
Abstract
Introduction
The aim of this study was to find a disease-specific activity score for Thromboangiitis obliterans (TAO).
Methods
About 173 admission records from 125 patients with TAO over the period 2005–2011 were evaluated. The outcome of the patients was categorized as saved-limb or limb-loss. The risk of limb loss associated with each clinical sign or symptom and complete blood count (CBC) data were then assessed. This risk assessment value was multiplied by 100 to obtain the percentage risk, which was then considered to be the risk score. The receiver operating characteristic (ROC) curve was used for demonstrating cut-offs for each score. The reliability of the risk score was evaluated using a split-half reliability test. The divergent validity of the risk score was tested using the Pearson correlation coefficient between the total scores of the patients with and without limb loss.
Results
The maximum possible clinical and CBC scores were 221 and 180, respectively, giving a maximum total score of 401. The cut-offs for clinical, laboratory and total score were 115, 75 and 213, respectively.
Conclusion
Further cohort studies for evaluating the efficacy of different treatments for limb salvage of TAO patients based on these score are suggested.
Introduction
The activity of vasculitis is usually measured using the Birmingham vasculitis score (BVAS), which aims to improve treatment and management of the disease. 1 Although some researchers consider Thromboangiitis obliterans (TAO) to be a medium and small-sized vasculitis, in most vasculitis classifications, TAO is not included. 2 To calculate the BVAS, multiple organs must be assessed, while in TAO, involvement of the visceral vasculature is rare 3 ; on the other hand, some symptoms that get very high scores in BVAS, such as paraesthesia, are common in TAO sufferers in early stages of the disease. 2 Therefore, the BVAS does not seem to be suitable for assessment of TAO activity. The aim of this study was to find a disease-specific activity score that can be used in treatment and management of TAO.
Methods
The prevalence of the clinical signs and symptoms of 125 patients suffering from TAO.
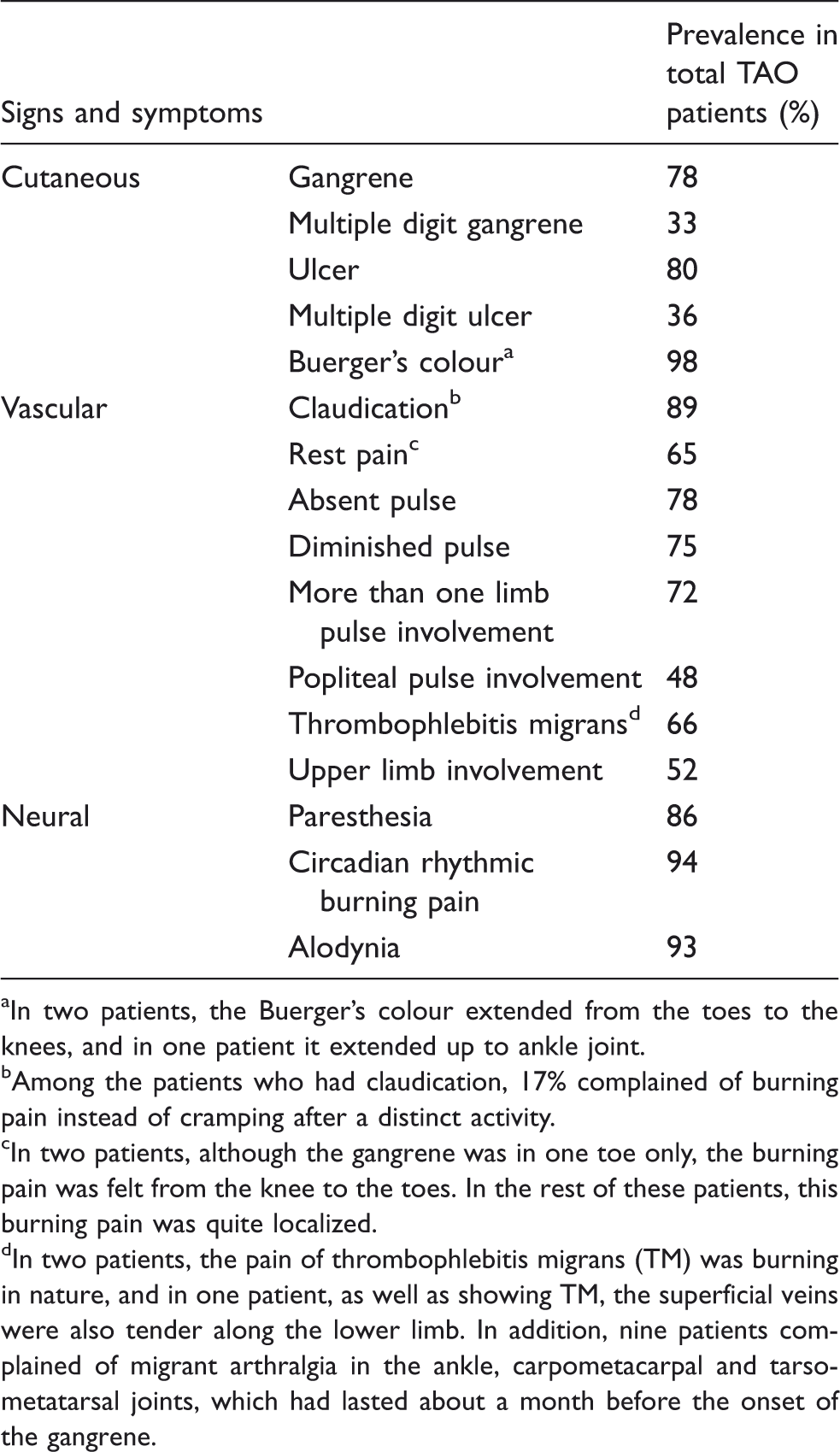
In two patients, the Buerger’s colour extended from the toes to the knees, and in one patient it extended up to ankle joint.
