
Abstract
Tarsal tunnel syndrome is a compressive neuropathy of the posterior tibial nerve within the tarsal tunnel. Its etiology varies, including space occupying lesions, trauma, inflammation, anatomic deformity, iatrogenic injury, and idiopathic and systemic causes. Herein, we describe a 46-year-old man who presented with left foot pain. Work up revealed a venous aneurysm impinging on the posterior tibial nerve. Following resection of the aneurysm and lysis of the nerve, his symptoms were alleviated. Review of the literature reveals an association between venous disease and tarsal tunnel syndrome; however, this report represents the first case of venous aneurysm causing symptomatic compression of the nerve.
Introduction
Venous aneurysm is defined as an isolated, persistent venous dilation twice its normal diameter. 1 Similar to arterial aneurysm, it is categorized into true aneurysm and pseudoaneurysm. True aneurysm is caused by focal weakness in all three layers of the vessel associated with a loss of elastic fibers and smooth muscle cells with fragmentation of the internal elastic lamella. 2 Conversely, pseudoaneurysm is usually caused by trauma or infection which focally disrupts vessel wall.
While venous aneurysm can lead to severe consequences such as compartment syndrome and pulmonary embolism, most are benign and do not draw much clinical attention. Surgical management is often limited to symptomatic cases involving compression of adjacent structures.
Within the tarsal tunnel, located on the medial aspect of the ankle, the posterior tibial nerve and vein lay adjacent to one another. Compression on the nerve may result in pain. While the literature suggests an association between venous disease and tarsal tunnel syndrome (TTS), herein we present a unique case of venous aneurysm causing this syndrome and successfully treated with resection of the vein and lysis of the nerve.
