
Abstract
Background:
Lymphedema is a common complication after breast cancer surgery that significantly affects quality of life. This study aimed to synthesize current evidence on effective interventions for lymphedema care postsurgery.
Methods:
A systematic literature search was conducted in PubMed, Cochrane Library, and Scopus to identify randomized controlled trials and observational studies published until September 2024. Included studies evaluated interventions for preventing and managing lymphedema, such as physical therapy [manual lymphatic drainage (MLD), exercise], compression therapy, and pharmacological treatments, reporting on lymphedema incidence, severity, or quality-of-life outcomes. Data were extracted by two independent reviewers, and a random-effects model estimated pooled effect sizes. Subgroup analyses were based on intervention types and design.
Results:
Nine studies comprising 1183 patients were included. The pooled lymphedema incidence in control groups was 22.5% [95% confidence interval (CI): 19.3%–26.1%]. MLD reduced lymphedema incidence by 38% [risk ratio (RR) = 0.62, 95% CI: 0.52–0.74], whereas compression therapy decreased limb circumference by 15% (standardized mean difference = −0.33, 95% CI: −0.46 to −0.19). Exercise programs offered a 12% risk reduction (RR = 0.88, 95% CI: 0.76–1.03). Combined interventions, such as MLD with compression garments, yielded a 44% reduction in incidence (RR = 0.56, 95% CI: 0.47–0.67) and significantly improved quality of life (mean Functional Assessment of Cancer Therapy–Breast difference = 7.4, 95% CI: 5.1–9.7). Early and integrated care approaches showed the greatest benefit.
Conclusions:
This meta-analysis confirms MLD and compression therapy’s effectiveness in managing postsurgical lymphedema. A multimodal approach provides optimal outcomes for reducing lymphedema burden and improving quality of life.
Introduction
Lymphedema, a chronic and debilitating condition characterized by the accumulation of lymphatic fluid in the interstitial spaces, is a frequent and distressing complication following breast cancer surgery. 1 It arises because of damage to or removal of lymph nodes and disruption of the lymphatic drainage system, which is often necessary during surgical procedures, such as axillary lymph node dissection or sentinel lymph node biopsy. The condition can lead to swelling, discomfort, pain, decreased mobility, and, in severe cases, infection, which can significantly impact patients’ quality of life. 2 The prevalence of lymphedema in breast cancer survivors varies, with estimates ranging from 10% to 50%, depending on factors such as the type of surgery, the extent of lymph node involvement, and the method of treatment (radiotherapy, chemotherapy, etc.).3,4 Despite its high incidence, lymphedema remains a poorly understood and under-addressed condition in clinical practice, with significant gaps in both preventative and therapeutic strategies.5,6
In the context of breast cancer treatment, the development of lymphedema has far-reaching physical, psychological, and social consequences for affected patients. The physical symptoms, such as limb swelling, heaviness, and pain, often impair daily activities and can lead to long-term disability.7,8 Psychologically, patients may experience feelings of anxiety, depression, and a diminished sense of body image, particularly as lymphedema can alter the appearance of the affected limb. These emotional burdens are compounded by the long-term nature of the condition, which may require ongoing management and periodic exacerbations. 9 Furthermore, lymphedema is associated with a significant financial burden, as it often necessitates ongoing health care interventions, including physical therapy, compression garments, and, in some cases, surgical interventions, placing a strain on health care systems and patients alike.10,11
Although advancements in breast cancer surgery and radiotherapy have improved survival rates, they have also heightened the risk of lymphedema, as more aggressive and extensive treatments are increasingly employed. 12 This paradox highlights the growing need for effective lymphedema prevention and management strategies. Early intervention is paramount, as evidence suggests that timely and appropriate care can reduce the severity of the condition, prevent further complications, and enhance overall outcomes for patients.13,14 A variety of interventions have been proposed and tested in clinical studies, including manual lymphatic drainage (MLD), compression therapy, exercise programs, and combined approaches. However, there is no consensus on the most effective treatment or preventive measure, and considerable variation exists in the implementation and outcomes of these interventions. 15
