
Abstract
Introduction
Intra-procedural acute thrombosis (IPAT) is a complication of endovascular procedures. We aim to identify risk factors for IPAT and compare the outcomes of patients with or without IPAT.
Methods
Paired T test and χ2 test were used to identify risk factors and short-term outcomes. Kaplan–Meier survival analysis was used for mid-term outcomes.
Results
A total of 228 procedures were performed with 21 IPAT events (9.21%). The odds ratio of Indian patients developing IPAT was 2.8x (95% CI 1.1–7.6). Patients with in-stent occlusion or prior IPAT were 5.6x (95% CI 1.3–24.2) and 5.6x (95% CI 1.3–24.4) more likely to develop an IPAT event. Patients without IPAT had significantly more improvement in mean runoff score (−1.15 ± 1.31, p < 0.01). The odds of patients with IPAT requiring subsequent endovascular intervention and arterial bypass surgery were 4.2x (95% CI 1.6–10.7) and 7.1x (95% CI 1.9–27.0). There was no significant Kaplan–Meier estimated overall survival or amputation-free survival difference between patients with or without IPAT event.
Conclusion
Indian ethnicity, in-stent occlusion and previous IPAT were associated with higher risk of IPAT. Even after successful endovascular salvage, patients with IPATs were more likely to require secondary revascularization procedure. Patients with IPATs had no decrease in overall survival or amputation-free survival.
Introduction
The incidence of peripheral arterial disease (PAD) is increasing in many developed countries, particularly with the increasing prevalence of diabetes. 1 Endovascular interventions have gained acceptance as a primary therapeutic option for critical limb ischemia, given the potential for shorter hospital stays, lower anesthetic risks and decreased peri-operative morbidity.2,3
Intra-procedural acute thrombosis (IPAT) due to emboli or thrombosis is a known complication of endovascular procedures. The incidence of distal emboli related to endovascular intervention ranges from 50% to 100% in Doppler studies and post-procedural analyses of embolic filter devices,4–6 while 0–7.3% are angiographically significant.6–9 Significant IPAT is limb-threatening, requiring immediate salvage intervention which often translates into additional procedures, more contrast usage and radiation exposure for the patient. 10
Currently, knowledge about the predictive factors of IPAT occurrence and outcomes of patients with IPAT after successful salvage is limited. Some literatures suggest that the demographic characteristics 9 and severity of arterial lesion 7 may be associated with an increased risk of IPAT. The purpose of this study is to identify predictive factors of IPAT among our PAD patients and also to review the short- and mid-term outcomes of patients with IPAT.
Methodology
PAD patients with severe limb ischemia who underwent endovascular intervention between July 2008 and December 2010 were reviewed. Data review of this group of patients was approved by the hospital Institutional Review Board. Those who had IPAT events during endovascular procedures were identified. An IPAT event was identified during the intervention procedure when there was angiographic evidence of occlusion or interval worsening of distal runoff arteries after catheterization or treatment of the target vessel. Patients with no IPAT event during their endovascular intervention were considered as the control group. The demographic features, clinical data, lesion characteristics and pre-procedure tibial arteries runoff scores (modified Society for Vascular Surgery scoring) 11 were recorded and compared between the IPAT group and the control group to identify risk factors associated with IPAT.
All patients were followed up at 1 month and subsequently 3 monthly after hospital discharge for their lower limb perfusion status and symptoms. Additional follow-up or admission was arranged if clinically indicated. Arterial duplex scan was arranged during follow-up if there was a clinical suspicion of re-stenosis.
The clinical outcomes of patients who suffered from IPAT were compared to the control group. IPAT patients with unsuccessful salvage were excluded from outcome analysis and reported separately. The post-procedure runoff scores and ankle-brachial pressure index (ABPI) were compared with the individual’s pre-procedure values to assess any change in limb hemodynamics. Patients’ lower extremity symptoms, secondary endovascular intervention, arterial bypass surgery, major amputation in the treated limb and overall survival were recorded.
