
Abstract
The aim of the study was to investigate the effect of recent chemotherapy (Chx) on outcome of aorto-iliac aneurysm (AAA) repair. The 2005–2010 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was queried to identify vascular patients undergoing AAA repair within 30 days after Chx. Seventy-one patients underwent AAA repair within 30 days of receiving Chx, group A (71 ± 8.4 years, 77.5% males) and 20,024 patients underwent AAA repair without prior Chx, group B (73 ± 9 years, 79.2% males). The two groups did not significantly differ with respect to open or endovascular repair (open repair A: 32%, B: 35%, P = 0.66). However, patients in group A presented more often as emergent cases (A: 27%, B: 12%, P = 0.001). Multivariable regression analysis for emergent cases after adjustment for relevant confounders also demonstrated that patients with recent Chx present more often as emergency (P = 0.001, odds ratio [OR]: 2.4). Thirty-day non-surgical complications were more common in group A (A: 25%, B: 16.5%, P = 0.046) while surgical complications were equivalent (A: 15.5%, B: 12.3%, P = 0.414). Risk of death was significantly higher in group A in univariate analysis (A: 13%, B: 5%, P = 0.005, OR: 2.6). Patients who receive Chx within 30 days prior to AAA repair present more frequently as emergencies leading to higher mortality. The reason for this cannot be sufficiently explained by the current database but patient selection for elective repair or the effect of Chx on the natural course of AAA may play a role.
Introduction
The simultaneous finding of aorto-iliac aneurysms (AAA) and malignant diseases has been frequently reported in the literature within case reports or small series, and different management concepts have been proposed.1–5 Open or endovascular aortic aneurysm repair (EVAR) either simultaneously with the malignancy or in a two-stage approach has been suggested as a feasible and safe treatment option.
Although coincidence of cancer and AAA has been widely reported, only limited reports exist concerning the effect of neoadjuvant or adjuvant chemotherapy (Chx) to the morphology, wall structure and rupture risk of aortic aneurysms.6,7 Aneurysm diameter, sac expansion rate, blood pressure and female sex are some of the known clinical risk factors associated with higher risk of AAA rupture. The effect of recent Chx has never been investigated in a larger cohort of patients. We used the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database to report the 30-day outcome of patients with malignant disease who received Chx treatment within 30 days prior to aortic aneurysm repair.
Methods
Data source
ACS-NSQIP is a risk-adjusted data collection mechanism that collects and analyses clinical outcomes data. Participating hospitals use their collected data to develop quality initiatives that improve surgical care and to identify elements in provided health care that can be improved when compared with other institutions.
The ACS-NSQIP collects data on a variety of clinical variables, including preoperative risk factors, intraoperative variables and 30-day postoperative mortality and morbidity outcomes for patients undergoing major surgical procedures in both the inpatient and outpatient setting. A site's surgical clinical nurse reviewer using a variety of methods including medical chart abstraction captures outcomes data. 8
Data selection and definitions
Using the 2005–2010 ACS-NSQIP database, we identified patients who underwent Chx for malignancy within 30 days prior to aorto-iliac reconstructions for aneurysmal disease in a subcohort of patients who were registered as patients of the Vascular Specialty.
Chx regimens included, but were not restricted to, oral and parenteral treatment with chemotherapeutic agents for malignancies such as colon, breast, lung, head and neck, and gastrointestinal solid tumors as well as lymphatic and hematopoietic malignancies such as lymphomas, leuk and multiple myeloma. Treatment that consisted solely of hormonal therapy was not considered. Chx treatment had to be for malignancy (NSQIP variables definition). Size of AAA, type and length of Chx before the procedure are not captured in the 2005–2010 ACS-NSQIP database.
Current Procedural Terminology (CPT, American Medical Association, Chicago, IL, USA) codes used were 35081, 35082, 35091, 35092, 34830–34832 that describe open repair of AAA or iliac aneurysm plus repair using a tube, aortobiiliac, or aortobifemoral prosthesis as well as the CPT codes 34800, 34802–34805 used to describe EVAR for aortoiliac aneurismal disease. The variable ‘chemotherapy for malignancy in ≤30 days preoperative’ was used to identify patients with recent Chx.
