
Abstract
Introduction
We aimed to investigate whether the temperature of tumescent anesthesia is important, if so, to establish an opinion about the ideal temperature.
Materials and methods
Endovenous laser ablations were performed in 72 patients; 35 patients (Group A) received tumescent anesthesia at +4℃, while other 37 patients (Group B) received tumescent anesthesia at room temperature. The groups were compared in terms of intraoperative pain, postoperative regional pain, ecchymosis, paresthesia, skin burns and necrosis. At month 1, great saphenous vein was evaluated for recanalization and patient satisfaction.
Results
The survey on intraoperative pain showed that patients receiving tumescent anesthesia at +4℃ experienced much less pain. Interestingly, statistical analysis showed that this difference was not significant (p = 0.072). No skin burns or necrosis occurred in either group, whereas ecchymosis and paresthesia were the most frequently observed side effects in both groups, but no significant difference was found between the groups. There was no significant difference between pain levels on postoperative days and no significant difference between the groups in terms of satisfaction with endovenous laser ablation procedure and postoperative satisfaction. All venous segments treated with endovenous laser ablation in both groups were occluded. At month 1 no recanalization was observed.
Conclusion
We conclude that the temperature of tumescent anesthesia solution is not important, while the proper administration of tumescent solution in adequate amounts ensuring delivery of the fluid to all segments appears to be a more significant determinant for the success of the procedure.
Introduction
Great saphenous vein (GSV) incompetence is a serious disease with a high global prevalence, significantly impairing the quality of life and causing pain, swelling and skin color changes. 1 Along with conventional surgery (stripping and/or high ligation of GSV) and conservative treatments (veno-active drugs and/or compression stockings), a new minimally invasive method of treatment, endovenous laser ablation (EVLA), has gained popularity for the last 10 years as very positive results have been reported in the literature.2,3 EVLA of the GSV was first described by Puglisi in 1989 and its successful results were first published in 2001 in cohort studies.4,5 The original laser fiber wavelength used in the first applications was 810 nm diode laser, but different laser wavelengths such as 940 nm, 980 nm, 1064 nm, 1320 nm and 1470 nm are also used today.4−7 EVLA treatment consists of several procedural steps, the most important of which is the delivery of tumescent anesthesia into the structures around the target vein. Tumescent anesthesia prevents any sensation of pain while the laser is firing and its presence around the vein prevents the heat of the laser from being transmitted to the adjacent tissues. Although there are numerous studies in the literature evaluating and comparing the outcomes of different laser wavelengths, the optimum temperature for tumescent anesthesia applied in EVLA has not been yet well-established. In this study, we aimed to investigate whether the temperature of tumescent anesthesia is important, if so, to establish an opinion about the ideal temperature.
Materials and methods
Patients applying to our clinic between June 2011 and June 2013 with a diagnosis of GSV incompetence were re-assessed for eligibility for EVLA. After an initial medical history was taken and physical examination was performed, patients were categorized according to the Clinical, Etiological, Anatomical, and Pathological (CEAP) classification, and their demographic data were recorded. Patients were re-evaluated through ultrasound examinations of venous systems, performed using a portable Doppler ultrasound machine with a 7−13 MHz linear probe (SonoSite MicroMaxx Ultrasound machine). We measured the GSV diameter, distance from skin and reflux time at saphenofemoral junction, examining the course of GSV in different segments (10 cm below saphenofemoral junction and above segments) in an upright position. Patients with reflux time of 0.5 s and above were considered significant, and EVLA was performed in those with proper GSV course below the saphenofemoral junction and a GSV diameter of ≥5 mm. In our clinic, tumescent anesthetic solutions at +4℃ or room temperature are used in EVLA procedures, based on the surgeon’s preference. The differences in the