
Abstract
A 63-year-old female was diagnosed with severe aortic stenosis, who underwent a diagnostic coronary angiography via transradial approach prior an aortic-valve replacement. After imaging the left coronary system, entrapment of the diagnostic catheter was encountered as a result of spasm of the radial artery. An arteriogram of the arm revealed an anatomical variation in the radial artery (high take-off). Several attempts to remove the entrapped catheter resulted in avulsion of the artery, which was managed successfully with coil embolization. To our knowledge, no such complication has been reported.
Introduction
Trans-radial approach (TRA) for coronary catheterization has been gaining favor. In recent studies, TRA has been proven to be as safe and effective as trans-femoral approach (TFA). Furthermore, the use of TRA has been associated with a reduction in vascular complications. However, uncommon, but severe complications of TRA have been described, some of which may put patients’ limbs at risk.
We are reporting the case of a 63-year-old female who underwent a diagnostic coronary angiography via TRA prior to an aortic-valve replacement. Entrapment of the diagnostic catheter was encountered as a result of spasm of a radial artery with an anatomical variation (high take-off); this resulted in avulsion of the artery, which was managed successfully with coil embolization. To our knowledge, no such complication has been reported.
Case presentation
A 63-year-old female with history of diabetes mellitus, who presented with exertional dyspnea for 1 year, was diagnosed with severe aortic stenosis. The patient was admitted electively for a diagnostic coronary angiogram prior an aortic-valve replacement.