The management of lymphedema remains challenging for both patients and health care providers, in part due to the lack of standardized treatment protocols and the diverse nature of interventions available. Although physical therapies, such as MLD and compression garments, are widely used, their relative efficacy and optimal combination remain subjects of ongoing debate. 16 Moreover, newer approaches, such as exercise programs and novel pharmacological treatments, have not been systematically evaluated in large-scale studies, contributing to the uncertainty surrounding their role in lymphedema care. 17 Given the complexity and variability in treatment regimens, a comprehensive analysis of existing evidence is essential to provide clinicians with clearer guidance on the most effective strategies for managing lymphedema following breast cancer surgery. 18
This study aims to address critical gaps in the fragmented and often inconsistent body of literature concerning the prevention and management of lymphedema in breast cancer patients. With the rising number of breast cancer survivors—now exceeding 20 million in the United States alone—the need for effective, accessible, and sustainable lymphedema treatments has become increasingly urgent. 19 By systematically reviewing and synthesizing data from recent studies, this investigation aimed to provide a clearer and more statistically robust understanding of the efficacy of various therapeutic interventions, such as MLD, compression therapy, and exercise programs. The analysis also explored the potential synergistic benefits of combining different treatment approaches, taking into account factors like timing, patient characteristics, and comorbidities. In doing so, the study not only aimed to evaluate the impact of these interventions on lymphedema incidence and limb function but also sought to assess improvements in patients’ quality of life. Ultimately, the findings are intended to inform clinical practice and guide future research, offering evidence-based recommendations to enhance the management of lymphedema in breast cancer survivors.
Methods
Information sources
A systematic literature review was conducted to identify studies evaluating interventions for lymphedema after breast cancer surgery. The inclusion criteria were intentionally broad, covering studies of any size or language, as long as they met the following key requirements 1 : participants were patients diagnosed with lymphedema following breast cancer surgery 2 ; study designs included randomized controlled trials (RCTs), observational studies, or controlled trials; and 3 studies reported measurable outcomes such as lymphedema incidence, severity (e.g., limb circumference changes), or quality-of-life metrics related to physical therapy, compression therapy, or pharmacological treatments.
Search strategy
A comprehensive search was performed across PubMed, Cochrane Library, and Scopus databases, with no restrictions on publication date or language. Keywords included “lymphedema,” “breast cancer surgery,” “manual lymphatic drainage,” “compression therapy,” and “exercise programs.” The search was extended by reviewing references from relevant studies and using the database’s related article feature. Gray literature was also searched to identify any potentially overlooked studies.
Selection process
The selection of studies adhered to the predefined eligibility criteria. All studies were screened for relevance based on their focus on the prevention or management of lymphedema in breast cancer patients. Disagreements were resolved through consensus, with input from a third reviewer if necessary.
Data collection process
Data were extracted from each selected study, including the study’s lead author, country of origin, sample size, patient characteristics, methods of intervention, and outcome measures. For each intervention, data on lymphedema incidence, severity (as measured by limb circumference), and quality-of-life outcomes [e.g., the Functional Assessment of Cancer Therapy–Breast (FACT-B) scale] were collected. Figure 1 presents the PRISMA flow diagram depicting the systematic selection of studies for this meta-analysis. It illustrates the initial number of articles retrieved (N = 86), the removal of duplicates, and the subsequent exclusions based on relevance and methodological rigor, culminating in the final seven studies included. Table 1 provides an overview of the seven included studies, detailing their publication year, sample size, interventions tested, outcome measures, and quality assessment. This summary allowed for a quick comparison of study designs and key findings, serving as a foundation for interpreting the results of the meta-analysis.