preferences of surgeons motivated us to conduct the current study. Patients with perforating vein insufficiency or small saphenous vein insufficiency were excluded from the study. Therefore, a total of 72 patients (78 lower extremities) were included in the study. The participants were given information about the aim and content of the study, and written informed consent of all subjects was obtained before initiating any study procedures. The EVLA procedures were performed with bare-tip laser fiber and 1470 nm diode laser (Quanta System, Italy). Of the patients receiving EVLA, 29 were males and 43 females, with a mean age of 40.6 ± 16.57 (ranging from 18 to 74 years). Thirty-five randomly selected patients (Group A) received tumescent local anesthesia at +4℃, while other 37 patients (Group B) received tumescent local anesthesia at room temperature through ultrasound-guided injection of 10–15 ml of perivenous local anesthetic to each 1-cm site. The groups were compared in terms of intraoperative pain during the EVLA procedure and regional pain on postoperative days 0, 1, 10 and month 1, as well as ecchymosis, paresthesia, skin burns and skin necrosis. For patients undergoing EVLA on both extremities, these data were evaluated separately for each limb. Intraoperative and postoperative pain were measured by visual analog pain scale (0–10 rating, 0 = no pain, 10 = worst pain ever), while ecchymosis, paresthesia, skin burns and skin necrosis were assessed by the number of limbs developing such complications. Analgesic request comparison was made based on the number of days patients used analgesic drugs. During the follow-up at month 1, GSV was evaluated for recanalization and patient satisfaction about the treatment procedure and postoperative period was assessed through retrospective survey. For this measurement, we used a 5-point Likert scale (0 = extremely satisfied, 1 = satisfied, 2 = quite satisfied, 3 = dissatisfied, 4 = completely dissatisfied).
EVLA procedure
All patients were monitorized, and the EVLA procedures were performed while patients were under intravenous midazolam sedation with oxygen supplementation. GSV around the knee was determined by Doppler ultrasound examination. The GSV was punctured using a 17-gauge needle and a guide-wire inserted into the vein. The bare tip laser fiber was advanced over the guide-wire into the GSV and locked at 2 cm below the saphenofemoral junction. Under Doppler ultrasound guidance, perivenous tumescent local anesthesia (9% normal saline 1000 cc, 2% prilocaine 40 ml, 1:1000 adrenaline 1 ml, 10 mEq NaHCO3) was administered, injecting 10–15 ml of anesthetic agent to each 1-cm site. Endovenous laser energy was delivered at a power of 12 Watts, continuous mode and withdrawal of the catheter was performed, aiming for a target linear endovenous energy density (LEED) of 91.1 Joules per centimeter (J cm−1).8,9 After completing the procedure, the saphenofemoral junction was checked, and closure of the GSV was confirmed by Doppler ultrasound examination. In addition, we performed miniphlebectomy for removal of veins under local anesthesia (2% Prilocaine) in patients with varicosities requiring excision. A compression bandage was applied over the course of the treated vein for 24 h. Four hours after the procedure, each patient was administered a single subcutaneous, prophylactic dose of the low-molecular-weight heparin. On postoperative day 1, bandages were removed and patients were assessed for ecchymosis, paresthesia, pain, skin burns and skin necrosis. At the same time, patients were mobilized and checked for mobility restrictions. All patients were discharged on postoperative day 1. Patients were given 30–40 mmHg compression stockings and advised to wear them continuously for the following 10 days and walk on a regular basis during recovery period. All patients were prescribed supplementary analgesia (Flurbiprofen 100 mg/twice a day) to be used as required.
Statistical analysis
All the data obtained in this study were analyzed using the Statistical Package for the Social Sciences for Windows (SPSS Inc., Chicago, Illinois, USA) version 16.0. Preoperative and postoperative data were expressed as mean ± standard deviation (SD). For comparisons between the two groups, Chi square test was used for the nominal data, while numerical data were compared using Mann-Whitney U test. A p value less than 0.05 (p < 0.05) was considered statistically significant.
Results
Preoperative patient demographics.