For study purposes, two groups were identified to use for comparison: group A comprised of patients with AAA repair and Chx 30 days prior to surgery and group B of all other patients undergoing AAA repair.
An emergency case is defined, according to ACS-NSQIP, as one that is performed as soon as possible and no later than 12 hours after the patient has been admitted to the hospital or after the onset of related preoperative symptoms. Both surgeon and an should report the case as emergent.
Risk factors and endpoints
All risk factors available in the ACS-NASQIP database were evaluated and compared between groups. The primary endpoint of the study was the effect of prior Chx in presentation of patients as emergent cases and 30-day mortality. Secondary endpoints included postoperative morbidity, procedure-related complications and length of hospital stay. Composite endpoints were created to facilitate a better understanding of the outcomes. Surgical complications (all surgical site infections, wound disruption, bleeding requiring transfusion, graft/prosthesis/flap failure and peripheral nerve injury), renal complications (progressive and acute renal failures), pulmonary complications (pneumonia, unplanned intubation and respiratory insufficiency requiring ventilation for 48 hours), any sepsis (systematic inflammatory response syndrome [SIRS], sepsis and septic shock), any non-surgical complication (any complication except surgical complications), cardiovascular complications (pulmonary embolism, stroke/cerebrovascular event, cardiac arrest, myocardial infarction and deep vein thrombosis/thrombophlebitis) were the complication endpoints.
Statistical analysis
Categorical data were described using absolute numbers and percent prevalence (%) in the study cohort. Continuous variables were presented as means (±standard deviation). Categorical variables were compared by use of the chi-squared test or Fisher's exact test, while independent two-sample t-tests were used for continuous variables or the Wilcoxon rank sum test for non-parametric data.
