
Abstract
Objective
To evaluate the possibility of using heparin-bonded polycaprolactone grafts to replace small-diameter arteries.
Methods
Polycaprolactone was bonded with heparin. The activated partial thromboplastin time of heparin-bonded polycaprolactone grafts was determined in vitro. Small-diameter grafts were electrospun with heparin-bonded polycaprolactone and polycaprolactone and were implanted in dogs to substitute part of the femoral artery. Angiography was used to investigate the patency and aneurysm of the grafts after transplantation. After angiography, the patent grafts were explanted for histology analysis. The degradation of the grafts and the collagen content of the grafts were measured.
Results
Activated partial thromboplastin time tests in vitro showed that heparin-bonded polycaprolactone grafts exhibit obvious anticoagulation. Arteriography showed that two heparin-bonded polycaprolactone and three polycaprolactone grafts were obstructed. Other grafts were patent, without aneurysm formation. Histological analysis showed that the tested grafts degraded evidently over the implantation time and that the luminal surface of the tested grafts had become covered by endothelial cells. Collagen deposition in heparin-bonded polycaprolactone increased with time. There were no calcifications in the grafts. Gel permeation chromatography showed the heparin-bonded polycaprolactone explants at 12 weeks lose about 32% for Mw and 24% for Mn. The collagen content on the heparin-bonded polycaprolactone grafts increased over time.
Conclusion
This preliminary study demonstrates that heparin-bonded polycaprolactone is a suitable graft for small artery reconstruction. However, heparin-bonded polycaprolactone degrades more rapidly than polycaprolactone in vivo.
Keywords
Introduction
Cardiovascular disease is the most frequent cause of death in developed and some developing countries. In America, about 250,000 open surgical vascular reconstructions are performed every year.1,2 Autologous grafts are preferable for small-diameter vascular bypass surgery because they lead to good long-term patency. However, some patients have no suitable autologous grafts.3,4 Prosthetic grafts, such as expanded polytetrafluoroethylene (ePTFE) and Dacron, have been very successful in large-diameter (internal diameter >6 mm) arterial reconstruction, but they have poor early and late patency in small-diameter arterial reconstruction.5–8 Tissue-engineered blood vessels (TEBVs) are a promising alternative to traditional prosthetic grafts. 9 These grafts are composed of host vascular cells and biodegradable scaffolds. Scaffolds allow the growth of host cells within the scaffold. The scaffold is gradually replaced by an extracellular matrix (ECM) produced by the host tissue. Therefore, the scaffold plays an important role in the success of tissue-engineered blood vessel transplants.10,11 Some synthetic biodegradable polymers have been proposed as tissue-engineered scaffolds.12–14 Nevertheless, these polymers degrade very quickly in vivo, and this means that they rapidly lose adequate mechanical structure; 15 moreover, they can produce a local acidic environment when they degrade. 16
Polycaprolactone (PCL), another synthetic biodegradable polymer, has a longer degradation time than other polymers.17–21 As it degrades, PCL does not produce acids, which can inhibit cellular proliferation and elastin biosynthesis.22–24 Some groups have demonstrated that this material has adequate cell attachment and proliferation properties.25,26 Polycaprolactone scaffolds have been used in various tissue-engineered devices.13,27,28
Heparin is a classic anticoagulant, which can effectively reduce the incidence of thrombosis at the early and immediate stages after bypass grafting. Many groups have demonstrated that heparin can inhibit intimal hyperplasia after endovascular treatment and bypass surgery.29,30
Electrospinning is a useful method of creating a tissue-engineered scaffold. In this method, various properties of the scaffold, such as morphology, porosity and mechanical property, can be controlled. 31
In this study, PCL grafts containing heparin were electrospun. The activated partial thromboplastin time (APTT) of the grafts was determined in vitro. Degradation, histology and other characterizations of the grafts were analyzed after in vivo implantation in dogs.
Materials and methods
Preparation of heparin-bonded PCL grafts
Materials and measurement
ɛ-Caprolactone (ɛ-CL) (Sigma-Aldrich, USA) was purified by distillation under reduced pressure after being dehydrated by CaH2. Stannous 2-ethyl hexanoate, N-hydroxy-succinimide (NHS) and 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide (EDC) were all bought from Sigma-Aldrich, USA, and were used as received. 1,4-butanediol (BDO; Beijing Chemical Reagents Company, China) was purified by distillation under reduced pressure. All other chemical reagents and solvents used were of analytical grade.
