
Abstract
Musculoskeletal (MSK) shoulder disorders are multidimensional conditions that extend beyond physical impairment, encompassing psychological, sociocultural, and emotional dimensions as well. Qualitative research is particularly well suited to explore these aspects through individuals’ experiences. Since the last qualitative evidence synthesis in 2019, new studies and methodological advances have further deepened our understanding of these disorders. This qualitative evidence synthesis aims to systematically identify and synthesize the lived and treatment-related experiences of individuals with shoulder disorders. We will search Academic Search Premier, CINAHL Plus with Full Text, Embase, MEDLINE, PsycINFO, Scopus, and the Web of Science Core Collection. In addition, we will explore gray literature and conduct supplementary searches, including backward and forward citation tracking, manual searches, and outreach to researchers with expertise relevant to the review topic. We will include primary qualitative studies, as well as qualitative components of mixed-methods studies. All references will be imported into Covidence for comprehensive study selection. If needed, a purposeful sampling strategy guided by a maximum purposive sample frame may be employed. Data will be extracted using a standardized form designed for this synthesis. Methodological limitations will be assessed using the Cochrane qualitative Methodological Limitations Tool (CAMELOT). Evidence will be analyzed using thematic synthesis following a three-step approach: line by line reading, development of descriptive themes, and generation of analytical themes. Confidence in each review finding will be evaluated using the Grading of Recommendations, Assessment, Development and Evaluation confidence in evidence from reviews of qualitative research (GRADE-CERQual). Using a structured and transparent rationale for selecting the synthesis approach, we aim to develop analytical themes that advance understanding of the multidimensional experiences of shoulder disorders. Input from interest-holders will enhance interpretive rigor and ensure clinically meaningful, transferable findings. Anticipated challenges will be addressed through a rigorous, transparent, and reflexive collaborative approach.
Background
Musculoskeletal (MSK) shoulder disorders represent a major global health burden, substantially impairing quality of life through pain, functional limitations, and disrupted daily activities (Cieza et al., 2021; Ferrari et al., 2024). These conditions are often characterized by physical impairments. However, focusing primarily on physical deficits provides an incomplete understanding of individuals’ experiences, as psychological, sociocultural, and emotional dimensions are often central to their lived burden (Cormack et al., 2023; Mintken et al., 2025). Notably, commonly emphasized biomedical indicators, such as structural imaging findings or orthopedic special tests have not demonstrate a clear causal relationship with symptoms that might be experienced (Ibounig et al., 2026; Salamh & Lewis, 2020; Sanders et al., 2025). In contrast, factors such as low pain self-efficacy (Chester et al., 2019; De Baets et al., 2019; Dubé et al., 2024), catastrophizing (Clausen et al., 2023; De Baets et al., 2019), fear-avoidance beliefs (González Aroca et al., 2023; Vogel et al., 2022), low expectations (Dubé et al., 2024; Dunn et al., 2016; Lluch-Girbés et al., 2025), or limited social support (Brindisino et al., 2025) are consistently associated with outcomes and should be considered by clinicians to capture key prognostic information. Together, these findings support a shift toward a biopsychosocial (BPS) and enactive understanding of shoulder disorders (Cormack et al., 2023; Ng et al., 2021).
Qualitative research provides a valuable methodological approach for capturing the multidimensional nature of shoulder disorders and informing more comprehensive care (Carroll, 2017; Flemming et al., 2019). By valuing subjectivity, reflexivity, and the contextual meaning that individuals attribute to their experiences, it enables an in-depth exploration of illness that extends beyond the scope of quantitative data (Lim, 2025). Two previous qualitative evidence syntheses (QES) have explored the experiences of individuals with shoulder disorders (Maxwell et al., 2021; Page et al., 2019). Collectively, these studies confirm that patients experience these conditions as multidimensional, with pain affecting daily life and being closely intertwined with sleep disruption, emotional distress, activity limitations, and social participation restrictions (Page et al., 2019). Individuals frequently reported fear, frustration, and uncertainty, and often adopted a biomechanical lens when interpreting their condition and seeking structural explanations of their symptoms. This perspective sometimes contributed to dissatisfaction with conservative care (Maxwell et al., 2021). Overall, these QES underscored the interconnected physical, psychological, and social dimensions of shoulder disorders and highlighted the importance of patient-centered care grounded in lived experience. However, both QES included studies only up to 2019. Since then, additional qualitative studies have been published, reflecting a growing interest in exploring patient experiences (Maxwell et al., 2022; Poulsen et al., 2025; Powell et al., 2023; Sousa Filho et al., 2024; Vishal et al., 2024). In addition to being outdated, these QES were limited by restrictive inclusion criteria regarding participant characteristics, a relatively narrow range of shoulder conditions, and the absence of more recent methodological advances in QES.