Among the patients who had claudication, 17% complained of burning pain instead of cramping after a distinct activity.
In two patients, although the gangrene was in one toe only, the burning pain was felt from the knee to the toes. In the rest of these patients, this burning pain was quite localized.
In two patients, the pain of thrombophlebitis migrans (TM) was burning in nature, and in one patient, as well as showing TM, the superficial veins were also tender along the lower limb. In addition, nine patients complained of migrant arthralgia in the ankle, carpometacarpal and tarsometatarsal joints, which had lasted about a month before the onset of the gangrene.
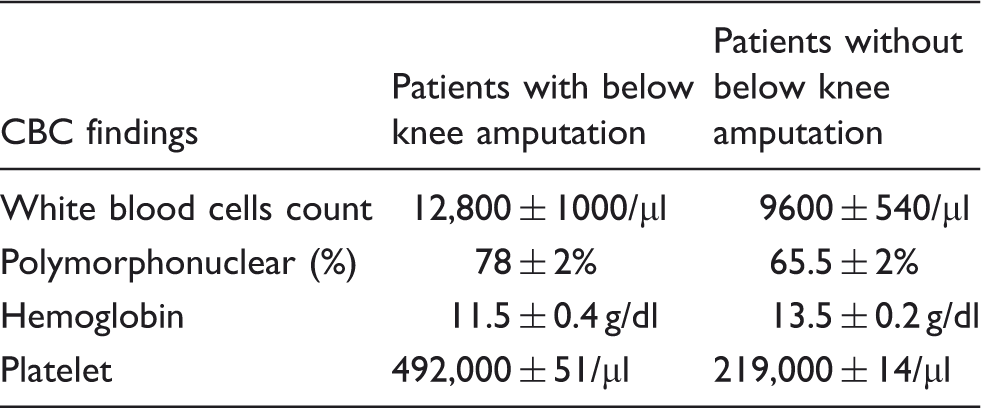
Additionally, counts of white blood cells (WBC), red blood cells (RBC) and platelets (Plt) were evaluated in all patients for any possible difference between limb loss and saved-limb groups.
Statistical Package for the Social Sciences (SPSS) version 16.0 was used for statistical analysis. The descriptive data are presented as mean ± standard deviation (mean ± SD). Normality of the data was assessed using the Kolmogorov–Smirnov test. Independent samples t-tests were used to test for any differences in clinical, laboratory and total scores between saved-limb and limb loss groups. Split-half reliability tests were used for evaluating the reliability of the clinical, CBC and total scores. The Spearman–Brown equal length (SBeq) cut-off value was considered to be 0.5. The divergent validity of the risk score was evaluated using the Pearson correlation coefficient between the total scores of the patients with and without limb loss, with no correlation confirming divergent validity. The receiver operating characteristic (ROC) curve was used for determining the cut-off point for clinical, laboratory and total score of the patients with and without limb loss. P-values of less than 0.05 were considered significant, with a confidence interval of 95%.
Results
Of the 125 patients, only one was female. Twenty-two patients (17.6%) underwent below the knee amputation. The mean ages of the patients with and without limb loss were 45 ± 1 and 40 ± 2, respectively. The prevalence of clinical signs and symptoms are summarized in Table 1.
The CBC finding of 125 patients suffering from TAO.
We also noticed that monocyte levels in 15% TAO patients were low (less than 4%). Notably, 39% of the patients had anaemia (haemoglobin (Hgb) <13.5 for male patients). The Hgb of 24 patients who had more than two admissions was evaluated. The mean Hgb level change between the two administrations (a duration of 4.43 ± 0.84 months) was 3.56, with a maximum of difference of 6 and a minimum difference of 0.9. Figure 1 shows the Hgb changes of five patients who had three or four hospital admissions over a six-month period. Unfortunately, no additional data about the patients’ reticulocyte counts or other indices for evaluating the type of anaemia (such as haemolytic anaemia), which could explain this finding, were available.
Hgb changes of five patients who had three or four hospital admissions over a six-month period.
Additionally, thrombocytosis and thrombocytopenia were observed in 6.4% and 2.9% of the patients, respectively.
