
Abstract
Lifestyle Medicine (LM) and Behavioral Health (BH) are increasingly recognized as complementary, synergistic disciplines that positively impact chronic disease. Limited data exist on public awareness, perceptions, preferences, and barriers to care. This study evaluated United States (U.S.) adults’ understanding and attitudes toward LM, BH, and their integration. A cross-sectional, nationally weighted survey of U.S. adults was conducted in November 2025. Measures included health status, familiarity with LM, provider communication, access barriers, BH attitudes, and preferences for integrated care. Overall frequencies and cross-tabulations were reported. Respondents included 1,001 adults (51% women), with 71% reporting one chronic disease. Half had never heard of LM, 91% were at least somewhat interested in changing lifestyle habits, and 41% were very or extremely confident in their ability to make behavior changes. Seventy-five percent said addressing mental health was very or extremely important, with 82% responding they would be at least somewhat likely to use BH services if offered by their primary care doctor. Commonly cited barriers were cost, insurance coverage, and scheduling difficulties. Overall, U.S. adults reported a strong desire to improve health through lifestyle changes and access integrated LM and BH services within primary care.
“U.S. adults perceive LM and BH services positively and value their integration into primary care.”
Introduction
Lifestyle Medicine (LM) and Behavioral Health (BH) are evidence-based, intersecting disciplines that improve both physical and mental health outcomes when applied in practice. Lifestyle Medicine employs therapeutic lifestyle interventions to prevent, treat, and, in some cases, reverse chronic disease by focusing on six pillars: avoidance of risky substances, connectedness, regular physical activity, restorative sleep, stress management, and a whole food, plant-predominant eating patter 1 ; whereas Behavioral Health addresses mental health disorders, substance use disorders, psychosocial stressors, crisis states, and stress-related physical manifestations. 2 Increasingly, these fields are recognized as complementary, with lifestyle interventions and mental health care capable of working synergistically to improve overall health outcomes. 3
Chronic disease remains the leading cause of morbidity and mortality in the United States, 4 with lifestyle-related factors, including poor nutrition, physical inactivity, insufficient sleep, chronic stress, substance misuse, and social isolation, contributing substantially to disease burden.5,6 In response, Lifestyle Medicine has emerged as a clinically effective and cost-efficient approach to preventing and treating diet- and lifestyle-related disease.7-9 However, despite growing evidence supporting its effectiveness, LM remains underutilized across many health systems.10-12 This underutilization is multifactorial and reflects challenges including limited public awareness, restricted access to care, and financial and logistical barriers that impede engagement in lifestyle interventions. 13 These barriers are particularly pronounced among lower-income and underserved populations. 14
Evidence demonstrates that behavioral health symptoms, such as stress and anxiety, contribute significantly to chronic disease and can be positively impacted by lifestyle.15,16 As a result, integrated Lifestyle Medicine and Behavioral Health (LMBH) models are gaining increasing attention. 3 Nevertheless, national-level insights into public awareness, perceptions, preferences, and barriers remain limited.
Realizing the potential of LMBH integration requires a deeper understanding of the patient perspective, including individuals’ interests, motivations, and the practical barriers they encounter when seeking care. Attention to patients’ lived experiences is essential for effective policy development and the successful integration of care models.
This study examines United States (U.S.) adults’ knowledge of and attitudes toward Lifestyle Medicine, Behavioral Health, and their integration using a nationally representative survey of adults aged 18 years and older. By providing empirical data on public perceptions of these care models, the findings aim to inform patient-centered care design, guide resource allocation, and support strategies that accelerate the transition of these essential, evidence-based services from specialized offerings to broadly covered, accessible, and foundational components of population health.
Methods
Study Design
A cross-sectional, nationally weighted online survey was administered to adults aged 18 and older in the U.S. The survey included measures assessing lifestyle habits and the desire for change, familiarity with LM, integration of LMBH services into health care, behavioral health considerations, and access-related barriers.
Participants and Data Collection
One thousand participants were recruited from November 6-13, 2025, through the Cint Marketplace Platform. 17 Cint is a learning house of different panel providers that enables recruitment of demographic variables, including age, gender, race/ethnicity, and region, to ensure an appropriately weighted sample is ascertained.
