
Abstract
Objective
The aim of the present study is to evaluate whether blood count parameters differ according to the stages of Fontaine’s classification and to investigate the relationship between hemogram parameters and the severity of the disease.
Method
Eighty-two peripheral arterial disease patients were examined prospectively. Patients were classified according to the Fontaine classification system. Fifty newly diagnosed patients were included in the study. The neutrophil-to-lymphocyte ratio, mean platelet volume, and red blood cell distribution width values were recorded.
Results
Mean neutrophil-to-lymphocyte ratio values were found to be 3.31 ± 1.1% in Stage I, 3.11 ± 1.3% in Stage II, and 3.48 ± 1.1% in Stage III (p > 0.05). Mean platelet volume values were found to be 7.8 ± 0.6 fl (Stage I), 8.2 ± 1.0 fl (Stage II), and 9.0 ± 0.9 fl (Stage III) (p < 0.05). Red blood cell distribution width values were found to be 13.6 ± 1.0% in Stage I, 14.8 ± 1.7% in Stage II, and 15.4 ± 2.3% in Stage III, being significantly different among all three stages (p < 0.05).
Conclusion
Both red blood cell distribution width and mean platelet volume are found to be associated with the severity of atherosclerotic disease in patients with peripheral arterial disease. This finding hypothesizes that complete blood counting parameters may serve as a beneficial and cost-effective method for monitoring atherosclerotic peripheral disease.
Keywords
Introduction
Peripheral arterial disease (PAD) is an important age-dependent disease that is related with high morbidity rates and strongly disrupts the quality of life. In symptomatic patients, claudication is the main presenting complaint in PAD. 1 There are the two valid classification systems for patients with PAD currently. Fontaine’s Stages and Rutherford’s Categories are used to identify the severity of the symptoms in PAD. Rutherford’s Categories is an improved form of Fontaine’s Stages including more subcategories. Nevertheless, basic scopes are similar in both two classification systems. 2 These classification systems are based on patients’ symptomatology and do not include any laboratory parameter. In the present study, we aim to search if some of blood count parameters have a statistically significant correlation with the severity of PAD.
Recent studies have also focused on clarifying the possible interactions between routine blood parameters and disease severity. These parameters have also been investigated to see whether a relationship exists between cardiovascular risk and PAD population. 3 The role of inflammatory processes in atherosclerosis, which is closely associated with PAD, has also been well described.3,4 These data encouraged researchers to investigate the complete blood count parameters in atherosclerotic events. Interactions have been detected between platelet function and vascular events in previous reports.3,4 Thus, mean platelet volume (MPV) was investigated in atherosclerotic vascular disorders as an indicator of platelet activation and reactivity.
Briefly, MPV is a descriptive indicator of increased size and more reactive platelets.5,6 Other inflammatory markers such as white blood cells and their subtypes (e.g., neutrophils, monocytes, lymphocytes, and eosinophils) have also been studied in various cardiovascular diseases. 3 The neutrophil-to-lymphocyte ratio (NLR) is a current concerted version to the long list of these inflammatory markers. 7 Red blood cell distribution width (RDW) a coefficient measure of the size variability of circulating erythrocytes, is shown to be strongly related with the risk of cardiovascular morbidity and mortality. The relation between RDW and atherosclerosis also has been investigated. 8
In the current study, the relationship between routine blood parameters and the severity of the symptoms of PAD according to Fontaine’s Stages was investigated.
Patients and methods
Study design and patient selection
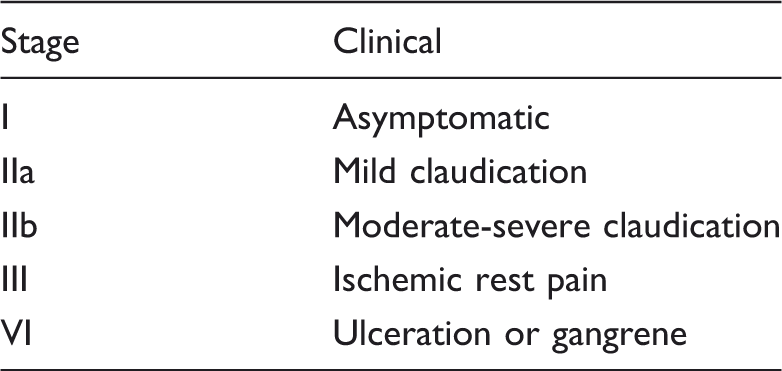
In this cross-sectional study, 82 consecutive PAD patients were examined prospectively. The severity of their symptoms was categorized according to Fontaine’s Stages (Table 1) as described in previous literature.