χ2 test, Fisher’s exact test and the T test were used to identify risk factors and outcomes associated with IPATs. Paired T test was used to assess the change in runoff score before and after intervention. Odds ratios with 95% confidence intervals were used where relevant. Kaplan–Meier analysis with log-rank test was used to analyze overall survival and amputation-free survival. We took p ≤ 0.05 and 95% confidence intervals as statistically significant. Analysis was performed using Statistical Package for Social Sciences (SPSS) version 20.0 (SPSS Inc., Chicago, IL).
Results
A total of 228 endovascular interventions were carried out for 183 patients during the study period. Twenty-one (9.21%) of these procedures were complicated by IPAT occurrences. Among the 21 procedures in which IPAT occurred, successful endovascular salvage was achieved in 20 of them, with only one failure. Among the successfully salvaged patients, catheter aspiration of the thrombus was performed as first line of salvage with one patient required additional intra-arterial urokinase infusion. The patient with failed endovascular salvage subsequently underwent arterial bypass surgery. No procedure-related mortality occurs in this series of patients.
Demographics
Demographic characteristics of patients.

N/A: not applicable.
Multivariate analysis of risk factors.

Lesion characteristics
Lesion and procedural characteristics.

Procedural details
All 228 procedures in this study were exclusively angioplasty ± stenting. Stent deployment was not found to be associated with higher rates of IPAT when compared to the control group (Table 3). Patients with a history of IPAT during previous endovascular intervention of the ipsilateral limb had a 5.6x (95% CI 1.3–24.4) odds ratio of developing another IPAT in the secondary procedure.
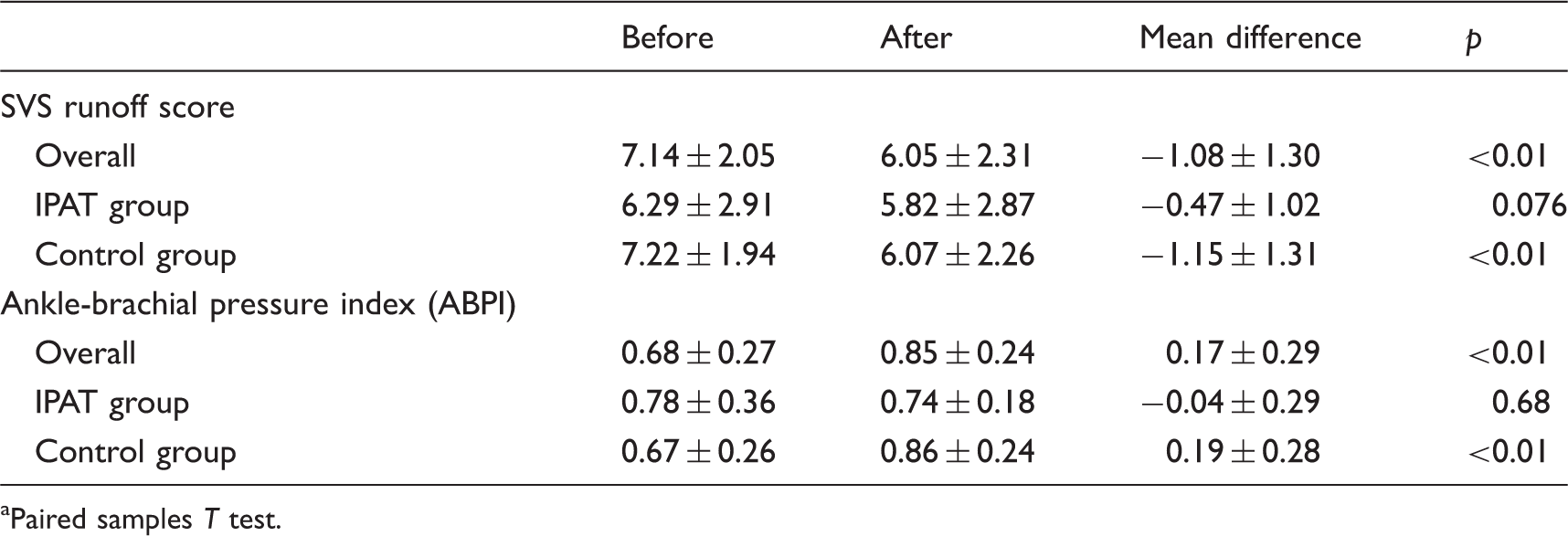
Limb hemodynamics
Limb hemodynamics. a

Paired samples T test.