Radial access was obtained using a 5-Fr sheath, and diagnostic angiography using a 4-Fr catheter was initiated. Multiple images of the left coronary system were obtained. Upon switching to the right coronary system, the catheter became difficult to manipulate, preventing the cannulation of the right coronary artery. The initial suspicion was of radial artery spasm. Multiple attempts to remove the catheter were unsuccessful, including the use of verapamil, nitroglycerin, and intra-arterial nicardipine. The procedure was aborted and completed via TFA; coronary arteries were normal. While in the recovery room, after giving the patient some rest, the radial artery access was reevaluated, but the catheter was still entrapped; a brachial plexus nerve block was performed without success.
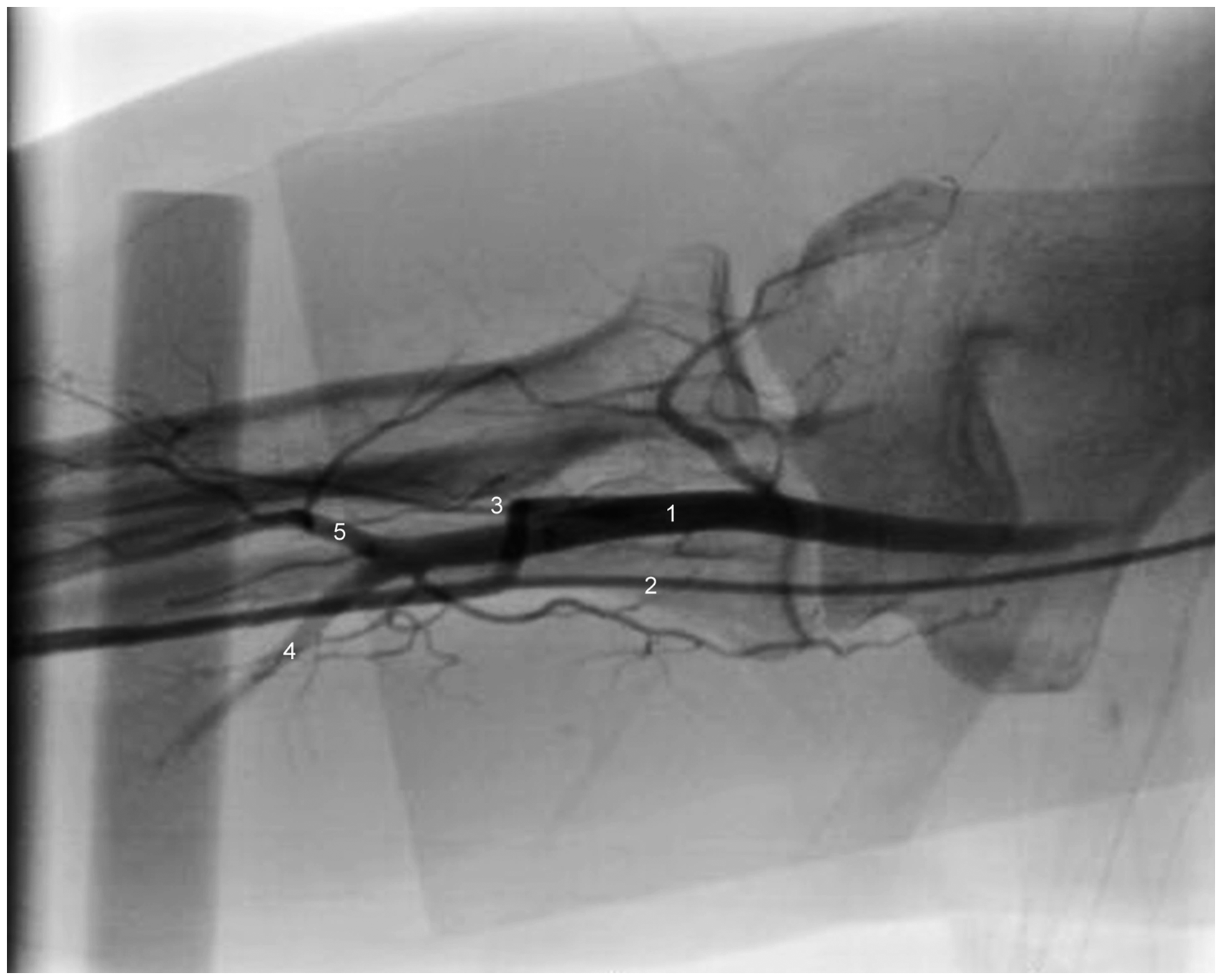
The patient was transferred back to the catheterization laboratory, and the radial artery access was re-assessed. The sheath appeared to be moving freely; however, the catheter was not moving. An aortogram showed the catheter in the true lumen of the ascending aorta. Next, an arteriogram performed via the right RA sheath evidenced a high-take-off RA with a steep angle at the ostium (Figure 1). Furthermore, images at the level of the elbow showed a connection between the radial and brachial arteries, suggestive of a type-3 high take-off (Figure 2).
Angiogram showing the catheter in the radial artery traveling in parallel to the brachial artery. Arrow pointing to the high take-off of the radial artery at the level of the upper arm. Angiogram at the level of the elbow showing a type two-third high-take-off radial artery. (1) Brachial artery. (2) Diagnostic catheter traveling up to upper arm through the high-take-off radial artery. (3) Connection between the brachial and radial arteries. (4) Ulnar artery. (5) Interosseous artery.