This review is specifically designed to synthesize up-to-date themes from qualitative research that are transferable and meaningful for clinicians, patients, and decision-makers. Engaging stakeholders throughout the review process will support the credibility, relevance, and interpretive grounding of the synthesis, helping ensure that emerging themes reflect both experiential and clinical realities. For clinicians and patients, this QES will provide a deeper understanding of how individuals experience shoulder disorders, thereby supporting patient-centered care, shared decision-making, effective communication, and health education. By synthesizing experiences across diverse settings, this review will also inform decision-makers in the organization of care pathways that are equitable, context-sensitive, and responsive to real-world needs.
Objectives
This review aims to systematically identify and synthesize the lived and treatment-related experiences of individuals with MSK shoulder disorders.
Methods
A QES of primary qualitative studies will be conducted following the recommendations of the Cochrane-Campbell Handbook for QES (Noyes et al., 2024). Both the protocol and manuscript will consider the Cochrane Effective Practice and Organisation of Care (EPOC) guidance for qualitative evidence synthesis (Glenton C, 2023; Glenton et al., 2022) and adhere to the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) statement (Flemming et al., 2018; Tong et al., 2012). However, if the PRISMA extension for Qualitative Evidence Synthesis (PRISMA-QES) is published during the drafting phase, we will adopt this reporting guideline. This protocol was prospectively registered on the Open Science Framework (https://doi.org/ 10.17605/OSF.IO/A2S8U). Any deviations from this protocol will be reported in the final manuscript to ensure methodological transparency. All data associated with this work will be available in an online repository.
Interest-Holders’ Engagement
Engaging interest-holders is increasingly recognized as essential to ensure that a QES is meaningful, relevant, and impactful for end users (Akl et al., 2024; Bullock et al., 2024; Flemming & Noyes, 2021). Consistent with this principle, our review integrates the perspectives of patients from France and caregivers. The Authors and Consumers Together Impacting on eVidencE (ACTIVE) framework was used to guide and describe interest-holders’ engagement in this QES protocol (Pollock et al., 2019). We involved two individuals (one male and one female) living with shoulder disorders (painful shoulder instability and rotator cuff-related shoulder pain) for more than two years and two practicing physiotherapists (both female) from Orléans, France. They were recruited through a closed approach from the personal network of one author (AR). These interest-holders contributed to the development of the research question and will be involved at the “controller” level in planning the research methods and drafting this protocol (Pollock et al., 2019). They will remain actively engaged throughout the review via direct exchanges (meetings and email) and will be particularly consulted during the synthesis phase at the “contributor” level to provide their perspectives and feedback on the interpretation of findings (Belton et al., 2019; Pollock et al., 2019). This ensures that the analytical themes accurately and meaningfully reflect the lived and treatment-related experiences of individuals with shoulder disorders. All the interest-holders declined payments for their contributions.
Criteria for Considering Studies for This Review
Types of Studies
We will include primary studies that use qualitative study designs (e.g. phenomenology, ethnography, case studies, grounded theory, qualitative content analysis, qualitative descriptive studies). Eligible studies must have used qualitative methods for both data collection (e.g. individual interviews, focus group discussions, observation, document analysis, open-ended surveys) and data analysis (e.g. thematic analysis, framework analysis, grounded theory). We will also include qualitative findings from mixed-methods studies, provided that qualitative data are collected and analyzed separately from quantitative data. Studies may include comparators (e.g. different interventions) or not. We will exclude studies that used qualitative data collection methods but did not apply qualitative analytical approaches (e.g. responses to open-ended surveys analyzed using descriptive statistics only). Both published and unpublished studies will be considered, including peer-reviewed and non-peer-reviewed sources. Gray literature will also be included, such as master’s and doctoral theses employing qualitative or mixed-methods approaches. Conference abstracts will be excluded, as they are unlikely to provide sufficient qualitative data for synthesis. The following sources will be excluded: review articles, clinical guidelines, study protocols, reports, policy documents, government publications, and blogs. Studies will not be excluded based on methodological limitations; instead, these limitations will be considered when interpreting the results and assessing confidence in the review findings.
