
Abstract
Purpose:
In times when health and physical activity are gaining in value, the search for effective methods to support fitness and improve quality of life is becoming a priority. One of the therapies that is gaining increasing popularity is pressotherapy, which supports the regeneration of the body on many levels.
Methods:
The study was conducted on a group of 15 healthy, young women. The participants underwent 10 pneumatic compression therapy treatments using the CarePump Expert8 device. The participants were examined 4 times: a week before the first treatment, immediately before the first treatment, after the 10th treatment and a week after the 10th treatment.
Results:
Statistical analysis of mean changes in the range of motion values showed significant decrease in: right (p < 0.05) and left (p < 0.05) hip joint extension; right (p < 0.05) hip joint horizontal abduction; horizontal adduction of the right (p < 0.05) and left (p < 0.05) hip joint; dorsiflexion of the right (p < 0.05) and left (p < 0.05) ankle joint, and also an increase in: right (p < 0.05) and left (p < 0.05) hip external rotation. Statistical analysis of changes in mean values of circumferences showed significant decrease at all tested levels: P1 right (p < 0.05) and left (p < 0.05); U1 right (p < 0.05) and left (p < 0.05); U2 right (p < 0.05) and left (p < 0.05); K right (p < 0.05) and left (p < 0.05); G1 right (p < 0.05); and left (p < 0.05); G2 right (p < 0.05) and left (p < 0.05).
Conclusions:
A series of pressotherapy sessions did not improve lower limb range of motion or body composition indices; however, it did reduce circumferences at all levels of the lower limbs. Long-term use of pressotherapy can help maintain healthy fluid levels, improve circulation, and improve overall physical fitness.
Introduction
As health and physical activity become more valued, the search for effective methods to support fitness and improve quality of life is becoming a priority. In this perspective, physiotherapy as a field dealing with the treatment and prevention of injuries and diseases of the musculoskeletal system plays a key role in promoting a healthy lifestyle and ensuring optimal functioning of the body. However, despite significant progress in the field of medicine, there are still areas that require further research and exploration to better understand the impact of physical therapy on the health and well-being of an individual.
One of the therapeutic methods that is becoming increasingly popular is pressotherapy, also known as pneumatic compression therapy. This innovative form of therapy is based on mechanical pneumatic compression and is an effective tool supporting the therapy of lymphedema, improving blood circulation, and reducing swelling and lymphatic congestion. 1 Pressotherapy uses special compression cuffs that are placed on individual limbs. 2 These cuffs have internal chambers in which the pressure can be controlled in the range of 20–220 mmHg. An air pump is used to regulate the pressure, which is connected to cuffs containing several chambers. By changing the pressure in individual chambers, it is possible to exert controlled pressure on the limbs, thus imitating a natural massage that reflects the flow of blood and lymph in the veins and lymphatic vessels. It is often a supplement to manual lymphatic drainage or is its continuation. 3
Indications for lymphatic drainage include lymphedema, which occurs when the capacity of the lymphatic system to transport lymph is insufficient in relation to the amount of interstitial fluid produced. This imbalance may result from decreased functional efficiency of lymphatic vessels, structural abnormalities of the lymphatic network, an increased formation of tissue fluid, or a combination of these mechanisms. As a consequence, lymph accumulates in the interstitial space, leading to chronic swelling and progressive tissue changes.
Lymphedema may develop due to a wide range of underlying conditions, including traumatic injuries, prolonged periods of immobilization, surgical interventions such as mastectomy with lymph node dissection, infectious or parasitic diseases, inflammatory and dermatological disorders, dysfunctions of the nervous system, certain types of cancer causing obstruction or infiltration of lymphatic vessels, diabetes mellitus, drug-induced lymphadenopathy, and circulatory failure or related cardiovascular diseases. Both primary (congenital) and secondary (acquired) forms of lymphedema may therefore constitute indications for lymphatic drainage therapy. In addition to the treatment of lymphedema, lymphatic massage is commonly used to alleviate the sensation of heavy and tired legs, support metabolic processes, and facilitate the removal of metabolic by-products from tissues. In physically active individuals and athletes, lymphatic drainage may play a supportive role in accelerating post-exercise recovery by reducing muscle edema and improving microcirculation following intense physical effort. Through the application of mechanical pneumatic compression, pressotherapy enhances lymphatic and venous outflow, reduces lymphatic stasis, and promotes more efficient fluid redistribution. As a result, this therapeutic modality contributes to the reduction of swelling, improvement of blood and lymph circulation, and acceleration of regenerative processes in fatigued or overloaded muscle tissues. 4
This allows athletes to return to training or competition more quickly. Intermittent pneumatic compression (IPC), also used in prevention, can play an important role in preventing swelling, especially in people who are exposed to prolonged sitting or standing, such as during office work 5 or long air travel. 6 Regular sessions of this type of therapy can help maintain proper lymph and blood circulation, which in turn can effectively prevent the occurrence of lower limb swelling. In cosmetology, pressotherapy is often used to improve the appearance of the skin and reduce cellulite. 7 Mechanical pneumatic compression helps to remove excess fluid from tissues, which can help reduce the visibility of cellulite and improve skin firmness and elasticity. In addition, pressotherapy can support the skin detoxification process by improving lymph and blood circulation, which helps eliminate toxins from the body.