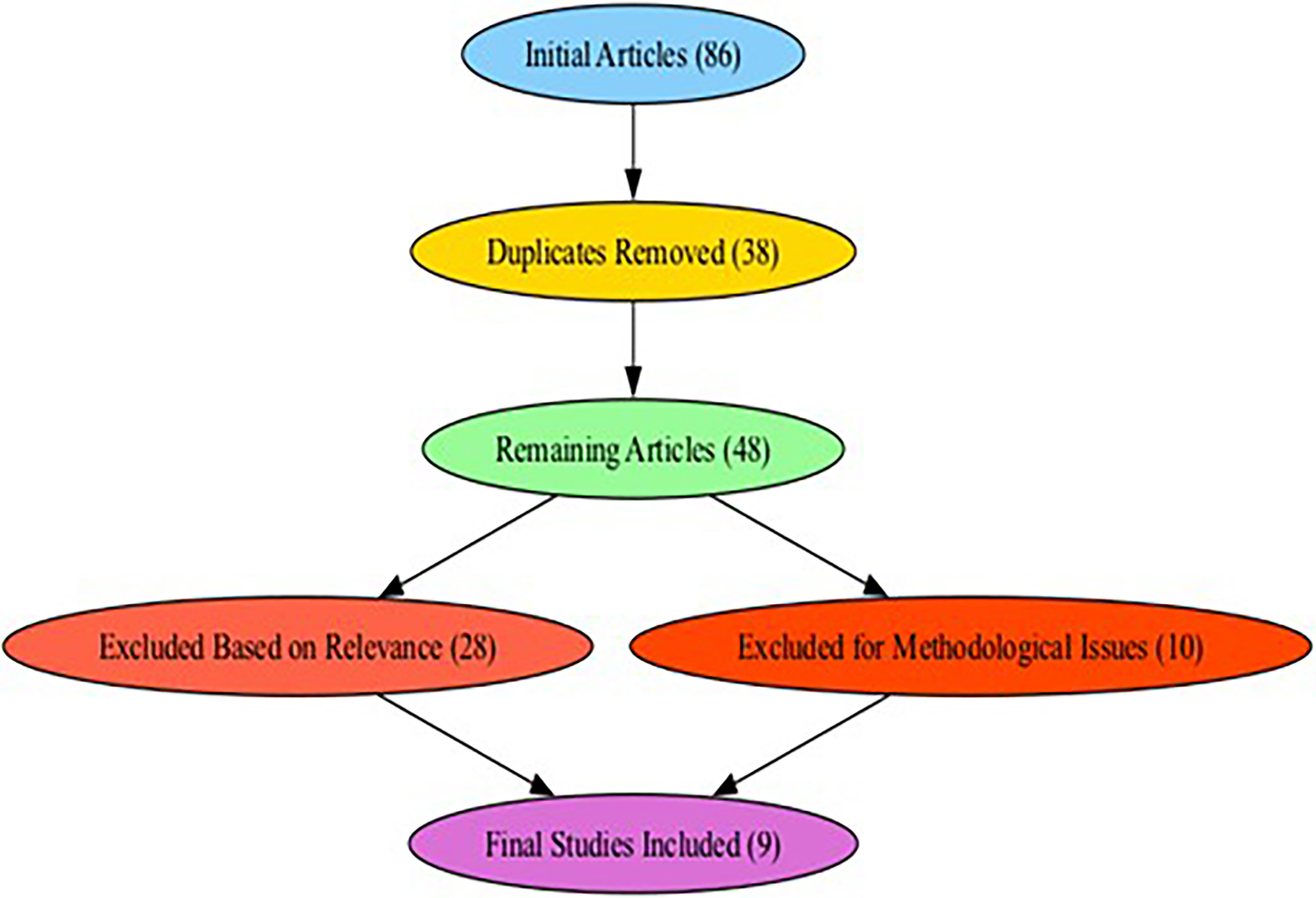
PRISMA flow diagram.