Heparin with molecular weights ranging from 5000 to 20,000 Da was purchased from Beijing Century Zhongwei Science Development Company, and used without further purification. The APTT kit was bought from the Shanghai Sun Biotechnical Limited Company.
Preparation of heparin-bonded PCL (hPCL)
Firstly, stannous 2-ethyl hexanoate (0.2 mmol) and BOD (0.1 mmol) were added to a vessel filled with ɛ-CL (0.087 M). The mixture was stirred for 30 min in a nitrogen atmosphere and then degassed for more than 1 h. The vessel was sealed and transferred into an oil bath at 150 ℃ to polymerize for 24 h under vacuum. The resulting PCL was dissolved in chloroform and then precipitated three times in excess methanol. The precipitate was filtered and dried overnight under vacuum. An FTIR spectrum showed peaks at 2906 cm−1 (alkyl groups), 1759 cm−1 (carboxyl groups), 1112 cm−1 (C-O groups). Analysis with 1H NMR showed peaks for 4.10, 2.31, 1.62 and 1.38 ppm (demonstrating five methylene groups in the CL unit with the resonance peaks of the second and the fourth methylene overlapping) and 3.65 ppm (indicating the methylene group next to the terminal hydroxyl).
hPCL was prepared by a direct coupling reaction. 32 Heparin (8.0 g) was dissolved in 10 ml (2-(N-morpholino)-ethanesulfonic acid (MES, pH = 6.0) buffer solution and EDC (0.08 g) and NHS (0.09 g) were added. The solution was stirred for 1 h in an ice-water bath to activate the heparin. PCL (10 g) was dissolved in 25 ml THF and added dropwise to an MES solution containing heparin. The coupling reaction was carried out at room temperature for 24 h. Afterwards, THF was removed by rotation evaporation. The product was redissolved in 50 ml chloroform. The chloroform solution was washed with 20 ml water twice and dried under anhydrous MgSO4. The dried chloroform solution was precipitated in excess methanol. To eliminate residual solvent, the precipitate was dried at 35 ℃ for 24 h under vacuum after filtering. The FTIR spectrum showed peaks at 3460 cm−1 (hydroxy groups), 2906 cm−1 (alkyl groups), 1759 cm−1 (carboxyl groups), 1645 cm−1 (amino groups), 1260 cm−1 (sulfonic groups), 1112 cm−1 (C-O groups). The 1H NMR analysis showed peaks at 4.10, 2.31, 1.62 and 1.38 ppm (demonstrating five methylene groups in the CL unit with the resonance peaks of the second and the fourth methylene overlapping), 2.68 ppm and 3.52 ppm (the latter two are resonance peaks ascribed to heparin).
Preparation of hPCL grafts
Electrospun grafts were prepared as described previously. 32 Briefly, the grafts were fabricated by electrospinning using hPCL and PCL (PCL grafts as a control group). The electrospinning apparatus included a high-voltage supplier, a syringe pump, a syringe with blunt-ended needle and a custom-made rotating mandrel of 2.5 mm diameter to collect the fibres. A 20-kV voltage was applied to drive the hPCL solution. The solution was delivered to the rotating mandrel at a constant flow rate of 5 ml/h. The distance between the mandrel and the tip of the syringe was 20 cm.
Determination of activated partial thromboplastin time of grafts in vitro
The anticoagulant activity of hPCL was determined using an activated partial thromboplastin time (APTT) assay. Briefly, the PCL and hPCL films were cut into 1-cm × 0.5-cm rectangles and placed in a test tube. Citrated standard plasma (100 μl) and Pathromtin SL (100 μl) were then pipetted into a test tube pre-warmed to 37 ℃, which was incubated for 3 min at 37 ℃. On adding the calcium chloride solution (100 μl, 0.025 M) at 37 ℃, the timer on a fibrin timer (TEChrom IV plus, China) began to measure the APTT.