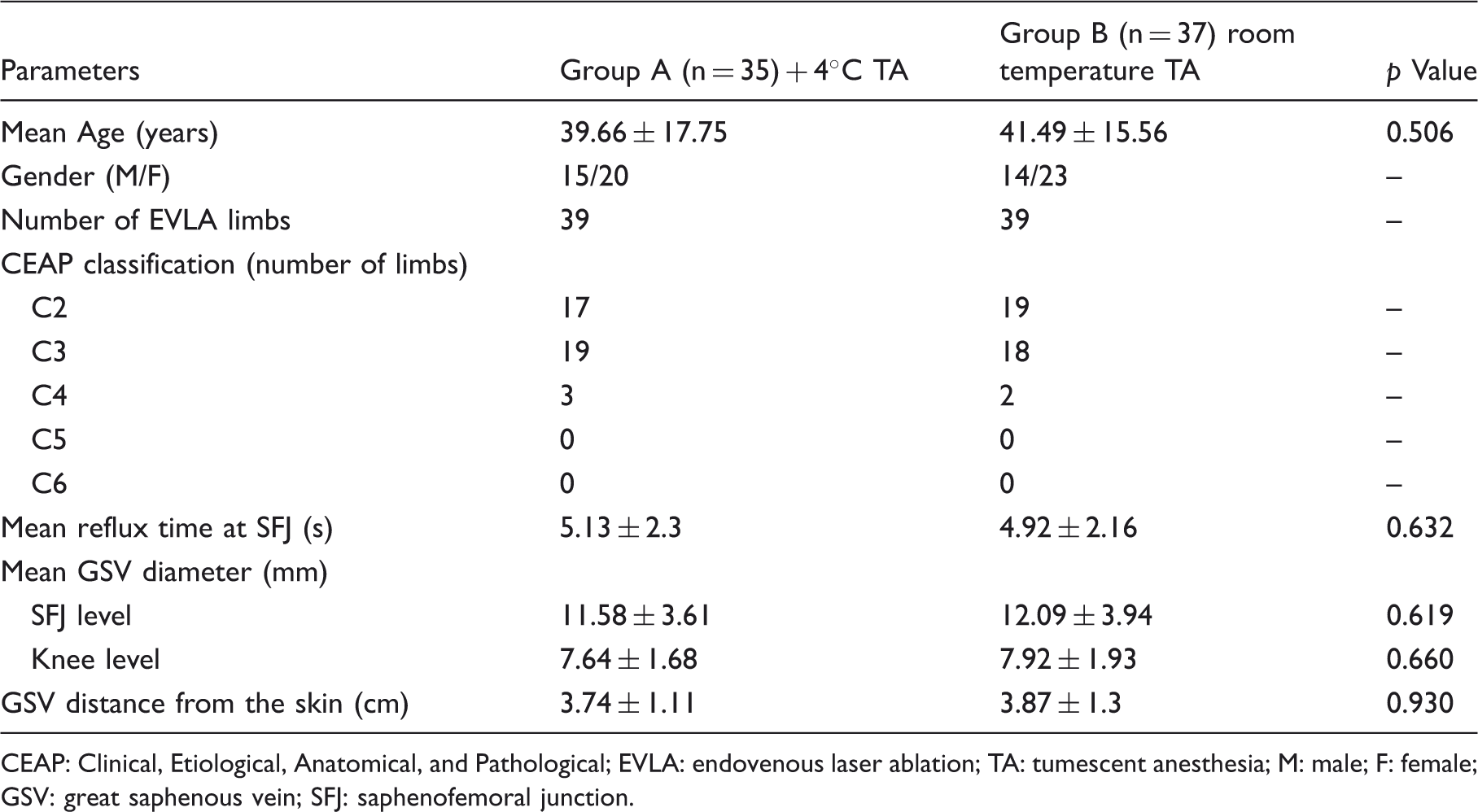
CEAP: Clinical, Etiological, Anatomical, and Pathological; EVLA: endovenous laser ablation; TA: tumescent anesthesia; M: male; F: female; GSV: great saphenous vein; SFJ: saphenofemoral junction.
Operative patient data.

GSV: great saphenous vein; TA: tumescent anesthesia; LEED: linear endovenous energy density; EVLA: endovenous laser ablation.
Postoperative patient data.
