
Abstract
Objectives
To present our experience regarding endovascular stent placement for the treatment of spontaneous isolated superior mesenteric artery dissection (SISMAD) and to evaluate the safety and feasibility of the endovascular therapy.
Methods
The clinical data from six patients with SISMAD who underwent endovascular stent placement in two institutions from March 2010 to May 2012 were analyzed retrospectively. Four patients were implanted a self-expanding stent, and an additional stent was deployed in two of these patients after the first stent was implanted. One patient was subjected to a self-expanding stent implantation combined with coil embolization. The remaining patient underwent thrombectomy plus partial intimectomy 2 months before a balloon-expandable stent was implanted.
Results
All of the patients recuperated uneventfully without any reoccurrence of the symptoms in the follow-up period (range 12–38 months). Contrast-enhanced computer tomography scanning was performed 3 months after the procedure in all of the patients, and the images showed that the false lumen was nearly thrombosed and that the true lumen was maintained patent.
Conclusions
Endovascular stent placement is a simple and safe alternative to aggressive surgery or uncertain observation.
Introduction
Spontaneous isolated superior mesenteric artery dissection (SISMAD) is a very rare condition in the clinic. It is defined as a superior mesenteric artery (SMA) dissection without the presence of an aortic dissection. The first case was reported by Bauersfeld in 1947. 1 The clinical manifestations of SISMAD are diverse, and include acute abdominal pain, diarrhea, vomiting, and chronic intestinal angina. SISMAD most likely leads to catastrophic consequences, such as fatal hemorrhagic bowel infarction and arterial rupture.2,3 Three treatment options have been suggested: conservative management, open surgical repair, and endovascular stent placement. 4 Conservative management is the first choice for most patients (especially asymptotic patients), and many positive results have been reported with this treatment. 5 An emergency operation is necessary for patients who suffer from an impending arterial rupture or bowel gangrene.6,7 Interventional radiological techniques exhibit superiorities compared with conservative and surgical treatments for the patient with acute or chronic mesenteric ischemic conditions, because the endovascular stent placement can result in immediate relief from ischemia with minimal invasion. An increasing number of authors have reported the successful interventional treatment of SISMAD cases in recent years.2,8–13 From March 2010 to May 2012, 20 patients with SISMAD were admitted to the vascular department of the Clinical Medical School of Yangzhou University and the Union Hospital of Tongji Medical College of Huazhong University of Science and Technology. Six of the patients underwent endovascular stent placement successfully. All of the patients recuperated uneventfully, and the symptoms were relieved soon after the operation. We present our experience and evaluate the effect, safety, and feasibility of the endovascular therapeutic method.
Patients and methods
First, all of the 20 patients, with the exception of one patient who suffered from severe mesenteric ischemia, were administered the conservative treatment, which included blood pressure control, anticoagulation, and bowel rest, after being diagnosed. If the symptoms could not be relieved or if the diameter of the false lumen increased, interventional therapy was recommended to sustain the blood flow and/or to limit the progression of the dissection. Because the trauma of the surgical treatment is much bigger than intervention therapy, and there are more complications in the emergency open surgery, we did not recommended surgical treatment as the first choice for the patients without impending bowel gangrene.
Clinical characteristics of the patients.

These six patients were male with a median age of 52.5 years (range 45–65 years) and were diagnosed through contrast-enhanced computer tomography (CT). Patient no.1 was asymptomatic with a past history of hypertension. He received a routine examination which included a trans-abdominal ultrasound scanning which suggested the likelihood of SISMAD. Thus he received a contrast-enhanced CT and was diagnosed with type II SISMAD. Because he had no symptoms of mesenteric ischemia and his true lumen was patent, he was administered a conservative treatment combining antihypertensive and antiplatelet therapies. However, the follow-up CT revealed dilation of the niche sign, and the true lumen was obviously narrower after 3 months. To prevent further extension of the dissection, a self-expanding stent was implanted. Patients no. 2–4 suffered from upper abdominal pain and patient no. 5 suffered from left flank pain. They all received conservative treatment for one week. However, these treatments did not bring considerable relief from the pain; thus, these patients also received a self-expanding stent. After the first stent was delivered to the entry site, the patients underwent digital subtraction angiography. Based on the angiography findings, an additional stent was implanted in patients no. 3 and 5 (Figure 1). The false lumen of patient no. 4 was embolized by coils.