Clinical outcomes
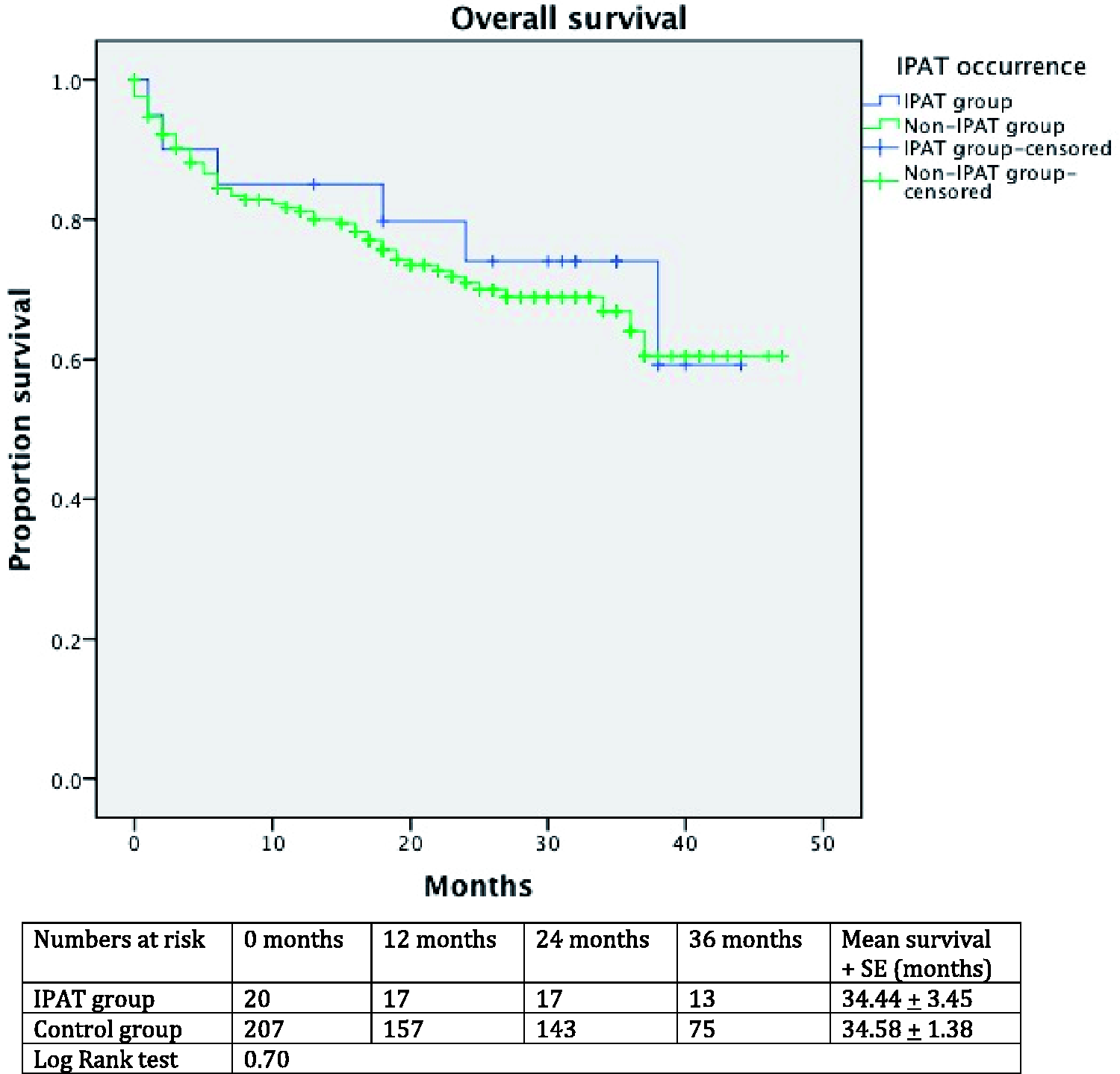
The mean duration of follow-up was 20.0 ± 13.2 months. Data on survival, major amputation and subsequent interventions or bypass surgery were reported in Table 5. Patients with IPAT required more subsequent endovascular interventions (IPAT vs. control, 50.0% vs. 19.3%, p = 0.004) and arterial bypass surgery (IPAT vs. control, 20.0% vs. 3.4%, p = 0.01) than patients in the control group. The odds of a patient with IPAT requiring endovascular re-intervention or arterial bypass surgery were 4.2x (95% CI 1.6–10.7) and 7.1x (95% CI 1.9–27.0), respectively. There was no significant difference in the major amputation rate (IPAT vs. control, 15.0% vs. 18.8%, p = 1.00) or 30-day mortality (IPAT vs. control, 30.0% vs. 27.5%, p = 1.00) between both groups. There was also no significant difference in Kaplan–Meier estimated amputation-free survival (Figure 1) and overall survival (Figure 2) between the two groups.