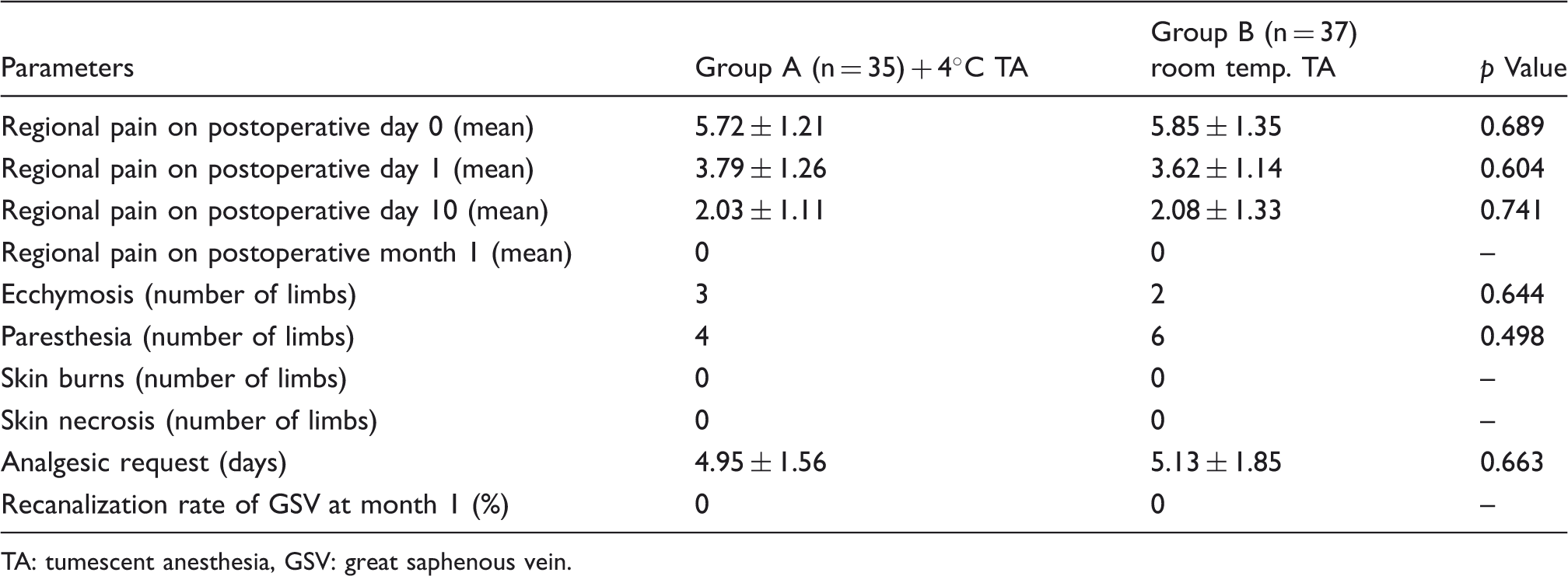
TA: tumescent anesthesia, GSV: great saphenous vein.
Patient satisfaction data.

TA: tumescent anesthesia.
Discussion
Since the first publication by Navarro et al. in 2001, 5 which reported first successful results obtained by the use of 810 nm endovenous laser wavelength, laser technology has become a popular option in varicose vein surgery. After that date, numerous health centers began to perform EVLA, reporting excellent results with minimal discomfort. These positive outcomes and increased interest have attracted the attention of medical companies, enabling further investment and research on EVLA technology. As the research evolved, longer laser wavelengths than the original 810 nm laser have been introduced in the EVLA treatments, including 940 nm, 980 nm, 1064 nm, 1320 nm and most recently 1470 nm diode laser. Longer wavelengths have been reported to reduce side effects such as postoperative pain, ecchymosis and skin burns, producing better short, medium and long-term outcomes.6–12 Although there are studies that compared the conventional surgery techniques (stripping and/or high ligation of GSV) with EVLA, and reported that EVLA treatment produced excellent results, there are other studies reporting that both methods were equally effective or EVLA was less successful. However, most of these published studies agree that EVLA procedure involves minimal discomfort with fewer complications as compared to surgery.13–16
The review of historical evolution of EVLA indicates that the studies in this field were conducted to improve the effectiveness of EVLA causing minimal patient discomfort with fewer complications and side effects. In this regard, longer laser wavelengths are generally preferred in EVLA. The reason behind the application of different wavelengths is that each wavelength has its own absorption spectrum. At lower wavelengths (810 nm–980 nm), absorption of deoxygenated hemoglobin is higher, whereas at higher wavelengths (1064 nm–1470 nm), absorption of water is higher, but absorption of deoxygenated hemoglobin is lower. 17 As a result, perforation of the venous wall during EVLA is minimized, and significantly fewer complications and adverse advents occur during and after the procedure, which ensures a successful and comfortable treatment.18,19
Laser ablation works on the principle of occluding the vein by high thermal energy. The heat produced is variable and depends on many factors. This heat varies depending on the unit of power (watt) delivered, duration, diameter of the vein, specific heat of blood and venous blood flow rate. 20 Studies measuring the amount of intravenous heat generated during EVLA report that peak temperatures at the laser fiber tip can exceed 1000℃ and continuous temperatures of at least 300℃ should be maintained in the firing zone during the procedure for an effective treatment.21,22 It is considered that extreme intravenous temperatures might cause serious thermal injury in the adjacent tissues. Therefore, correct delivery of perivenous tumescent local anesthesia is one of the most important steps of the EVLA procedure. The purpose of tumescent anesthesia, along with anesthetic effects, is to create a protective barrier by filling the perivenous space with the anesthetic fluid to prevent heating of non-target tissues by intravascular peak temperatures. Another goal here is to increase circumferential contact between the vein walls and laser fiber tip. 17
