
Abstract
The American Heart Association recommends that, unless contraindicated, all patients undergoing surgical revascularization for critical limb ischemia should be placed postoperatively on antiplatelet therapy and remain on it indefinitely. The goal of this study was to evaluate if preoperative use of aspirin was associated with improved bypass grafting patency rates and limb salvage. We performed a four-year, retrospective review of one center's experience with open infra-inguinal bypass. We examined the effect pre- and postoperative usage of antiatherosclerotic agents (i.e. aspirin, statin, etc.) have on graft outcomes such as two-year secondary patency, stenosis and limb salvage via univariate Kaplan–Meir survival curve analysis and multiple regression analysis. Our cohort included 165 bypasses in individuals with multiple co-morbidities. The most frequent indication was critical limb ischemia (79%) and most bypasses crossed the knee (63%). Pre- and postoperative aspirin usage was associated with increased two-year secondary prosthetic graft patency over control (preoperative: 78% versus 44%, P < 0.002 and postoperative: 72% versus 50%, P < 0.01). Preoperative aspirin usage was associated with an improvement in the rate of amputation (odds ratio [OR] = 0.44 [95% CI 0.198–0.997]) and stenosis (OR = 0.45 [95% CI 0.217–0.956]). Medications commonly prescribed for atherosclerosis such as aspirin are associated with a significant patency benefit when administered pre- and postoperatively. In a population undergoing infrainguinal bypass with prosthetic graft for predominantly critical limb ischemia, medical optimization should include both pre- and postoperative antiatherosclerotic drug regimens.
Introduction
The American Heart Association (AHA) recommends with class 1A evidence that, unless contraindicated, all patients undergoing revascularization for critical limb ischemia should be placed postoperatively on antiplatelet therapy and remain on an antiplatelet medication indefinitely. 1 Within these same set of recommendations, there is support for daily antiplatelet therapy to reduce the risk of myocardial infarction, stroke and vascular death among individuals with peripheral arterial disease (PAD). Although these general recommendations affect treatment patterns, they do not describe what influence preoperative antiplatelet therapy has on graft patency.
Lower extremity arterial reconstruction is most commonly performed in patients with moderate to severe limb ischemia secondary to progressive atherosclerotic PAD. Surgical revascularization of the lower extremity is a safe, effective and proven therapy for acute and chronic ischemia. Henke et al. 2 described that patients undergoing lower extremity surgical revascularization, as a group, are greatly under-prescribed cardioprotective medications recommended by the AHA including statin agents, angiotensin converting enzyme inhibitors and antiplatelet agents (i.e. aspirin and clopidogrel). In fact, only 50% of their patient population had been on statin therapy at the time of surgery. Their work demonstrated a patency benefit from statin use and suggested that greater preoperative use of these medications could contribute to improved patency with decreased morbidity and mortality rates.3,4
Several factors have a significant negative impact on lower extremity bypass patency rates. These include poor conduit, inadequate inflow/outflow, diseased arterial target vessel, diabetes, renal failure, dialysis dependence and critical limb ischemia.5,6 Poor conduit characteristics include small luminal diameter, low wall compliance, sclerosis and calcifications. 7 Ipsilateral greater saphenous vein is the best conduit for long-term patency. Synthetic grafts have substantially worse outcomes when compared with autogenous grafts when grafting to below the knee target vessels. As such they are chosen often as a last resort for distal revascularization after better options have been exhausted.
Patients who have many co-morbidities, have undergone multiple prior revascularization (open and endovascular) therapies and have limited autologous graft options could potentially benefit the most from preoperative optimization. Our institution is a tertiary referral center that often treats patients who meet these criteria. As such the goal of this study was to retrospectively review our institution's success with infrainguinal bypasses and to determine what impact preoperative administration of antiatherosclerotic agents has on graft stenosis, patency rates and limb salvage. Our hypothesis was that there exists a significant difference in outcome between groups treated preoperatively with medications demonstrated to have specific antiatherosclerotic benefit (i.e. aspirin) and those that were not.