Clarifying Question Formulation, PerSPE(c)TiF Table Based on Booth et al. (Booth et al., 2019)

Topic of Interest
We will explore both the lived and treatment-related experiences of individuals with shoulder disorders, focusing on how participants experience, perceive, and manage their condition and the care they receive. This includes individuals’ physical, psychological, and social experiences, as well as their perspectives, opinions, needs, preferences, and values. We are particularly interested in qualitative findings that illuminate the subjective dimensions of illness, including narratives and themes emerging from participants’ accounts of their everyday experiences. Studies that explore perspectives other than those of individuals living with shoulder disorders, such as those of healthcare providers or caregivers, will be excluded.
Types of Participants
We will include studies involving participants with shoulder disorders, which primarily refer to non-traumatic conditions, the most common being rotator cuff-related shoulder pain (RCRSP). This umbrella term “encompasses a spectrum of shoulder conditions including subacromial pain (impingement) syndrome, rotator cuff tendinopathy and symptomatic partial-and full-thickness rotator cuff tear” (Lewis, 2016). Calcific tendinopathy, biceps tendinopathy and subacromial bursitis, conditions not included in the original definition of RCRSP, will also be considered. Other shoulder disorders of interest include frozen shoulder; glenohumeral conditions (anterior, posterior, or multidirectional glenohumeral instability; dislocations, sprains, osteoarthritis, and glenoid labrum pathologies); acromioclavicular and sternoclavicular joint conditions (sprains, instability, or osteoarthritis); and fractures of the humerus, scapula, or collarbone. Experiences related to surgical management of these conditions will also be considered. We will exclude qualitative or mixed-methods studies focusing on shoulder disorders secondary to referred pain originating from the cervical or thoracic spine, as well as those resulting from neurological disorders, vascular diseases, visceral conditions, systemic inflammatory diseases, or a history of cancer.
Aligned with current recommendations to consider key domains of disadvantage in equity-focused reviews, no restriction will be applied based on equity, diversity, and inclusion (EDI) criteria or healthcare setting (e.g. private practices, hospitals, primary care clinics) (McCann et al., 2025). Particular attention will be paid to environmental determinants of experience, such as infrastructural, logistical, organizational, and systemic factors. No restrictions will be applied regarding the timing of the experience. Individuals will be considered regardless of their stage within their care, disease, health, or life trajectory.
Search Methods for Identification of Studies
Electronic Searches
A preliminary search was conducted in MEDLINE (Ovid) using an initial strategy developed in collaboration with an experienced research librarian (MGa) (Harris et al., 2018), followed by an analysis of the titles, abstracts, and indexing terms of the retrieved records. This process informed the estimated number of potentially eligible studies and supported the iterative refinement of the final search strategy, which incorporated all relevant keywords and indexing terms identified during the preliminary phase. This strategy was developed based on key terms and on the PerSPE(c)TiF elements defined in our eligibility criteria. A comprehensive systematic search (Appendix I) will be conducted across seven electronic databases: Academic Search Premier (EBSCOhost), CINAHL Plus with Full Text (EBSCOhost), Embase (Embase.com), MEDLINE (Ovid), PsycINFO (Ovid), Scopus (Scopus.com) and Web of Science (Core Collection, as provided by Université Laval; Editions: SCI-EXPANDED, SSCI, AHCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI). In accordance with the Peer Review of Electronic Search Strategies (PRESS) guideline, the search strategy was peer-reviewed by a second independent research librarian, and changes were made by MGa based on revisions suggested (Appendix II) (McGowan et al., 2016).
Gray Literature
One reviewer (AR) will conduct a gray literature search to identify unpublished reports such as master’s or doctoral theses. The following sources will be consulted: AHRQ (www.ahrq.gov), Eldis (www.eldis.org), EThOS (www.ethosdatabase.org), Grey Literature Report (www.greylit.org), HAL (hal.science), Google Scholar (scholar.google.com), NICE (www.nice.org.uk), OATD (oatd.org) and OpenGrey (opengrey.eu). Unpublished and ongoing trials (for mixed-methods studies only) will also be searched via WHO International Clinical Trials Registry Platform (www.who.int/ictrp/en/) and the US National Institutes of Health (clinicaltrials.gov). Google Scholar will be searched following the methodology described by Bramer et al. (Bramer et al., 2017), whereby the first 200 references will be screened, including both review articles and gray literature sources. The search strategies used for gray literature will be reported in the final manuscript.