Multivariable logistic regression models were used to assess the association between Chx and emergency procedure while controlling for possible confounders. Confounders were identified by running regression models with Chx and one additional preoperative risk factor or demographic variable at a time as predictors and seeing how the results differed from running a logistic model using Chx alone. A change of more than 10% between the crude and adjusted odds ratio (OR) of Chx was used as evidence that the covariate was a possible confounder. A final logistic regression model was run using Chx and all confounders found this way. 9
A P value of less than 0.05 was considered the limit for statistical significance. Patients of age >90 years were transformed into 90 in the database. Data were analyzed using SPSS 19 (SPSS Inc, Chicago, IL, USA) ORs are presented with 95% confidence intervals.
Results
Patients’ characteristics and risk factors
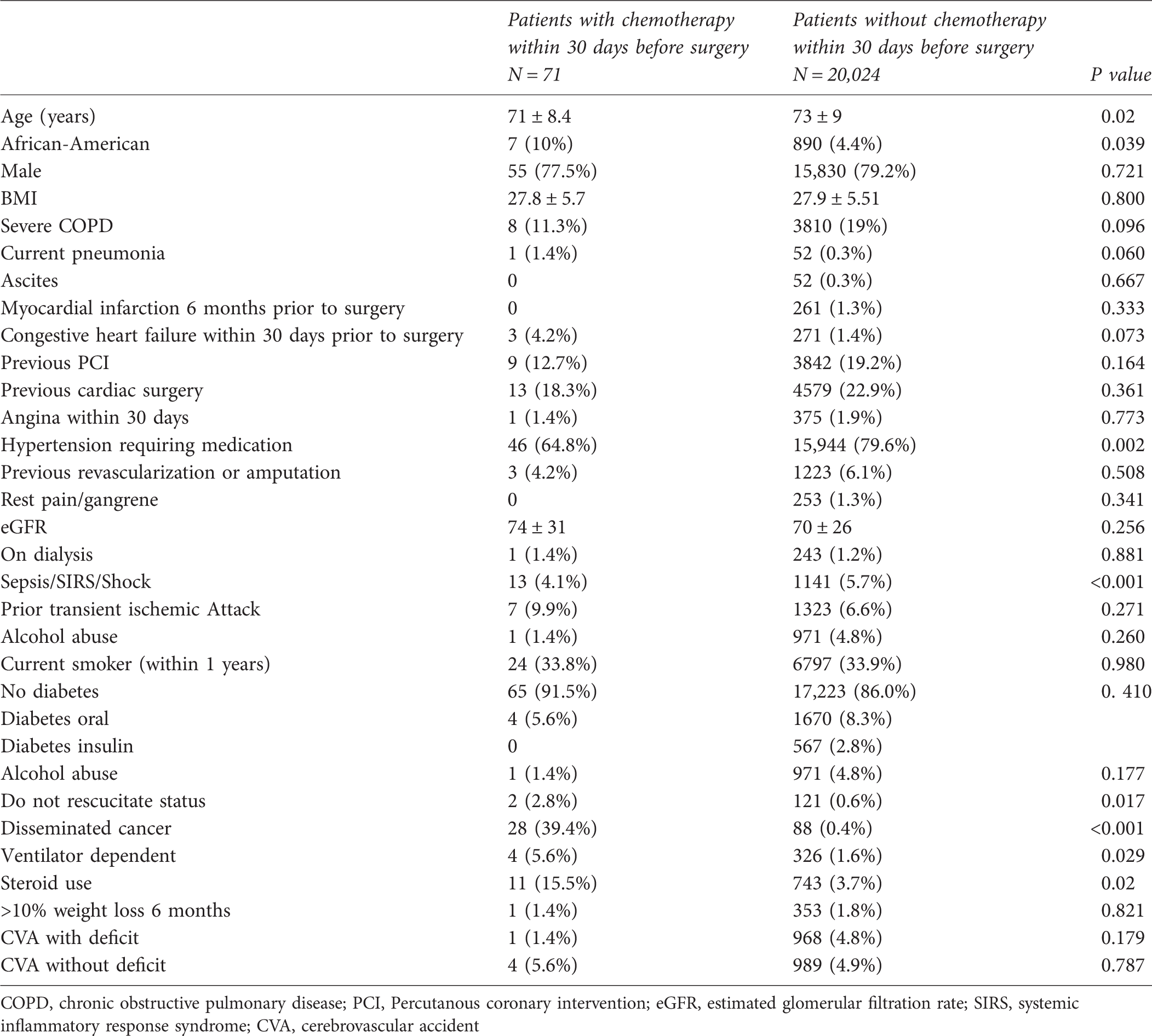
COPD, chronic obstructive pulmonary disease; PCI, Percutanous coronary intervention; eGFR, estimated glomerular filtration rate; SIRS, systemic inflammatory response syndrome; CVA, cerebrovascular accident
Patients with disseminated cancer and recent Chx (n = 28, 39.4% of group A) presented as emergency in 40% of the cases, while patients with disseminated cancer without Chx (n = 88, 0.4% of group B) presented emergently in 21% of the cases (P = 0.086).
Patients in groups A and B were different with respect to perioperative risk as mirrored in the American Society of Anesthesiologists (ASA) classification. At the time of surgery 41% of patients in group A were classified as ASA IV–V patients while 28% in group B (P = 0.004).
Multivariate analysis for emergent repair of patients with repair of aorto-iliac aneurysms

Type of repair was not significantly different between the two groups, with endovascular repair performed in 68% of Chx patients and 65% of patients without Chx (P = 0.656).
Duration of the procedure and length of postoperative stay were not significantly different between the two groups (A: 170 ± 112 minutes, B: 184 ± 92 minutes, P = 0.195 and A: 6.4 ± 9 days, B: 5.7 ± 9 days, P = 0.529, respectively). The groups differed significantly in preoperative serum sodium (A: 138, B: 139, P = 0.003), serum creatinine (A: 1.3, B: 1.2, P = 0.01), serum albumin (A: 3.3, B: 3.8, P < 0.001), total bilirubin (A: 0.53, B: 0.68, P = 0.009) and hematocrit value (A: 34.6, B: 39.6, P < 0.001). There was no significant leucopenia due to Chx or leucocytosis due to the increased incidence of SIRS/sepsis in the Chx group (A: 9.04, B: 8.12 leucocytes/nL, P = 0.284).