Case report
A 46-year-old man presented in January 2013 with a chief complaint of left lower extremity pain for three months. The pain was distributed along the side of his calf, ankle, and foot and was relieved by plantar flexion. Previous evaluation and treatment elsewhere, including nerve ablation and lumbar and epidural steroid injections, did not relieve his pain. His medical history was notable for metabolic syndrome. He denied trauma to the region, with the exception of a left ankle sprain three years previously. He denied history of deep vein thrombosis and varicose veins.
On physical examination, he was modestly overweight (BMI 29). His lower extremities were well perfused with normal pulses. He had no appreciable edema or varicose veins. A nonpulsatile mass along with overlying skin trophic changes were noted immediately above his left medial malleolus. This region was modestly tender. Motor and sensory examinations were normal; however, there was a positive Tinnel’s sign over the tarsal tunnel.
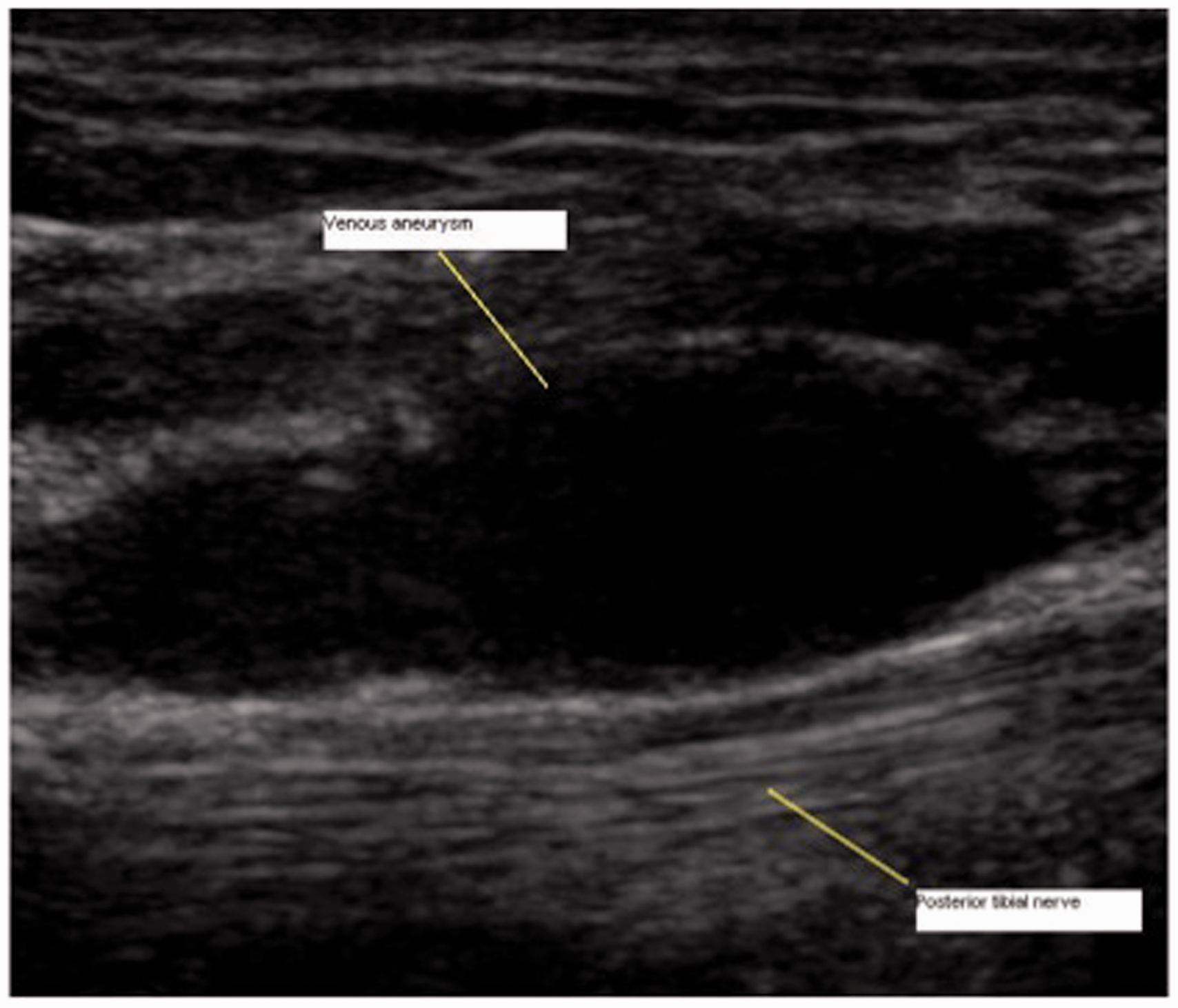
Magnetic resonance imaging (MRI) four months prior suggested a 1.2 × 0.8 × 0.8 cm mass (hyperintense on T2 and isointense on T1) arising from the left posterior tibial nerve in the left ankle (Figure 1). However, subsequent ultrasound examination performed at our institution revealed that the reported mass was compressible and arose from the left posterior tibial vein, now measuring 2 × 0.7 × 0.7 cm (Figure 2). The adjacent nerve appeared normal without intrinsic mass. Based on these findings, the patient was diagnosed with left TTS caused by a posterior tibial venous aneurysm.
