
Abstract
Despite proven efficacy in preventing HIV, the global uptake of pre-exposure prophylaxis (PrEP) remains limited and uneven, particularly among men who have sex with men (MSM). A meta-analysis by Zhao et al. reveals that only 20% of PrEP-eligible MSM have ever used the medication, with stark disparities across regions and income levels. While uptake has increased over time, significant barriers persist, especially in low- and middle-income countries (LMICs). These barriers include financial constraints, limited health care infrastructure, provider knowledge gaps, and pervasive stigma, which together impede equitable access to PrEP. In regions such as sub-Saharan Africa, Asia, and Latin America, MSM face challenges related to health care access, while younger MSM and marginalized groups, including transgender individuals, are particularly underserved. This viewpoint calls for global strategies that address these inequities through targeted, evidence-based interventions that focus on reducing systemic barriers and incorporating intersectional approaches. To scale up PrEP access and ensure equitable HIV prevention, multilevel strategies are necessary, involving policy changes, provider training, community-led initiatives, and youth-centered outreach. Addressing the financial, structural, and social determinants of health is essential for bridging these gaps and ensuring that PrEP fulfills its potential as a global tool for HIV prevention.
Keywords
Introduction
The meta-analysis by Zhao et al. (2025), which synthesized data from 50 studies involving 96,151 participants, underscores a critical gap in global HIV prevention: only about 20% of PrEP-eligible men who have sex with men (MSM) have ever used HIV pre-exposure prophylaxis (PrEP). While uptake has increased over time, it remains uneven across different regions and national income levels. MSM in low- and middle-income countries (LMICs), including China, report particularly low uptake, despite expanding awareness campaigns and policy initiatives. It is important to note that China is considered an LMIC in this analysis.
Moreover, other LMICs in sub-Saharan Africa, Asia, and Latin America face substantial barriers to PrEP access, contributing to slow uptake and uneven coverage (Admassu et al., 2024; Batista et al., 2024; Perez-Urbano et al., 2024; Vega-Ramírez et al., 2022; Were et al., 2021). In sub-Saharan Africa, Admassu et al. identify barriers to PrEP use and adherence among adolescent girls and young women, reflecting structural, funding, and health-system constraints that impede sustained PrEP use (Admassu et al., 2024). In Latin America, Vega-Ramírez et al. show limited PrEP awareness and provider knowledge among physicians in Brazil and Mexico, while PrEP uptake remains uneven across the region (Vega-Ramírez et al., 2022) implementation model demonstrates that rollout remains slow in LMIC health systems due to regulatory, logistics, and supply-chain challenges despite policy endorsement (Were et al., 2021). Research in the Brazilian Amazon by Batista et al. (2024) highlights provider information gaps and the need to decentralize PrEP services, with social media playing a vital role in shaping awareness and demand Batista et al., 2024). Community insights from Tshwane, South Africa, further reveal uptake gaps among transgender people and MSM driven by community-level barriers and health care access issues (Perez-Urbano et al., 2024). Collectively, these studies corroborate regionally diverse yet overlapping barriers to PrEP access in LMICs (Admassu et al., 2024; Batista et al., 2024; Perez-Urbano et al., 2024; Vega-Ramírez et al., 2022; Were et al., 2021). These disparities suggest that PrEP implementation is fragmented, with structural, financial, and systemic barriers hindering equitable access to HIV prevention. This viewpoint emphasizes the need for global strategies that address these inequities, focusing on targeted, evidence-based approaches to ensure effective HIV prevention among MSM worldwide, particularly in resource-constrained settings.
PrEP’s Promise Versus Implementation
The efficacy of PrEP is well established: when taken as prescribed, it can reduce HIV incidence among MSM by up to 97% (Molina et al., 2017). Both on-demand and daily regimens have been shown to be effective in controlled trials. However, global uptake is considerably lower than what would be expected given its proven benefits. Recent pooled estimates suggest that approximately 16.04% of eligible MSM currently use PrEP (Huang et al., 2023). While uptake has grown in recent years, persistent gaps point to challenges in translating clinical effectiveness into widespread public health impact. Barriers such as geographic location, health system structure, and socioeconomic conditions remain key determinants of access and uptake.