Methods
This work is an institutional review board approved retrospective review of the clinical experience within our institution. The study examined the rate of vascular graft outcomes after pre- and postoperative antiatherosclerotic medication usage on all open infra-inguinal revascularization procedures performed between 1 January 2006 and 31 December 2009.
Patient selection
We queried the hospital's operative log by CPT code to identify patients who underwent infrainguinal revascularization procedures. From this data-set, only patients identified as having undergone open, lower extremity revascularization were included. Procedures that involved concurrent operations elsewhere in the body, including bilateral femoral to femoral bypass grafting and adjuvant endovascular therapies, were excluded from the cohort.
Graft surveillance
Bypass grafts were evaluated with duplex ultrasound during the first postoperative clinic visit then every 3–6 months for the first two postoperative years. After that period the frequency decreased based on the surgeon's preference. If the patient developed symptoms or findings that were concerning for ischemia the graft was then evaluated either by duplex ultrasound or by selective angiography, based on the surgeon's level of clinical suspicion.
Data collection
The study population's electronic medical records were reviewed for evidence of graft occlusion and subsequent tissue loss. We collected information pertaining to demographics, co-morbid diseases, medication use, graft patency, limb salvage and mortality. Preoperative medication usage was considered if the patient had been on the therapy for at least one month prior and up until the time of surgery. Postoperative medications were those started in the immediate postoperative period and continued throughout follow up.
Definitions
We defined primary patency as the time from the patients’ revascularization surgery until the most recent follow up that objectively documented flow through the graft (i.e. via ultrasound or angiography) without intervention to maintain flow. Primary-assisted patency included the time from the patients’ revascularization surgery until their most recent follow up that objectively documented flow through the graft even after non-surgical intervention (i.e. percutaneous angioplasty, stenting, etc.) to prevent and treat both stenosis and acute occlusion. We defined secondary patency as the time from the patients’ revascularization surgery until their most recent follow up that objectively documented flow through the graft prior to an open surgical intervention required to restore blood flow through the previously implanted graft. Those patients who required an entirely new graft to maintain limb perfusion were considered a new revascularization concluding their prior data collection and initiating new data collection (n = 8 patients). Amputation was defined as the surgical excision of ischemic tissue along the grafted extremity that had not been planned prior to revascularization.
Tabulation/statistical analysis
The data were tabulated and plotted using Microsoft Excel (Redmond, WA, USA). The tabulated data were subsequently imported into IBM's SPSS statistical software version 18.0 (Armonk, NY, USA). Kaplan–Meir survival curves and tables were generated to evaluate limb salvage, mortality, primary patency, primary-assisted patency and secondary patency rates. We performed a univariate Kaplan–Meir survival curve analysis by stratifying the population according to medication or other risk factor. As this analysis was completed in 2011, two-year patency was the basis of comparison of this cohort (2006–2009). The subsequent stratified survival curves were compared using log rank testing. Factors that demonstrated statistically significant contribution to patency, occlusion, stenosis and amputation were then analyzed using multiple regression analysis. Odds ratios for factors that had significant contribution to the aforementioned outcomes were then tabulated. P values <0.05 and confidence intervals >95% were considered statistically significant.
Results
Population
We identified 150 patients who underwent 165 infrainguinal bypasses during the study period. The redundancy corresponded to bilateral disease and re-operation for complete graft occlusion not amenable to graft intervention. The mean age was 64 and 59% of the patients were men. Patients had an average body mass index of 28 (SD 6.8), a serum creatinine of 1.49 (SD 1.63) and a serum albumin of 3.1 (SD 0.7). Bypasses were performed for lifestyle limiting claudication in 12% and the remainder had critical limb ischemia (i.e. rest pain, tissue loss). Coexisting diseases included hypertension (79%), diabetes (47%), hyperlipidemia (56%), coronary artery disease (25%), congestive heart failure (12%), chronic obstructive pulmonary disease (4%), hemodialysis dependence (15%) and active tobacco use (32%).