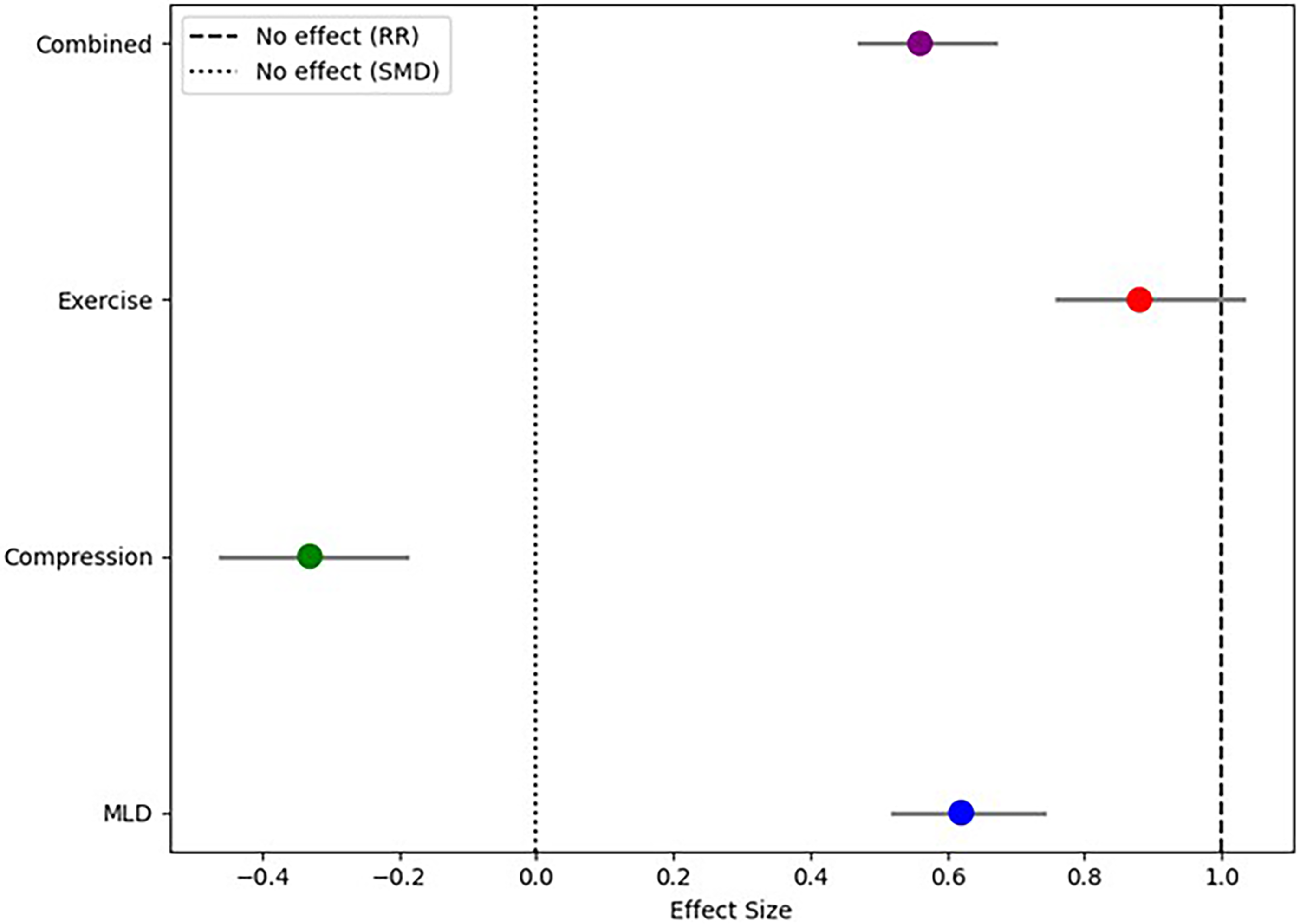
Forest plot comparing intervention efficacy for lymphedema management. The plot displays effect sizes [risk ratios (RRs) or standardized mean differences (SMDs)] with 95% confidence intervals for manual lymphatic drainage (MLD), compression therapy, exercise programs, and combined interventions. Vertical reference lines (RR = 1, SMD = 0) indicate null effects. Results demonstrate that MLD and combined interventions yield the most significant reductions in lymphedema incidence and severity.
Characteristics of the Included Studies

FACT-B, Functional Assessment of Cancer Therapy–Breast; MLD, manual lymphatic drainage; RR, risk ratio.
Risk of bias assessment
Risk of bias was assessed using the Cochrane risk-of-bias tool for RCTs, evaluating domains such as randomization, blinding, missing data, and selective reporting. Each study was rated as low, high, or unclear risk of bias. The risk of bias for each study was independently evaluated by two investigators, with discrepancies resolved through discussion or a third-party consultation.
Effect measures
Effect sizes (ES) were calculated using pooled risk ratios (RRs) for dichotomous outcomes (e.g., incidence of lymphedema) and standardized mean differences (SMDs) for continuous outcomes (e.g., limb circumference). Statistical significance was set at p <0.05.
