
Abstract
Complex iliac anatomy including extreme tortuosity constitutes a relative contraindication for endovascular abdominal aortic aneurysm repair with additional risk of limb-graft occlusion. The Gore Excluder limb-graft is a flexible stent-graft, which adapts easily to iliac tortuosity. Nevertheless, the presence of the stiff guide wire does not always allow for an ideal apposition of the stent graft to the angulated common iliac artery vessel wall. We describe herein a modified technique for Gore Excluder limb-graft deployment with partial removal of the stiff wire in cases with difficult tortuous or narrow iliac arteries during endovascular abdominal aortic aneurysm repair.
Introduction
Limb-graft occlusion has been an important reason for re-intervention following endovascular treatment of abdominal aortic aneurysms (AAA).1–4 During the last decade several factors contributing to limb-graft occlusion have been identified; tortuous or narrow iliac arteries (including a landing zone in the external iliac artery), aortic bifurcation with angulation more than 60 degrees, and the use of unsupported limb-grafts.1–4 Our experience with the Gore Excluder AAA endoprosthesis (W.L. Gore & Associates, Flagstaff, Arizona, USA) showed a zero percent limb-graft occlusion with a selective use of this graft especially in difficult iliac anatomy. 5 This reflects the superior flexibility of the Gore Excluder limb-graft. However, its deployment, although simple and rapid, is not always accurate, especially in angulated iliac arteries. The presence of the stiff wire diminishes extreme iliac artery angulations before limb-graft deployment and consequently the limb-graft is deployed in a more “straightened” common iliac artery, which however tends to return to its previous