The aim of the study was to investigate the effects of a series of pressotherapy treatments in young healthy women, with particular emphasis on the range of motion of the lower limbs, lower limb circumferences, and body composition analysis. The main aim was to conduct a comprehensive analysis of the therapeutic effects of pressotherapy in the context of prevention and improvement of health of people who do not struggle with any serious health problems or lower limb injuries. IPC treatments are becoming increasingly available, which means that not only professional athletes, people with injuries or diseases have access to pressotherapy. Scientific studies usually address the topic of pressotherapy in the treatment and secondary prevention of venous diseases of the lower limbs, edema, in cosmetology, and in regeneration. However, there is a lack of studies assessing the effects in healthy people and the use of pressotherapy in primary prevention. The studies conducted in healthy individuals will also allow for the possible identification of side effects and adverse reactions, which may be difficult to price in people with various problems. This will allow for increased safety during subsequent procedures and tests. Specially selected use of pressotherapy in this diverse group of patients can provide important information on its potential benefits and effectiveness in the context of improving physiological parameters. It was decided to study young women first, because they are more likely to use preventive treatments and are more likely to encounter potential problems later in life, and it is also planned to extend further studies to include women with lipodystrophy and/or lymphatic congestion and edema.
Methods
Participant
The presented prospective, controlled study was consistent with the assumptions of the Helsinki Declaration; each volunteer read the information about the study design and was given the opportunity to ask questions, after which he gave informed written consent to participate in the study; A physiotherapist took care of the participants’ safety.
The study was conducted on a group of 15 young women aged 20 to 26 years (22.53, SD = 1.55), body height 164.60 cm (SD = 5.74), body weight 62.65 kg (SD = 8.09) who were healthy women without comorbidities and lower limb injuries. The study lasted for 4 weeks, during which the participants received daily pressotherapy treatments lasting 30 minutes for 2 weeks.
Inclusion Criteria:
female gender, age 20–26 years, generally good health, not undergoing regular physical training, no changes in diet immediately before and during the study (participants’ diets were self-reported and were not monitored during the study).
Exclusion Criteria:
comorbidities, contraindications to participation in pressotherapy procedures, use of other physiotherapy treatments immediately before and during the study.
Experimental design
During the study, three main physiological parameters were measured: lower limb ranges of motion using a goniometer (MSD Europe BVBA Health, Fitness & Wellness Products, Londerzeel, Belgium), lower limb circumferences using a centimeter tape SECA 203 (Seca gmbh & co. kg, Hamburg, Germany), and body composition analysis using a Tanita BC-418 MA scale (Tanita Corporation, Tokyo, Japan). Measurements were performed in controlled conditions, ensuring adequate privacy and comfort for the study participants. All measurements were performed by qualified research personnel who had been previously trained in standard measurement procedures and use of the equipment used. This ensured the consistency and accuracy of the measurement data.
Goniometric measurements were performed to accurately assess the range of motion of the participants’ lower limbs. Each time, the mobility of the hip joint was measured in the sagittal, frontal, transverse, and rotational planes, the knee joint in the sagittal plane, and the upper ankle joint in the sagittal plane. A goniometer was used to perform the measurements. It consists of a base and two arms, one of which is movable.
The lower limb circumferences were measured in a standing position. These measurements included the circumference of the gluteus brevis (P1), the circumference of the thigh at its widest point (U1) and 6 cm above the base of the patella (U2), the circumference of the knee joint (K), the circumference of the lower leg at its widest point (G1) and the circumference above the ankle joint (G2), which allows for the assessment of any changes in body dimensions after a series of pressotherapy treatments.
The standard method, dual energy X-ray absorptiometry, is difficult to perform in routine clinical practice, unlike the bioelectrical impedance analysis (BIA) method; therefore, we used BIA in our study. The study used the Tanita BC-418 scale, an advanced device used to measure body weight and analyze body composition. Its operation is based mainly on the principle of a BIA, which helps determine body composition by passing a low current signal through the body. During the measurement, the person stands barefoot on a scale platform, on which eight electrodes are placed—four in the lower platform and four in the hand grips. The device sends a low electric current through the body and then measures the resistance that this current encounters as it flows through various tissues, such as muscle, fat, bone, and water. The analyzer provides a full profile of the body composition of the tested person in about 20 seconds. Based on this data, the Tanita scale determines various parameters related to body composition. The Tanita scale provides information on: Total body mass, muscle mass, fat mass (FAT MASS), body fat percentage (FAT%), body mass index (BMI), fat free mass (FFM), total body water, bone mineral mass, protein mass, basal metabolic rate. The study was developed in accordance with standardized procedures.8,9
The study was conducted over a period of 4 weeks, during which the participants underwent a series of 10 pressotherapy treatments and measurements of physiological parameters. Pressotherapy treatments were conducted daily for 30 minutes, using the CarePump Expert8 device (Bardomed LLC, Krakow, Poland) supporting eight chamber cuffs for the lower limbs, with a gradient set at 1 mmHg, a 3-second “hold” parameter (a break after the end of filling one chamber before filling the next one), and pressure individually selected to the participant’s sensations (maximum tolerated pressure without pain sensations). A standard program was used, which involves sequential filling of subsequent chambers while maintaining the pressure in previously inflated chambers. Participants were examined four times: 1 week before the first treatment, immediately before the first treatment, after the 10th treatment, and 1 week after the 10th treatment.