Amputation-free survival of patients with IPAT vs. control. Overall survival of patients with IPAT vs. control. Clinical outcomes.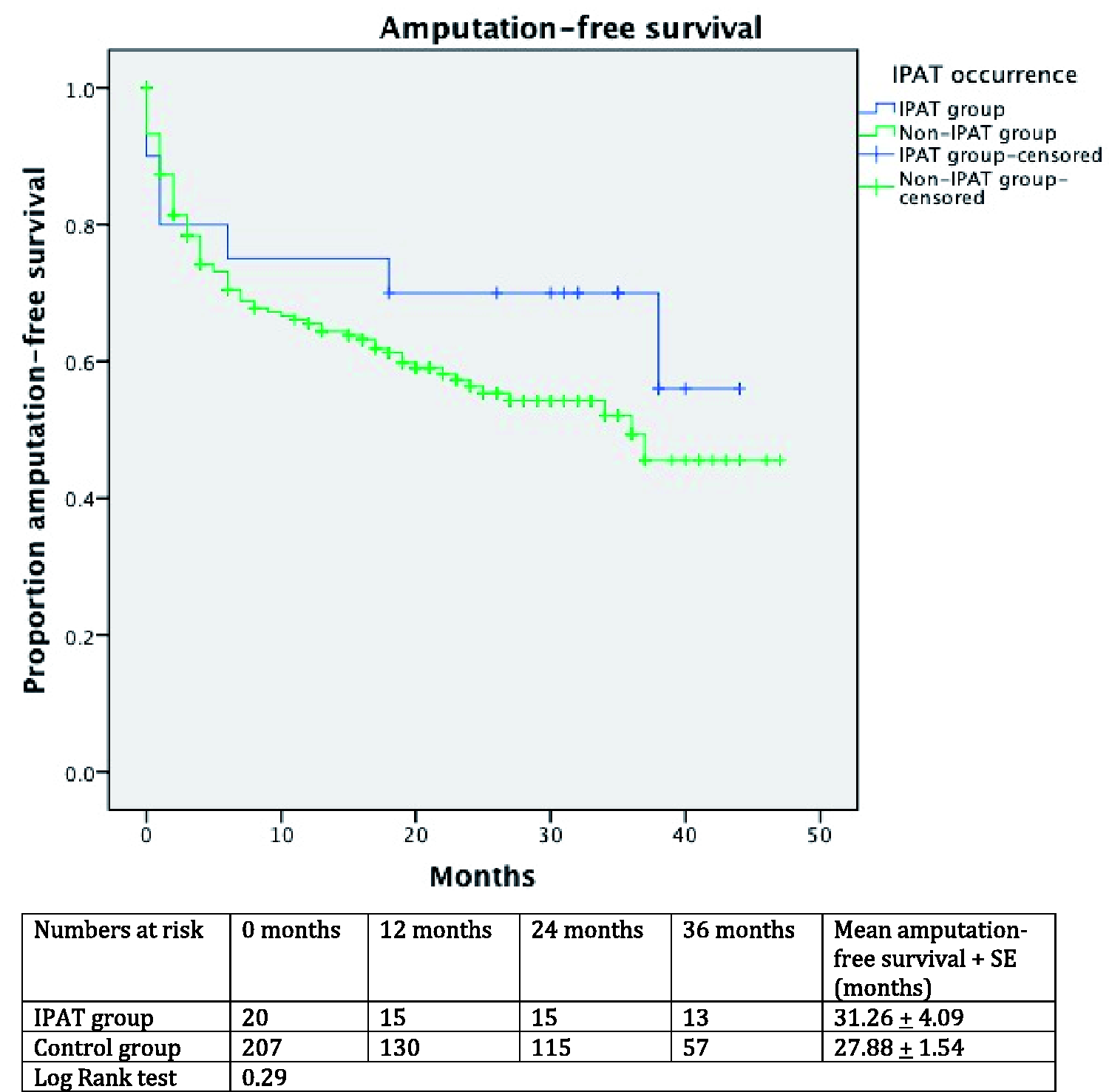
Discussion
Thromboembolic phenomenon is a well-described complication of endovascular interventions and may arise through various mechanisms including inadequate anti-coagulation, distal embolization of an existing thrombus or plaque fragment during angioplasty/stenting, and acute thrombosis of distal stenotic area during balloon occlusion of the proximal flow. Lam et al. 5 performed Doppler study of the popliteal artery during superficial femoral artery intervention and found that distal emboli signal was detected in every single case, with angiographically significant embolic complications occurring in only one patient who successfully underwent endovascular salvage. Angiographically detectable distal embolization and thrombosis (IPAT) are reported to occur in 0–7.3% of endovascular procedures.6–9
Where IPAT is not correctable, lower limb perfusion is likely to be further impaired and may lead to limb loss. However, little data have been published on the outcomes of patients after successful endovascular salvage procedures for the IPAT event. It is uncertain whether there is any subclinical thrombosis of small vessels that may occur even after successful clot removal and lead to poor clinical outcomes. Although we do not know the actual mechanism, the result of the current study showed there is less hemodynamic improvement of patients after salvage from IPAT event compared to those without IPAT event. This may be because the occurrence of IPAT hinders the proceduralist to further open up remaining occluded or stenosed tibial vessels aggressively. Patients with an IPAT event also required secondary endovascular and bypass procedures more frequently. This indicated that even after a successful salvage of the IPAT event, there is longer term sequalae related to the event. This could be due to the less aggressive approach after IPAT event happened, or restenosis due to the presence of residual thrombus adhered to the arterial lumen after successful endovascular salvage.