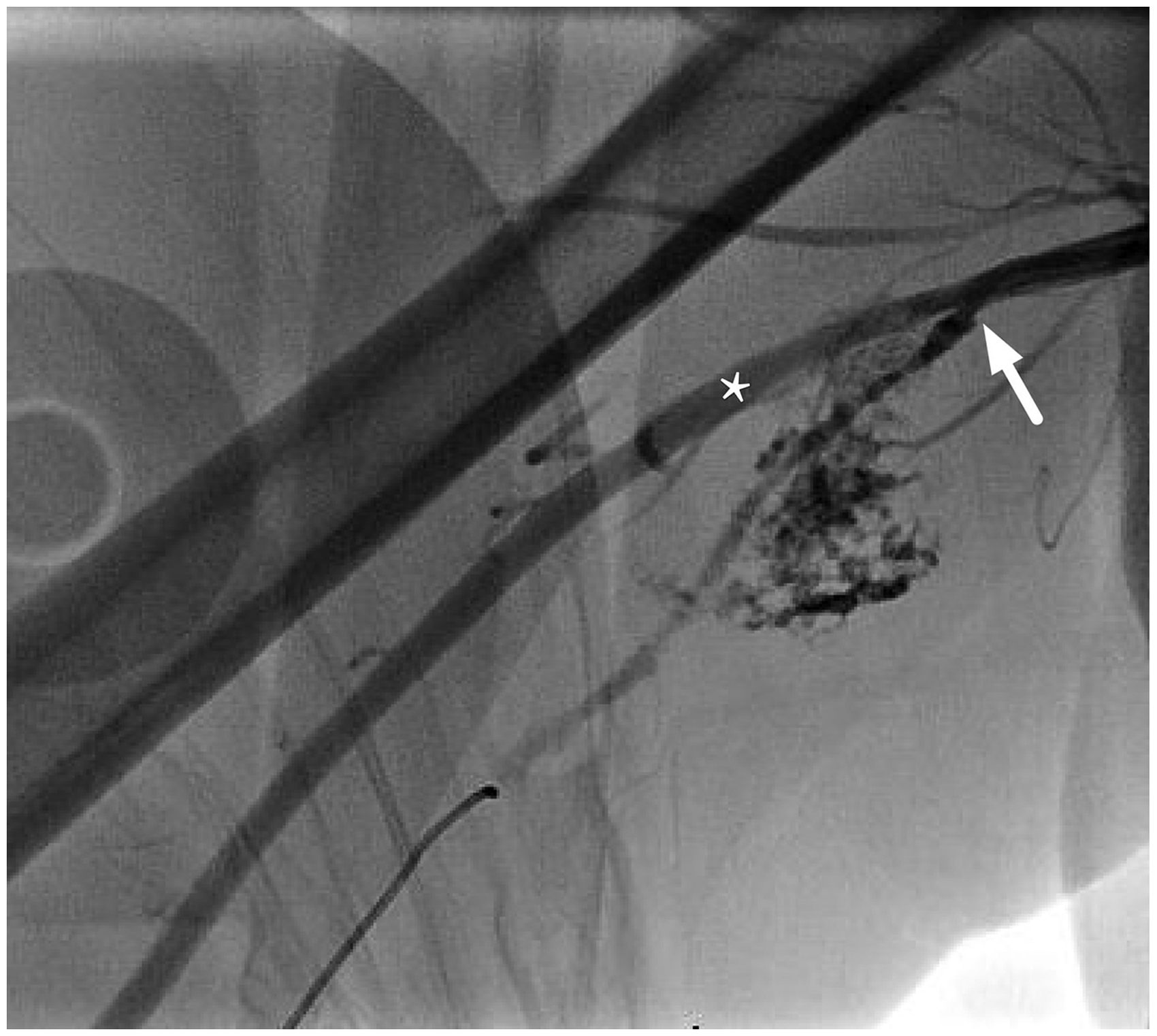
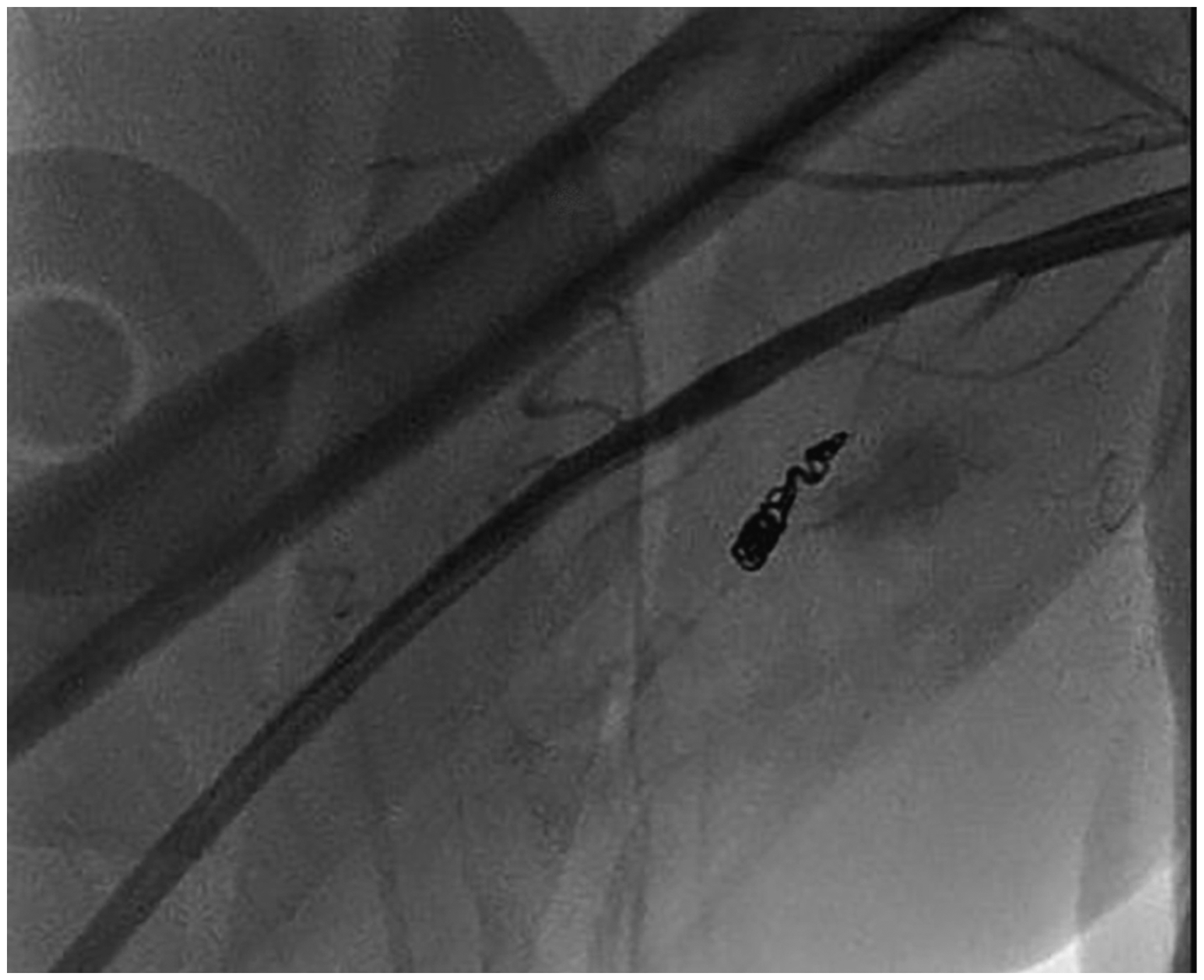
An attempt to remove the catheter using a 0.035-in J-wire failed. After switching a Super Stiff Amplatz wire and using extra force, the catheter was removed. An angiogram showed extravasation of contrast material at two different points in the arm (Figures 3 and 4). The left femoral artery was accessed and entered a 6-Fr sheath. An angiogram of the radial artery was performed, confirming the avulsion of the artery at two points. After demonstrating patency of the proximal segment of the high-take-off radial artery and that the ulnar artery reconstituted the palmar arch, a Renegade microcatheter was placed, and the radial artery was coil embolized proximally (14 cm × 3-mm micro nester embolization coil). The procedure went uneventful with resolution of the extravasation (Figure 5). Pressure was applied to the puncture site for 15 min; the arm remained soft, with normal motor and sensory functions. Pulse was intact in the right ulnar artery. Next day, the patient underwent a successful minimally invasive aortic-valve replacement.