Statistical analysis
Descriptive statistics were determined: mean as well as standard deviation. The normality of distributions was verified with the Shapiro-Wilk test. In order to determine the level of significance of changes within the study group depending on the moment of measurement, the ANOVA/MANOVA test for repeated measurements was used. Homogeneity of variances was tested by Levene’s test. In the case of statistically significant differences in the analysis of variance, post-hoc tests were performed (Dunn’s multiple comparisons of mean ranks for all tests). The significance level of p = 0.05 was assumed in the analyses. To determine the sample size, the formula for the minimum sample size was used, which assumed a confidence interval of 95%, a fraction size of 0.5, and a maximum error of 5%. Effect sizes were interpreted using eta squared (η2), with values of 0.01–0.05 considered small, 0.06–0.13 moderate, and ≥0.14 large effects. The analyses were performed with the use of the Statistica 13 package (Tibco Software Inc., USA).
Results
The average results of individual measurements are given in Table 1.
Lower Limb Joint Mobility Ranges, Lower Limb Circumferences and Tested Body Composition Indices (Mean ± Standard Deviation)
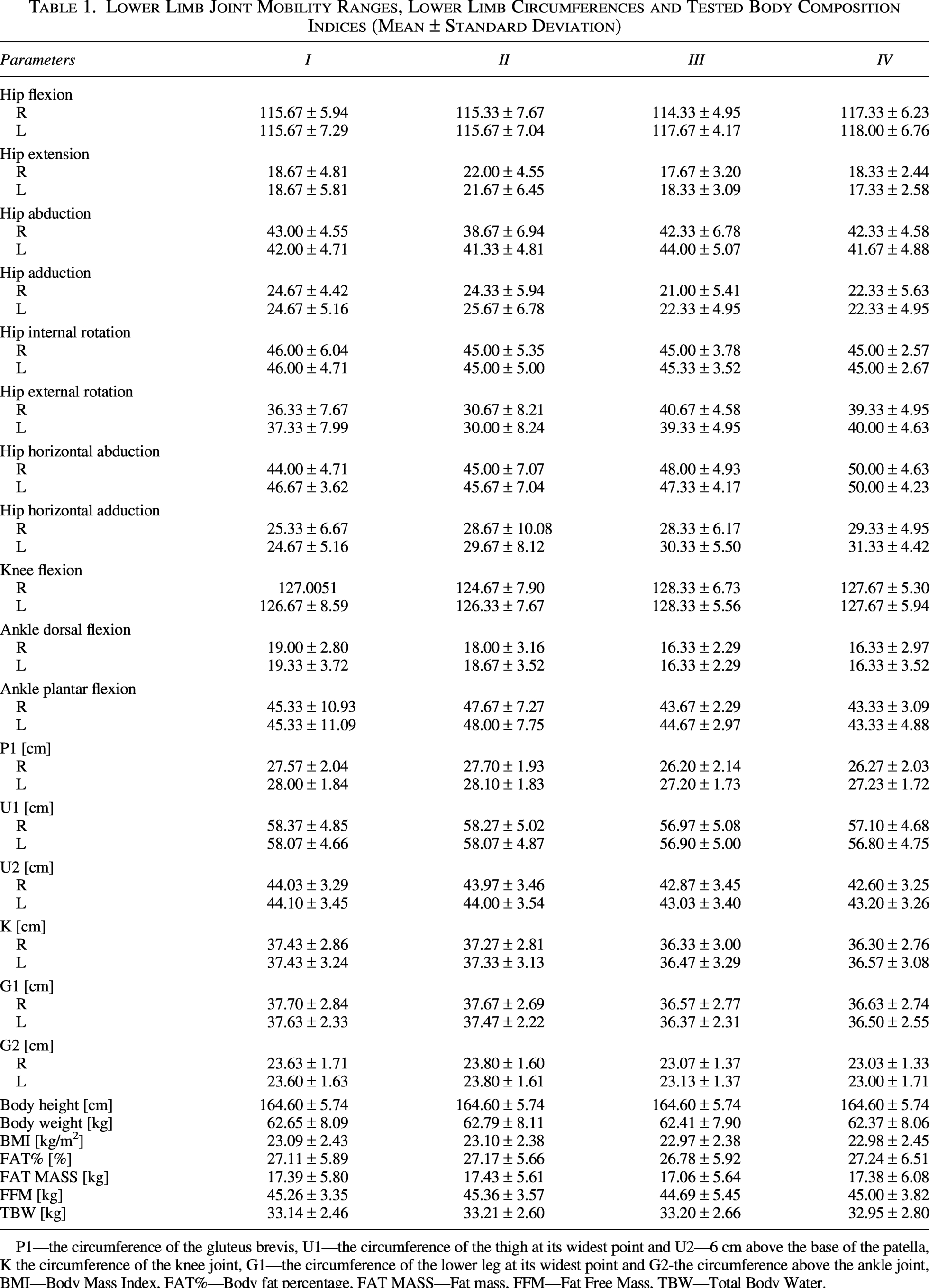
P1—the circumference of the gluteus brevis, U1—the circumference of the thigh at its widest point and U2—6 cm above the base of the patella, K the circumference of the knee joint, G1—the circumference of the lower leg at its widest point and G2-the circumference above the ankle joint, BMI—Body Mass Index, FAT%—Body fat percentage, FAT MASS—Fat mass, FFM—Fat Free Mass, TBW—Total Body Water.