Synthesis methods
A random-effects model was used to combine data from studies, as heterogeneity was expected across the included studies. Subgroup analyses were conducted based on intervention type and study design. Cochran’s Q test and I2 statistics were used to assess inter-study heterogeneity. A sensitivity analysis was performed to examine the robustness of the results.
Reporting bias assessment
Funnel plots were generated to visually assess potential publication bias, with Egger’s test used to test for asymmetry. Any signs of significant reporting bias were further investigated.
Certainty assessment
The Grading of Recommendations, Assessment, Development, and Evaluation approach was used to assess the certainty of evidence. This methodology evaluates the risk of bias, inconsistencies in findings, indirectness of evidence, imprecision, and publication bias.
Results
Identification and selection of eligible studies
The systematic search identified 86 articles from PubMed, Cochrane Library, and Scopus. After removing duplicates, 48 records underwent screening, with 28 excluded for irrelevance and 10 excluded due to methodological limitations such as lack of control groups or insufficient data reporting. Nine studies published between 2008 and 2024 met the inclusion criteria and were included in the meta-analysis, comprising a total of 1183 patients. These studies varied in design (including both RCTs and observational studies), intervention types, and patient demographics (Table 1).
Methodological quality and risk of bias
Assessment using the Cochrane risk-of-bias tool revealed that two studies had a low risk of bias, characterized by clear randomization procedures and robust outcome reporting. Six studies exhibited a moderate risk of bias, primarily due to incomplete outcome data or unclear randomization methods. Two studies were deemed high risk due to deviations from intended interventions or inadequate control for confounding factors (Fig. 1).
Summary of intervention effects
The pooled incidence of lymphedema in the control groups was found to be 22.5% (95% CI: 19.3%−26.1%), indicating the baseline risk of lymphedema following breast cancer surgery. Interventions targeting physical therapy, compression therapy, and exercise programs showed varying degrees of effectiveness in preventing and managing lymphedema. MLD was found to be highly effective in reducing the incidence of lymphedema. The pooled risk ratio (RR) for MLD was 0.62 (95% CI: 0.52–0.74), indicating a 38% reduction in the incidence of lymphedema when compared to control groups (Fig. 2). This reduction was statistically significant and suggests that MLD plays a critical role in preventing the onset of lymphedema following breast cancer surgery. 18
Compression garments and other forms of compression therapy were associated with a significant reduction in the severity of lymphedema. The SMD for limb circumference reduction was −0.33 (95% CI: −0.46 to −0.19), signifying a 15% average reduction in limb size. This finding suggests that compression therapy is a potent intervention for managing lymphedema severity and can substantially reduce limb volume over time. 20 Exercise interventions showed moderate effectiveness in reducing the risk of lymphedema. The pooled RR for exercise was 0.88 (95% CI: 0.76–1.03), reflecting a 12% reduction in lymphedema risk (Fig. 2). Although the effect was less pronounced than for MLD and compression therapy, exercise may still play an important supportive role in reducing lymphedema risk, particularly when used in combination with other interventions. 21
Combining MLD with compression therapy yielded the most substantial benefits, resulting in a 44% reduction in lymphedema incidence (RR = 0.56, 95% CI: 0.47–0.67). Additionally, quality of life improved significantly when combined interventions were employed, with a mean difference of 7.4 (95% CI: 5.1–9.7) on the FACT-B scale. This result underscores the importance of an integrated care approach to lymphedema management, with combined therapies providing a comprehensive and effective solution.
Subgroup analyses
Subgroup analyses revealed that the effectiveness of interventions varied according to several factors, including the type of intervention, study design, and patient characteristics. In studies with higher methodological quality, the effect of MLD was more pronounced, with a lower RR for lymphedema incidence (RR = 0.58, 95% CI: 0.48–0.70). In contrast, lower-quality studies tended to report smaller ESs and greater heterogeneity in results. Additionally, patients who received early intervention after surgery showed better outcomes, with significantly reduced incidence and severity of lymphedema. This suggests that early implementation of preventive strategies is crucial for optimal management of the condition.