A 34-item survey was developed and used that included Likert scales, multi-select answers, and open-ended questions. Item content included general demographic information, self-determined health status and diagnoses, familiarity, interest, and perception of LMBH, confidence in making behavior changes and finding a provider who provides these types of services, access and barriers to receiving LMBH care, and opinions on LMBH communication, services, and resources.
Analysis
Analyses were conducted using overall frequencies and cross-tabulations by demographic subgroups. Bayesian confidence interval for N = 1,000 approximated a margin of error of ±3.1 percentage points.
Ethics
This study was determined to be exempt by the Beyond Bound institutional Review Board (Category 2; DR2603JB-004) as it involved anonymous surveys regarding health care perceptions and did not collect identifiable personal information.
Results
Demographics and Health Characteristics of Respondents
Demographic Characteristics of Survey Respondents.
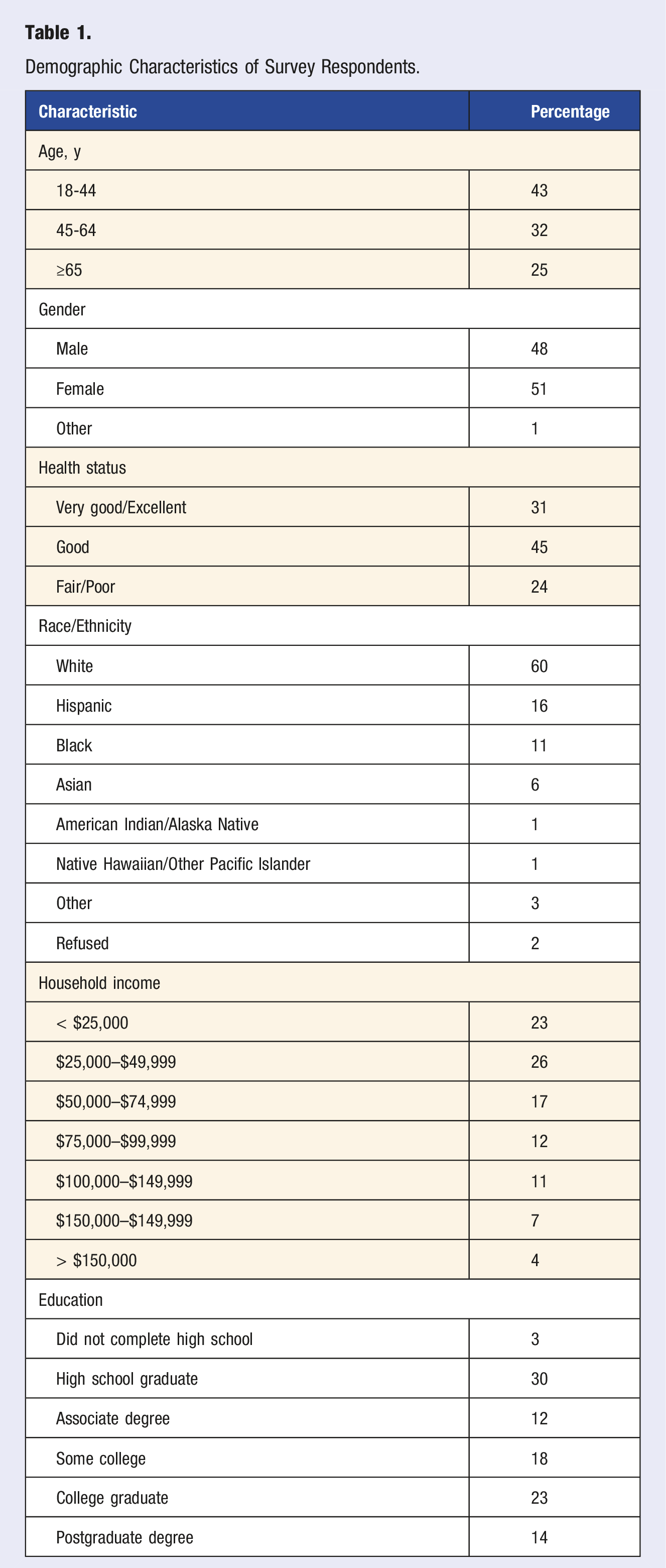
Seventy-one percent of respondents were diagnosed with at least one chronic condition, and 24% rated their health as fair/poor (31% reported their health as very good or excellent). Chronic conditions reported by participants included high blood pressure (35%), anxiety (28%), high cholesterol (27%), overweight/obesity (22%), or diabetes/prediabetes (21%).