Statistical analysis of mean changes showed statistically significant differences for the analysis of variance for repeated measurement of the range of motion of the lower limbs.
Statistical analysis of mean changes in the range of motion values showed significant decrease in: right (F = 5.80, p < 0.05, η2 = 0.29) and left (F = 3.41, p < 0.05, η2 = 0.20) hip joint extension; right (F = 3.63, p < 0.05, η2 = 0.10) hip joint horizontal abduction; horizontal adduction of the right (F = 29.74, p < 0.05, η2 < 0.05) and left (F = 4.03, p < 0.05, η2 = 0.22) hip joint; dorsiflexion of the right (F = 3.45, p < 0.05, η2 = 0.12) and left (F = 3.83, p < 0.05, η2 = 0.21) ankle joint and also increase in: right (F = 7.08, p < 0.05, η2 = 0.36) and left (F = 7.56, p < 0.05, η2 = 0.35) hip external rotation (Table 2). Differences between individual studies are listed in Table 3.
Analysis of Variance for Repeated Measurement of Lower Limb Mobility Ranges, Lower Limb Circumferences and Body Composition—F-Test Value and p-Level of Significance
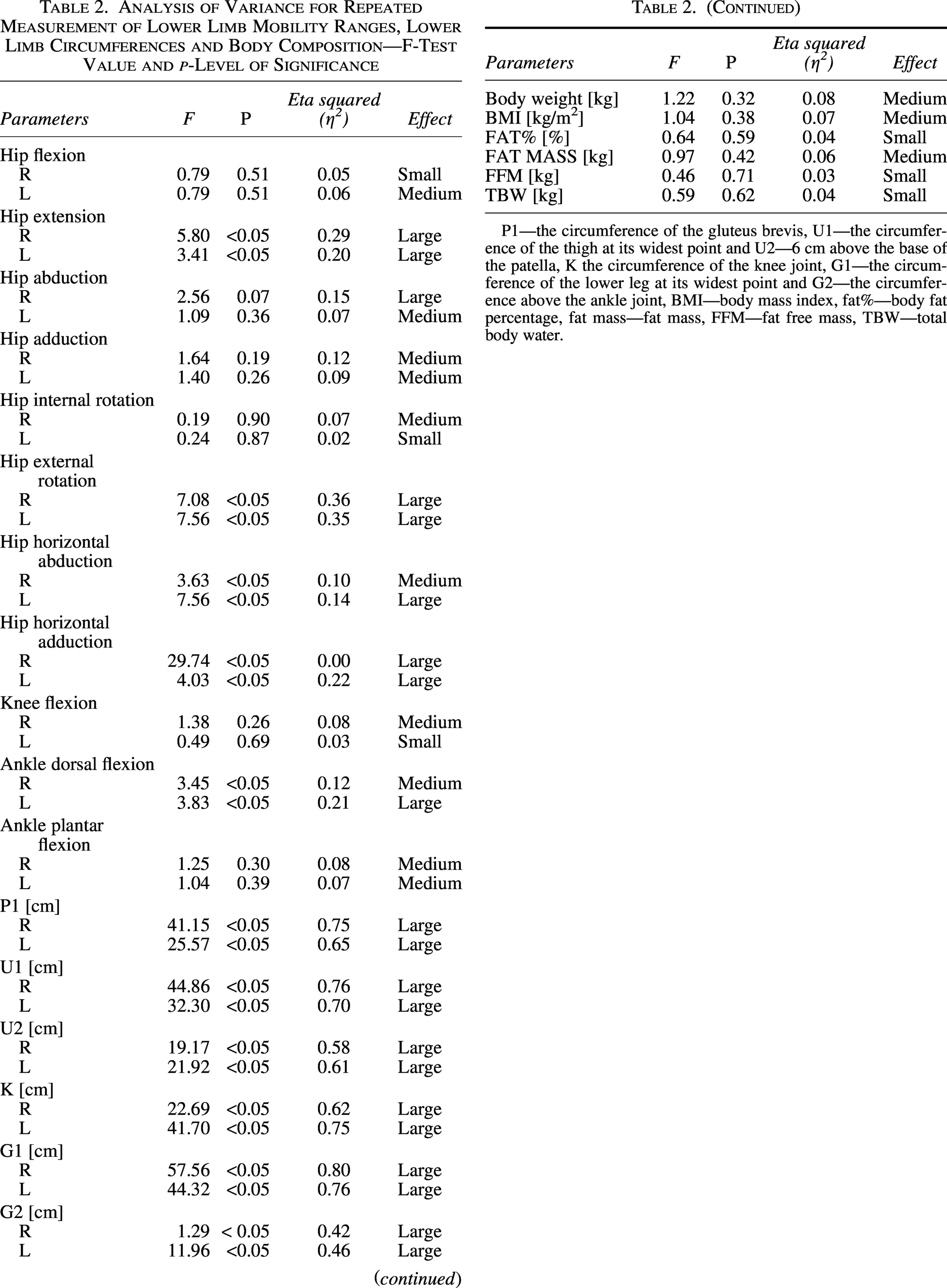
P1—the circumference of the gluteus brevis, U1—the circumference of the thigh at its widest point and U2—6 cm above the base of the patella, K the circumference of the knee joint, G1—the circumference of the lower leg at its widest point and G2—the circumference above the ankle joint, BMI—body mass index, fat%—body fat percentage, fat mass—fat mass, FFM—fat free mass, TBW—total body water.