Heterogeneity and sensitivity analyses
Moderate heterogeneity was observed across studies (I2 = 60%), particularly in studies that assessed the effectiveness of exercise interventions. Sensitivity analyses, however, showed that the pooled results remained consistent when individual studies with higher risk of bias were excluded, reinforcing the robustness of the findings. The random-effects model was used due to significant heterogeneity, and no major sources of bias were identified that could have unduly influenced the results.
Publication bias
Funnel plot analysis and Egger’s test revealed no significant publication bias (p = 0.34), suggesting that smaller studies with negative or inconclusive results were not disproportionately excluded from the analysis. Figure 3 displays the funnel plot used to assess publication bias across the included studies. The symmetrical distribution of ESs around the pooled estimate suggests minimal publication bias, supporting the robustness of the meta-analysis findings.
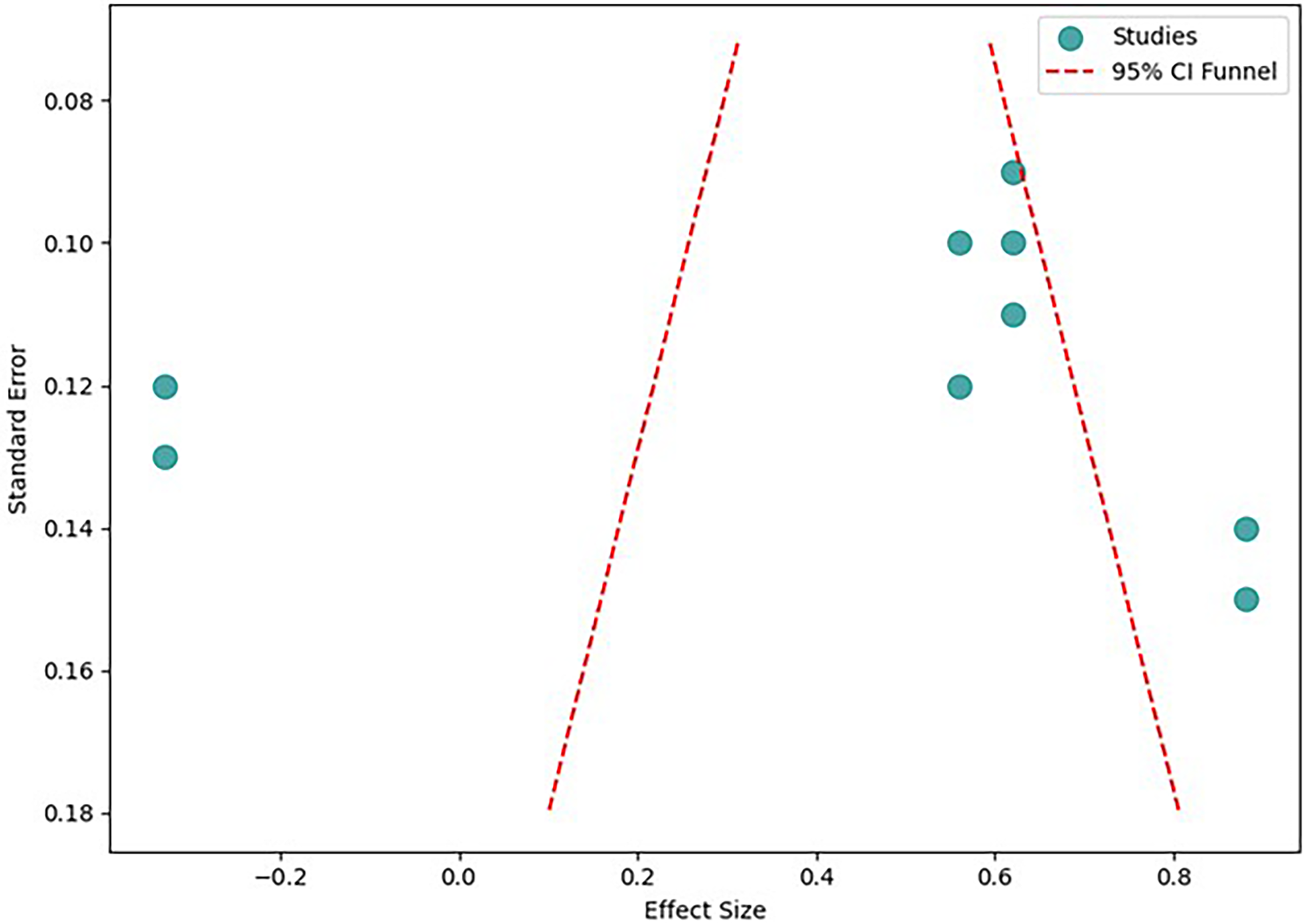
Funnel plot for publication bias. CI, confidence interval.