Lifestyle Medicine Perceptions
Seventy percent of participants reported that their health care provider discussed lifestyle or behavior changes as part of their medical care. Ninety one percent reported being at least somewhat interested in changing their own lifestyle habits to improve health (Figure 1), with 41% being very or extremely confident they could make lifestyle behavior changes (86% at least somewhat confident). Interest in lifestyle change.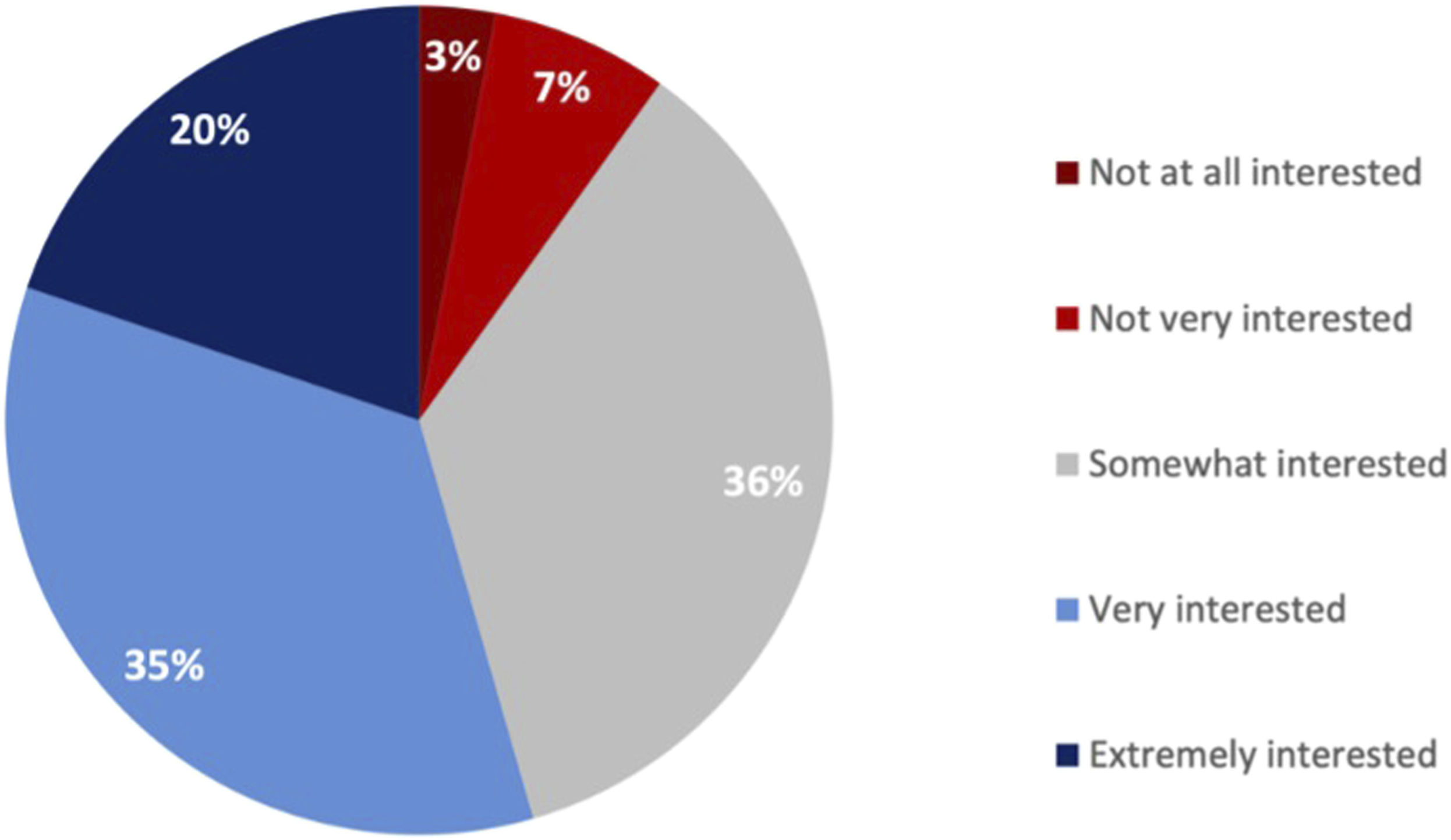
Familiarity with Lifestyle Medicine
Fifty percent of survey respondents reported never having heard of LM (Figure 2). Another 17% said they had heard of it but didn’t know what it meant. Men, younger adults, and higher-income earners reported greater familiarity with LM; the converse was also true: those with lower incomes, older adults, and those who rated their health as fair/poor were more likely to report never having heard of LM. Fifty-eight percent of respondents thought LM reflected key pillars of lifestyle medicine and whole-person care, with 18% thinking it was a medical specialty and 15% believing that LM was a medication or supplement that improves overall health. Familiarity with lifestyle medicine.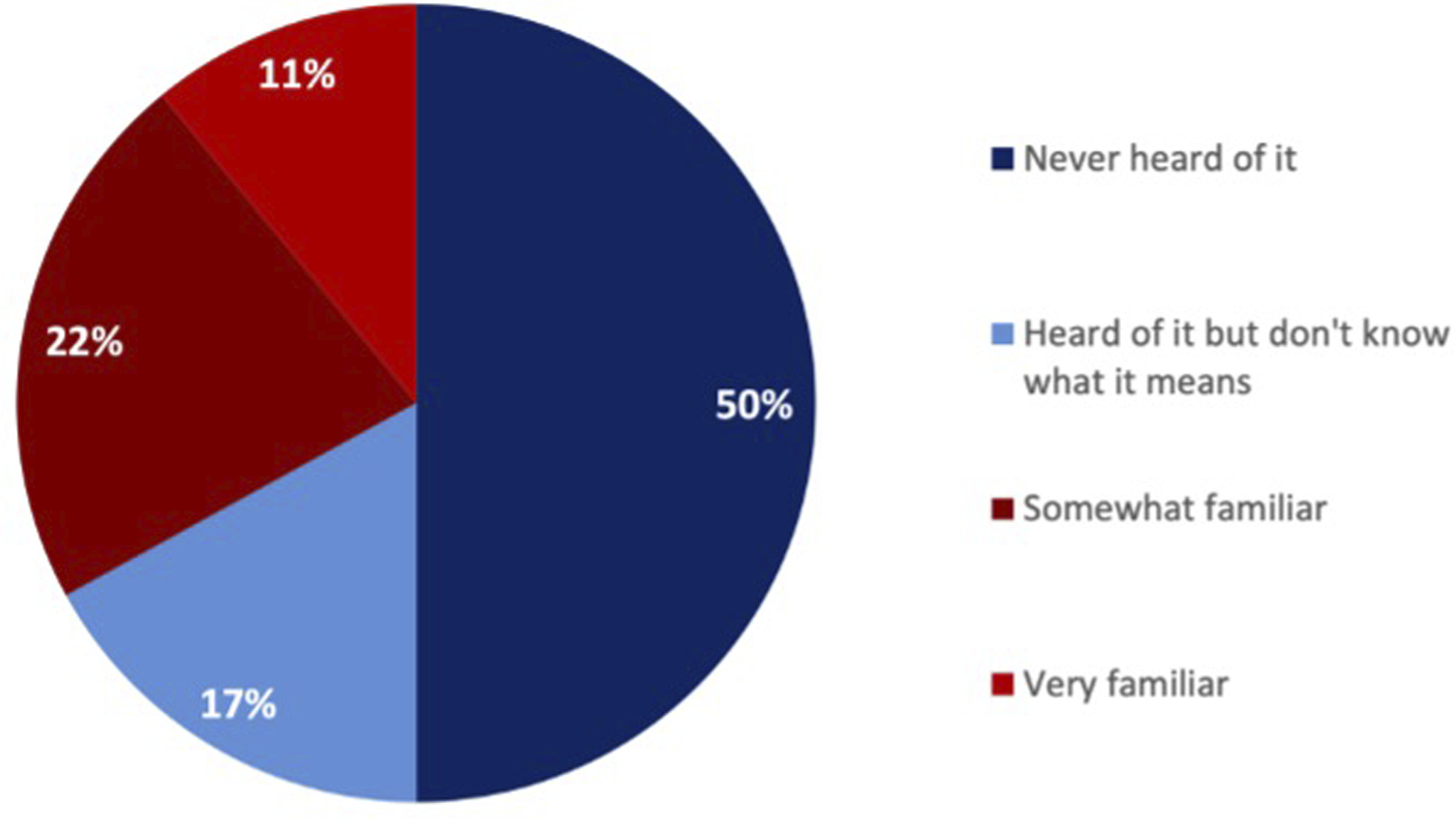
Despite the lower familiarity with LM, more than half (56%) of the respondents reported that their provider had explained how lifestyle habits (sleep, nutrition, stress, exercise) can be an effective part of treatment for physical or mental health conditions. Men, younger adults, and those in better health reported being more likely to have a health care provider who had explained that lifestyle habits can be an effective part of treatment for physical or mental health conditions. Higher-income earners (91% of households earning $100,000 annually or more compared to 73% of those earning less than $25,000 annually) and those with reported better health (87% who report they are in very good or excellent health compared to 74% who report their health is fair/poor) were more likely to report that lifestyle habits can help treat or manage physical or mental health conditions. Older adults and lower-income earners were more likely to report being unsure about the impact of lifestyle habits on health (Supplemental).