Bypass characteristics
Fifty-seven percent (n = 94) of the cohort used vein grafts for bypass. The remaining population used prosthetic bypasses (PTFE) with the most common indication being a lack of autogenous material due to prior harvest. The majority of bypasses (63% [n = 105]) crossed the knee to distal targets. Ten grafts (6%) originated below the knee and travelled to distal targets. Only 30% of bypasses had both inflow and outflow above the level of the knee. Bypasses included: femoral to above knee popliteal artery (n = 49, 14 vein grafts), femoral to femoral artery (n = 1), femoral to below knee popliteal artery (n = 56, 25 vein grafts), femoral to tibial artery (n = 32, 17 vein grafts), femoral to peroneal artery (n = 1, vein graft), above knee popliteal to below knee popliteal artery (n = 7, all vein grafts), above knee popliteal to anterior tibial artery (n = 6, all vein grafts), above knee popliteal to peroneal artery (n = 3, all vein grafts), below knee popliteal to anterior tibial artery (n = 3, all vein grafts), below knee popliteal to dorsalis pedis artery (n = 3, all vein grafts) and below knee popliteal to posterior tibial artery (n = 4, 3 vein grafts). As bypasses were performed for advanced atherosclerosis, all had perianastamotic endarterectomies.
Medication use
Fifty-six percent (n = 93) of patients were on preoperative aspirin therapy. In total, 67% (n = 110) of patients were on 81 mg of aspirin postoperatively started on postoperative day number one. Of note, all except four patients treated preoperatively with aspirin continued the therapy postoperatively. All four individuals not treated postoperatively underwent amputation within the first postoperative month. As there was no more graft or potential limb salvage the operating surgeons in these cases elected to forgo aspirin therapy. Fifty-eight patients were on clopidogrel postoperatively, all but four of these also received aspirin. Thirty-four patients were on coumadin postoperatively.
Follow up, salvage and survival
Mean follow-up was 426 days (range 1–2093 days). Bypass flow was evaluated in 40 of the 165 in the cohort at two years or more. The limb salvage was 83% at one year and 80% at two years. Patient survival was 93% at one year and 89% at two years.
Patency analysis
At two years, primary, primary-assisted and secondary graft patency rates were 29, 55 and 78%. (Figure 1) Patient gender had no statistically significant association with patency. Graft material was associated with patency. Specifically, two-year primary-assisted and secondary graft patency was 69 and 88% for synthetic and 91 and 95% for vein grafts. (Figure 2) These differences were statistically significant (P < 0.03). This cohort did not have a statistically significant difference between two-year secondary patency for all grafts that crossed the knee and those that did not (76 versus 79%; P > 0.05) (Figure 3). However, if this comparison is stratified by graft material, we found that prosthetic grafts that cross the knee were associated with reduced primary, primary-assisted and secondary patency when compared with those that do not (32, 57 and 87% versus 16, 26 and 57%; P < 0.05). There was no significant reduction in patency associated with vein grafts that crossed the knee.