(a) The true lumen of the superior mesenteric artery was markedly narrowed, and an ulcer-like projection was found. (b) and (c) After two bare stents were implanted, the entry site was almost completely sealed off, and the true lumen was expanded.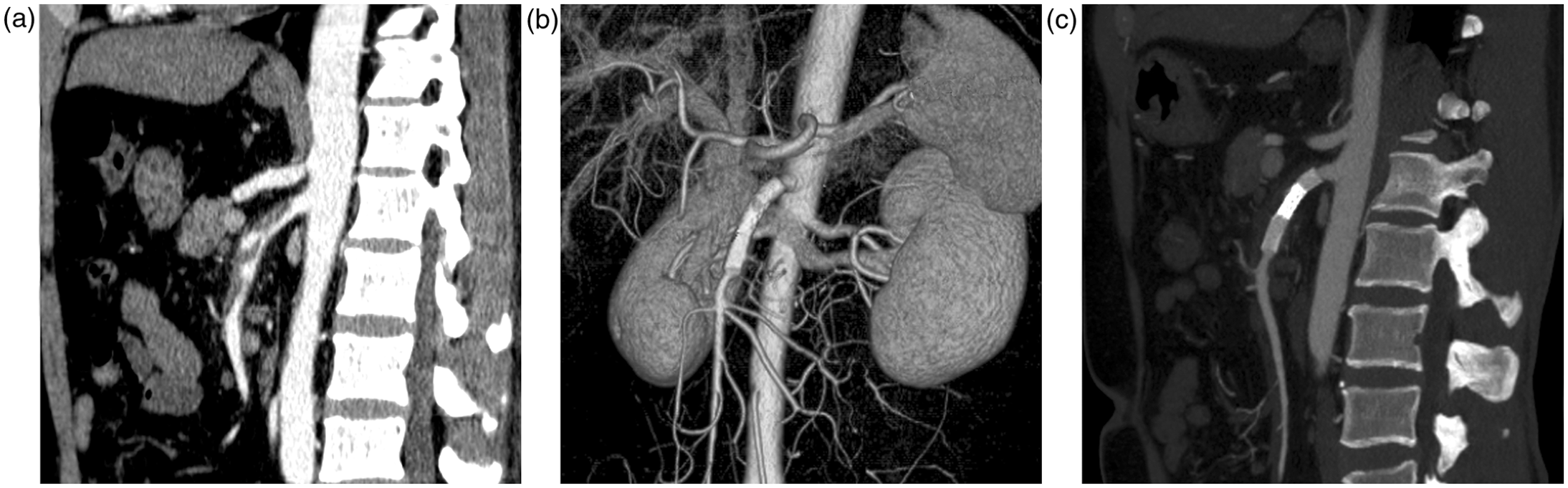
Patient no. 6 was admitted to the emergency department for severe abdominal pain, nausea, and vomiting. The contrast-enhanced CT revealed that the superior mesenteric artery was completely occluded. The emergency exploratory laparotomy found a dissection in the proximal superior mesenteric artery. The true lumen was completely compressed by the thrombosed false lumen. The patient thus underwent thrombectomy and partial intimectomy. One week after the operation, he had no abdominal pain but suffered from severe diarrhea, and his serum albumin level began to decrease continuously. The postoperative contrast-enhanced CT showed that the main superior mesenteric artery trunk remained occluded by approximately 1 cm. Nevertheless, the collateral pathway could be found around the occluded segment. We presumed that the blood supply of the intestine was not sufficient and that the chronic ischemic injury resulted in protein-losing enteropathy. Thus, we placed a balloon-expandable stent in the stenotic segment of the SMA to increase the blood supply.
Interventional technique: Using the transfemoral approach, a 6F sheath was introduced into the abdominal aorta. A 6F guiding catheter was then used as an access channel to the SMA root. It is not difficult to confirm the true lumen based on the morphology characteristics of the angiogram, such as the velocity and detention time of the contrast medium and the shape of the lumen. A 0.035-inch guide-wire was used for the selective cannulation of the distal SMA via the true lumen. Subsequently, the self-expanding stent (Precise, PRORXTM, Cordis, 6 × 40 mm) was placed in the true lumen at the level of the dissection over the guide-wire. A 0.014-inch hydrophilic coating guide-wire was more suitable for the implantation of the balloon-expandable stent (Hippocampus, Medtronic, 6 × 20 mm).