2
Exclusion criteria included the following:
–Fontaine Stage IV patients who have gangrenous or necrotic lesions were excluded in order to avoid the possible effect of infection in complete blood count parameters, –Patients with other systemic problems such as hematological disease, acute or chronic infections, liver disease, and drug usage (especially, antiaggregants, anticoagulants, and steroids) were excluded. Fontaine Stages in patients with peripheral arterial disease.
2
Among 82 PAD patients, 50 newly diagnosed patients without previous treatment were included in the study. Patients were divided to three groups: Fontaine Stage I, II, and III. Ethical approval was granted from a local ethics committee. Study participants were informed about all contents of the study and informed consent was obtained.
Blood sampling
Peripheral venous blood samples were obtained from each patient during a routine blood draw. Each sample was drawn into vacutainer tubes containing 0.04 mL of 7.5% K3 salt of EDTA and was analyzed within 1 h after sampling with a commercially available analyzer (CELL-DYN 3700; Abbott Diagnostics, Abbott Park, IL). The NLR (%), MPV (fl), and RDW (%) values were recorded for each patient and were compared between groups.
Statistical analysis
All statistical procedures were performed using SPSS (Statistical Package for Social Sciences) software version 15.0 (SPSS Inc., Chicago, IL). Means were given together with standard errors, and frequencies were expressed as percentages. The t-test was used to compare the two independent groups. The relation between the severity of symptoms which was assessed using Fontaine’s Stages and complete blood count parameters was analyzed through the method one-way analysis of variance. A p value of 0.05 was considered statistically significant and Tukey HSD (Tukey’s honestly significant difference) was used as a post-hoc test.
Results
Clinical features and demographic findings of the patients in each stage.

LDL: low-density lipoprotein; HDL: high-density lipoprotein.
*p < 0.05 is significant.
Comparison of stages according to the neutrophil-to-lymphocyte ratio.
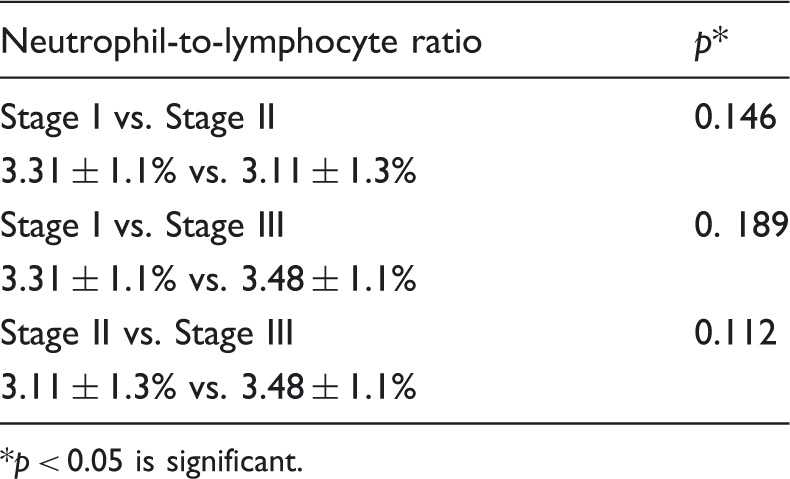
p < 0.05 is significant.
Comparison of stages according to the mean platelet volume.
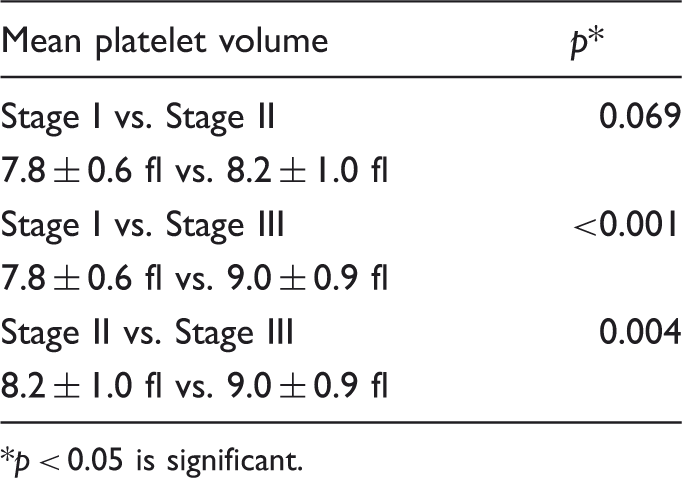
p < 0.05 is significant.