Davies et al. 9 reported lower 5-year limb salvage rate (distal embolization vs. control, 68.0 ± 8.0% vs. 87.0 ± 2.0%, p < 0.05) in the distal embolization group. In contrast, Shrikhande et al. 7 reported no difference in 2-year limb salvage rate (distal embolization vs. control, 83.3 ± 15.2% vs. 72.6 ± 3.1%, p = 0.699) of 2137 lesions in 1029 patients. In the current study, there was no significant difference in the major amputation rate, estimated overall survival and the amputation free survival among patients with or without IPAT. This may be due to the relatively small sample size of our study. Nonetheless, perfusion is only one of the many factors that determine limb salvage. The medical management of comorbidities 12 and wound-care 13 have well been shown to correlate with limb preservation. In the situation where many factors are interacting with one another, the effect on limb salvage imposed by the IPAT event may not be easily isolated out. This also applies to the survival of patients as most of them had multiple medical co-morbidities. 13
Currently there are limited measures to prevent IPAT. Adequate anti-coagulation is an important basic measure to avoid formation of clots during the intervention. For arterial lesions with angiographic feature of thrombus component, one could consider applying mechanical (± pharmacological) thrombolytic therapy or deployment of a covered stent to avoid distal embolization. Some advocate the prophylactic use of embolic protection device (most commonly in the form of distal protection filter). Routine use of prophylactic embolic protection device in peripheral intervention is still controversial. Siablis et al. 6 and Karnabatidis et al. 8 performed series of peripheral endovascular intervention with the usage of an embolic protection filter and reported high incidence (100% and 94%, respectively) of macroscopic particles of various sizes captured by the filters. Similarly, the single center registry using embolic protection filter for peripheral intervention carried out by Shammas et al. 14 reported 55% retrieval rate of macroscopic emboli. On the other hand, we have very limited knowledge about the actual clinical effects of these macroscopic emboli. 5 All the studies of embolic protection devices for peripheral intervention are single-armed. There is no comparative or randomized control study to demonstrate the benefit of using embolic protection device for lower limb intervention.