Assay of burst pressure
Burst pressure was measured and recorded by increasing the pressure within grafts until failure occurred. In brief, a pressure transducer catheter was inserted through a cannulating fixture at one end of the graft and a water pump connected at the other end of the graft. The pressure in graft was gradually increased until bursting occurred and the highest pressure value before bursting was recorded. This value was defined as burst pressure.
Small-diameter arterial reconstruction: grafts, follow-up and sacrifice
Twelve adult mongrel dogs (weight range 15–25 kg, age range 2–3 years, Ke Yu Animal Center, Beijing, China) of either sex were operated upon. Each subject received two vascular grafts, one in each femoral artery. General anaesthesia was induced by intramuscular injection of 2 mg/kg xylazine HCl (Hua-mu Animal Health Products Co., Ltd. Jilin, China) and 1 mg/kg diazepam (Tianjin Pharmaceutical Group Jiaozuo Co., Ltd. Henan, China). Xylazine injections were repeated when required. The bilateral inguinal region was shaved. Bilateral skin inguinal incisions (approximately 8 cm long) were made along the femoral artery. Femoral arteries were isolated. A heparin solution (0.8 mg/kg) was injected into one of the femoral arteries. After proximal and distal clamping, two segments of the bilateral femoral arteries, approximately 5-cm long, were resected in a bevelled shape. hPCL grafts (n = 12) were implanted and anastomosed in an end-to-end fashion to the artery by simple sutures of 7-0 nylon using a magnifying glass under sterile conditions. As a control group, the same number of PCL grafts were implanted in the same way. The connective tissue and skin were closed. The dogs were fed ad libitum with normal food and water. From the first 3 days after surgery, 800,000 units of penicillin were administered intramuscularly every 12 h. No anticoagulant or antiplatelet agents were administered during the follow-up. The dogs were followed up at 4, 8 and 12 weeks (two dogs of each kind of grafts for each endpoint). At the end of the follow-up time, the dogs were anaesthetized with the same method mentioned above. The left carotid artery was isolated and cannulated (4 F catheter). After successful cannulation of the target artery, digital subtraction angiography (DSA) was performed through the catheter. Then the grafts were explanted for further testing and the dogs were sacrificed by intravenous injection with an overdose of sodium phenobarbital.
In vivo degradation assessment of the grafts
The in vivo degradation of graft materials was measured by gel permeation chromatography (GPC) using a Waters 2414 with three Waters styragel high molecular weight columns at 35 ℃, with THF as eluent. The explanted graft was dissolved in THF by ultrasound. The THF solution was then filtrated by syringe filter with 0.2-µm pore diameter before it was injected into the GPC instrument. The molecule weight of explanted graft was then determined as calibrated with polystyrene standards.
Histology
Part of the explanted grafts (except parts for other tests) were fixed in 4% paraformaldehyde for 24 h, then dehydrated and embedded in paraffin. Sections of 5-µm thickness were cut. Specimens were stained with hematoxylin and eosin (H&E) for cells and Masson staining for collagen. Von Kossa staining was performed to evaluate the calcification of the grafts. The specimens were used for immunohistochemical staining of von Willebrand factor (vWF). The explanted grafts were stained with anti-vWF antibody (code number: A0082, DAKO, Denmark) for endothelial cells.
Collagen content assay of the grafts
The explants were stored at −20 ℃. After freezing, specimens were vacuum freeze dried. The specimens were defatted in chloroform-methanol solution (2:1) for 24 h, then dried again and weighed, and hydrolyzed in 6 M HCl for approximately 2 h at 130 ℃. Then the solutions were neutralized to 7 pH with NaOH. The samples were mixed with chloramine-T and p-dimethylaminobenzaldehyde, and hydroxyproline content was determined by spectrophotometry according to Woessner. 33 Absorbance was measured at 570 nm. Collagen content was calculated using a 1:10 ratio of hydroxyproline to collagen. 34
Statistical analysis
Statistical tests were performed with SPSS (version 11.5; SPSS Inc, Chicago, Ill). Results are expressed as mean ± SD. The one-factor analysis of variance was used to compare the differences between groups. The level of significance was set at p < 0.05.
Results
Morphology of hPCL grafts
The grafts were ivory-white. They were more elastic when dry than when wet. Surface analysis by scanning electron microscopy (SEM) revealed a smooth surface. The fibres of the grafts were uniform without beading and the fibre diameters ranged from 0.6 to 4 µm.