Real-world uptake and persistence of PrEP among MSM show significant variability and often fall short of potential, despite strong evidence of efficacy (Wang et al., 2022). This gap persists because systematic reviews highlight that uptake and adherence are shaped by a complex range of individual, interpersonal, and health-system factors, alongside broader social determinants (Wang et al., 2022). For example, studies from West Africa identify socio-behavioral factors like stigma and trauma that adversely affect PrEP use (Eubanks et al., 2022), while experiences in Cameroon and Benin reveal ongoing challenges in scaling PrEP, indicating a need for sustained, targeted support (Diabaté et al., 2023; Ndenkeh et al., 2022). Conversely, Slovenia’s well-resourced healthcare system demonstrates how systemic qualities like coverage can improve outcomes (Ambrožič et al., 2024).
To address these disparities, initiatives such as community-centered mobile PrEP programs in the U.S. target geographic and racial disparities among Black and Latino MSM (Butts et al., 2023). Furthermore, decentralized care models are emerging as viable strategies to enhance engagement for those facing stigma in conventional clinics (Charest et al., 2021). Critically, regional studies show marked differences in modality preferences among MSM in countries like Brazil, Mexico, and Peru, emphasizing the need to offer preferred options (Cameron et al., 2024; Torres et al., 2023). This principle also applies in India, where local preferences significantly shape PrEP adoption (Cameron et al., 2024). Additionally, evidence of risk compensation highlights the need for integrated prevention messaging and STI screening alongside PrEP programs (Dyer, 2022; Manguro et al., 2022).
Therefore, to bridge promise and practice, programs should diversify delivery modalities and adapt to local preferences. Specifically, evidence supports offering various PrEP options, such as daily oral, on-demand, and long-acting injectable PrEP, to enhance uptake and persistence (Cameron et al., 2024; Torres et al., 2023). However, successful implementation of these flexible options requires attention to supply chain management and provider education (Brink et al., 2022; Doyle et al., 2023). Here, investment in long-acting injectable PrEP is critical for addressing adherence challenges, particularly for individuals who struggle with daily regimens (Rogers et al., 2023; Pilgrim et al., 2022). Concurrently, digital health strategies, including mobile PrEP programs, have shown promise in improving access among underserved populations (Butts et al., 2023; Charest et al., 2021). Ultimately, successful scale-up depends on aligning implementation with local health-system capabilities and equity concerns, ensuring reliable supply chains and targeted outreach to marginalized MSM communities (Ambrožič et al., 2024; Brink et al., 2022; Butts et al., 2023; Diabaté et al., 2023; Ndenkeh et al., 2022).
Financial Barriers
Affordability remains a critical factor influencing PrEP uptake. In high-income countries like the United States, France, and Brazil, the availability of government subsidies, health insurance coverage, and the integration of PrEP into sexual health services has facilitated broader access. However, there are significant differences in how each country’s financial and health care systems impact PrEP access. In the United States, PrEP is often covered under insurance plans, but access can be limited by high out-of-pocket costs for those without adequate insurance or in regions with fewer health care resources (Billioti de Gage et al., 2022). In France, the national health system subsidizes PrEP and integrates it into sexual health services, allowing for more equitable access across diverse populations (Luz et al., 2018). Brazil’s public health system also provides free PrEP to those at high risk, but challenges remain in ensuring distribution to underserved regions, especially in rural areas . By contrast, in many LMICs, PrEP access depends largely on donor-funded pilot programs or self-financed purchases, which limit its reach to at-risk populations. This stark contrast highlights how financial barriers, though surmountable, are deeply intertwined with national health system structures and policies.
Health Care System Factors
Health care systems significantly shape PrEP uptake. Evidence shows that provider training, clinical guidelines, and service delivery structures either facilitate or hinder access to PrEP. In high-income countries, the integration of PrEP into established health care frameworks often leads to improved uptake, but challenges such as inconsistent prescribing practices and gaps in provider knowledge persist (Coukan et al., 2023). In the United States, disparities in health care access due to regional differences, insurance coverage, and provider education can hinder PrEP initiation, particularly in underserved communities (Eubanks et al., 2022). France has made strides by creating clear clinical guidelines for PrEP and training providers on its use, but stigma within health care settings can still affect engagement (Azzi et al., 2024). In Brazil, health care providers face challenges related to training and awareness, especially in remote areas, despite the country’s robust public health system. In LMICs, PrEP access is often constrained by limited health care infrastructure, inadequate provider training, and restrictive eligibility criteria, which can exclude individuals who would benefit most from PrEP (Haines et al., 2021). These disparities illustrate how health care system factors, compounded by broader systemic inequities, shape whether PrEP services are accessible and acceptable to MSM in different global contexts.