Searching Other Resources
A supplementary search will include citation tracking through both backward and forward citation searching (Hirt et al., 2023). We will also manually screen the reference lists of the two previously identified QES (Maxwell et al., 2021; Page et al., 2019), as well as studies included in other relevant systematic reviews related to our topic identified in the Cochrane Library. In addition, about ten researchers who have been identified as having relevant expertise (i.e., authors with multiple publications in MSK shoulder disorders) will be contacted following database searches to request any potentially eligible studies that might meet our inclusion criteria. They will be contacted once by email and details of the authors contacted will be reported.
Selection and Sampling of Studies
Following completion of database searches, all retrieved records will be imported into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia) for screening and analysis. Duplicate records will be automatically removed prior to study selection. Eligible gray literature will be imported into Covidence through Zotero (Zotero software, Corporation for Digital Scholarship, Fairfax, VA, USA). Two reviewers (AR and PM or TL) will initially screen a 5% sample of titles and abstracts during a calibration phase to ensure consistency in applying the pre-specified eligibility criteria (Ames et al., 2024). Following calibration, two reviewers (AR and PM or TL) will independently assess the titles and abstracts of all retrieved records for eligibility. Full texts of potentially eligible studies will then be reviewed independently by two reviewers (AR and PM or TL). Disagreements will be resolved through discussion between the two reviewers, or, when required, by involving a third review author (MGu or JSR). Study authors will be contacted for additional information when required. This study selection process will be reported using a PRISMA flow diagram template adapted for a QES (Page et al., 2021).
For titles and abstracts published in languages not mastered by the review team (other than English or French or Spanish), initial translation will be performed using ChatGPT Plus (Open AI, San Francisco, CA, USA) (Chan & Tang, 2024). If this preliminary translation suggests potential eligibility, or does not allow a clear decision, the full text article will be translated and assessed. Assistance from colleagues who are native speakers of the relevant language will be sought to confirm any inclusion. If such assistance is unavailable, the study will be categorized as “awaiting classification” to maintain transparency.
In accordance with Cochrane-Campbell Handbook guidance for QES, once all studies that meet our inclusion criteria are identified, we will assess whether their number may pose challenges for analysis (Ames et al., 2024; Booth, 2016). Based on our preliminary searches, we anticipate that the volume, quality, and richness of the available evidence should be sufficient to support a manageable synthesis (Sandelowski, 1995). However, if the number of eligible studies exceeds what is feasible for a comprehensive study selection, we will retain our initial eligibility criteria (Benoot et al., 2016) but consider applying a purposeful sampling strategy (Ames et al., 2024). This sampling strategy will follow a maximum variation purposive frame, as recommended for less experienced review authors (Ames et al., 2024). Sampling would consider three dimensions of variation (i) type of shoulder disorders, (ii) inclusions in two previous QES (Maxwell et al., 2021; Page et al., 2019), and (iii) studies where the focus closely aligned with the objectives of the current synthesis. The rationale and criteria for any applied sampling will be fully documented and reported in the final review.
Data Extraction
Characteristics of Included Studies Table Considering PerSPE(c)TiF and CAMELOT Items

Methodological Strengths and Limitations Assessment in Included Studies
The methodological quality of all included studies, whether gray literature or peer-reviewed, will be assessed using the CochrAne qualitative Methodological LimitatiOns Tool (CAMELOT) (H. M. Munthe-Kaas et al., 2024). Specifically developed to support QES and aligned with the Grading of Recommendations Assessment, Development and Evaluation confidence in evidence from reviews of qualitative research (GRADE-CERQual) framework, CAMELOT is an evidence‐based tool for assessing the methodological strengths and limitations of primary qualitative research studies in a QES. The tool includes 12 domains, including four Meta domains and eight Method domains (H. M. Munthe-Kaas et al., 2024).
Two reviewers (AR and PM or TL) will independently appraise each study, with consensus checks at each stage. Prior to full appraisal, a calibration phase will be conducted on a sample of five studies to ensure consistency in interpretation and application of the tool. Any disagreements will be resolved through discussion between the two reviewers, or, when required, by involving a third review author (MGu or JSR). The assessment process will follow a structured and iterative approach, with each domain systematically extracted and annotated as necessary. Reviewers (AR and PM or TL) will then evaluate the overall “fit” between Meta and Method domains, categorizing it qualitatively as “no or minimal concerns”, “minor concerns”, “moderate concerns”, “serious concerns” or “unclear”. Each judgment will be accompanied by a narrative rationale to ensure transparency. Overall methodological concern for each study will be determined based all domains strengths and limitations rather than numeric scoring, using the first four-level categorization (H. M. Munthe-Kaas et al., 2024). Finally, assessments of fit across the studies will be combined, contributing to a review finding. A level of concern regarding methodological limitations will be categorized using the same first four-level categories mentioned. Summary of the results of the CAMELOT assessments will be presented in a table including author(s) and year, and the overall CAMELOT judgment of methodological limitations.