Post hoc Test Values for the Studied Lower Limb Mobility Ranges and Lower Limb Circumferences
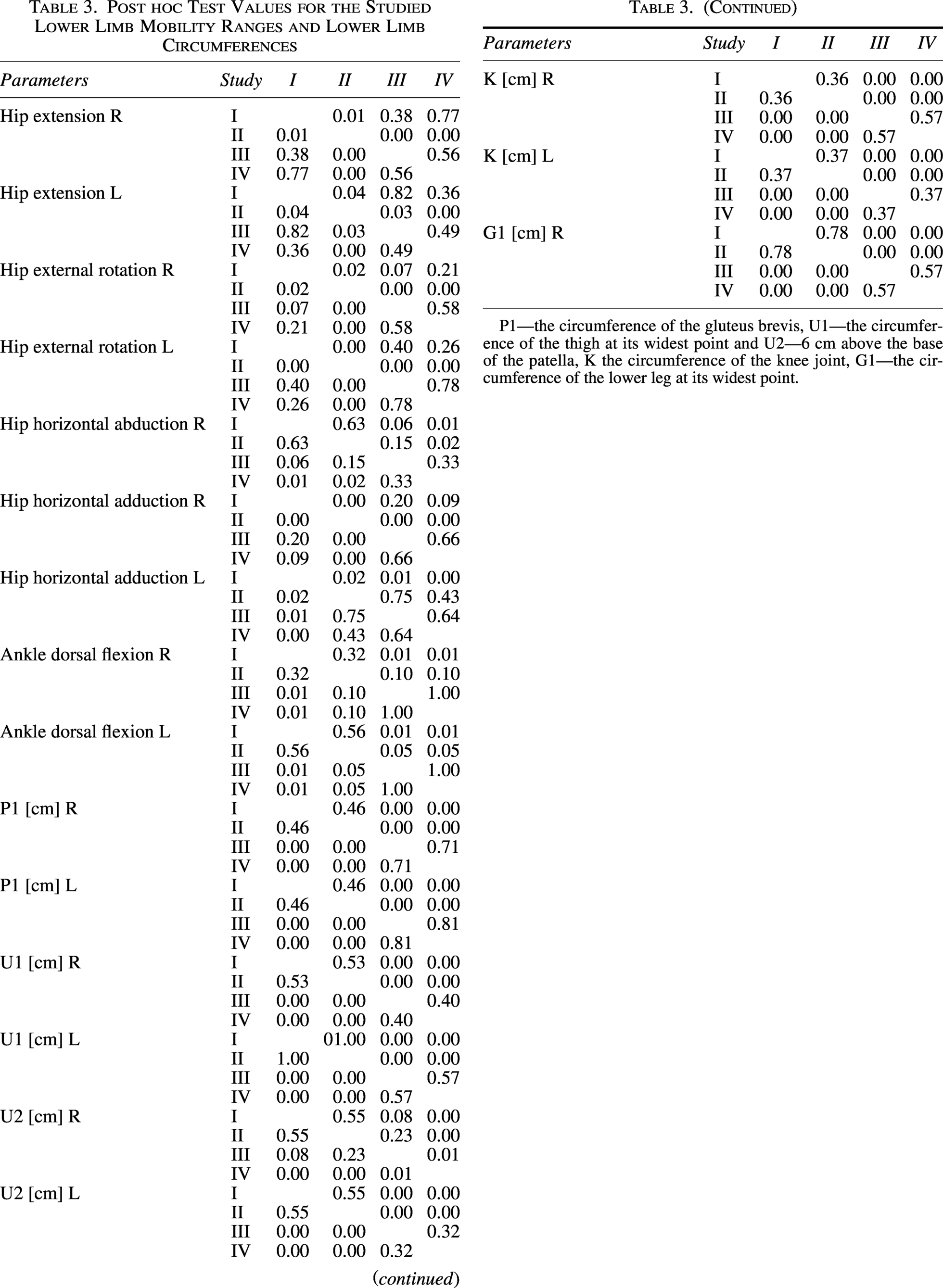
P1—the circumference of the gluteus brevis, U1—the circumference of the thigh at its widest point and U2—6 cm above the base of the patella, K the circumference of the knee joint, G1—the circumference of the lower leg at its widest point.
Statistical analysis of changes in mean values of circumferences showed significant decrease at all tested levels: P1 right (F = 41.15, p < 0.05, η2 = 0.75) and left (F = 25.57, p < 0.05, η2 = 0.65); U1 right (F = 44.86, p < 0.05, η2 = 0.76) and left (F = 32.30, p < 0.05, η2 = 0.70); U2 right (F = 19.17, p < 0.05, η2 = 0.58) and left (F = 21.92, p < 0.05, η2 = 0.61); K right (F = 22.69, p < 0.05, η2 = 0.62) and left (F = 41.70, p < 0.05, η2 = 0.75); G1 right (F = 57.56, p < 0.05, η2 = 0.80); and left (F = 44.32, p < 0.05, η2 = 0.76); G2 right (F = 10.29, p < 0.05, η2 = 0.42); and left (F = 11.96, p < 0.05, η2 = 0.46) (Table 2). According to conventional thresholds for eta squared (η2), values of 0.01–0.05 indicate a small effect, 0.06–0.13 a moderate effect, and values ≥0.14 a large effect, as reflected in the results presented in Table 2 (Table 4). Differences between individual studies are listed in Table 3. Statistical analysis of mean changes did not show statistically significant differences for analysis of variance for repeated measurements of body composition analysis (Table 2).