angulated anatomy upon removal of the stiff wire. The latter can occasionally result in a less accurate deployment and defective apposition of the limb-graft to the artery wall. We describe herein a modified technique for Gore Excluder limb-graft placement consisting of partial removal of the stiff wire prior to device deployment in cases with difficult tortuous or narrow iliac arteries in order to enhance deployment accuracy and adaptation of the limb-graft to the angulated iliac artery.
Technique
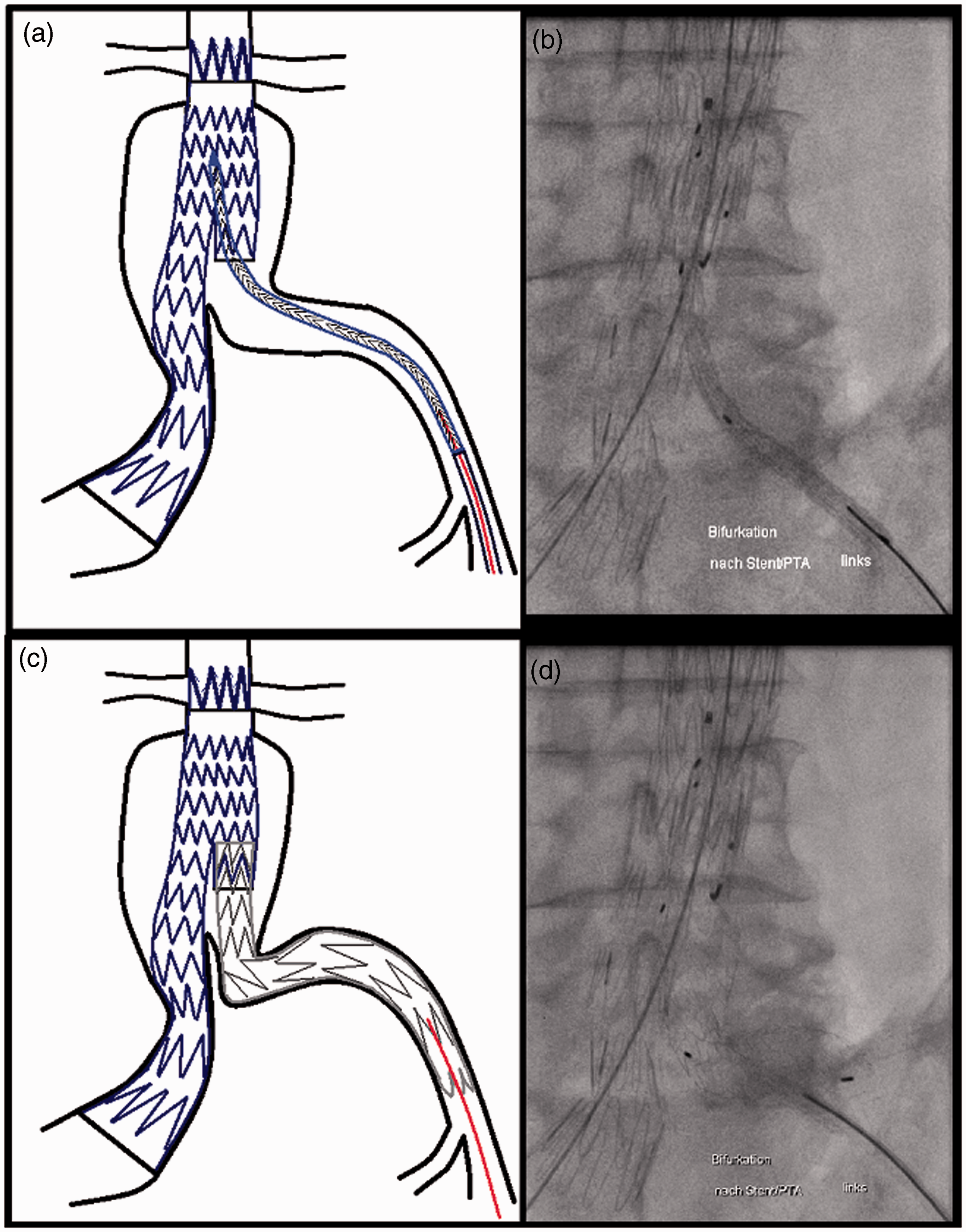
After complete deployment of the main body stent-graft and catheterization of the contralateral gate, an angiogram points the level of the internal iliac artery origin (Figure 1a and b). A stiff wire, most commonly a Lunderquist extra stiff guide wire (Cook Medical Inc, Bloomington, Indiana, USA) is subsequently used for limb-graft insertion. The Gore Excluder limb-graft catheter is inserted through a 12/18 F sheath and advanced over the stiff wire within the main body (Figure 1c and d). After retraction of the 12/18 F sheath, and before graft deployment, the stiff wire is meticulously withdrawn down to a point that its floppy tip lies proximally to the iliac bifurcation, allowing the limb-graft device to adapt gradually to the common iliac artery angulation (Figure 2a and b). A retrograde angiogram is performed followed by slow deployment of the first 3–4 cm of the Gore Excluder limb-graft, so that the contralateral gate is fully filled. Subsequently, we start to manipulate the delivery catheter for exact graft positioning and the rest of the limb-graft is meticulously deployed (Figure 2c and d). Once the limb-graft is completely deployed, the stiff wire is repositioned in order to regain access and allow for safe catheter removal.