Data Management, Analysis and Synthesis
Selection of the Most Appropriate QES Method Considering RETREAT Criteria (Booth et al., 2018)
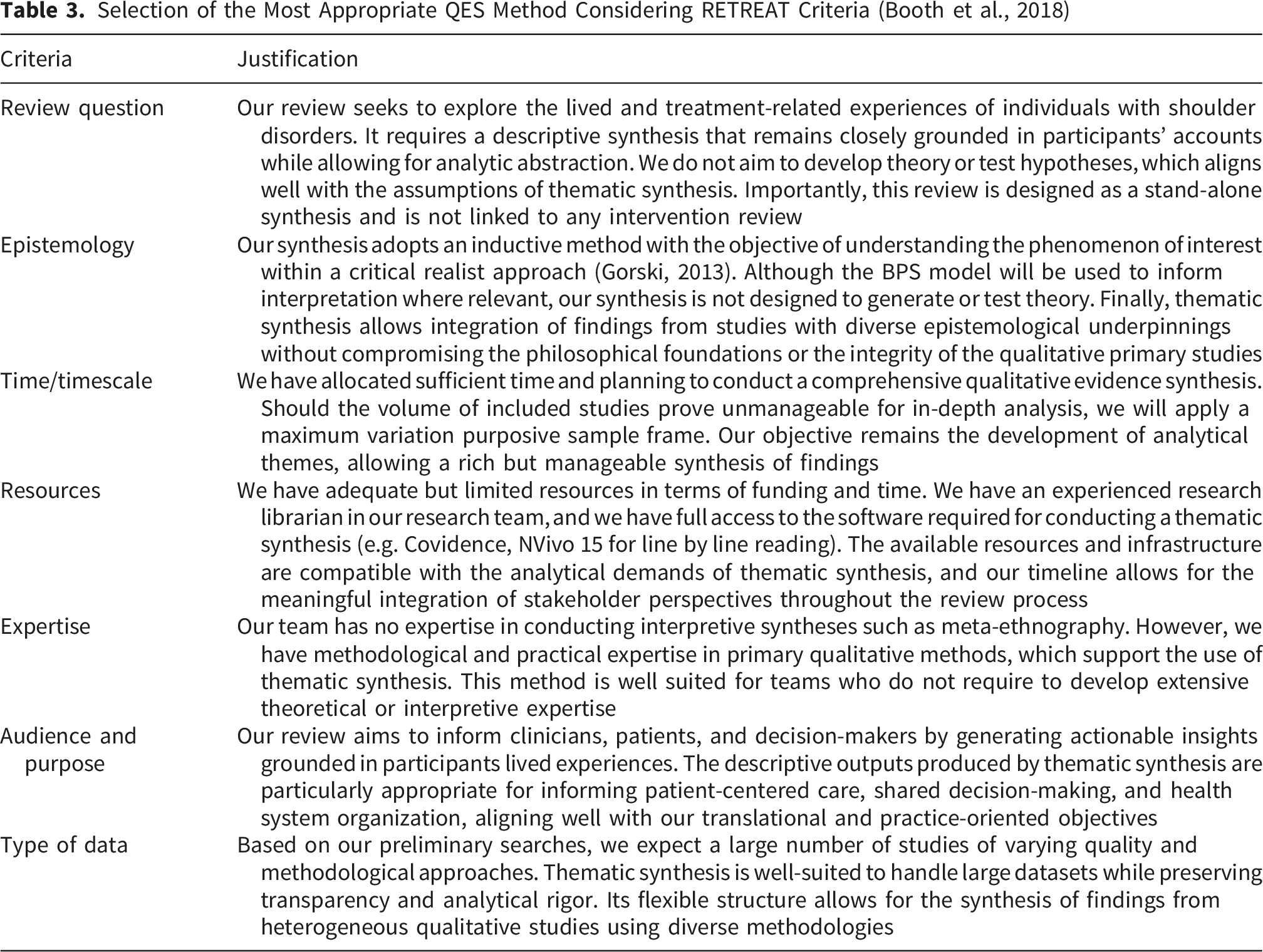
Thematic synthesis, which mirrors the thematic analysis commonly used in primary qualitative studies, facilitates the development of findings at both descriptive and interpretative levels (Harden et al., 2025), generating insights that can directly inform clinical practice, policy-making, and guideline development (Flemming et al., 2019; Noyes et al., 2019). Our synthesis will proceed in three key stages: line by line reading, development of descriptive themes, and generation of analytical themes (Harden et al., 2025). The analytical themes generated will aim to go beyond description by identifying patterns of meaning across studies and proposing inductive insights. This QES does not aim to develop a formal theory. In this context, “a theory is the outcome of a form of knowledge synthesis, where different forms of knowledge (including other theories) are assembled to understand or describe a phenomenon” (Thomas et al., 2023). Our research question is nevertheless informed by the BPS model (Cormack et al., 2023), which will guide interpretation of findings especially during the generation of analytical themes. This model will not guide the coding a priori, but may inform the development of analytical themes, as it offers a patient-centered perspective integrating physical, psychological, sociocultural, and emotional dimensions (Cormack et al., 2023). We will adopt an inductive approach to capture the meaning and content of each individual finding (Thomas & Harden, 2008). In this context, findings are defined as analytic outputs that “based on data from primary studies, describes a phenomenon or an aspect of a phenomenon” (Lewin et al., 2015). We do not plan to conduct subgroup analyses, as we anticipate that findings will be broadly applicable to all individuals with shoulder disorders.