The Mean and Standard Deviation Changes per Subject for Statistical Signifance Parameters
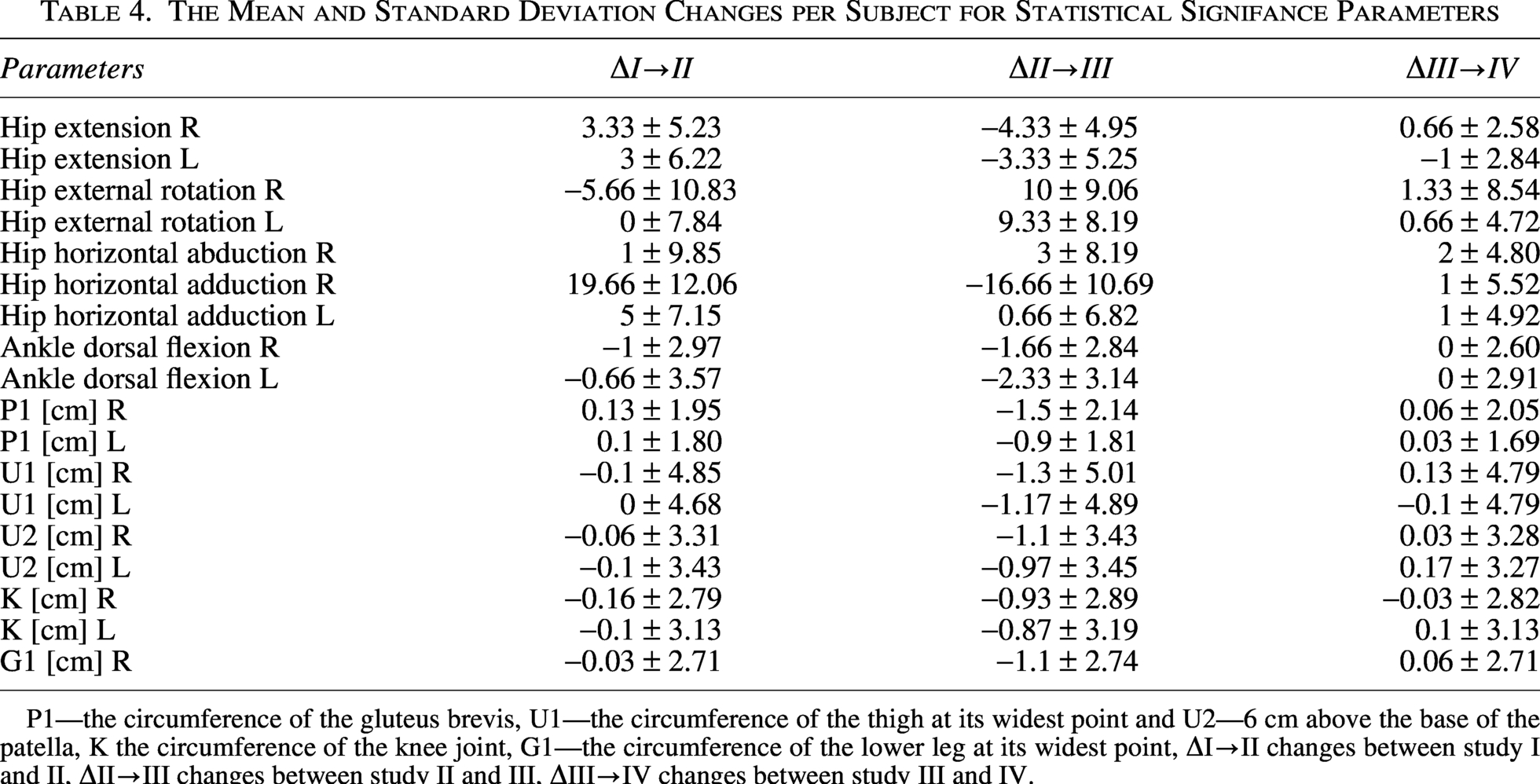
P1—the circumference of the gluteus brevis, U1—the circumference of the thigh at its widest point and U2—6 cm above the base of the patella, K the circumference of the knee joint, G1—the circumference of the lower leg at its widest point, ΔI→II changes between study I and II, ΔII→III changes between study II and III, ΔIII→IV changes between study III and IV.
The present findings indicate that pressotherapy induces statistically significant changes in selected parameters of lower limb function; however, the magnitude and clinical relevance of these changes differ across outcome measures. For joint range of motion, the observed effects were predominantly small to moderate, as reflected by partial eta squared values ranging from 0.10 to 0.36. Although statistically significant, the decreases noted in hip extension, horizontal abduction and adduction, and ankle dorsiflexion suggest that pressotherapy does not meaningfully enhance joint mobility in healthy individuals. The increases in hip external rotation, which demonstrated moderate effect sizes, may reflect transient neuromuscular or soft tissue responses to cyclic compression rather than structural adaptations of the joint. In contrast, the reductions in limb circumferences were associated with large effect sizes (η2 = 0.42–0.80), indicating a robust and clinically relevant response to pressotherapy in terms of fluid displacement and edema reduction. The absence of significant changes in body composition further supports the interpretation that pressotherapy primarily affects extracellular fluid distribution rather than inducing alterations in muscle or fat mass. Collectively, these results suggest that while pressotherapy is highly effective in reducing limb volume, its influence on joint mobility in healthy populations is limited and of questionable functional significance, underscoring its role as a supportive rather than mobility-focused intervention.