Two-year patency rates for the retrospective review. The primary, primary-assisted and secondary patency rates are shown and distributed according to bypass graft material. There was poor primary patency at one year. Primary-assisted and secondary patency rates were much higher, and there was a statistically significant difference between prosthetic and vein grafts. Significance corresponded to figures displaying an asterisk ( The effect aspirin use has on patency rate when stratified according to bypass graft material. The top two images demonstrate the effect preoperative aspirin (ASA) use has on the populations’ patency rate. The bottom two images demonstrate the effect postoperative aspirin use has on the populations’ patency rate. The left two images demonstrate patency rates for those individuals who underwent bypass grafting with vein grafts. The right two images demonstrate patency rates for those individuals who underwent bypass grafting with prosthetic material. In all groups aspirin use had no deleterious effect on two-year secondary patency. Although preoperative aspirin use had only a minor improvement in vein graft patency, this improvement was significant. No difference in vein graft patency was observed with postoperative aspirin use. However, both pre- and postoperative aspirin use had a statistically significant improvement in patency for prosthetic grafts. Significance corresponded to figures displaying an asterisk ( Effect aspirin use has on patency rate when stratified according to bypass grafts that cross the knee. The top two images demonstrate the effect preoperative aspirin (ASA) use has on the populations’ patency rate. The bottom two images demonstrate the effect postoperative aspirin use has on the populations’ patency rate. The left two images demonstrate patency rates for those individuals who underwent bypass grafting above knee. The right two images demonstrate patency rates for those individuals who underwent bypass grafting that either crossed the knee or originated below the knee. In all groups aspirin use had no deleterious effect on two-year secondary patency. Preoperative aspirin use had a significant improvement in above and below graft. No difference in above knee graft patency was observed when stratified by postoperative aspirin use. However, postoperative aspirin use did have a statistically significant improvement in patency for those grafts that did cross the knee. Significance corresponded to figures displaying an asterisk (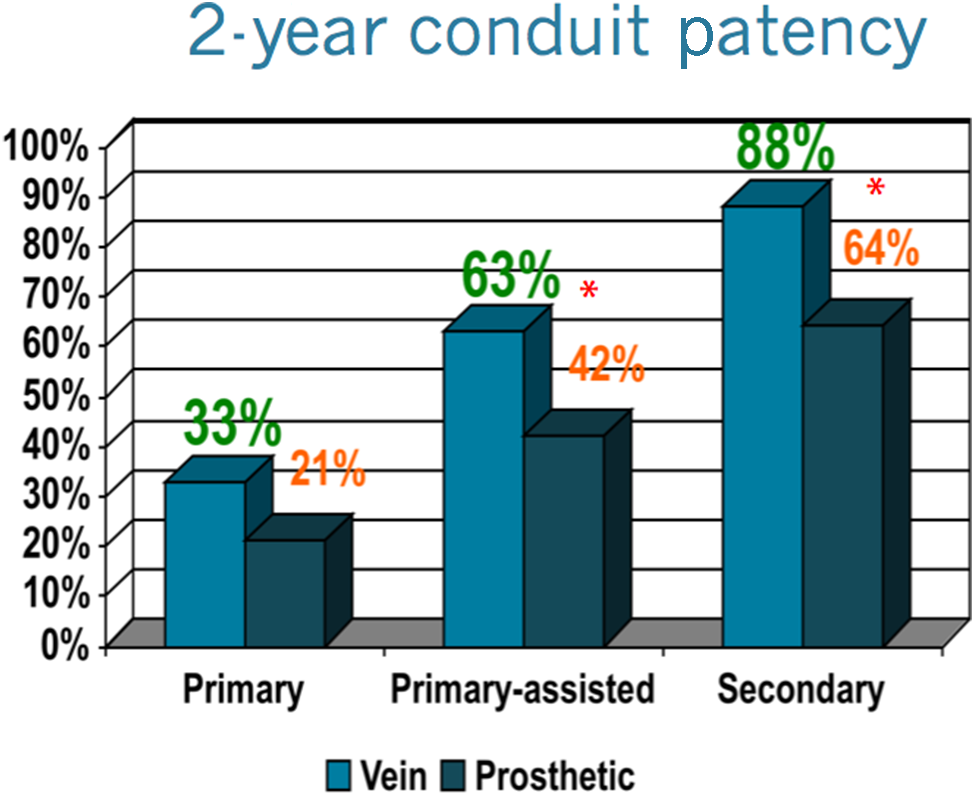

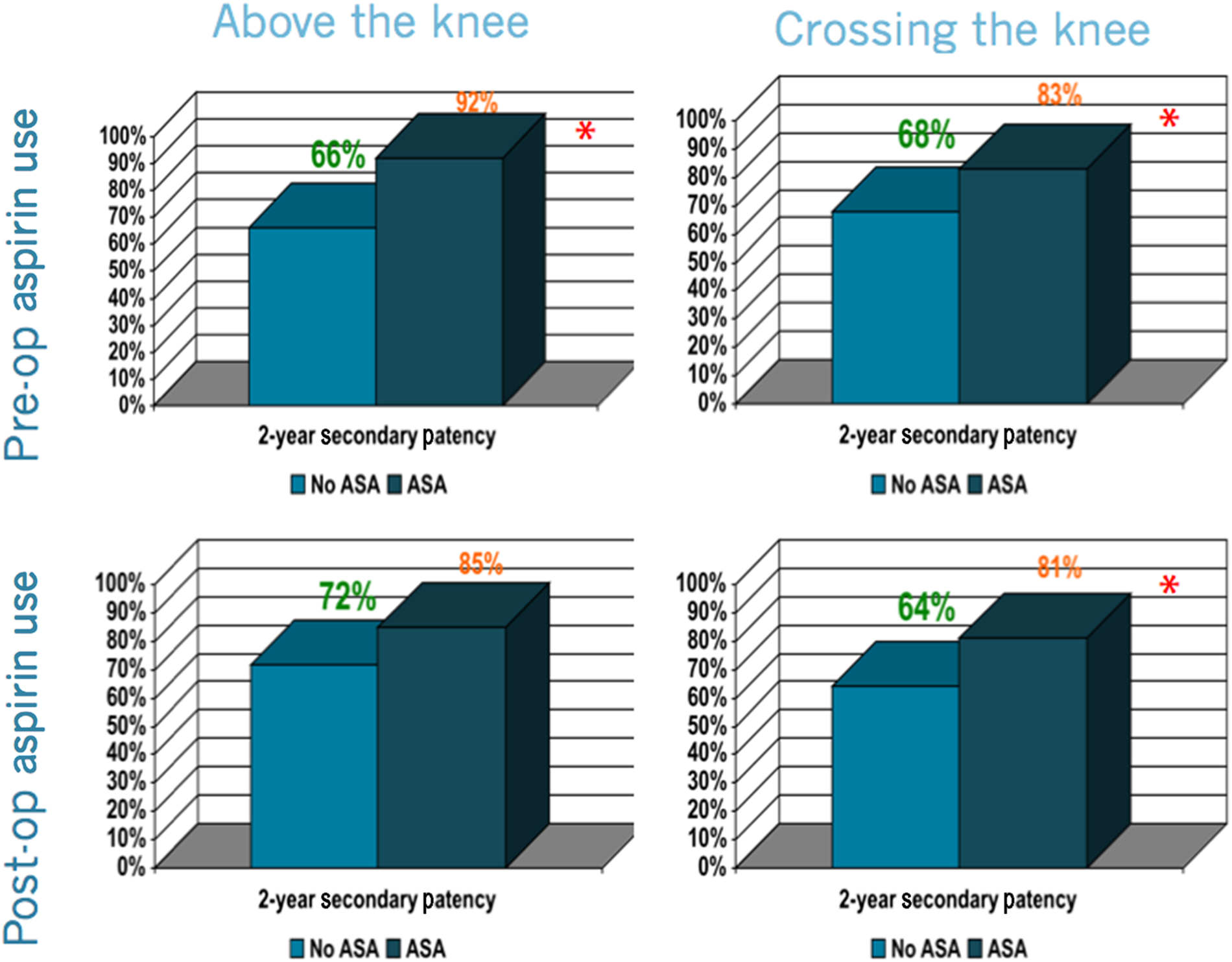
Medication usage influenced patency rates. Pre- and postoperative aspirin usage was associated with increased two-year secondary prosthetic graft patency over control (preoperative: 78% versus 44%, P < 0.002 and postoperative: 72% versus 50%, P < 0.01). Specifically, pre- and postoperative aspirin usage was associated with increased two-year secondary prosthetic graft patency over control in those patients with prosthetic grafts that crossed the knee (preoperative: 83% versus 69%, P < 0.017 and postoperative: 81% versus 68%, P < 0.01).