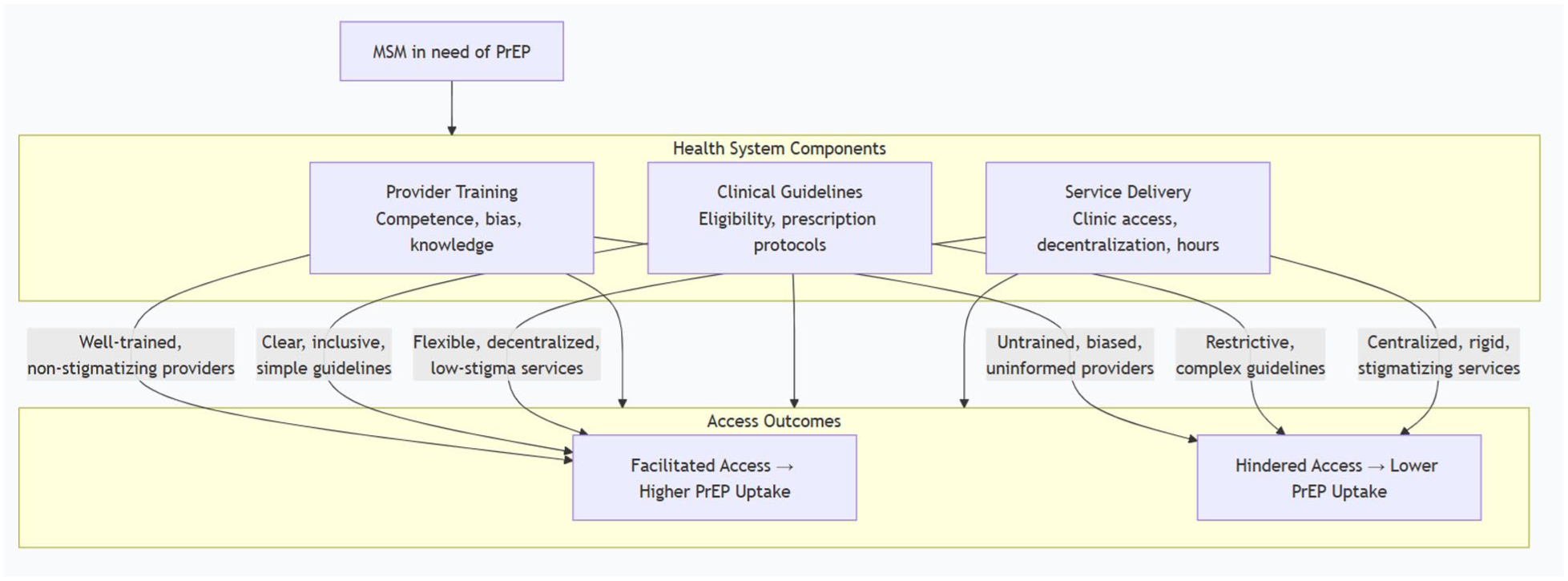
How Health Systems Shape PrEP Access for MSM population.
Stigma and Social Context
Stigma is a consistent barrier identified across studies. Negative perceptions of PrEP sometimes framed as promoting promiscuity can discourage individuals from seeking prescriptions and may affect disclosure of sexual identity in health care encounters. Younger MSM, in particular, may experience overlapping stigma related to age, sexuality, and gender expression, further limiting engagement with PrEP services (Azzi et al., 2024; Miller et al., 2022). Addressing stigma, both within health care and in society more broadly, remains essential to improving uptake and adherence.