After being presented with a definition of LM, 78% of participants reported it as being at least moderately appealing (47% very or extremely appealing). Those most interested included younger men, middle-aged women, middle- to higher-income earners, and those who rated their health as very good or excellent.
Desired Aspects of LM as Part of Medical Care
Top areas of LM that respondents desired additional emphasis on as part of their medical care were physical activity, nutrition advice, and stress management. Additional areas are listed in Figure 3. Younger and middle-aged adults, as well as those who rated their health as poor or fair, wanted a greater focus on stress management. Middle and higher-income earners wanted a greater emphasis on nutrition advice. Older adults and those in poorer health wanted a greater emphasis on medication options, and younger adults wanted a greater emphasis on substance abuse support (Supplemental). Desired areas of medical care focus.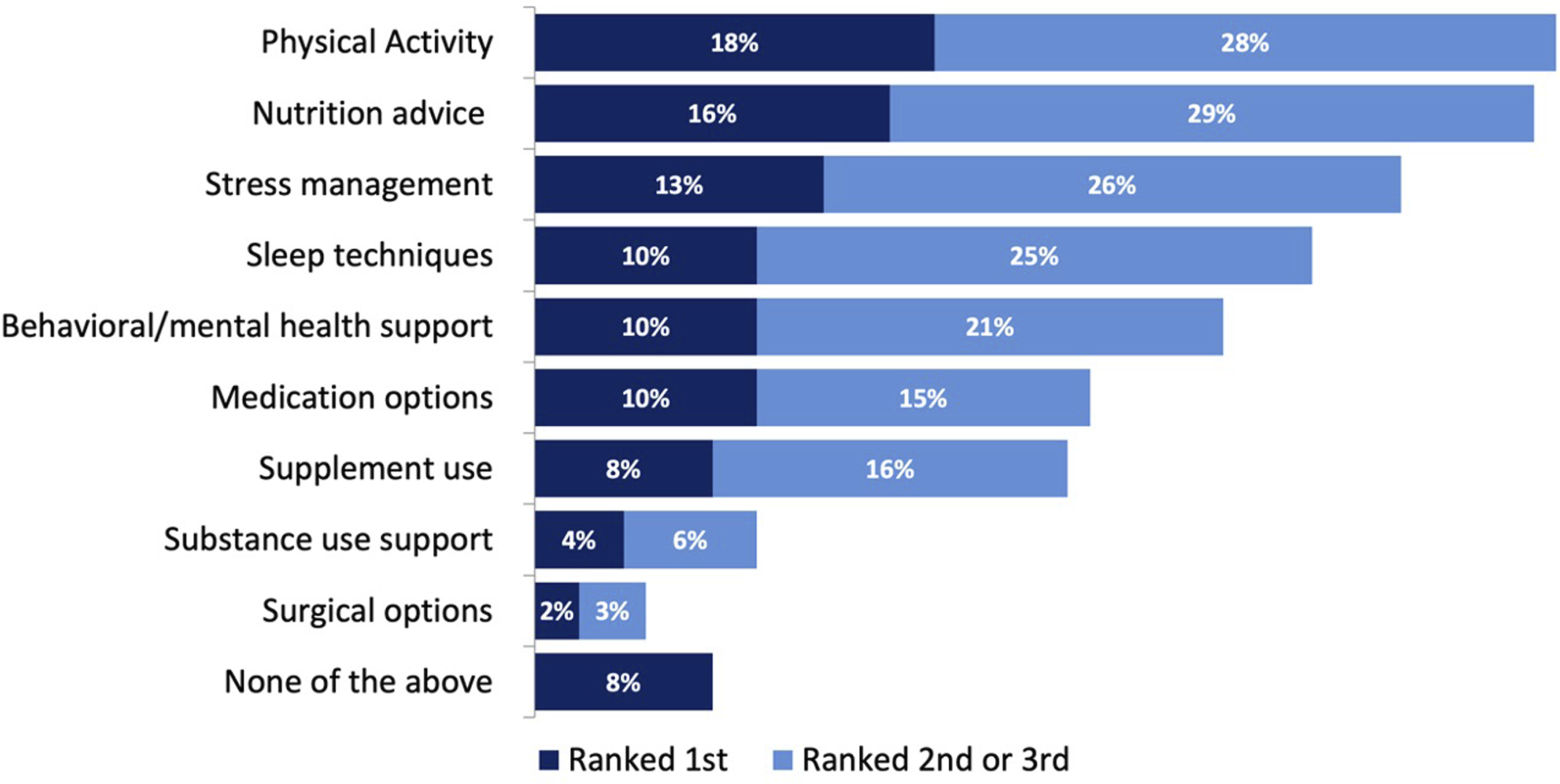
Behavioral Health Perceptions
Nearly all (96%) of respondents reported that it was at least somewhat important that health care providers should address mental health and emotional well-being as part of an individual’s care. Those who were middle-aged and younger were more likely to think that health care providers should address mental health and emotional well-being. Middle- and especially higher-income earners also saw mental health as very important, as did those who reported having good health (Supplemental).
Nearly half (49%) of respondents said that they would be very or extremely likely to use behavioral health services if offered by their primary care doctor. Six in 10 felt LMBH should be a regular part of medical care, and another 22% said these services should be optional or add-on. Nearly half (47%) of respondents say they would be very or extremely likely to choose the provider that offers both LMBH services.