Regression analysis
Regression analysis for pre- and postoperative medication use, graft material and graft knee-crossing on graft occlusion, stenosis and amputation
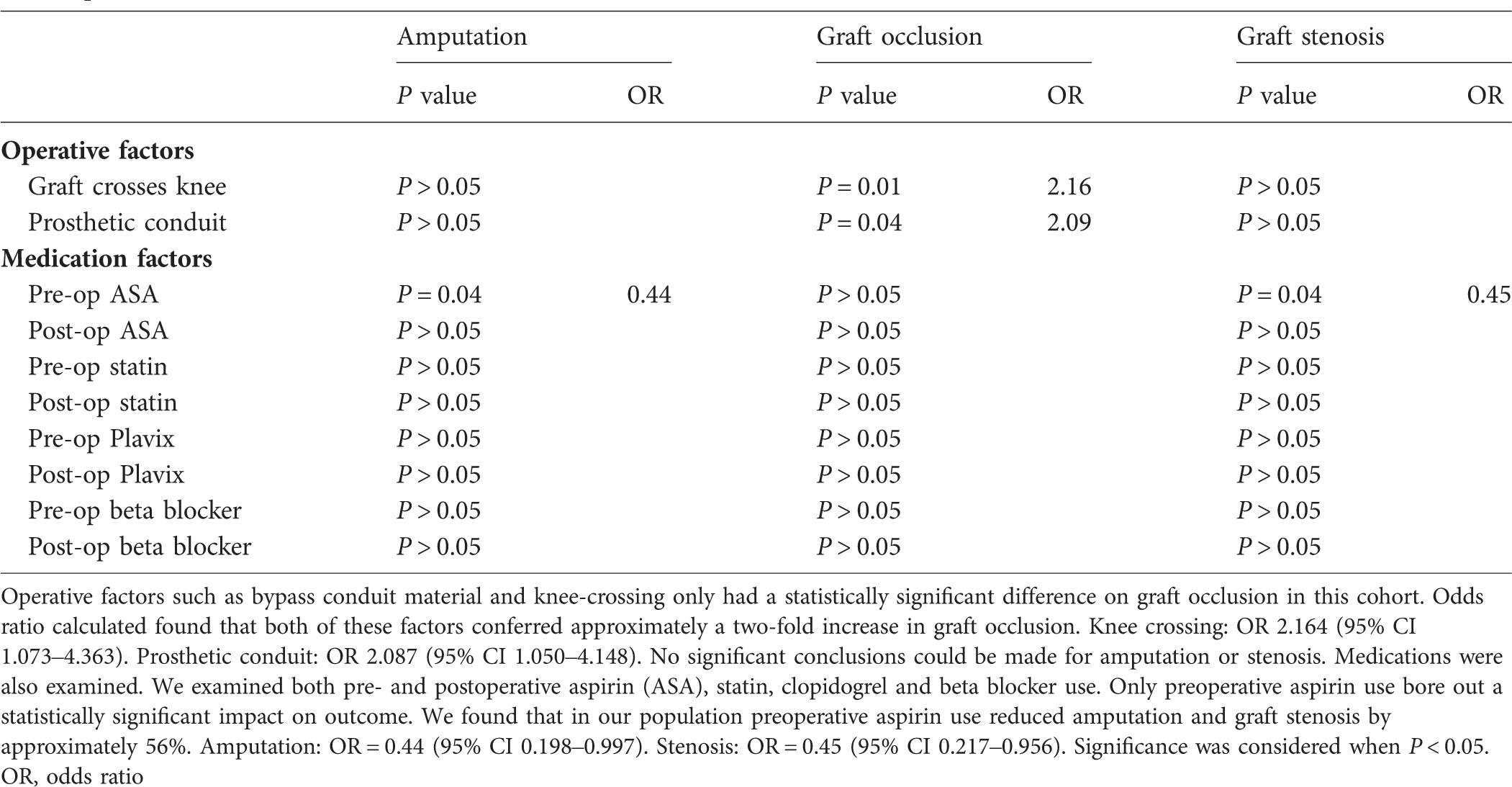
Operative factors such as bypass conduit material and knee-crossing only had a statistically significant difference on graft occlusion in this cohort. Odds ratio calculated found that both of these factors conferred approximately a two-fold increase in graft occlusion. Knee crossing: OR 2.164 (95% CI 1.073–4.363). Prosthetic conduit: OR 2.087 (95% CI 1.050–4.148). No significant conclusions could be made for amputation or stenosis. Medications were also examined. We examined both pre- and postoperative aspirin (ASA), statin, clopidogrel and beta blocker use. Only preoperative aspirin use bore out a statistically significant impact on outcome. We found that in our population preoperative aspirin use reduced amputation and graft stenosis by approximately 56%. Amputation: OR = 0.44 (95% CI 0.198–0.997). Stenosis: OR = 0.45 (95% CI 0.217–0.956). Significance was considered when P < 0.05.