Magnetic resonance image (MRI) of the left ankle region demonstrating a mass associated with the posterior tibial nerve. This image was initially interpreted as the mass arising from the tibial nerve, a finding that was negated by ultrasound imaging of the same region, and ultimately our operative findings. Ultrasound image of the left ankle region demonstrating that the mass was a venous aneurysm of the posterior tibial vein immediately adjacent to the posterior tibial nerve.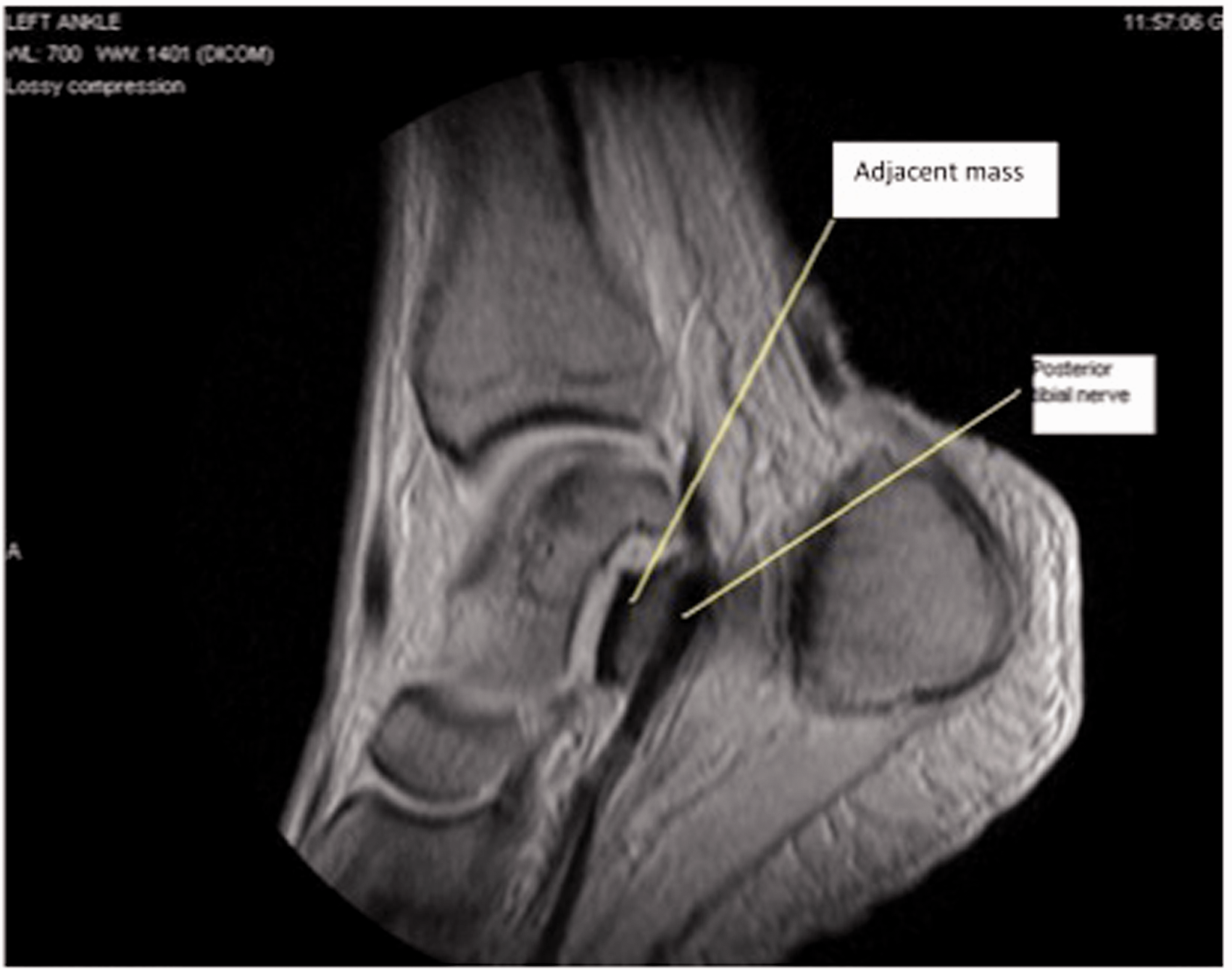
The patient underwent surgery to excise the venous aneurysm and perform neurolysis of the posterior tibial nerve. Under general anesthesia, intra-operative ultrasound was performed to visualize the aneurysm. A longitudinal incision 1 cm posterior to the medial malleolus was made to uncover the fascia of the deep posterior compartment. The fascia was incised, exposing the neurovascular bundle within tarsal tunnel. The posterior tibial vein was dissected free, revealing aneurysmal change (Figure 3). The vein proximal and distal to the aneurysm was normal. Direct nerve stimulation demonstrated decreased conduction velocities within the tibial nerve. Following excision of the aneurysm and external neurolysis, these velocities normalized. The subcutaneous tissues and skin were then closed with absorbable sutures. The patient was discharged the same day following recovery from anesthesia.
Intra-operative image following dissection of the posterior tibial aneurysm (blue vessel loops) and nerve (red vessel loop) within the exposed region of the tarsal tunnel of the patients left foot.
The histopathological examination of the venous aneurysm revealed a true venous aneurysm (Figure 4 (a) and (b)).