Schematic diagram (a) and digital subtraction angiography (b) after deployment of the main body stent-graft and catheterization of the contralateral limb. Note the angulation of left common iliac artery. This case represents a hybrid approach consisting of a Zenith (Cook Medical Inc, Bloomington) main body endograft combined with a Gore Excluder limb-graft (W.L. Gore & Associates, Flagstaff, Arizona) to deal with the extreme left common iliac artery tortuosity. Schematic diagram (c) and fluoroscopy (d) demonstrating the Gore Excluder limb-graft advanced over the stiff wire (red line) and placed appropriately before deployment. Note the “straightened” common iliac artery due to stiff wire insertion. Schematic diagram (a) and fluoroscopic image (b) demonstrating the stiff wire (red line) partial removal below the common iliac artery angulation prior to limb-graft deployment. With such a manipulation the common iliac artery obtains again its original tortuosity enabling gradual adaptation of the limb-graft to iliac angulation prior deployment. Schematic diagram (c) and fluoroscopic image (d) showing accurate deployment of the Gore Excluder limb-graft with very good apposition to vessel wall and adaptation to the common iliac artery extreme angulation.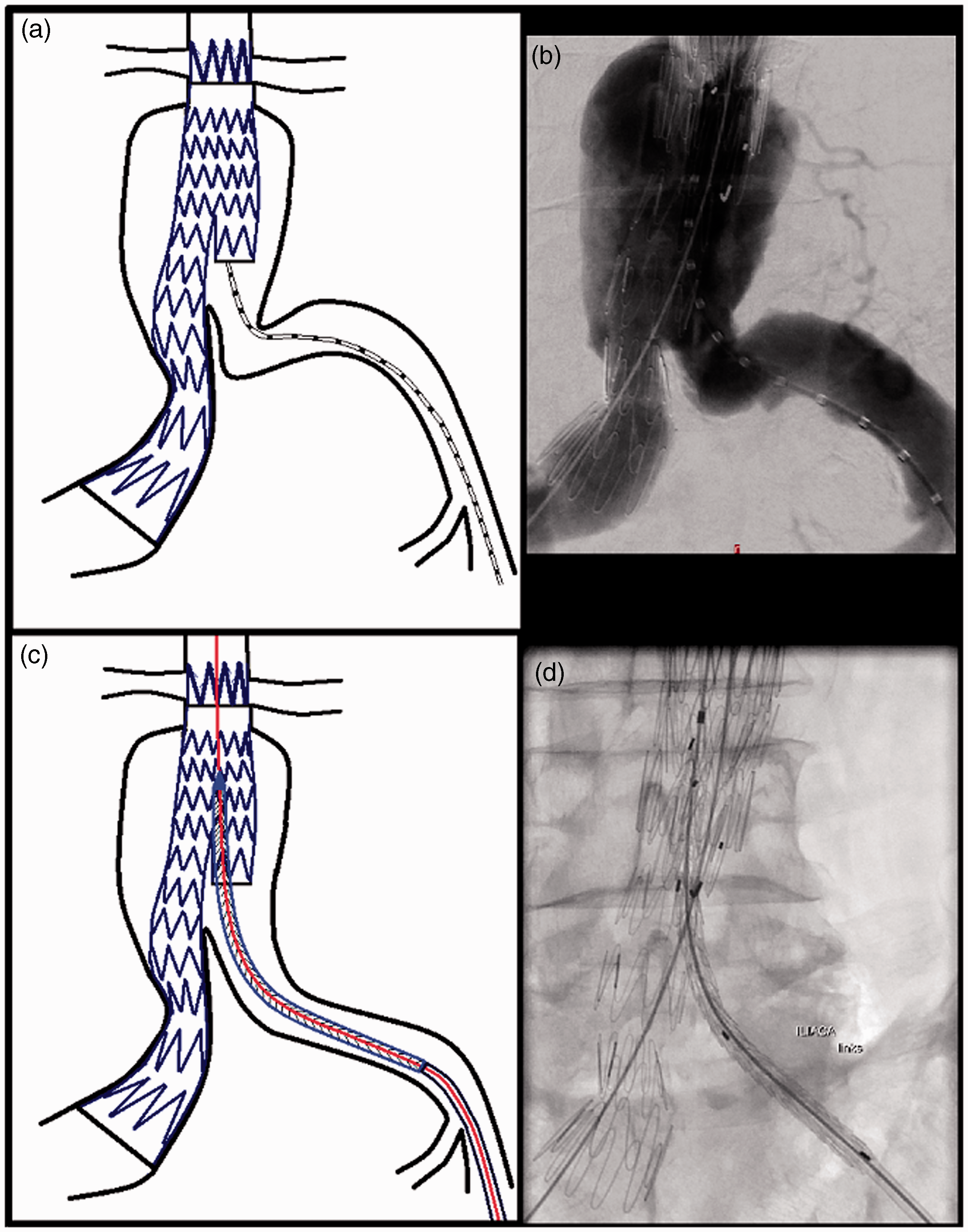
Discussion
In our institution we developed a preferential strategy for the Gore Excluder AAA Endoprosthesis in AAAs with long neck (>20 mm) and more complex iliac artery anatomy (sharp aortic-iliac angulation, small or tortuous iliac arteries). 5 In aneurysms with a shorter neck anatomy (<20 mm), we use preferentially the Zenith endograft (Cook Medical Inc, Bloomington, Indiana, USA) with suprarenal fixation. In cases with short proximal neck that required a Zenith main body and coexistent difficult iliac anatomy (sharp aortic-iliac angulation, small or tortuous iliac arteries), two different strategies were used. Either we deployed Zenith limb-grafts, which were subsequently relined with self-expandable stents in order to reduce the risk of kinking, 6 or we applied a hybrid approach consisting of a Zenith main body and one or two Gore Excluder limb-grafts as previously described. 7 This combination with the use of stent-grafts from two manufacturers has been shown to be safe in terms of durability, connection security, and patency with zero limb-graft disconnection or migration, and zero limb-graft occlusion at mid-term follow-up.