All of the patients were postoperatively managed with antiplatelet therapy for 12 months. The follow-up data included clinical examinations on an outpatient basis and a contrast-enhanced CT scan. During the first 6 months after discharge, all of the patients with SISMAD were required to receive a contrast-enhanced CT scan to evaluate the progression of the SISMAD. The patients who underwent stent implantation received a CT scan 3 months after the operation to ensure the patency of the stents. They were also recommended to obtain a CT or ultrasound scan once a year.
Results
The angiograms after the implantation of the first stent in patients no. 1–5 showed that all of their true lumens were successfully dilated by the self-expanding stent. The single stent placement resulted in the total exclusion of the false lumen in patient no. 1, and the branches of the SMA were unaffected. In patient no. 2, the blood flow of the false lumen was markedly reduced but a slight residual perfusion remained. Because the angiogram administered 10 minutes later showed a further reduction in the residual perfusion, we did not take any additional measures. The false lumens of patients no. 3–5 had not been completely sealed off, and the residual perfusion of the false lumen had not decreased compared with that observed in the preoperative angiogram. Thus, we implanted an additional longer stent inside the former stent in patients no. 3 and 5. In patient no.4, after first stent was deployed, the residual perfusion of the false lumen was more than patients no. 3 and 5 and the diameter of ulcer-like projection is more than 2 cm. We considered that an additional bare stent would not take effect and there was not flexible stent-graft available then. Thus, we chose bare stent combined with coil embolization. It can promote thrombogenesis of the false lumen and the branches originating from the true lumen will not be involved. Ten coils were delivered to the false lumen by a microcatheter that was guided through the stent mesh. The second angiogram showed nearly complete occlusion of the false lumen and restoration of excellent distal blood flow. The distal blood supply of the SMA of patient no. 6 increased markedly after the balloon-expandable stent was implanted in the stegnotic segment.
After the operation, the abdominal pain was completely resolved in patients no. 2–5, and the diarrhea experienced by patient no. 6 stopped 10 days later. During the follow-up period (range 12–38 months), all of the patients recovered uneventfully without the reoccurrence of diarrhea or abdominal pain. The contrast-enhanced CT showed that the true lumens were patent and that the false lumens were nearly thrombosed 3 months after the procedure. In the whole follow-up period, no stent migration or blockage was discovered by the ultrasound or CT scanning and the dissections in these patients were disappeared. There was no significant difference in the patency in the follow-up period between the patients who received the conservative and the interventional therapies, although the symptoms of patients received stent implantation were much severer.
Discussion
The incidence of spontaneous dissection of the SMA is 0.06%. 15 However, an increasing number of patients with or without specific symptoms were diagnosed in recent years due to the improved recognition to the SISMAD by physicians, particularly to the rapid development of modern imaging techniques. In the two institutions, twenty patients were treated within 26 months. Thus, we hypothesize that the morbidity of SISMAD in China may be higher than we realized.
The possible etiologic factors of SISMAD are considered relative to atherosclerosis, fibromuscular dysplasia, cystic medial necrosis, hypertension, congenital connective tissue disorders, and abnormal hemodynamic force due to the curvature of the SMA.16,17 The chief complaints of SISMAD patients include acute abdominal pain, diarrhea, vomiting, and chronic intestinal angina. The symptoms are likely associated with intestinal ischemia due to SISMAD or intraperitoneal hemorrhage secondary to arterial rupture. 18 Laboratory tests and abdominal radiography are usually unremarkable. Contrast-enhanced CT is the major method used to diagnose SISMAD which can provide images of mural thrombosis, intramural hematoma, and intimal flap with accuracy. And it can clearly demonstrate the patency of stent and thrombosis of the false lumen, thus it is regarded as the most important follow-up imaging after the stent implantation. More recently, CT angiography has been proven to be as accurate as catheter angiography with less trauma and cheaper price.