Operative parameters
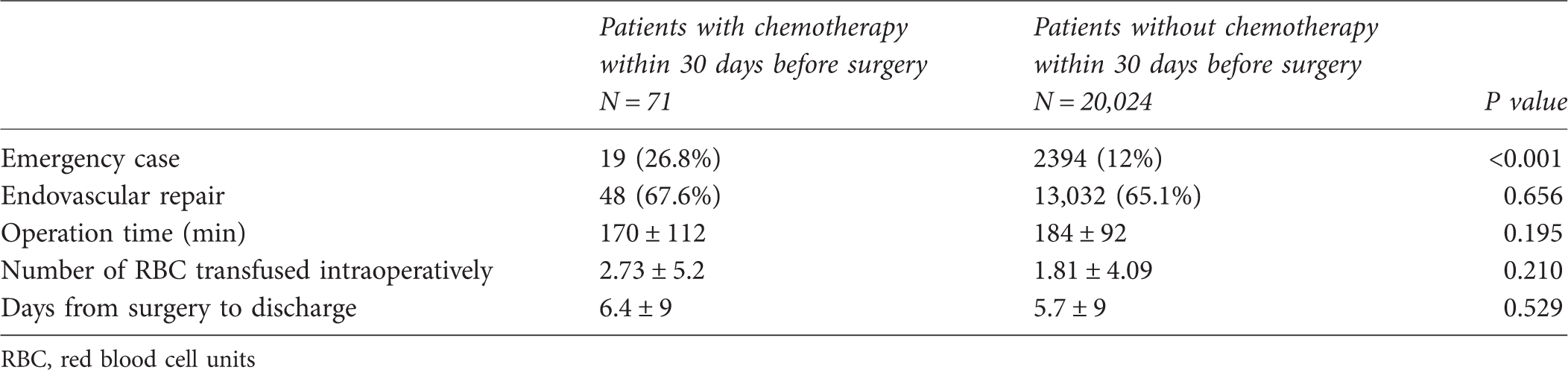
RBC, red blood cell units
Thirty-day outcome of patients with (group A) and without prior chemotherapy (group B)
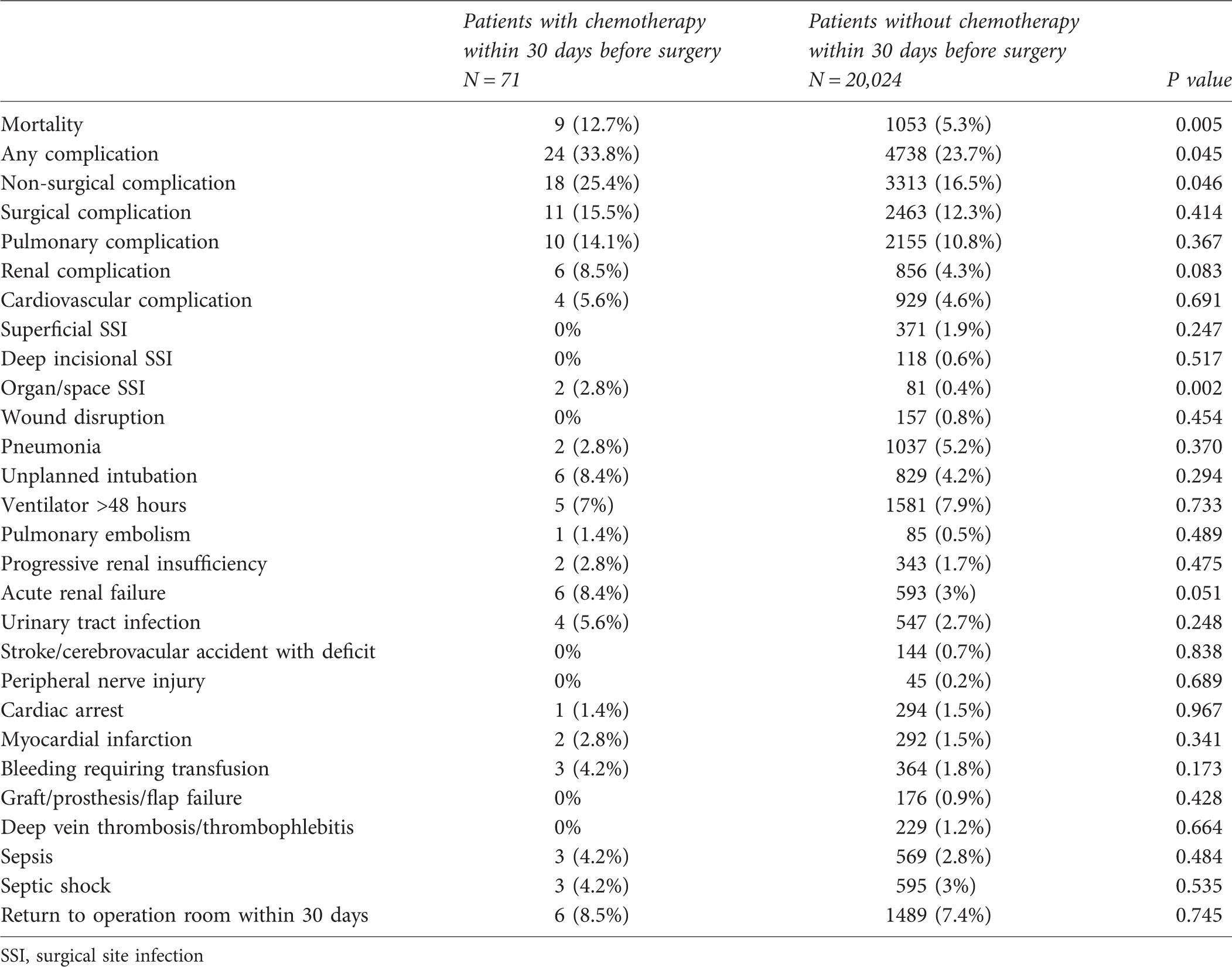
SSI, surgical site infection
In univariate analysis risk of death, any complication and acute renal failure were significantly higher in the Chx group (Table 4). This was mainly driven by the fact that Chx patients presented more frequently as emergency procedures, leading subsequently to more deaths and worse outcome.
In group A, mortality in elective cases was 0% (0/40) and 8.3% (1/12) for endovascular and open repair, respectively (P = 0.231), and in emergent cases 50% (4/8) and 36% (4/11), respectively (P = 0.658). In group B, mortality in elective cases was 1.4% (169/12,022) and 4.1% (223/5216) for endovascular and open repair, respectively (P < 0.001), and in emergent cases 18% (151/841) and 32.8% (510/1553), respectively (P < 0.001).
Discussion
Risk of AAA rupture is known to increase with aneurysm size, geometry growth rate, smoking, chronic obstructive pulmonary disease, female sex, hypertension and smoking.10,11 Apart from the above, several other risk factors have been presumed to accelerate aneurysm growth and increase risk of rupture such as prolonged use of corticosteroid or immunosuppressive medication.12,13 In contrast, Dobrin et al. 14 showed the positive effect of corticosteroids on aneurysm suppression and aortic wall degeneration.
Malignant diseases are among the main causes of induced immunosuppresion caused either by the disease itself or by the effect of Chx. Chx has been reported to cause cardiac toxicity, thrombus formation or even aortic dissection in an otherwise healthy aorta.15–17 Scarce