In AAA cases with difficult iliac anatomy where we used Gore Excluder limb-grafts, we have applied the herein described deployment technique with partial removal of the stiff guide wire.
Our results were satisfactory with always accurate limb-graft deployment and very good graft apposition to the tortuous common iliac artery. In two cases, removal of the stiff wire resulted in stent graft delivery catheter drop, which led us to reinsert the stiff wire and reposition the stent graft catheter before deployment. Therefore, it is important to initially position the limb-graft catheter a little bit above the 3 cm overlap zone within the main body, so as to compensate for a small drop that may occur during stiff wire withdrawal. Additionally, it is essential to initially deploy the proximal part of the limb-graft in order to fill the contralateral gate before starting to manipulate the delivery catheter for position adjustment.
The presence of a stiff wire changes temporarily the anatomic morphology of the tortuous iliac artery. Therefore, to measure the length of the intended limb-graft an angiogram is performed through a metric angio-catheter without any guide wire in it. As a consequence, the iliac artery takes its natural angulated anatomy and measurement of the angio-catheter markers provides an accurate measurement for the ‘real’ length of the iliac artery. The presence of a stiff wire prevents also accurate limb-graft landing and adaptation to the iliac tortuous anatomy. By removal of the stiff wire, the “real” common iliac artery anatomy is better visualized and the limb-graft angle changes (Figure 3). An alternative option is to completely remove the stiff wire after advancement of the limb-graft and exchange it for a softer wire, so as to minimize the chance of losing wire access. The limb-graft can be then easily repositioned during slow deployment by gentle pushing up of its delivery catheter. This results in accurate deployment with good adaptation to the common iliac artery tortuosity. With such a manipulation we can adjust both the position and the curve of the limb-graft by deploying slowly and relaxed with care and dexterity so as to land it exactly at the desired location, but also to “fill” the iliac curve. Thus, we avoid “cutting the corners,” which could be associated with a higher risk of limb-graft kinking and occlusion. Indeed, applying such a technique may have contributed to the zero percent limb-graft occlusion rate we observed in cases with severe iliac angulated anatomy as already reported.