Before the coding phase, one member of the review team (AR) will proceed with a phase of immersion and familiarization with the data by reading and rereading each of the included studies. After this phase, he will begin coding performing line by line reading of the abstract, results, discussion, and conclusion sections of all included studies (Harden et al., 2025). Regular meetings will be held with one (PM) or more members of the research team to discuss interpretations and refine the codes where needed. We will use NVivo 15 (QSR International, Burlington, MA, USA) for coding and synthesizing qualitative findings (Houghton et al., 2017). As each new study is coded, previously developed codes will be reviewed and refined, and new codes will be added as necessary. Upon completion of the coding phase, the research team will discuss the emerging codes by sharing their perspectives. In the second stage, related codes will be grouped to develop descriptive themes, with collaborative input from one (PM) or more members of the research team. Themes are defined as “patterns of meaning (e.g. concepts, ideas, experience, sense-making) that are underpinned and unified by a central idea” (Braun & Clarke, 2021). The progression from coding to theme development will follow an iterative logic where interpretations are repeatedly tested against the primary data and discussed by the review team. This reflexive process ensures that the analytical themes are grounded in individuals’ experiences. In the third and final stage, one member of the review team (AR) will interpret the descriptive themes to develop analytical themes that address the review objective and generate new interpretations. Regular meetings will be held with one (PM) or more members of the research team and with the interest-holders to revisit the descriptive themes in light of the review question and purpose, exploring their connections with the BPS model, and engaging discussions to interpret and refine emerging conceptual insights (Harden et al., 2025). Interest-holders will attend one or more in-person or online meetings with a member of the review team (AR) during this phase to share their perspectives and contribute to the development of themes. If relevant data are missing during data extraction or synthesis, study authors will be contacted via email. If no response is received within two weeks, a first follow-up email will be sent, followed by a second reminder two weeks later if necessary. Data obtained from authors will be included without reinterpretation.
Confidence in the Findings Assessment
Confidence in the review findings will be assessed using the GRADE-CERQual approach (Lewin et al., 2015). Specifically developed for qualitative evidence syntheses, this framework evaluates confidence in each review finding by considering four key components (Lewin, Booth, et al., 2018a): the methodological limitations (H. Munthe-Kaas et al., 2018), the relevance of the studies contributing (Noyes et al., 2018; Booth, Lewin, et al., 2018a), the coherence of data (Colvin et al., 2018), and the adequacy of data (Glenton et al., 2018). Two reviewers (AR and PM or TL) will independently assess the overall confidence in each finding using four levels based on “the review finding is a reasonable representation of the phenomenon of interest”: high confidence, moderate confidence, low confidence or very low confidence (Lewin et al., 2015). Each finding will initially be considered as high confidence and may subsequently be downgraded if substantial concerns are identified in relation to any of the GRADE-CERQual components. Any disagreements will be resolved through discussion between the two reviewers (AR and PM or TL), or, when required, by involving a third review author (MGu or JSR). We will present summaries of the findings and our assessments of confidence in these findings in the “Summary of Qualitative Findings” table, which will include each review findings, its assigned level of confidence and an explanation of the judgment (Lewin, Bohren, et al., 2018b). We will present detailed descriptions of our confidence assessment in an Evidence Profile.
