutation subtype.
Symptom improvement
Improvements were noted in venous malformation symptoms such as pain, oozing, and disfigurement across studies. Additionally, functional capacity and quality of life (QoL) measurements showed improvement in several studies.20,23,25,26 Only one study from the group of 26 examined topical sirolimus, a small (N = 2), short-term (12-week) study: both patients experienced a decrease in pain, and one exhibited some evidence of lesion improvement. 30 While most case reports reported improvements in lesion size, which was assessed by a variety of methods including MRI and CT, as appropriate, some did not observe clinically meaningful reductions even after prolonged treatment of up to 2 years.11–13,15,23
Coagulopathy
Almost all studies showed treatment with sirolimus reduced episodes of bleeding. Sirolimus treatment resulted in improvements in coagulopathy markers, that are relevant for internal venous malformations, such as D-dimer levels22,26,31,34,35 and anemia.12,14,15,17,18,24,25
Anemia/transfusions
In a total of 7 case reports,18,19,24,28,31–33 1 prospective study, 35 and 1 retrospective review 25 involving 21 patients, the initiation of sirolimus treatment led to a resolution of anemia to the extent that transfusions were no longer necessary. Notably, in all of these studies, patients were diagnosed with blue rubber bleb nevus syndrome. Additionally, in 2 separate studies of 5 patients, a reduced need for transfusions became evident after approximately 2 months of sirolimus treatment.24,25
Adverse events
The most frequent AE associated with sirolimus treatment was mucositis, observed in 7/26 (27%) studies, which was generally mild or moderate in severity. However, it necessitated a dose reduction in one patient 12 and study discontinuation in another patient. 6 Other potentially relevant AEs noted included infection and neutropenia. Another study 25 reported serious but transient neutropenia (without infection) in one patient, resulting in only temporary discontinuation of treatment. In this study, targeted sirolimus trough levels were considered “relatively low” at 10–13 ng/mL and all patients received background antibiotic therapy. AEs were not reported in 65% (17/26) of the studies.
Discussion
The publications reviewed suggest that sirolimus may be an effective pharmacologic option in the management of internal venous malformations.6,36,37 However, it is important to note that sirolimus is not currently FDA-approved for the treatment of any vascular anomaly, including venous malformations. 4
Our study was the first systematic review to focus solely on the potential role of sirolimus in the management of venous malformations, a common type of vascular anomaly. 4 Our findings confirm and extend previous findings supporting a potentially important role for sirolimus in vascular anomalies such as venous malformations, especially those impacting internal organ systems.9,36,38 Our results suggest that oral sirolimus has the potential to improve the clinical manifestations posed by venous malformations, especially those that have extensive involvement with deeper internal structures, including coagulation, D-dimer expression, and anemia. The majority of patients (72%) showed evidence of treatment efficacy, despite an inadequate response to previous standard treatment. Sirolimus was administered orally in all but one study, 30 with a target blood level usually in the range of 5–15 ng/mL, which appears standard for oral treatment.36,37
There were too few patients in our analysis to evaluate the effect of oral or topical sirolimus on the cutaneous manifestations of venous malformations such as swelling, bleeding, pain, and raised blueish lesions. However, since oral sirolimus has very low dermal penetration, a topical formulation that achieves therapeutic levels of sirolimus in the dermis may offer superior efficacy and improved tolerability in terms of fewer systemic AEs for patients with predominately dermatologic lesions.4,39
Our literature review revealed that sirolimus treatment has been reported to provide consistent and enduring symptomatic relief for many patients with venous malformations, with improvements seen in lesion bleeding and size, pain, and enhancements in QoL assessments. In some studies, sirolimus provided continued and well-tolerated efficacy over study evaluation periods ranging from 2 to 5 years.6,16,17,24 These findings are consistent with the interim results of the phase III Vascular Anomaly-Sirolimus-Europe trial, of oral sirolimus (serum level 10–15 ng/mL). 40 That study includes 132 patients with slow-flow vascular malformations, 74 (56%) of whom were diagnosed with a venous malformation. After treatment (54% for at least 1 year; 46% for 2 years), 85% of patients experienced at least some clinical improvement, chiefly pain reduction and function improvement. Sirolimus also exerted a rapid ameliorative effect, with 50% of patients reporting symptomatic improvement within the first month of treatment. In addition, there were no differences in efficacy noted across mutation subtypes.
Patients with venous malformation associated syndromes, especially those with rare, serious syndromes, such as some overgrowth syndromes and blue rubber bleb nevus syndrome, may experience frequent gastrointestinal bleeding and, in turn, anemia requiring transfusions. 41 Sirolimus seemed to demonstrate notable efficacy in alleviating anemia and bleeding in these patients, reducing or obviating the need for transfusions.
AEs in our review were generally consistent with those previously reported with sirolimus treatment for vascular malformation.6,36,37 Mucositis was the most common AE and resulted in one dose reduction 12 and one study discontinuation. 6 Side effects typically associated with oral sirolimus treatment in the kidney transplant setting after 24 weeks’ treatment, including anemia, thrombocytopenia, and leukopenia, were not seen. 42 In our analysis, evidence of serious immunosuppression such as infection or neutropenia was uncommon.
These findings, however, should be viewed in context. Most studies included were either case reports or case series and investigators have shown that the vast majority (>90%) of these study types tend to present positive results, raising the risk of overinterpretation. 43 In addition, there are generalizability limitations in this study due to considerable heterogeneity in study conditions, processes, and outcome assessments. These limitations obscure the interpretation of systematic reviews such as ours that rely primarily on retrospective analyses. The immunosuppressive effects of long-term, oral sirolimus treatment can result in uncommon, but potentially concerning, AEs, such as an increased risk for serious infections. 26 This risk has likely hampered the widespread use of oral sirolimus. For the above reasons, caution should be used in interpreting the results of our analysis, especially AE rates. Further work is needed to characterize the safety and efficacy of sirolimus in treating both cutaneous and internal venous malformations.
Conclusion
Together, our findings suggest that sirolimus is an important therapy in the management of venous malformations regardless of underlying mutations. However, due to the retrospective nature of this review and the heterogeneity of the many case studies included, the current findings, although intriguing, should be considered an impetus for future prospective, controlled studies to clarify the role of sirolimus in the management of symptomatic venous malformations. Furthermore, differences in responses to treatment and a potential relationship to the type and location of the disease is an area that merits future examination.
Sirolimus appears to be a valuable addition to the armamentarium for the management of venous malformations, especially those located internally. Although controlled studies are still needed, the preponderance of findings to date, as captured in our study, suggests that sirolimus can be effective and well tolerated in a patient population in need of alternative treatment options.
Authors’ Contributions
J.T.: Conceptualization, writing, and analysis. J.M.: Conceptualization, writing, and analysis. M.K.: Conceptualization, writing, and analysis. M.T.: Conceptualization, writing, and analysis. A.G.: Formal analysis.
Footnotes
Acknowledgment
The authors would like to thank Encompass Communications and Learning, Inc., for their editorial assistance in the development of this article.
Author Disclosure Statement
J.T., M.K. are consultants to Palvella Therapeutics. J.M. is an employee of Palvella Therapeutics. The other authors do not have any disclosures.
Funding Information
Dr. Martini is an employee of Palvella Therapeutics, that sponsors the project. Drs. Teng, Kelly and Tollefson did not receive compensation for their work related to this publication.