(a) Histopathological slide at 2× magnification demonstrating a slice of the venous aneurysm. (b) Segment of a histopathological slide at 40× magnification demonstrating the wall of the venous aneurysm. The thinned wall and the dilated nature of the vein demonstrating the aneurysmal changes of the excised venous segment are also noted.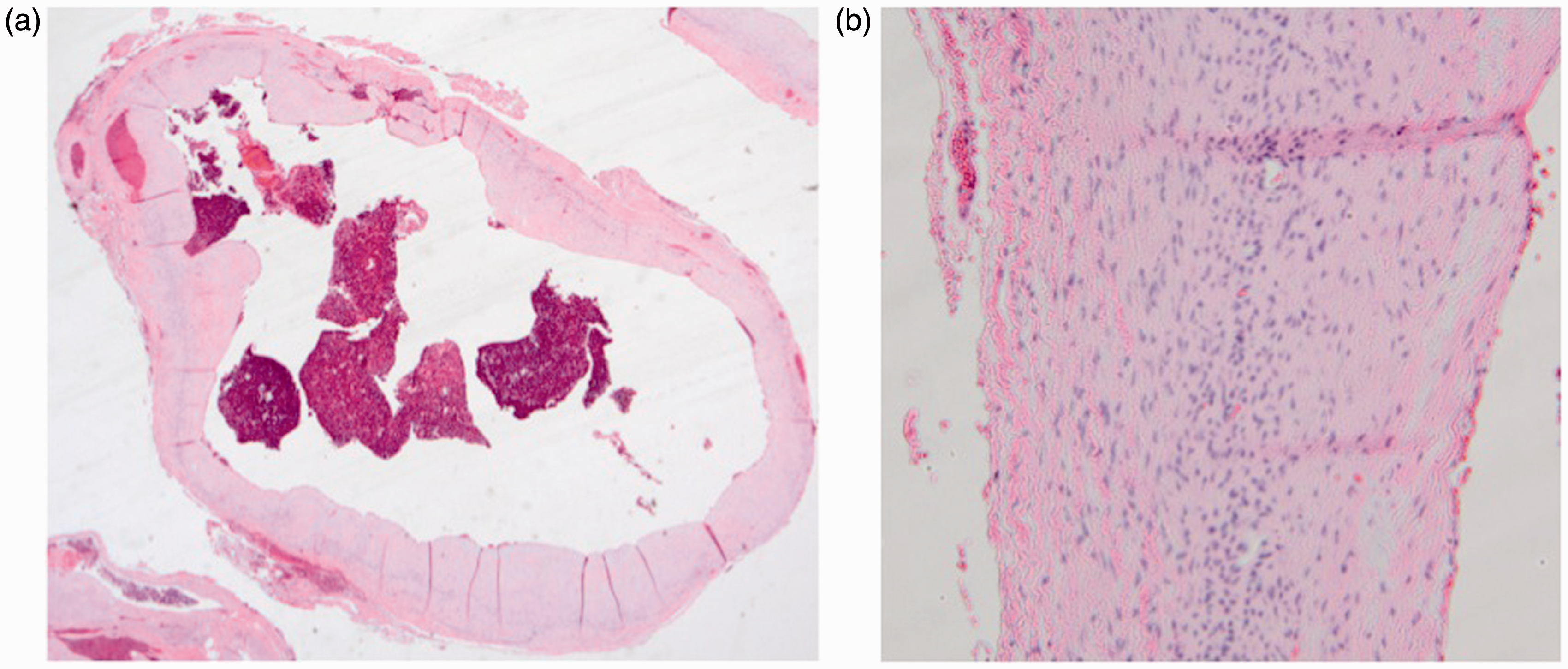
The patient experienced immediate decrease in his pain with near resolution two weeks after surgery; four months after surgery, his pain is completely resolved.
Discussion
Reported venous lesions causing tarsal tunnel syndrome.