Although these considerations might suggest that cold tumescent anesthesia could produce better results, there are no studies in the literature examining whether delivering cold anesthetic solution into the perivenous space can lead to difficulties in reaching the high temperatures required for intravenous occlusion, which might result in remaining incompetent segments. Similarly, there are a limited number of studies reporting the optimum temperature for tumescent anesthesia applied in EVLA. The most comprehensive work among them is the study conducted by Pannier et al. in 2010. In this study, Pannier et al. 23 compared the outcomes of EVLA procedures using warm (37℃) tumescent anesthesia with those using cold (5℃) tumescent anesthesia. The results showed no significant difference between the two groups in terms of pain and ecchymosis, while the intake of analgesics in the cold tumescent anesthesia group was significantly lower. 23
In our study, ecchymosis and pain was found to be low in both groups. While intraoperative pain during the procedure was much lower in the group receiving cold (+4℃) tumescent anesthesia, there was no significant difference in postoperative pain scores on day 0 and following days. Interestingly, statistical comparison of intraoperative pain during the EVLA procedure showed no significant difference between the groups (p = 0.072). None of our patients experienced complications like skin burns or skin necrosis, but the most common complaints in both groups were paresthesia and ecchymosis, respectively. There was no statistically significant difference between the groups in terms of paresthesia and ecchymosis. Contrary to the results reported by Pannier et al., consumption of postoperative analgesics in our study did not differ significantly in the two groups. The Doppler ultrasound examinations performed immediately after the procedure and on the following days demonstrated that laser ablation totally occluded the target vein along the entire segment, and administration of cold tumescent anesthesia did not cause any incompetent segments. At 1-month follow-up, no recanalization was detected in patients.
While most authors agree on the importance of tumescent anesthesia, the ideal temperature for the tumescent solution is a highly controversial topic. Advocates of cold tumescent anesthesia argue that it should reduce the side effects that may occur in the surrounding tissues due to high temperature. On the other hand, proponents of warm tumescent anesthesia assert that the use of cold anesthetic solution inhibits generation of high temperatures required for intravenous occlusion, which might result in unoccluded segments and a higher risk of early recanalization. Our study revealed that there was no difference between the two groups in terms of the parameters examined during and after the procedure. In the same way, all venous segments treated with laser ablation using either cold or warm anesthetic solution were occluded, and no recanalization was observed at the 1-month follow-up.
Conclusion
We conclude that the temperature of tumescent anesthetic solution is not important, while the proper administration of tumescent solution in adequate amounts ensuring delivery of the fluid to all segments appears to be a more significant determinant for the success of the procedure.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.