Barriers to Accessing LM and BH Within the Current Health Care System
The primary barriers to accessing behavioral health and LM reported were financial and logistical constraints. Fifty-nine percent reported that insurance coverage would make it easier to use LM or BH services. Other primary barriers include time and scheduling conflicts (48%), lack of awareness (35%), transportation limitations (31%), and privacy/stigma concerns (24%) (Figure 4). Middle-aged and older adults, along with those in poorer health, were more likely to report wanting health insurance coverage for services; older adults wanted these services provided where they already received care, and younger adults wanted it in their community or online (Supplemental). Barriers preventing use of behavioral or lifestyle medicine services.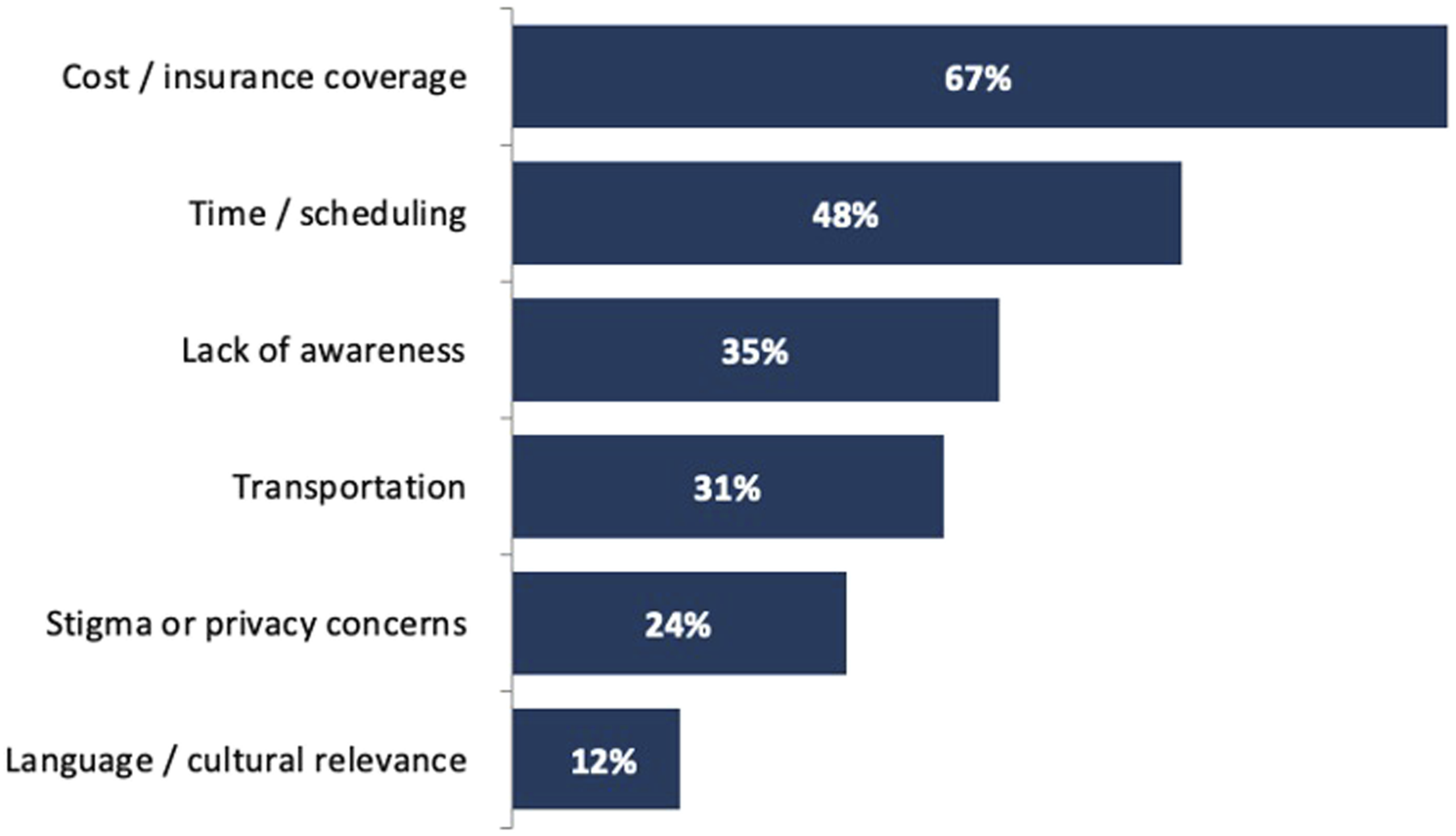
Seventy-seven percent felt that LM should be available to everyone, with 40% reporting that it was unlikely or very unlikely that individuals with lower incomes or without insurance could access LM services. Despite that, 32% of respondents were very or extremely confident that they could find a doctor or clinic that offered LM services, whereas 33% reported being not very confident or not at all confident that they could find these services.
The top two types of information or resources requested by participants were information from their doctor (53%) and educational materials such as videos, articles, and webinars (43%). Specifically, older adults wanted information from their doctor, younger adults and higher-income earners wanted social media or other awareness campaigns, and middle-aged and middle-income earners wanted educational materials (Supplemental).
Discussion