5
Schematic diagrams and fluoroscopic images demonstrating how the undeployed limb-graft (a, b) changes angle in the angulated iliac artery after stiff wire removal (c, d).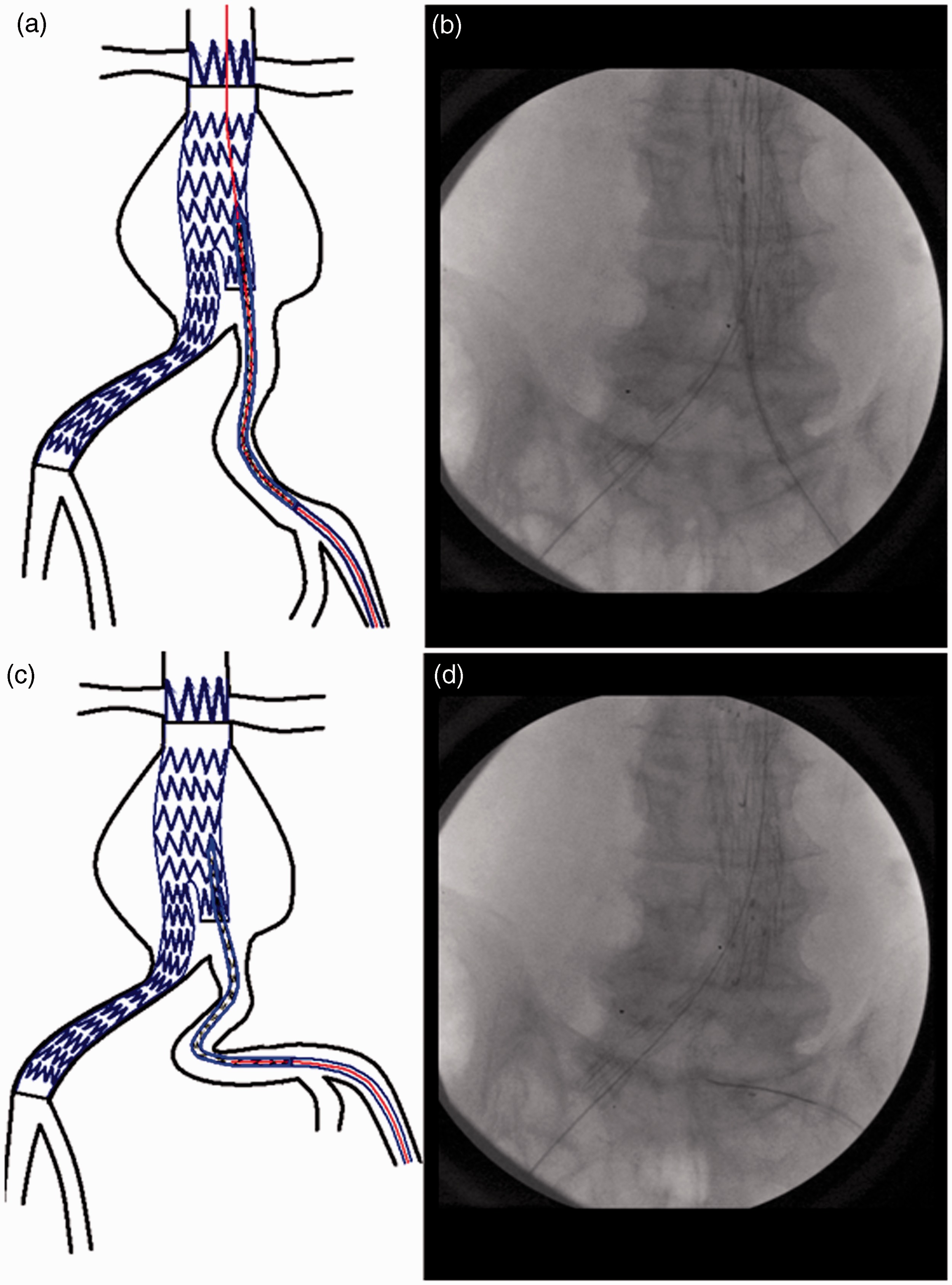
Conclusion
Partial removal of the stiff wire prior to Gore Excluder limb graft deployment is a safe technique useful in cases with difficult tortuous or narrow iliac artery anatomy. This maneuver results in more accurate limb-graft deployment with better apposition to the vessel wall and adaptation to tortuous iliac anatomy reducing thus the risk of limb-graft kinking and consequent occlusion. It is to note that such a manipulation could be potentially applied also with other devices apart from the Gore Excluder and in additional arterial beds other than the common iliac artery, which are prone to severe angulations (e.g. subclavian artery).
Footnotes
Conflict of interest
Eric LG Verhoeven has received educational grants and is a consultant for Cook Inc, W.L. Gore & Associates, Atrium and Siemens.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.