Stigma surrounding PrEP among MSM is multidimensional, internal, anticipated, and experienced—and embedded in broader social contexts, consistently undermining PrEP uptake, adherence, and persistence across various settings (Babel et al., 2021; Farley et al., 2024; Nagai et al., 2023; Ort & Bardy, 2024; Zhang & Liu, 2022). Healthcare discrimination and intersecting stigmas based on race and sexual orientation significantly shape access to PrEP information and services; for instance, Black MSM report experiencing discrimination, and disclosure of same-sex behavior to healthcare providers can improve awareness, although stigma remains a barrier in countries such as Ghana and Senegal (Babel et al., 2021; Nagai et al., 2023; Rosen et al., 2023). Social networks can perpetuate PrEP stigma (e.g., associating PrEP with promiscuity) while also facilitating information diffusion and peer support that promote uptake, as observed in contexts like the Philippines and Brazil (Restar et al., 2022; Santos et al., 2022). Interventions that encompass societal campaigns, community-based approaches, and patient-centered delivery models, such as telehealth and mobile PrEP initiatives, have shown potential in mitigating stigma and enhancing PrEP uptake and persistence (Adeagbo, 2024; Assaf et al., 2021; Chamberlin et al., 2023; Nagai et al., 2023; Wang et al., 2022).
The Youth Gap
Zhao et al. (2025) also highlight lower PrEP use among younger MSM, a population disproportionately affected by new HIV infections. Factors such as limited youth-friendly services, underdeveloped digital health platforms, and prevention messaging that does not resonate with younger demographics may contribute to this gap. Tailored strategies that prioritize accessibility, confidentiality, and relevance to young people’s experiences may be needed to address this disparity.
The Youth Gap in PrEP use refers to the persistent underutilization of HIV PrEP among young men who have sex with men (YMSM), despite their willingness and awareness of its benefits. Research consistently reveals a significant mismatch between the willingness to use PrEP and actual uptake, particularly due to barriers such as stigma, financial constraints, and lack of youth-friendly services (Buffel et al., 2021; Liu et al., 2024). Factors such as risk perception, social discrimination, and confidentiality concerns also contribute to the gap, creating a complex interplay of individual and structural barriers to PrEP access for this demographic (Bhatta et al., 2022; Dijk et al., 2021).
The gap is evident across different regions, including Europe, the United States, Asia, and Africa. For example, in China, a study found that although many MSM were willing to use PrEP, uptake remained low due to multi-dimensional barriers (Guan et al., 2023). Similarly, in South Africa, structural and social stigma hindered daily PrEP uptake among MSM (Perez-Urbano et al., 2024). However, regional studies also highlight the potential for addressing these challenges through tailored interventions, such as youth-friendly PrEP services, stigma reduction, and digital health strategies (Charest et al., 2021; Hamilton et al., 2021).
Promising strategies for closing the Youth Gap involve decentralizing PrEP delivery into primary care and community settings, enhancing knowledge through educational programs, and expanding dosing options like long-acting PrEP to address adherence issues (Balasubramanian et al., 2022; Wu et al., 2024). Additionally, peer-led programs and provider education to reduce stigma are critical for increasing acceptance among youth (Pulerwitz et al., 2024; Sevelius et al., 2021). Longitudinal research to track awareness, willingness, and uptake, alongside investments in infrastructure for youth-friendly clinics, is essential for furthering PrEP adoption (Liu et al., 2024; Newman et al., 2023).
Intersectional Approaches to Strengthen PrEP Access and Adherence
Equity-focused HIV prevention requires population-specific, evidence-informed strategies that address the unique needs of groups such as adolescent girls and young women (AGYW), Black women, sex workers, transgender women, and MSM, while also incorporating intersectionality and stigma reduction (Latka et al., 2023; Rousseau et al., 2024). For AGYW, prioritizing PrEP delivery alongside reproductive health services and long-acting products is essential, with an emphasis on youth-friendly and peer-led outreach (Rousseau et al., 2024). Black women benefit from prevention programs addressing social determinants and health care barriers, while sex workers require community-led services that expand access to PrEP and ART (Obioma et al., 2024; Witte et al., 2022). Transgender women need gender-affirming care integrated with HIV prevention, and MSM can benefit from differentiated outreach, including digital tools and community-led models to optimize PrEP uptake (Peng et al., 2022; Rucinski et al., 2022). Across all groups, implementing stigma reduction strategies and legal supports is critical to sustaining equitable access to HIV prevention (Spence et al., 2022; Stangl et al., 2023). These strategies are directly related to PrEP use by addressing the specific barriers and needs of each group, thereby improving uptake and adherence to PrEP and other HIV prevention methods (Claassen et al., 2021; Smith et al., 2023).