This is the first nationally representative survey of U.S. adults to explore the perceptions, understandings, and attitudes towards lifestyle medicine and behavioral health. There was clear interest in accessing these services, as 91% of respondents were at least somewhat interested in changing their lifestyle habits to improve their health.
Despite this interest in improving lifestyle habits, 50% of respondents had never heard of lifestyle medicine. There also appears to be confusion about what constitutes LM, since participants reported being counseled on multiple LM pillars by clinicians. Potential marketing, outreach, and educational campaigns targeting consumers that describe what lifestyle medicine is, how it might benefit them, and where they can access resources could be useful.
In our survey, younger men with higher incomes were most familiar with LM and its impact on health. This may be due to an inherent interest in healthy aging or longevity among this demographic, 21 or a result of clinicians’ bias in discussing these concepts with some individuals and not others. The lack of familiarity with LM among other demographics, as well as misconceptions noted (15% thought it was a medication or supplement), suggest a clear education gap between the specialty of lifestyle medicine and the population at large.
Despite a lack of familiarity with the term LM, 70% reported being counseled on lifestyle and behavior changes and nearly 80% of respondents found LM at least moderately appealing. This is consistent with findings in an Australian survey of 649 adults. In that study ∼75% of adults felt positive about LM and that it aligned with their personal values. Eighty-six percent reported understanding how LM worked, and 70% believed it would be effective. 12 In this U.S. LM survey, people were most interested in physical activity, nutrition advice, and stress management. These may be ideal areas to focus on first to attract adults and improve engagement with LM services.