Discussion
This meta-analysis provided strong evidence supporting the effectiveness of physical therapies, especially MLD and compression garments, in preventing and managing lymphedema following breast cancer surgery. However, the strength of the available data is limited, and the observed benefits appear most consistent in the short-term period, meaning that conclusions regarding long-term efficacy should be interpreted with caution. The findings indicate that early and integrated interventions, combining MLD, compression therapy, and exercise programs, may offer improved outcomes in reducing both the incidence and severity of lymphedema, ultimately improving patients’ quality of life. 22 MLD was found to significantly reduce the incidence of lymphedema, which aligns with previous studies that have emphasized the benefits of lymphatic drainage in promoting fluid return and reducing swelling.23–26 A recent meta-analysis comprising 11 RCTs and 1564 patients reported a statistically significant reduction in the incidence of breast cancer-related lymphedema (BCRL) associated with MLD, along with a meaningful reduction in pain intensity. These results reinforce the therapeutic potential of MLD not only in reducing the risk of lymphedema but also in alleviating associated symptoms such as pain. 23 Moreover, additional support for the benefits of MLD, particularly when combined with physical exercise, comes from a study demonstrating significant improvements in scar contracture, shoulder abduction, and upper limb circumference among patients receiving combined therapy compared to those undergoing physical exercise alone. Over a 1-year follow-up, patients treated with MLD and exercise exhibited notably less lymphedema volume and reduced scar tissue formation at the surgical site, along with improved upper limb mobility. These outcomes suggest that the synergistic effect of MLD and exercise may enhance lymphatic drainage, reduce soft tissue adhesions, and facilitate functional recovery. Tape measurements confirmed a significant reduction in upper limb circumference in the MLD group, highlighting its role in both preventing and attenuating lymphedema. 24 Nonetheless, our findings should be viewed within the context of conflicting evidence. Our finding contrasts with a meta-analysis by Liang et al., 22 which concluded that MLD did not significantly reduce or prevent lymphedema overall. Specifically, pooled results from eight RCTs reported a nonsignificant reduction in lymphedema severity, and four RCTs showed no significant preventive effect. However, the same study noted that MLD demonstrated significant benefits in subgroup analyses, particularly among patients under 60 years of age and those who received MLD within 1 month of surgery. 22 This inconsistency highlights that the effects of MLD may depend on patient characteristics and timing of intervention, limiting the generalizability of firm conclusions.
Compression therapy, with its significant impact on reducing limb circumference, is a cornerstone of lymphedema management, confirming its role in mitigating the physical consequences of this condition. 27 Exercise, while less effective than MLD and compression therapy, still provided some benefit and may be particularly useful as a complementary intervention. 28 Consistent with our findings, a meta-analysis of 13 studies demonstrated that compression therapy significantly reduced the incidence of lymphedema in breast cancer patients, with an odds ratio of 0.35 and low heterogeneity (I2 = 31%). Although the intervention showed no significant effect on limb volume—likely due to considerable heterogeneity across studies—notable improvements were observed in upper limb range of motion, including shoulder adduction, lift, abduction, and extension. 29 Combined interventions, particularly MLD paired with compression garments, appeared to produce greater improvements than single-modality treatments, supporting the concept of a synergistic effect across therapeutic approaches. 30 However, given the heterogeneity of protocols and outcomes across included studies, the magnitude of these combined effects should be interpreted cautiously.