A summary of the risk scores for each of the signs or symptoms recorded.

The upper limit clinical and laboratory scores were calculated as 221 and 180, respectively; hence, the maximum total score was 401. The total scores (using both clinical and laboratory results) were then calculated for 50 of the patients that did not have any missing values.
Subsequently, the 50 patients were randomly divided into two groups for evaluating the reliability of the total score, which was confirmed by the split-half reliability test (Spearman–Brown equal length = 0.687). The split-half test was also performed for clinical (SBeq = 0.51) and CBC (SBeq = 0.53) scores.
The divergent validity of the risk score was also confirmed using Pearson’s correlation coefficient of the scores for patients who underwent or did not undergo below knee amputation (p = 0.4). The lack of correlation confirmed the divergent validity of the risk score.
The mean clinical score of patients in this group who underwent below the knee amputation was 144 ± 10, with top score of 197 and lowest score of 111 (out of a maximum 221). The mean clinical score for those who had their limbs saved was 93 ± 4, with a highest score of 155 and a lowest score of 44 (out of a maximum 221). The mean laboratory scores, out of a maximum of 180, for limb loss and saved-limb groups were 112 ± 13 (with scores ranging from 50 to 140) and 23 ± 5 (ranging from 0 to 80), respectively. The mean total score for the limb-loss group was 256 ± 14 (out of 401) with a highest score of 306 and a lowest score of 171; for saved limb group, the mean total score was 116 ± 7, with a highest score of 180 and a lowest score of 44 (out of 401).
Based on an independent samples t-test, a significant difference in clinical scores was observed between those patients with saved limbs and those with below knee amputation (p = 0.001). There was also a significant difference in the laboratory scores of limb loss and saved-limb patients (p < 0.001). Based on ROC method, the cut-off point for clinical score was 115 (sensitivity 87.5%, specificity 87.5%, p < 0.001, ROC = 0.94). The cut-off point for laboratory score was also 75 (sensitivity 85.5%, specificity 98%, p < 0.001, ROC = 0.97). The cut-off point for total score was 213 (sensitivity 87.5%, specificity 100%, p < 0.001, ROC = 0.996).
Conclusion
Limb loss is one of the most tragic events that can befall sufferers of TAO, who are usually young males. The socioeconomic situation of these patients usually aggravates after the onset of their disability. 5 Furthermore, because they are almost always from low socioeconomic backgrounds and have minimal insurance cover, treatment options for these patients may be limited. 5 Therefore, finding a score to estimate the likelihood of limb loss in patients with TAO would help towards developing a treatment policy to increase the chance of saving the limb.
In this study, we reviewed all the common clinical signs and symptoms in patients with TAO and assessed the risk of limb loss that was associated with each sign. In the data analysis phase, we noted leucocytosis, anaemia and thrombocytosis in the CBC of TAO patients, in particular those who underwent below knee amputation. Therefore, the risk of limb loss correlated with CBC findings was assessed. The CBC is an inexpensive and widely available test even in low-income countries.
The SBeq of the split-half test showed that the total score was more reliable for assessing TAO activity than clinical or CBC scores individually.
To the best of our knowledge, until recently no score was used for the evaluation of TAO activity and there was no established treatment policy for different activity phases of the disease. Several expensive treatments, such as prostaglandin I2 analogues (PGI2), are not practical for use in all TAO patients, since many are of low socioeconomic status. However, if patients can be stratified according to the risk of limb loss, expensive treatments such as this can be used only in cases with a favourable cost–benefit ratio. A cohort study for evaluating the application of this score and establishment of a treatment policy is therefore recommended.
Additionally, anaemia was observed in about 40% of patients, while erythrocytosis is expected in many TAO sufferers, who are almost always heavy smokers.1,6 Although many of the patients in this study had haemoglobin levels greater than 13.5, Hgb of 13.5–14.5 is not usually expected for heavy smokers. 6 In patients that had serial CBCs taken, it was found that Hgb decreased over a short period of time; this trend did not resemble trends found in chronic anaemia as observed in other kinds of vasculitis. 7 Therefore, anaemia might be a part of pathophysiology of TAO.
Additionally, thrombocytosis and thrombocytopenia were observed in some TAO patients in the current study. As smoking does not affect platelet count, 8 it is possible that thrombocytosis and thrombocytopenia may also be a part of the pathophysiology of TAO.
Low monocyte levels were also observed in some TAO patients, especially in the below knee amputation group. This may represent weak collateralization and angiogenesis in the ischemic limb. 9
Notably, about 99% of the population study was male and it is unclear if the scoring system gives the same results for female patients.
In sum, further cohort studies are required for assessing the efficacy of the TAO activity score in patients to predict and manage limb-loss. Haematological assessment of TAO patients is also highly recommended, which may help to elucidate the pathophysiology and aetiology of TAO.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgments
The authors appreciate the Medical Record Department of Emam Reza Hospital and the support of Mashhad University of Medical Sciences for this study.