DSA results
After surgery, 12 dogs survived without special clinical event until the predetermined study endpoints. Digital subtraction angiography showed that two hPCL grafts were occlusive (4 weeks and 12 weeks after transplantation, respectively) and three PCL grafts were occlusive (4 weeks, 8 weeks and 12 weeks after transplantation, respectively). The other grafts were patent. No aneurysmal dilatation or stenosis were found in the patent grafts (Figure 1).
A patent hPCL graft at 12 weeks post operation. Neither patent graft had aneurysmal dilatation or stenosis. The arrows show the anastomosis.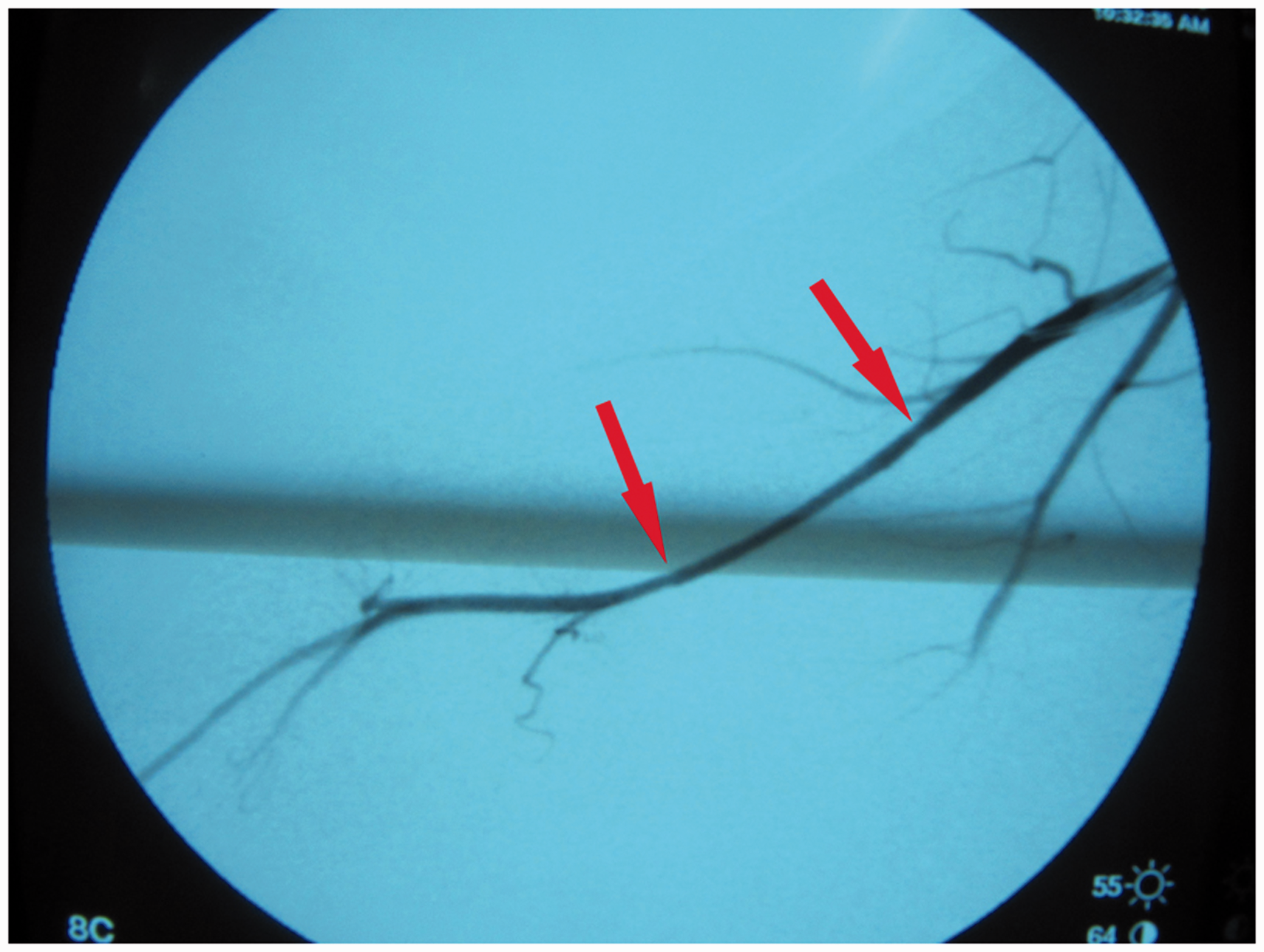
Anticoagulant efficiency of the grafts in vitro
As the prepared hPCL is expected to be applied in vascular tissue engineering, it is important to evaluate its anticoagulant properties in vitro by determining the APTT. The unique anticoagulant property of heparin is that it binds to antithrombin III (AT-III) in the blood plasma. Antithrombin III is the major inhibitor of the coagulation cascade; thereby the complex formed readily reacts with thrombin to inhibit the formation of a fibrin network, which is an important step in thrombosis. Covalently bonded heparin might be assumed to possess this anticoagulation property.