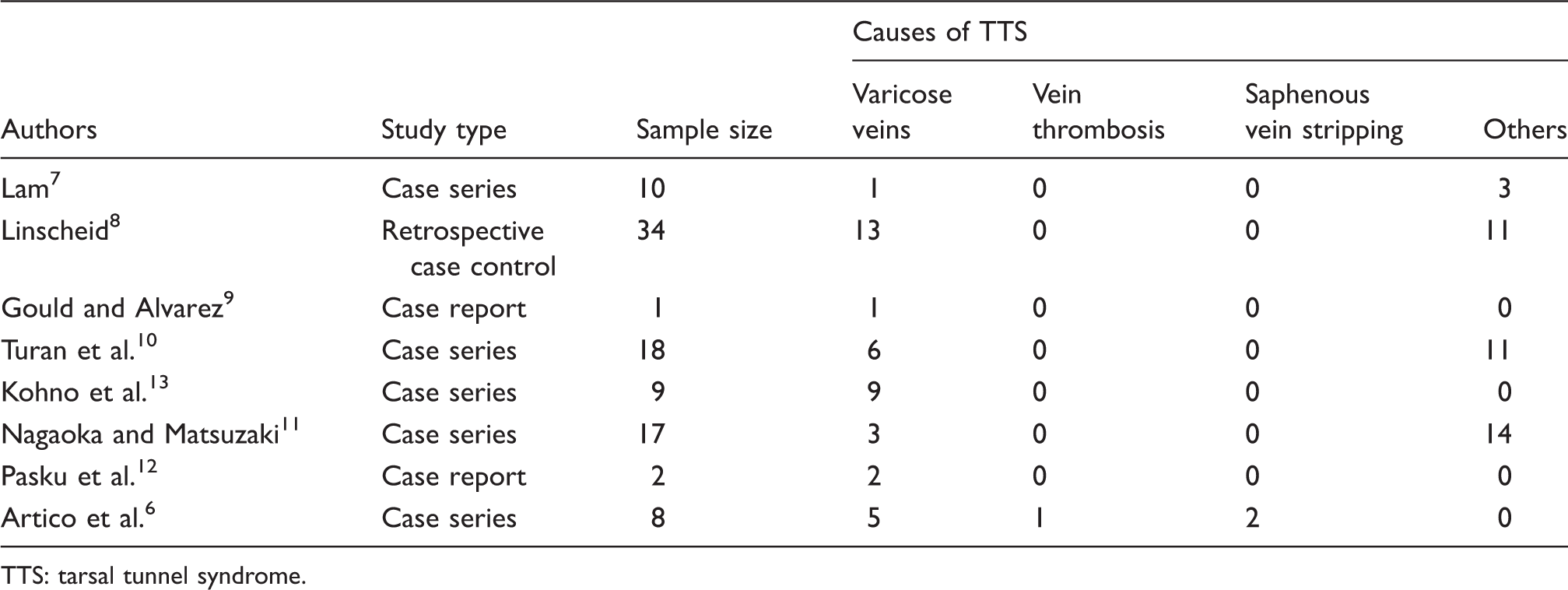
TTS: tarsal tunnel syndrome.
A search on PubMed, for English literature till March 2014, with the Mesh terms (“tarsal tunnel syndrome” and “veins”) and (“tarsal tunnel syndrome” and “aneurysm”) revealed 12 results,9–20 none of which reported a venous aneurysm as an etiology of TTS. Further search with the keywords “tarsal tunnel syndrome vein” revealed 18 results,6,9–19,21–26 none of which indicated venous aneurysm as a cause of TTS. Finally, we also reviewed the references from these 19 articles and found none reporting venous aneurysm as an independent etiology of TTS. Hence, we believe this report represents the first case of TTS caused by a posterior tibial venous aneurysm.
An interesting aspect to this case was the initial diagnosis of posterior tibial nerve mass based on MRI. MRI is a useful tool to visualize the anatomy of the tarsal tunnel and to detect abnormalities.6,27,28 Nevertheless, it has its limitations, and recent studies have reported the challenges in distinguishing a nerve lesion from its adjacent structures in the tarsal tunnel (most notably the vessels). The high number of tibial terminal nerve branches and the lack of surrounding soft tissue may reduce the ability of MRI to accurately define tarsal tunnel anatomy. 14 Since the tibial nerve runs superficially in the tarsal tunnel, ultrasound may be a better modality to visualize the tunnel. This modality appears to have greater spatial resolution which enables higher definition of the neurovascular bundle. 29 In this case, the ultrasound findings were completely consistent with what we found surgically.
Pathological examination revealed this to be a true venous aneurysm. The patient did have a remote history of ankle sprain which may have caused this entity (the aneurysm) initially. There is literature to suggest the association between trauma and venous lesions in this setting, but this appears to be limited to varicose veins12,30 and one report of TTS related to a post-traumatic pseudoaneurysm. 20
In conclusion, this report describes an unusual cause of TTS, namely a focal, true aneurysm of the adjacent posterior tibial vein. It also highlights the sometimes difficult differential diagnosis of lower extremity pain which may require multiple imaging modalities, as well as multiple specialists, to diagnose and treat this rare disorder. Ultimately, decompression of the tunnel provided the patient with long-lasting pain relief.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements
An abstract of this manuscript was presented at the EVS 27th annual meeting on 20 September 2013. No patient identification data were used in this case report. No patient consent is required.