evidence suggests a correlation between malignancy, Chx and aneurysmal degeneration.6,18 In these few case reports,6,18 growth rate substantially exceeded the expected 0.11 cm expansion per year for aneurysms 3–3.9 cm 19 or 0.13 ± 0.15 cm per year for ectatic aortas between 2.5 and 2.9 cm. 20
Vascular specialists often face the challenge of managing patients with malignancies and concomitant AAA that require repair and several treatment strategies have been suggested. However, no data exist about the natural course of pre-existing AAA in patients receiving Chx or the risks of performing AAA repair after recent Chx. Therefore, no recommendations are available regarding intervention or optimal time of intervention for patients with AAA who undergo Chx or are planned to do so.
Interpretation of results
The present study represents the first and largest study to report results of aortoiliac aneurysm repair in this unusual cohort of vascular patients with recent Chx. A total of 71 patients (group A) who received Chx within 30 days prior to surgery were identified. These patients were slightly younger than the other patients undergoing aortoiliac repair in the same time period and presented more often as emergent cases requiring surgery within 12 hours.
In multivariate analysis, recent Chx was an independent risk factor for emergency procedure. Patients with disseminated disease and recent Chx presented two times more frequently as emergency when compared with patients with disseminated cancer without recent Chx (41% versus 20%), but this did not reach significance (P = 0.086).
This observation should be interpreted cautiously in knowledge of the limitations of the NSQIP database and the absence of similar data from other studies.