The APTT of hPCL was measured to be above 300 s (n = 6, the maximum value measured by the fibrin timer is 300 s), and it was obviously prolonged compared with a PCL control (plasma 50.7 ± 1.2 s, PCL 51.4 ± 0.7 s, all n = 6). There were statistical differences between hPCL and plasma, and between hPCL and PCL (the value of hPCL was set to 300 s, p < 0.001). This result showed the excellent anticoagulation properties of the hPCL and its potential for vascular tissue engineering.
Degradation assessment of the grafts
The explants degraded gradually over time. By comparison with the heparin-bonded grafts, the hPCL explants at 12 weeks lost about 32% for weight-average molecular weight (Mw) and 24% for number-average molecular weight (Mn). The PCL explants at 12 weeks lost about 23% for Mw and 15% for Mn compared with PCL grafts.
Histology
It was observed that the explants were surrounded by connective tissue. No aneurysm-like changes were observed in any explant. The H&E staining showed that the full thickness of the graft was infiltrated by the host cells at each time point. Over time, the grafts degenerated gradually and holes appeared in the graft walls. Masson staining demonstrated that the collagen in the grafts increased as a function of implantation time. There was no evident calcification in the grafts of each endpoint, as revealed by von Kossa staining. Immunohistochemical staining of vWF demonstrated that the inner surfaces of the hPCL grafts were covered by the endothelial cells at each time point. The coverage of endothelial cells and the numbers of infiltrating microvessels in the wall of the grafts increased over time. Compared with hPCL grafts, the explanted PCL grafts were dense at 12 weeks (Figure 2).
Histological analysis of hPCL and PCL. (a) H&E staining of hPCL at 12 weeks after transplantation. (b) vWF immunohistochemical staining of hPCL at 12 weeks after transplantation. (c) Masson staining of hPCL at 12 weeks after transplantation. (d) H&E staining of PCL graft at 12 weeks. H&E staining showed that the full thickness of the grafts was infiltrated by the host cells at 12 weeks. The grafts degenerated gradually and holes appeared in the graft walls. Compared with hPCL, PCL grafts were dense at 12 weeks. Immunohistochemical staining of vWF demonstrated that the inner surfaces of the hPCL grafts were covered by the endothelial cells and infiltrated microvessels in graft walls at 12 weeks. Masson staining showed the collagen deposition in hPCL at 12 weeks. Arrows show the inner surface of grafts. Original magnification: a, c and d: × 100, b: × 200.
Burst pressure results
Burst pressure testing showed that hPCL grafts closely matched PCL grafts before implantation. The burst pressure of hPCL explants at 12 weeks was similar to the controls. Both kinds of explants at 12 weeks decreased in burst pressure compared with grafts before implantation. However, there were no statistical differences (Figure 3).
Burst pressure of hPCL and control group.
Quantification of collagen content
The collagen content of grafts from each explantation point (4, 8 and 12 weeks; all n = 4) gradually increased. The collagen contents per 100 g of dry samples was 5.392 ± 0.221 g in the 4-week explants, 8.038 ± 0.163 g in the 8-week explants and 10.292 ± 0.082 g in the 12-week explants.