Survey participants also strongly supported BH as a component of health care services, with 75% rating it as very or extremely important. The majority (82%) of survey respondents felt that it should be part of routine care provided by their primary care provider. An impressive 41% of respondents were very or extremely confident that they could make behavior changes that support their mental and emotional health. This desire for LM and BH services by adults shows that there is both a recognition about the importance of mental health, stress, and other health-related social needs, as well as an appetite to engage in services that address those issues. However, the high levels of confidence in making behavior changes does not necessarily translate into new behaviors. For example, it is estimated that 47% of individuals who intend to exercise never actually do. This “intention-behavior gap,” is well-recognized and remains a challenge in translating positive intentions into meaningful health changes. 22
Several barriers were reported that made access to LMBH services difficult. Financial constraints, lack of insurance coverage, scheduling challenges, transportation limitations, and limited service availability emerged as the most commonly cited barriers. This was more common among older adults, those with lower incomes, and those in fair or poor health, the same demographics that often have higher rates of diet-related chronic disease.23,24 These barriers closely mirror what has been reported in the literature regarding access to BH care. 25 Although these individuals express interest in making lifestyle changes, they were also less confident in their ability to access LM services. Understanding and working to address barriers, particularly among the lower-income demographic, are critical to improving overall care. Recognizing the relevance of the fundamental cause theory will be valuable when implementing lifestyle medicine interventions to avoid inadvertently worsening health equity.26,27
This survey highlights consumer interest, understanding, knowledge gaps, and barriers to accessing LMBH care. Exploring ways to educate patients, provide appropriate resources, and better integrate LMBH care are needed. Given the critical role LMBH plays in overall health, it is imperative to transition LMBH from specialized services to fundamental, covered, and accessible resources. Leveraging Federally Qualified Health Centers (FQHCs) and empowering primary care sites to deliver LMBH is not merely an option; it is a critical step toward ensuring these vital services are delivered to individuals and families who stand to benefit the most.
Limitations
The cross-sectional survey design elicits reported perceptions about topics and may not reflect true actions or behaviors. The online platforms used to recruit participants invariably created a selection bias toward individuals with access to technology and the time to complete questionnaires. An attempt was made to create a representative sample of U.S. adults, though this artificial recreation may have introduced other unrecognized biases. The surveys were not administered within any specific community, which increased generalizability, though could make the data less relevant to specific health care systems and communities with varying amounts of resources and access to services. Finally, significant testing was not performed, which could have added further credence to the differences observed between subgroups.
Conclusion
U.S. adults perceive LM and BH services positively and value their integration into primary care. Most adults were interested in improving their lifestyle habits and were confident that they could make recommended changes to improve their mental health. However, barriers such as education, access, and financial and logistical obstacles make utilizing LMBH services challenging. These findings should inform patient-centered care design, guide resource allocation, and support strategies that accelerate the transition of these essential, evidence-based services from specialized offerings to broadly covered, accessible, and foundational components of population health.
Supplemental Material
Supplemental Material - Public Perception of Lifestyle Medicine and the Integration of Behavioral Health: A Nationally Representative Survey of U.S. Adults 18+
Supplemental Material for Public Perception of Lifestyle Medicine and the Integration of Behavioral Health: A Nationally Representative Survey of U.S. Adults 18+ by Jonathan Bonnet, Alexandra Lewin-Zwerdling, Steven Mauro, Janet Calhoun, Ron Stout in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Public Perception of Lifestyle Medicine and the Integration of Behavioral Health: A Nationally Representative Survey of U.S. Adults 18+
Supplemental Material for Public Perception of Lifestyle Medicine and the Integration of Behavioral Health: A Nationally Representative Survey of U.S. Adults 18+ by Jonathan Bonnet, Alexandra Lewin-Zwerdling, Steven Mauro, Janet Calhoun, Ron Stout in American Journal of Lifestyle Medicine
Footnotes
Ethical Considerations
This study was determined to be exempt from the Beyond Bound Institutional Review Board (Category 2: DR2603JB-004) .
Author Contributions
JPB, ALZ, SM, and RS assisted in the study design, and all drafted and edited the manuscript. JC assisted in study design and edited manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ardmore Institute of Health provided funding to support this study.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jonathan Bonnet serves on the editorial board of the American Journal of Lifestyle Medicine, on the board of the American Board of Lifestyle Medicine, and as a consultant go Guidepoint Consulting and Synquery AI Consulting.
Data Availability Statement
Data will be made available as a supplement to the article.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.