Comparison of stages according to the red cell distribution width.

p < 0.05 is significant.
Discussion
The present study is to investigate whether routine inexpensive complete blood count parameters are related with the severity of patients with PAD. According to our results, mean MPV and RDW values strongly correlate with severity of symptoms in patients with PAD. In particular, mean RDW values were significantly increased in a symptom-dependent manner. In other words, our data support that increments in RDW and MPV values do have a relationship with the severity of disease. We also noted that differences of mean NLR values were insignificant between the stages. This report is a unique study in the literature researching the relationship between complete blood count parameters and the symptoms classification in patients with PAD.
NLR has been investigated in recent studies as a biomarker in diseases in which inflammation has been thought to play an important role in pathogenesis. Atherosclerosis is also an inflammatory process, and recent reviews reported that NLR is related with atherosclerosis and an increased coronary calcium score that are found to be important indicators of cardiovascular disorders.4,7 It has been reported that NLR is associated with the severity of atherosclerosis by Kaya et al. 9 They suggested that NLR values may beneficial for cardiac risk classification in patients with coronary artery disease (CAD). 9 It was even found that high NLR values have been associated with mortality in patients with CAD. 7 Kullar et al. 10 reported that NLR can be predictive for graft patency following lower limb revascularization. Gary et al. 11 found that NLR is closely associated with the severity of critical limb ischemia in patients with PAD. These results conflict with ours, but, diabetes and other systemic problems which can alter the NLR values, were not excluded in the study by Gary et al. 11 In addition, patients in Stage IV (necrosis or gangrene) who have more critical limb ischemia were not included in our study as well.
Increased MPV values are related with an increased number of megakaryocytes in the bone marrow, being an indicator of platelet activation and/or reactivity. This distorted heterogeneous distribution of megakaryocytes might be a predictor of various disorders. 12 Chu et al. 13 reported that MPV elevations might be an indicator of increased cardiovascular risk. Moreover, Berger et al. 14 concluded that MPV is an independent indicator of PAD. However, their sample size is larger than ours with an additional comparison of PAD cases with healthy subjects. MPV has been suggested to be a guide to identify high-risk patients with disturbed microcirculation related disease in previous reports. 15 In another study reported by Yavuz et al., 12 the authors argued that higher MPV levels might be a predictor of disrupted peripheral circulation. The results of this study correlates similarly with to our study, diverging with PAD population being thromboangiitis obliterans patients.
RDW is an indicator of anisocytosis, the size variability of circulating erythrocytes. 16 Erythrocytes have been presented as oxygen sensors and vascular tone modulators in the literature. 17 Thus, ischemia can trigger variations in the size of the circulating erythrocytes and also RDW levels. Ye et al. 18 found that a 1% increase in RDW levels was associated with 10% greater risk of mortality in patients with PAD. They also concluded that RDW, a part of a standard complete blood count, is an independent prognostic predictor in PAD. 18 The relation between PAD and RDW was presented in a large cohort study by Zalawadiya et al. 19 Based on findings, they concluded that “increased RDW levels are independently related with high risk of PAD and can importantly improve the risk stratification beyond that estimated by ACC/AHA-defined PAD screening criteria.” 19 Similarly, we demonstrated that high RDW is associated with severity of disease in patients with PAD. However, we studied the relationship between the severity of symptom classification and RDW.
Severity of atherosclerosis is closely associated with progression of PAD. Atherosclerosis is an inflammatory process and recent studies focused on to this reactive inflammatory view. Thus, reactive inflammatory biomarkers are also important in the progression of atherosclerotic process.4,20 For example, C-reactive protein, previously adopted mainly as a clinical marker of inflammation, is currently considered biomarker in endothelial dysfunction and atherosclerosis. 21 On the other hand, some of the complete blood counting parameters reactivity are also shown in atherosclerotic events such as high platelet reactivity is associated with increases in both atherosclerosis burden and plaque calcification in previous reports.12,22 In the view of these correlations, our results supported that increased bone marrow reactivity may play a role in progression of disease. According to our results, high plasma RDW and MPV levels can be sourced by increased bone marrow reactivity and this process should be investigated with further clinical researches.
To sum up, our findings indicate that an increment in both RDW and MPV values might help with symptom stratification in PAD patients who are followed up periodically. Also, it might be beneficial for further progression estimation in patients with PAD. More research is required to transfer our findings into clinical practice, but in the meanwhile this study may illuminate new points of relations between complete blood parameters and the severity of atherosclerotic vascular diseases.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.