Equity, Diversity, and Inclusion
To ensure EDI representation of diverse perspectives, experiences and contexts, we will use the EQUALSS GUIDE Multiple framework (McCann et al., 2025). This framework informed the development of our eligibility criteria and will guide data extraction by assessing how EDI dimensions are addressed in the included studies. In addition, EDI considerations will inform the interpretation and reporting of findings to ensure that the synthesis is conducted in an equity-sensitive manner (Harden et al., 2025).
Review Authors’ Reflexivity
The review team acknowledges that QES is an interpretive process, shaped by researchers’ positionalities, disciplinary backgrounds, and prior experiences. Reflexivity is therefore critical to recognize and manage potential influences on the conduct and interpretation of the review (Flemming & Noyes, 2021). To foster reflexivity throughout the process, the team will hold regular consensus meetings to deliberate on methodological decisions, discuss emerging findings, and critically reflect on individual assumptions or preconceptions that may influence interpretation. Our team comprises five white male physiotherapists (AR, PM, TL, MGu, JSR) and a white female research librarian (MGa). AR, PM, and MGu are from France, TL is from France and has English origins, JSR and MGa are from Canada.
AR is a physiotherapist with clinical expertise in managing MSK shoulder disorders in private practice. He is currently working as a lecturer at the University of Orléans and as a doctoral student under the supervision of JSR and MGu, focusing on comparing usual physiotherapy care and education-based interventions for individuals with acute RCRSP. His interest in qualitative synthesis stems from a belief that a deeper understanding of patients’ experiences may inform the design and tailoring of educational content in a future randomized controlled trial. He has already conducted systematic and scoping reviews.
PM is a physiotherapist, with previous clinical expertise in the management of MSK conditions, particularly in the treatment of patients with shoulder pain, in various settings and environments. He is currently working as a doctoral student under the supervision of JSR, focusing on understanding shoulder pain in workers using mixed-methods. He acknowledges that his experience as a physiotherapist and social status could influence his work. However, he is convinced of the importance of understanding the experience or perspective of patients. Finally, he has already conducted various reviews, qualitative studies, and been involved in other articles related to QES.
TL is a physiotherapist, with previous clinical expertise in the management of MSK conditions. He is currently working as lecturer and doctoral student. His research topics include the clinical and health-economic evaluation of care pathways of patients with MSK shoulder disorders, as well as innovative care pathways (particularly through task-shifting protocols). He has already conducted various reviews.
MGa is a research librarian with solid experience supporting multiple knowledge syntheses across health-related disciplines. Her primary interest lies in the methodology of evidence synthesis, with a particular focus on optimizing search strategies and ensuring comprehensive coverage of the literature. She believes that high-quality reviews play a critical role in providing an up-to-date understanding of the current state of knowledge to better inform healthcare professionals. In this review, her role is to help ensure that the search process captures the full scope of relevant evidence on the topic.
MGu is a physiotherapist and associate professor at the University of Orléans. His research focuses on the neurophysiological mechanisms underlying upper-limb sensorimotor control, with the aim of developing strategies to improve prosthesis use in individuals living with an amputation. He also has a particular interest in pain management, especially phantom limb pain and how this pain could affect sensorimotor control, quality of life and use of the prosthesis.
JSR is a physiotherapist and professor at the School of Rehabilitation Sciences at Université Laval. He has conducted several studies in populations with shoulder disorders, primarily RCRSP. These studies aimed to better understand the development and chronicity of shoulder disorders and to evaluate the effectiveness of various interventions. He recently published a clinical practice guideline for rotator cuff tendinopathies.
The professional and disciplinary diversity within the review team may influence various stages of the review process, including question formulation, search strategy design, definition of eligibility criteria, interpretation of findings, and theme development. While such heterogeneity introduces the potential for differing interpretive lenses, it also offers a valuable safeguard against the dominance of any single perspective. To manage these dynamics, we will engage in an ongoing reflexive process, supported by the use of reflexive notes and structured team discussions at all stages of the project, including during the preparation of this protocol. Where appropriate, we will report how researcher positionality informed the development of analytical themes and influenced the interpretation of findings. This commitment to reflexivity is intended to enhance the credibility, transparency, and trustworthiness of the synthesis, in alignment with best practices for qualitative evidence synthesis Noyes et al., 2024.
Discussion
Based on the scope and objective of this thematic synthesis, we anticipate identifying several analytical themes that reflect the multidimensional and contextual nature of individuals’ lived and treatment-related experiences of shoulder disorders. These insights are expected to deepen understanding from a BPS perspective of how physical, psychological, and emotional dimensions intersect within diverse healthcare and sociocultural contexts. Engaging interest-holders as contributors during the process is intended to strengthen interpretive grounding, enhance relevance for clinical practice, and ensure that analytical themes resonate with experiential realities.