Discussion
Tissue-engineered blood vessels are promising to improve the patency rate of small-diameter arterial bypasses. Their key factor lies in the TEBV’s plasticity or degradation in vivo. However, TEBVs have some disadvantages at present. Firstly, each TEBV should be individualized with the host’s own cells during its construction. Secondly, the in vitro production time of TEBV is longer, restricting the use of the TEBV in urgent clinical cases and increasing the possibility of infection of the TEBV. 35 Finally, the construction is complex and needs more sophisticated apparatus. Owing to these factors, some authors 15 have attempted to develop a degradable vascular scaffold, which is replaced gradually with tissue ingrowth in vivo, ultimately creating a complete autogenic vascular conduit. These scaffolds possess the same role of TEBV in vivo, but can be produced more easily than the TEBV.
Scanning electron micrography showed that the fibres of hPCL were oriented randomly and formed a non-woven three-dimensional structure. At some points, the fibres adhered to each other and constructed interconnected pores. This structure is beneficial to cellular adhesion and proliferation and to the transport of oxygen and nutrition. 36
In our study, heparin was covalently attached to PCL in an EDC/NHS reaction system. Compared with physical mixing or absorption by PCL molecules, covalent binding is a firm modality. Our APTT tests showed that the hPCL has a good anticoagulant effect in vitro. This result demonstrates that the covalent binding mode does not reduce the anticoagulant effect of heparin. The heparin covered the full thickness of our grafts, rather than merely their inner surfaces. We think that the former will be advantageous over the latter because it can ensure that heparin will have both antithrombotic and anti-intimal hyperplastic effects during the whole course of graft degradation and tissue deposition. However, there were no differences in patency rate between hPCL and control group. We think the difference could not be observed in such short study period.
In our previous study, the contact angle of the hPCL is smaller than that of the PCL. 32 This result demonstrates that the hydrophilicity of the former is higher than the latter because the hydrophilic heparin was covalently attached to PCL. In this study, the hPCL grafts degraded with Mn and Mw losses of about 30% at the last endpoint (12 weeks). This degradation rate is higher than that described in the literature 37 and the control group. The difference is mainly caused by the higher hydrophilicity of hPCL, because the higher hydrophilicity can improve the interaction between cells (including phagocytic cells) and the grafts38,39 and accelerate the degradation of the grafts. The looser hPCL grafts shown in H&E staining at 12 weeks may be caused by the higher degradation. However, according to the DSA and data of burst pressure, the higher degradation rate did not decrease the mechanical strength of hPCL in this study.
Histological analysis demonstrates that not only did the intima cover the inner surface of the grafts but also that some holes were produced by the graft degradation and neo-microvessels formed in the graft walls. The degradation of the grafts may be caused by phagocytosis from macrophages and giant cells 40 and by arterial pulsatile mechanical forces. 37 Collagen is one of the important ECM components, which is produced by ingrowing vascular cells. 35 Shear stress is an important signal for vascular cells to induce synthesis of collagen in vivo. 41 In this study, collagen deposition is found to decrease gradually from the inner surface to the outer surface in the wall of hPCL graft. This is due to the vascular cells moving from the vascular lumen into the graft wall. The closer the lumen, the more vascular cells and the shear stress is only present between the intima of graft and blood.
The collagen content of the grafts increased over time in vivo. At 12 weeks, there was ≈10.2 g collagen in 100 g dry explants. This reveals that the ECM of the blood vessel in the grafts is produced by the cells infiltrating the wall. With the degradation of the grafts, more ECM will be produced and, finally, the ECM will have developed to form a new blood vessel.
Conclusions
This preliminary study demonstrates that hPCL is a suitable graft material for small artery reconstruction. It has the appropriate mechanical properties and it has an anticoagulant effect and good biocompatibility. However, compared with PCL, hPCL degrades rapidly in vivo. This disadvantage should be overcome in future work.
Limitations of present study
The main limitation of our experiment was that the observation time after grafts implantation was too short. This made no further data to be obtained to demonstrate the superiorities or other defects of hPCL. In the further study, this will be amended.
Footnotes
Funding
This study was supported by Natural Science Foundation of Shanxi Province (grant number: 2013011058-2) and National High Technology Research and Development Program (“863” program) of China (grant number: 2006AA02A134).
Conflict of interest
None declared.