Sakamoto et al. 14 categorized SISMAD into four types according to the image appearances. These researchers presumed that the patients who suffered from type I and type IV dissections could be managed by conservative therapy because the blood flow was not affected by the dissection. However, the patients who suffered from type II and type III dissections may require surgery or stent placement and close follow-up because the blind-ending false lumen of type II dissection can rapidly enlarge in the acute phase and result in the occlusion of the true lumen and because the ulcer-like projection of type III dissection may progress and lead to the rupture of the SMA. Based on our observations, the natural process of SISMAD is not predictable. We have observed the spontaneous thrombosis of a large ulcer-like projection that intruded into the false lumen of a patient. In another patient with type II dissection, the false lumen remained stable during a follow-up period of 14 months. 19 Thus, we consider the follow-up of the patency of the true lumen and the progression of the dissection to be equally important in the therapeutic decision-making process.4,5
The therapeutic options for SISMAD include conservative management, surgical revascularization, and endovascular therapy, but the choice of the ideal treatment for each patient is not definite. The primary purpose of SISMAD treatment is to maintain the blood flowing distally through the true lumen, to limit the progression of the dissection and to avoid the rupture of the SMA. 4 In the last decade, the application of endovascular techniques for SISMAD has gradually increased. Compared with conservative and surgical intervention, endovascular therapy can provide immediate relief from mesenteric ischemia, prevent further progression of the dissection, and lessen the operational trauma. This therapy was initially reported by Leung in 2000. 2 We hypothesize that that the indication of endovascular stent placement should be based on the symptoms and signs, the morphologic characteristics of the dissection and the progression of the dissection during the follow-up period. These signs includes (1) the severe compression of the true lumen by the false lumen, (2) the extension of the dissection, (3) the aneurysmal dilation of the SMA, which tend to rupture,20,21 and (4) obvious symptoms that cannot be relieved by conservative treatments. 4
At present, there are no evidence-based data that support the choice of the best type of stent for each specific situation. We chose a bare stent for our patients to avoid involving the branches adjacent to the segment of dissection. In many cases, the simple implantation of a bare stent in the true lumen of the SMA dissection can cover the intimal flap, expand the true lumen and reduce the blood flow into the false lumen without occluding the branches. 11 Kim et al. 22 found that the complex flow pattern observed in the false lumen can be suppressed by stent placement and that this effect can be increased by additional stent deployment. The false lumen may be obliterated by thrombosis gradually after the procedure. 23 If the first stent did not completely seal off the entry site, the addition of one or even two stents can achieve nearly complete occlusion of the false lumen without obstructing the side branches in the stented segment. 9 For the patients with organized thrombus in the false lumen, perhaps there are some difficulties to dilate the true lumen by a self-expanding stent. Additional balloon dilatation after self-expanding stent implantation or the balloon-expandable stent can be used to ensure the patency of the true lumen.
If the entry site of the false lumen is rather large, the residual perfusion of the false lumen may not decrease significantly after one or two bare stents are implanted. The stent graft placed in the portion of the dissection can cover the intimal flap perfectly and occlude the blood inflow to the false lumen. 24 However, the stent graft is difficult to implant in the curving SMA due to its rigidity and exhibits the risk of obliterating the important side branches of the SMA, which would result in severe intestine ischemia. In our opinion, a stent graft is more suitable for the broad-base dissection of the SMA and intraperitoneal bleeding from the dissection of the SMA.25,26
If there are some important branches originating near the entry site, the use of a stent graft is not advised. The method of using a bare stent combined with coil embolization can promote the thrombogenesis of the false lumen without involving the branches originating from the true lumen. 10 The risk of coil migration or coil bulging into the true lumen is very low if the coil is tightly packed in the false lumen.
The ideal stent for SISMAD should have good flexibility and should not continuously change its location. It is more feasible to implant a balloon-expandable stent accurately than a self-expanding stent at the exact position. However, the balloon-expandable stents are stiffer, and the resulting axial force is greater. For most of the patients, the dissection involved the proximal 2–6 cm portion of the SMA. Because this segment is curved, a self-expanding stent is more commonly used due to its flexibility, adaptability, and weaker radial force. 12
Conclusions
Based on our experience and the present literature, SISMAD can be managed with endovascular stent placement successfully and safely. Although the risk of the possible occlusion of side branches in long-term follow-up and restenosis after stent placement is not definite, endovascular stent placement represents a simple and safe alternative to aggressive surgery or uncertain observation.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.