Angiogram showing extravasation of contrast media at the level of the upper forearm. Angiogram performed via the femoral artery revealing an avulsed radial artery in its proximal portion. Contrast extravasation can be seen near the take-off at the level of the upper arm. Arrow pointing to the high take-off of the artery; asterisk showing the preserved brachial artery. Angiogram showing successful coil embolization of the proximal segment of the radial artery. There is no evidence of extravasation with contrast injection.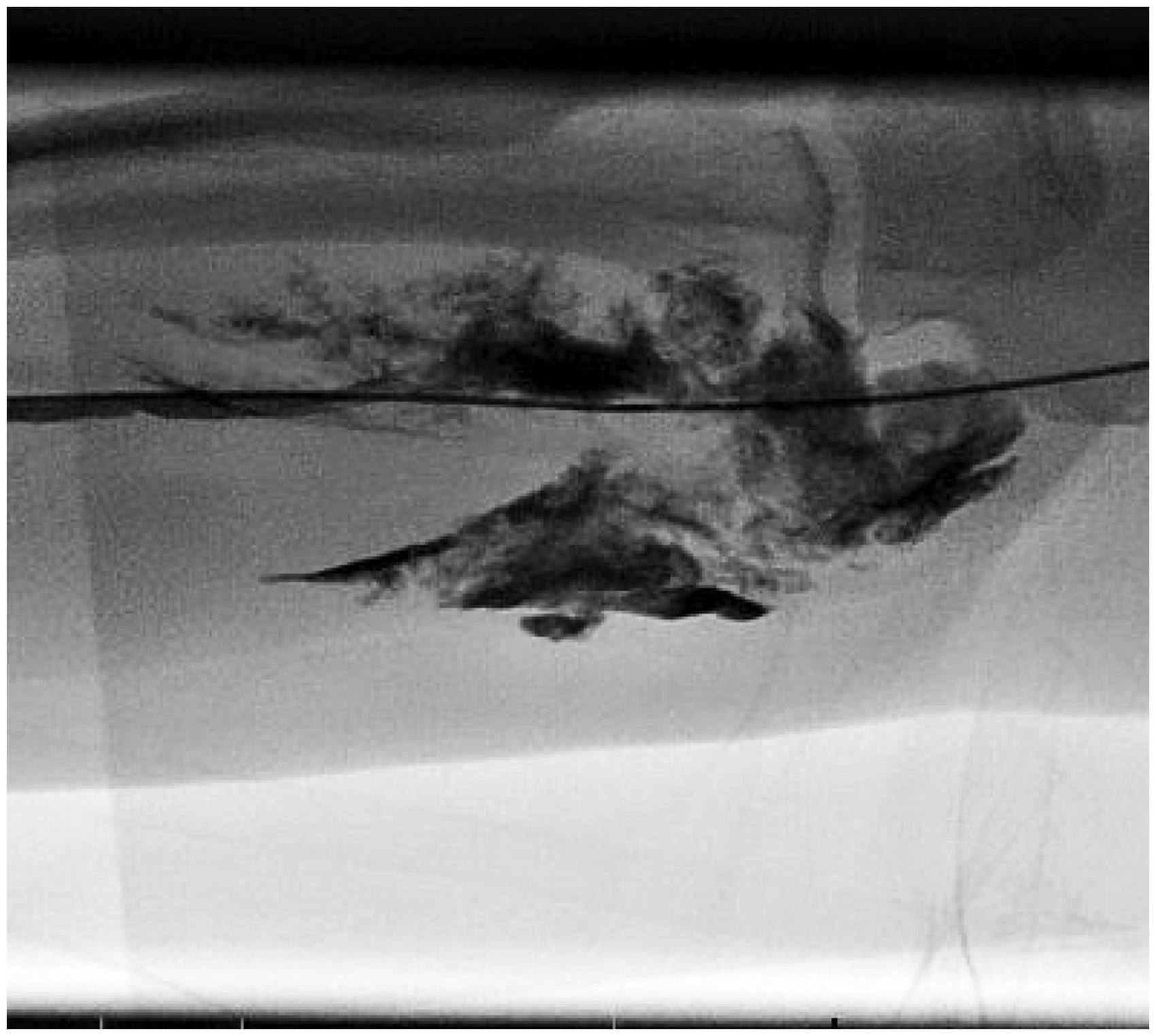
Discussion
TRA for cardiac catheterization has emerged as an alternative to TFA, with a better safety profile and similar success rate. 1 Although vascular complications with TRA are less common than with TFA, potential complications include asymptomatic radial artery occlusion, radial artery spasm, and perforation of the radial artery with the formation of hematoma and pseudoaneurisms. 2 Other complications such as compartment syndrome, perforation of arteries beyond the brachial artery, and catheter retention have also been reported.3–5
Anomalous radial artery anatomy as well as radial artery spasm may play a major role in failure of TRA angiography and in development of severe vascular complications. Four different types of high-take-off radial artery have been described; type 1 is a radial artery that begins in the upper arm and travels down to the forearm without having any connections with the brachial artery; types 2 and 3 are similar to type 1, with the exception that there is a connection with the brachial artery at the level of the antecubital fossa; being the main difference that in type 3, the segment of the artery above the connection is slender (associated with more procedural failure). Type 4 is a remnant high-take-off radial artery that has a short course and terminates in the upper arm. 6 We believe that a combination of anatomical variation (type III high-radial take-off) and radial artery spasm was the cause of procedural failure in our case.