Discussion
The effect of pressotherapy on the range of motion of the lower limbs
The results show that the range of motion of the lower limbs changes statistically significantly under the influence of pressotherapy treatments. Looking at the results, one can observe a decrease in the range of motion, i.e., extension of the right and left hip joint, horizontal abduction of the right hip joint, horizontal adduction of the right and left hip joint, flexion of the right and left ankle joint and an increase in the range of motion of rotation of the right and left hip joint. The obtained results may suggest that pressotherapy does not significantly increase joint mobility in healthy people without existing health problems in this area (e.g., swelling, congestion, circulatory problems).
The purpose of ROM measurement is not only to observe the extent of inhibition but also to identify the factors that restrict joint movement and to evaluate the effectiveness of treatment and training. The range of motion of the limbs ROM varies from person to person and can be influenced by various factors, including age, gender, physical structure, such as BMI, professional and recreational activity and testing procedures.10–13
Greater lean body mass is associated with reduced shoulder external rotation and horizontal extension, but increased ROM for wrist flexion and hip adduction. Conversely, increased body fat percentage has been associated with reduced shoulder external rotation, shoulder horizontal flexion and elbow flexion and extension. Negative correlations between body fat and several joint movements may be due to physical obstruction—i.e., fat tissue being trapped between the bones that make up the joint. 11
Average weight individuals have significantly greater active range of hip flexion, extension, and abduction than overweight and obese individuals. Higher BMI was positively associated with reduced trunk flexion and rotation, hip extension, external rotation, and ankle ROM. 14
The joint testing position can greatly affect the available ROM due to the length of the opposing muscle. 15 Muscles at one joint cross one joint and thus only affect movement at that joint. Shortening of a single joint muscle affects passive range of motion and active range of motion. There is limited agreement on the number of repetitions or warm-up protocols that should be used before assessing ROM. Evidence from stretching has shown increased mobility, stretch tolerance, and decreased passive torque during acute stretching training after only a few stretch repetitions.16–19 This phenomenon occurs during ROM assessment. Therefore, differences in the measurement protocol regarding measured repetitions and warmup exercises can lead to differences in measurement results of up to 6 degrees. 20
There are studies that report a beneficial effect on increasing the range of motion in the treated joints, but these studies concern people with various problems: axillary web syndrome after breast cancer 21 , total hip arthroplasty 22 , ACL injury 23 , upper and lower extremity lymphedema. 24 In our studies, we did not observe many significant increases in mobility in the examined joints, but it should be taken into account that at the beginning these parameters were correct and the mobility in the examined joints was not limited in any way.
Changes in the range of motion with a statistical significance close to p < 0.05 showed a large effect size—changes that were important from a clinical point of view. However, differences that did not show a statistically significant difference were correlated with a small effect and low clinical value.
The effect of pressotherapy on lower limb circumferences
The analysis of lower limb circumferences showed a significant reduction in the circumferences of the buttock, thigh, knee, calf, and ankleshin area after a series of pressotherapy treatments. Differences were observed in the measurement of lower limb circumferences before and after the series of treatments at the measurement level of P1 right (1.5 cm) and left (0.9 cm), U1 right (1.3 cm) and left (1.2 cm), U2 right (1.1 cm) and left (1 cm), K right (0.9 cm) and left (0.9 cm), G1 right (1.1 cm) and left (1.1 cm), G2 right (0.7 cm) and left (0.7 cm). This effect can be attributed to the reduction of fluid retention and reduction of lymphatic edema, which is one of the main applications of pressotherapy. 25
Studies by Muluk et al. (2013) using pneumatic compression devices have shown a positive effect on reducing lymphedema. 26 Chleboun et al. (1995) demonstrate that IPC is effective in recovery from short-term eccentric training, which also reduces pneumatic compression induced limb swelling and stiffness following intense exercise. 27 Szuba et al. (2002) demonstrate that IPC significantly reduces mean edema volume and is well tolerated with no detectable adverse effects on skin elasticity or joint range of motion. 28 Interestingly, recent work suggests that negative pressure may accelerate recovery of strength and power and reduce pain from muscle damaging exercises. 29
The obtained results are consistent with previous studies, which indicate the effectiveness of pressotherapy in reducing the circumference of the lower limbs in patients with lymphedema22,30,31 and athletes undergoing intensive training. 4 Won et al. (2021) evaluated the effect of IPC on its effect on relieving venous symptoms in healthy participants. This was a study to investigate the effects of the treatments in healthy volunteers who usually stand during work and complain of leg pain and swelling. Leg pain and circumference were significantly improved. IPC was found to be effective in reducing leg pain and circumference more than natural rest in healthy adults with long-term standing work, without causing adverse events. 32 These results were confirmed by Kim et al. (2022) in their study, where they compared the effects of medical compression stockings (MCS) and IPC in workers with prolonged standing (>8 hours/day). Leg pain and swelling after prolonged standing in adults were safely and effectively alleviated by both IPC alone and IPC with MCS. 33
Interestingly the measurement of circumference are often performed by physically active people (including professional athletes) in order to observe the increase or decrease in muscle mass. This is closely related to a sports lifestyle (mainly bodybuilding and strength sports). These kind of testing can verify whether the training plan bring the intended effect consistent with the characteristics of the sport discipline. In addition, a decrease in limb circumference is correlated with reduce the severity and duration of delayed onset muscle soreness in athletes suggesting its effectiveness in alleviating muscle soreness and better preparing to future competition. 34
The measurement of circumference is also used, among others, in orthopedic injures (sprains, dislocations, and any injures involving swelling or muscle athropy). From a clinical point of view, the limb circumference decrease during the physiotherapy process cause improve range of motion in joints, muscle strength, pain intensity, and functional status. This changes provide to faster restoring physical fitness after injury. Therefore, patients should undergo all treatments (including pressotherapy) to reduce circumference (causing by swelling e.g.,). 35
Changes in the all lower limb circumference showed a large effect size. That changes can be considered as important from a clinical point of view.