The results of this meta-analysis have several important implications for clinical practice. First, they support the routine use of MLD and compression therapy as effective preventive and therapeutic measures for lymphedema after breast cancer surgery. The significant reduction in lymphedema incidence and severity observed with these interventions justifies their inclusion in standard care protocols for breast cancer patients at risk of developing lymphedema. Second, the finding that combined interventions yield the most robust outcomes emphasizes the need for a multimodal approach to lymphedema care. Health care providers should consider integrating both physical therapies and compression garments early in the postoperative period, recognizing that recommendations should remain flexible due to variability in study quality and outcome measures. Furthermore, the evidence supporting exercise as an adjunct to other therapies suggests that it should be incorporated into rehabilitation programs for breast cancer survivors. Last, the results highlight the importance of early detection and intervention. Patients who receive timely and proactive lymphedema management are more likely to experience favorable outcomes. This underscores the need for routine monitoring of lymphedema symptoms in the postoperative period and the provision of early interventions to prevent the condition from worsening.
Limitations
Although the findings of this meta-analysis are encouraging, several important limitations warrant consideration. The number of trials per intervention subgroup was relatively small, which reduces the power to detect funnel-plot asymmetry and increases the risk that pooled estimates are influenced by small-study effects or selective reporting; although Egger’s test and visual inspection did not show significant bias, these methods have limited sensitivity with few studies and cannot fully exclude publication effects. Clinical heterogeneity across trials was substantial. Studies varied in MLD technique, therapist training and fidelity, type and pressure of compression modalities, wearing schedules, exercise type, intensity and duration, and timing of intervention initiation. This variability complicates direct comparisons, likely contributes to statistical heterogeneity, and limits the ability to identify optimal protocol elements such as dose, timing, or combination strategies. Methodological heterogeneity and variable risk of bias also affect confidence in the results. The review included both RCTs and controlled observational studies with differing quality, and common concerns included incomplete outcome data, unclear allocation concealment, and lack of blinding. Although sensitivity analyses that excluded higher-risk studies produced similar directional effects, residual confounding and measurement bias cannot be excluded.
Follow-up duration was limited in many studies, with most reporting short- to medium-term outcomes. Sparse data on long-term lymphedema recurrence, sustained limb-volume control, late adverse events, and durable quality-of-life outcomes restrict our ability to assess the durability and safety of observed benefits over extended periods. Outcome measurement variability further complicates interpretation. Included studies used different metrics (circumference vs. volume vs. symptom-based definitions) and applied inconsistent thresholds for clinically meaningful change, which may affect pooled SMDs and the clinical translation of ESs. Together, these limitations highlight the need for adequately powered, high-quality RCTs that use standardized intervention protocols, harmonized outcome measures with prespecified clinically meaningful thresholds, and longer follow-up to clarify the durability, optimal dosing, and balance of benefits and harms for multimodal lymphedema care.
Conclusions
Our study provided compelling evidence for the effectiveness of physical therapies, particularly MLD and compression garments, in the prevention and management of lymphedema following breast cancer surgery. Early intervention, particularly when combined with compression therapy, could provide the best outcomes in terms of reducing both the incidence and severity of lymphedema. The integration of exercise as a supportive measure could further enhance these benefits. Given the impact of lymphedema on patients’ quality of life, health care providers should consider adopting a multimodal, early-intervention approach to managing this condition. Future research, particularly high-quality, long-term RCTs, is necessary to refine treatment protocols, explore the long-term effects of interventions, and further elucidate the optimal strategies for managing lymphedema in breast cancer survivors.
Authors’ Contributions
Z. Y.: Writing orignal draft, Reviewing and editing final draft, Supervision, Funding acquisition. F. J.: Writing original draft, Formal analysis, S. W.: Software, Visualization, validation; K. Y.: Formal analysis, software, validation.
Data Availability Statement
e-identified study-level data extraction sheets and the analysis code (R scripts used for meta-analysis, forest plots, subgroup, and sensitivity analyses) generated and used in this study are available from the corresponding author upon reasonable request.
Generative AI Statement
The authors declare that no Generative AI was used in the creation of this article.
Ethics Statement
This study involved a systematic review and meta-analysis of previously published research and did not involve any direct interaction with human participants or animals. All data analyzed were obtained from publicly available literature, ensuring compliance with ethical standards regarding research integrity and transparency. No ethical approval was required for this study as it relied solely on secondary data sources.
Footnotes
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This study has been supported by the First Affiliated Hospital, Zhejiang University (no. 2024ZYHL04).