In a study done by Lo et al. 7 in 1540 patients undergoing coronary interventions via TRA, procedural failure was much higher in patients with anatomical variations (14.2%) than in those with normal anatomy of the radial artery (0.9%). Interestingly, 7% of all patients had a high-bifurcating radial artery (high take-off). However, only 4.6% of failed cases were due to a high-take-off radial artery, whereas 37% were related with radial artery loops, which were present in just 2% of all patients.
Since anomalous anatomy is not uncommon and may lead to severe vascular complications and failure of TRA angiography, knowing the anatomy prior to TRA angiography might be helpful. A duplex evaluation of the upper extremities could be performed, in order to assure the adequacy of the radial-ulnar palmar collateral circulation. However, if this approach is not feasible, contrast injection via the radial artery access sheath can be done. Some authors have suggested routine retrograde radial arteriography after sheath insertion to assess the anatomy prior to TRA procedures. 7 In addition, the use of smaller catheters may decrease the rate of development of arterial spasm and vascular complications; in our case, catheter entrapment occurred despite the use of a 4-Fr catheter.
Several approaches to the management of catheter entrapment have been reported. The use of intra-arterial nitroglycerine and verapamil has been shown to decrease the rate of radial artery spasm. 8 Others have proposed the use of sublingual nitroglycerine, systemic analgesics, and anxiolytics, and even the use of papaverine intra-arterial.9,10 Furthermore, the use of general anesthesia has been proposed in cases of severe spasm of the radial artery. 9
Khoubyari et al. 4 reported the case of a patient with a kinked and entrapped catheter in the radial artery, which was successfully removed by using a gooseneck snare via the femoral artery. In our case, the combination of anatomical variation and arterial spasm would have made this approach very difficult. In case of avulsion of the radial artery, hemostasis has to be achieved promptly. In cases of severe spasm and catheter entrapment, where mechanical complications might be expected, it would be prudent to have a femoral access obtained as an alternative access, should an emergent intervention be required.
Different to our approach, Butarak et al. 11 described the use of external compression with a sphygmomanometer cuff, while leaving a catheter within the artery, for management of a radial artery perforation. However, due to the anatomical variation encountered in our case and the avulsion of the radial artery more proximally in the axilla, external compression was deemed unfeasible.
We also recommend the collaboration with vascular surgery. In our case, as the catheter removal required force, a vascular surgeon was present, and once the arterial avulsion was seen, catheter embolization was performed successfully.
Conclusion
TRA is safe and effective when compared to TFA. Rare and severe complications that could jeopardize the upper limbs can occur. Early recognition of anatomical variations that can complicate TRA angiography is important as it is associated with a higher rate of procedural failure and complications. Retrograde radial arteriography should be considered, especially if there are difficulties advancing the wire or catheter through the radial artery. When catheter entrapment occurs, initial attempts to relieve spasm with the use of intra-arterial vasodilators, anxiolytics, and last general anesthesia can be attempted if the primary cause of entrapment is thought to be severe radial artery spasm.
If unsuccessful, femoral access should be obtained and vascular surgery called. In our case, femoral access should have been obtained earlier. If avulsion occurs, external compression can be performed if anatomy permits. When required, hemostasis by external compression, while leaving a catheter in the artery can be attempted, or as in our case, coil embolization can be performed.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.