The effect of pressotherapy on body composition
Studies conducted using the Tanita BC-418 MA body composition analyzer showed that a series of pressotherapy treatments did not contribute to a significant improvement in body composition parameters. The percentage of body fat (FAT%), FFM and total muscle mass remained at a similar level before and after the treatments. These results suggest that pressotherapy, although effective in reducing limb circumference, may not have a significant effect on changes in body composition in healthy individuals in the short term.
Socha et al. (2010) indicate that electrical bioimpedance is important for assessing the effects of a diet, controlling the effectiveness of the weight loss process or assessing the effects of sports training. 36 Studies conducted by Stańczyk et al. (2013) show that physical activity proposed by a sports school does not improve the nutritional status of 13–14-year old girls and boys, who have a significant increase in the content of body fat. 37 Janiszewska et al. (2013) prove that 3-month health training can be a tool for improving the body composition of overweight and obese people. 38 In the study conducted by Piotrowska et al. (2021) containing the effect of a single vibrotherapy treatment in women undergoing the treatment, no significant changes were found except for the percentage of water content. 39 Witkoś et al. (2021) reported that after 4 weeks from the introduction of the diet and muscle electrostimulation training, significant changes were observed in the reduction of body weight and the decrease in the percentage of adipose tissue, while the level of muscle tissue remained at the same level. 40 In our study, we did not control the diet of the participants (one of the inclusion criteria was only not changing the diet before and during the project). Introducing a different diet than before the project could have a multidirectional effect especially in the case of body composition analysis, but also in the case of circumferences and indirectly in the case of ranges of motion of the examined joints.
The above evidence proves that the pressotherapy procedure itself does not cause changes in body composition, so it can be successfully used in various cases, such as physiotherapy od posttraumatic patients or biological regeneration of athletes without the risk of changes in body composition that could affect the proper process of recovery to health or regeneration.
Changes in body composition showed small or medium size effect which may indicate low clinical value.
Summary
Despite promising results in terms of reducing lower limb circumference, the study has its limitations. The number of participants was relatively small, which may affect the generalization of the results. In addition, the study included only young, healthy women, which limits the possibility of relating the results to other demographic groups. It is also worth noting that studies on the effects of pressotherapy on healthy people are relatively few. There is a need for more research in this area to better understand the potential benefits and limitations of pressotherapy. In the future, it is worth conducting studies on larger groups and diverse populations to confirm the obtained results and examine possible differences in the effectiveness of pressotherapy depending on age, gender and health status. There are many gender-related factors that may be important for the indicators studied: differences in body build, testosterone levels, body composition, neuronal activation, coactivation of antagonist groups, or even different types of activity during childhood. In people with an existing problem, however, the effect of the treatment is often noticed more clearly or occurs more quickly. Further studies should involve longer observation, and perhaps the pressotherapy procedure itself should be extended.
Practical Applications
Based on the conducted studies, it can be concluded that pressotherapy has a significant effect on reducing lower limb circumference in young, healthy women. The lack of significant improvement in joint mobility and body composition suggests that the benefits of pressotherapy may be more visible in the context of reducing swelling than in other physiological areas. Regular use of this method can bring significant benefits in the context of health prevention and supporting regenerative processes.
Conclusions
A series of pressotherapy sessions did not improve lower limb range of motion or body composition indices; however, it did reduce circumferences at all levels of the lower limbs. Long-term use of pressotherapy can help maintain healthy fluid levels, improve circulation, and improve overall physical fitness.
Authors’ Contributions
Conceptualization, B.P. and O.K.; Data curation, O.K.; Formal analysis, B.P. and S.P.; Investigation, B.P. and O.K.; Methodology, B.P. and O.K.; Supervision, B.P. and S.P.; Writing—original draft, B.P. and O.K.; Writing—review and editing, B.P. All authors have read and agreed to the published version of the article.
Footnotes
Ethical Committee Approval (Code Number)
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethical Committee of the District Medical Chamber in Krakow: 64/KBL/OIL/2024 of 04/07/2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
The publication is financed within the program of the Minister of Science under the name “Regional Excellence Initiative” in the years 2024–2027, project number RID/SP/0027/2024/01 in the amount of PLN 4,053,904.00.