OR, odds ratio
Discussion
Peripheral arterial disease is highly prevalent in the western world, affecting nearly 10 million US citizens. PAD is a significant marker for advanced atherosclerotic disease. Adverse outcomes of PAD are due to the effects of impaired circulation on essential end organs (i.e. brain, heart, extremities). Infra-inguinal occlusive disease represents the most common manifestation of PAD. Treatment includes open surgical bypass or endovascular therapy. The mainstay treatment of patients with infra-inguinal occlusive disease, especially those with critical limb ischemia, continues to be open surgical bypass.
The AHA's support for daily antiplatelet therapy to reduce the risk of myocardial infarction, stroke or vascular death in patients with lower extremity PAD has been corroborated by large series meta-analysis. 8 Patients placed on antiplatelet therapy with aspirin postoperatively had an overall positive effect on patency 12 months after the procedure when compared with no antiplatelet therapy. In fact, for patients undergoing bypass with a prosthetic conduit a statistically significant improvement in patency was seen at 1-, 3-, 6- and 12-month intervals postoperatively.
Similar to studies by Dorffler-Melly et al., 9 we found that aspirin therapy had a statistically significant improvement in patency of prosthetic grafts compared with autologous venous grafts. In our study, there was a statistically significant improvement in secondary patency at two years for those prosthetic graft patients placed on aspirin therapy postoperatively (72 versus 50%, P < 0.01). These findings agree with the aforementioned conclusions and the known benefits of antiplatelet therapy. Henke et al. 2 suggested that patients with PAD are a population that are being undertreated, and preoperative administration of antiatherosclerotic agents would benefit these individuals. Our work corroborated these findings. Moreover, we found a significant benefit was seen when patients were placed on aspirin therapy preoperatively. There was a statistically significant improvement in secondary patency at two years for those prosthetic graft patients placed on aspirin therapy preoperatively compared with no aspirin therapy (78 versus 44%, P < 0.002). This benefit was not seen in patients who underwent autologous bypass grafting. Given these data, one may infer that preoperative aspirin usage benefited our population as an adjunct to postoperative administration. However, as this study did not control for preoperative usage alone, we may not infer as to the relative impact pre- and postoperative administration have on patency and limb salvage compared with each other. Admittedly, it would be difficult to conduct a prospective study controlling for these variables, as postoperative administration of antiplatelet therapy has a well-studied benefit.
One explanation for these findings surmises that the antiplatelet effect of aspirin therapy prevents the induction of platelet deposition secondary to a local inflammatory response ascribed to prosthetic grafts. 8 Aspirin therapy may therefore improve bypass graft patency through at least two mechanisms, inhibition of inflammation and platelet deposition. A limitation to this retrospective review is that we cannot identify a clear mechanism causing these associations.
Revascularization of PAD is linked with poorer outcomes when associated with poor conduit, diseased arterial target vessel and critical limb ischemia. Our population was predominantly comprised of individuals who had critical limb ischemia, requiring below knee or distal bypass grafting with a significant number of prosthetic bypasses used due to a lack of autogenous graft material secondary to prior atherosclerotic intervention. In the present study, not only were secondary patency rates in prosthetic graft patients improved with postoperative aspirin use, but preoperative aspirin therapy was associated with statistically significantly improved patency. The authors of this paper admit that these findings were drawn from a retrospective review of a small, heterogeneous, high-risk population which may account for why there were no significant effects on primary patency. While subsequent cases are added to the database, we recommend that vascular surgeons play a more active role in their patient's preoperative medical management. Furthermore, this preoperative optimization is critical in patients where distal and/or prosthetic material grafts will be required.