Multilevel Strategies for Scaling Global PrEP Uptake
Global PrEP uptake requires explicit, multilevel, and culturally tailored implementation strategies that address barriers at the individual, provider, and clinic levels to improve accessibility and adherence (Estcourt et al., 2023; Johnson et al., 2022; Wang et al., 2022). These strategies align with calls for scalable PrEP delivery models (Bavinton & Grulich, 2021; Rousseau et al., 2021) and evidence suggesting that diverse settings necessitate a comprehensive approach (Estcourt et al., 2023). To broaden PrEP’s reach, delivery models should be diversified by integrating PrEP into family planning, leveraging community-based and mobile delivery, adopting pharmacy-led models, and utilizing telemedicine (Gotsche et al., 2022; Rousseau et al., 2021). Provider training must be culturally sensitive, co-produced, and include guidance on non-daily dosing to address knowledge gaps and support both initiation and persistence (Estcourt et al., 2023; Johnson et al., 2022; Kayesu et al., 2022). In addition, targeted, population-specific strategies for groups such as adolescent girls and young women (AGYW), Black women, sex workers, transgender women, and MSM are essential, with an emphasis on peer networks, stigma reduction, and accessible service delivery (Amogne et al., 2022; D’Angelo et al., 2021; Joshi et al., 2023; Patel et al., 2022). Policy and financing actions, such as reducing costs, enabling diverse prescribers, and integrating PrEP into existing services, are vital for addressing systemic barriers and enabling global scale-up (Bavinton & Grulich, 2021; Comer & Fernández, 2022; Espinosa et al., 2021).
Global Disparities and Equity Considerations
The uneven distribution of PrEP raises questions about equity in HIV prevention. While uptake has increased in high-income countries, MSM in LMICs often report limited access despite high levels of need. As global health institutions set targets for HIV prevention, attention to equity across geography, income, and demographic subgroups will be essential to ensure that PrEP fulfills its potential as a global intervention. Significant global disparities in PrEP uptake and persistence among men who have sex with men (MSM) persist along lines of race/ethnicity, migrant status, language, geography, and stigma. Syntheses confirm that awareness, willingness, and access remain suboptimal and unevenly distributed worldwide, despite evidence of PrEP’s effectiveness (Huang et al., 2023; Sun et al., 2022). These inequities are structurally driven by policy, financing, and health-system factors, which create barriers such as insurance gaps and fragmented service delivery (Coleman et al., 2024; Estcourt et al., 2021). Within care continua, disparities are pronounced for Black, Hispanic/Latino, and migrant MSM, who face lower uptake and retention due to structural racism, discrimination, and cultural or language barriers (Babel et al., 2021; Bonacci et al., 2021; Schumacher et al., 2021).
Conclusion
Although PrEP remains a highly effective tool for HIV prevention, its global uptake among MSM has been modest and uneven. Zhao et al.’s (2025) findings highlight both progress and persistent gaps, especially in LMICs and among younger MSM. Moving forward, addressing cost, health care system barriers, and stigma will be essential for scaling up equitable access. While the statement touches on these challenges, it lacks concrete, evidence-informed solutions to create lasting change. For example, focusing on the licensing of innovative PrEP dosing options could help reduce costs and improve accessibility. In addition, strengthening youth-focused interventions, tackling systemic barriers, and framing PrEP implementation as an equity issue rather than just an efficacy issue can guide more inclusive strategies. Ensuring sustained policy commitment and addressing societal stigma will be crucial for bridging existing disparities and reducing HIV incidence among MSM worldwide.
Footnotes
Acknowledgements
We would like to extend our sincere gratitude to the CDC 2025 HIV Nexus for providing invaluable resources for clinicians, particularly the insights into the clinical guidance for PrEP. We are also deeply thankful to Dr. Antons Mozalevski for his contributions and for sharing the updated WHO guidance on integrated and differentiated PrEP services. Their support and expertise have been crucial to the development of this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.