Usage of embolic protection device also carries a potential risk of causing vessel spasm, dissection, thrombus formation, and filter overfill obstructing flow. Although, most published literature reported near-100% successful deployment of the device and a low incidence of device-related complications.6,8,14–17 Of note, an animal study 18 showed endothelial injury induced by filter deployment though the clinical significance in humans is not known. Cost of the embolic protection device is another issue for concern. Nonetheless, application of embolic protection device does not eliminate distal embolization completely. As shown in Shammas et al.’s registry, embolization to side branch proximal to the filter and filter overfill can occur. 14 Distal embolization may also happen during wire crossing of the lesion and before the deployment of the filter. Currently, most clinicians would take the strategy of selective use of embolic protection device for patients with high risk of distal embolization. Alternatively, one could use mechanical thrombolysis for high risk lesions (e.g. in-stent occlusion) before further angioplasty to prevent distal embolization. 19 Currently, there is no comparative study or randomized controlled trial to compare the effectiveness of distal embolization prevention between embolic protection devices and mechanical thrombolysis. Further studies in this aspect are warranted to guide the clinician’s decision making. Nonetheless, understanding the risk factors of IPAT is important for planning of endovascular strategy as well as pre-procedure counseling of patients. In certain patients with high risk of IPAT and yet low surgical risk, surgical bypass for revascularization may be a more preferred treatment modality.
Previous studies have found that demographic factors (female gender, smoking history and metabolic syndrome) 9 and lesion characteristics (multiple lesions, calcifications, length of the lesion, occlusive lesion, TASC-II C/D lesions, poorer pre-procedure runoff, in-stent restenosis and total occlusion)7,9 are predictors of thromboembolic phenomenon. The current study also revealed high IPAT risk associated with in-stent occlusive lesions. In our study, patients of Indian ethnicity had a higher risk of getting IPAT. This is the first time an association has been shown between ethnicity and IPAT occurrence. Variation in clinical outcomes between PAD patients of different ethnicities has been reported before. Chew et al. 20 showed that African Americans had poorer primary graft patency rates and limb salvage rates compared to Caucasians while Chong et al. 21 reported that Caucasians had the highest failure rates for angioplasty compared to Hispanics and African Americans. Studies have also reported an inter-ethnic difference in warfarin requirement and identified the gene responsible for that.22,23 Indian patients required a higher maintenance dose of warfarin compared to other ethnicities. These suggest that the presence of different biologic or socio-economic factors may cause variations in disease patterns and treatment outcomes between ethnic groups. Patients with prior IPAT during previous endovascular intervention also have a higher risk of IPAT again in subsequent endovascular intervention. This might indicate the occurrence of IPAT is related to the nature of the atherosclerotic plaque.
This study has a few limitations. With a limited sample size, some of our findings may not have reached statistical significance. Compared to other studies, our sample population is more heterogenous and consisted of patients with obstructive lesions over various level of the lower limb, rather than a homogenous group of patients with disease over femoro-popliteal vessels.
Conclusion
Indian ethnicity, in-stent occlusion and prior IPAT are associated with IPAT occurrence during endovascular interventions. Despite successful salvage, patients with IPAT appear to have poorer post-procedural runoff and are more likely to require subsequent endovascular procedures or arterial bypass when compared to patients from the control group. However, major amputation rates, overall survival and amputation-free survival are not significantly worse in IPAT patients.
Footnotes
Acknowledgements
This work was presented as Poster presentation at AsiaPCR/SingLIVE 2013, Singapore, 23–24 January 2013.
Authors’ note
This study was approved by the Institutional Review Board of the hospital. Research ethics approval: IRB: National Healthcare Group; Ref no: Study C/11/1991.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.