The higher rate of emergencies in patients with disseminated cancer and Chx when compared with disseminated disease without Chx could suggest that Chx patients are at a higher risk of presenting emergently even within the group of patients with disseminated disease. The fact that only 2.8% rate of patients were declared as ‘do not resuscitate’ (DNR) patients in the Chx group could suggest that they were not at a very bad general condition but could also just reflect a failure of counseling regarding palliative care and DNR status.
The increased rate of aortic emergencies in patients with recent Chx could potentially be attributed to the effect of Chx, an argument supported by the fact that disseminated cancer itself was not associated with a higher risk of emergent repair. According to this hypothesis, Chx could be regarded as a factor that alters the natural course of AAA causing rapid growth or rupture.
The limitations of the NSQIP database, however, do not allow reaching such a firm conclusion.
Unfortunately, it is not known whether patients presenting as emergencies had a newly diagnosed aneurysm that rapidly progressed under Chx. It is unlikely that a large AAA would be overlooked, since most patients with malignant disease undergo some kind of imaging of the abdomen during staging. 21
It is also not known whether surgeons chose to avoid elective repair in these patients due to their malignancy and therefore a subset of them presented emergently unrelated to a direct action of the chemotherapeutic agent. Furthermore, since NSQIP only tracks surgical procedures, it is unknown how many patients received chemotherapy and did not rupture or were not offered surgery when they did rupture.
Another issue is that of aneurysm size and its effect on rupture rates. It is likely that some surgeons would ‘wait’ until the aneurysms were larger in the cancer group before feeling the pressure to operate. This would naturally result in a higher rupture risk in that cohort.
Absence of data on preoperative aneurysm size as well as the reason for emergency procedure do not allow us to reach any conclusion regarding the effect of Chx on the aorta and whether aneurysms became symptomatic at a smaller size or whether aneurysms treated electively were larger than those treated in the normal population.
The differences between groups with and without Chx should be mostly attributed to the presence of malignancy. Disseminated malignant disease was present in 40% of the Chx patients, while the wide use of steroids in the same group reflects treatment regimens of cancer patients.
The effect of prolonged corticosteroid therapy was not included in the regression analysis given the fact that it is a substantial element of Chx regimens, thus making it impossible to differentiate its effects from those of Chx.
The higher rate of patients presenting with signs of SIRS or sepsis is probably associated with the more frequent presentation of Chx patients as emergencies since positive SIRS criteria are also commonly found in stress situations as aortic emergencies (two or more of the following: temperature >38 or <36℃, >90 beats per minute, >20 breaths/minute or PaCO2 <32 mmHg, white blood cells >12,000 cell/mm3, <4000 cells/mm3 or >10% immature (band) forms or anion gap acidosis).
Sullivan et al. 22 demonstrated that patients who received recent Chx were shown to have significantly higher rates of mortality and morbidity in emergent operations in comparison to a control group in another NSQIP study. We were able to demonstrate higher rates of postoperative mortality in patients undergoing aortoiliac surgery for aneurysmal disease but this was mainly driven by emergent indication for surgery and the effect of Chx lost significance in multivariate analysis when controlling for emergency.
We were not able to show a difference between open and endovascular repair in this study, probably due to the sample size. However, the use of endovascular repair for anatomically suitable patients who have received recent Chx or patients who are about to be treated with Chx appears reasonable in the authors’ personal opinion to minimize trauma and perioperative complications.
This is a study from a registry database. Limitations due to the database design are expected especially when a specific surgical entity is addressed. In this study, data concerning the type of malignancy, stage of disease, type, dosage and application form of the Chx are not available. Thus, we cannot identify specific Chx agents, dosages or Chx regimens that are more likely to affect outcome. Furthermore, data beyond 30 days are not available, which is a major limitation of any study concerning patients with malignancy. Data were collected from more than 300 hospitals in the USA so that a uniform pattern of patient management or indication of surgery is hard to identify.
Conclusion
Patients with recent Chx for malignancy present more frequently as emergencies and therefore have worse 30-day outcomes. The reason for this cannot be sufficiently explained by the NSQIP database and patient selection through physicians could be a relevant factor. The possibility, however, of Chx affecting the natural course of AAA should be further evaluated in studies focused on this question.