Selecting the most appropriate approach and search strategy posed a well-recognized methodological challenge (Kastner et al., 2016; Noyes; Booth, Cargo, et al., 2018). We first considered a scoping review to map the types of evidence available regarding our phenomenon of interest (Munn et al., 2018). However, a QES was deemed more appropriate for addressing our research question (Noyes et al., 2024). We also considered whether updating the meta-ethnography conducted by Maxwell et al. (Maxwell et al., 2021) was warranted, guided by a decision flowchart designed to determine why, when and how to update a meta-ethnography (France et al., 2016). Since 2019, the available qualitative research on shoulder disorders has increased, albeit without conceptual or epistemological shifts that would undermine the relevance of the original synthesis. The meta-ethnography remains methodologically rigorous, consistent with established reporting standards and provides a credible synthesis of the evidence. Although recent methodological developments, such as structured approaches to study selection, CAMELOT, and GRADE-CERQual could enhance transparency and confidence assessment, their absence does not necessarily invalidate the prior review. Moreover, meta-ethnography is a highly interpretive approach, requiring substantial immersion in primary studies and advanced qualitative expertise, which our team does not possess (Campbell et al., 2011; Houghton et al., 2017). Considering these factors, and guided by the RETREAT framework (Booth et al., 2018), we chose to carry out a thematic synthesis.
Several potential limitations must be acknowledged. First, variability in how shoulder disorders are defined and conceptualized across primary studies may affect which studies are eligible for inclusion, potentially increasing interpretive uncertainty during synthesis. In addition, we anticipate that our findings will be applicable to all individuals with shoulder disorders. However, diversity in participant characteristics, healthcare contexts, and disorder chronicity or etiology may limit the transferability of some themes and require careful attention to context when interpreting findings. Another limitation concerns the absence of a universally accepted framework for assessing methodological quality. We selected the CAMELOT approach for its domain-specific design, explicit alignment with GRADE-CERQual, and focus on identifying methodological strengths and limitations (H. M. Munthe-Kaas et al., 2024). The structured yet interpretive nature of these tools demands in-depth understanding, critical reflection, and team consensus to ensure accurate and transparent judgments. Our commitment to methodological rigor and transparency in a reflexive and collaborative synthesis approach is well suited to addressing these challenges.
Supplemental Material
Supplemental material - Exploring the Lived and Treatment-Related Experiences of Individuals with Musculoskeletal Shoulder Disorders: Protocol for a Qualitative Evidence Synthesis
Supplemental material for Exploring the Lived and Treatment-Related Experiences of Individuals with Musculoskeletal Shoulder Disorders: Protocol for a Qualitative Evidence Synthesis by Alexis Ramos, Jean-Sébastien Roy, Thomas Lathière, Martine Gagnon, Matthieu Guémann, and Philippe Meidinger in International Journal of Qualitative Methods.
Supplemental Material
Supplemental material - Exploring the Lived and Treatment-Related Experiences of Individuals with Musculoskeletal Shoulder Disorders: Protocol for a Qualitative Evidence Synthesis
Supplemental material for Exploring the Lived and Treatment-Related Experiences of Individuals with Musculoskeletal Shoulder Disorders: Protocol for a Qualitative Evidence Synthesis by Alexis Ramos, Jean-Sébastien Roy, Thomas Lathière, Martine Gagnon, Matthieu Guémann, and Philippe Meidinger in International Journal of Qualitative Methods.
Footnotes
Acknowledgments
We are grateful to Mrs. Lucie Bayart, Mrs. Marine Marchin, Mrs. Automne Pelletier, and M. Tanguy Varennes, interest-holders engaged in this research project.
Ethical Considerations
The data used in the analysis will be assessed based on studies that have already been published without the need for research ethics approval.
Author Contributions
Conceptualization: AR, PM, TL, MGu, JSR. Methodology: AR, PM. Validation: AR, PM, MGu, JSR. Resources: PM. Writing - original draft: AR, PM. Writing - review & editing: AR, PM, TL, MGa, MGu, JSR. Vizualisation: AR, PM, MGu, JSR. Supervision: PM, MGu, JSR. Project administration: AR.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AR receives a doctoral scholarship from the Center for Interdisciplinary Research in Rehabilitation and Social Integration (Cirris). PM receives a doctoral fellowship from Arthritis Society Canada (award#25-0304). The funders have not had, or will not have, any influence on the design, scope, or conduct of this review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.