
Abstract
Objective
To analyze the characteristics of patients with abdominal aortic aneurysms referred to a tertiary center and to compare with individuals with abdominal aortic aneurysm found at necropsy.
Methods
We have retrospectively analyzed the medical records of 556 patients with abdominal aortic aneurysm and 102 cases abdominal aortic aneurysm found at necropsy.
Results
At univariated analysis, hypertension, tobacco use and maximum diameter were significant risk factors for symptomatic aneurysm, while diabetes tended to be a protective factor for rupture. By logistic regression analysis, the largest transverse diameter was the only one significantly associated with abdominal aortic aneurysm rupture (p < .0001, odds ratio 1.7, 95% confidence interval 1.481–1.951). Intact abdominal aortic aneurysm found at necropsy showed similarities with outpatients in relation to abdominal aortic aneurysm diameter and risk factors.
Conclusion
Intact abdominal aortic aneurysm at necropsy and at outpatients setting showed similarities that confirmed that abdominal aortic aneurysm repair is less offered to women, and they died more frequently with intact abdominal aortic aneurysm from other causes.
Introduction
There is ample scientific support for repairing abdominal aortic aneurysm (AAA). Several randomized trials have demonstrated the benefit of repair when the AAA reaches a certain transverse diameter or if there are symptoms associated with dilation.1,2 However, some aspects of the natural history of AAAs remain controversial, especially their evolution in young people and women, the characteristics of AAAs with unusual morphologies and risk factors for AAA growth and rupture.
Screening studies of populations at high risk of developing AAAs have improved the understanding of the natural development of dilation and of patient characteristics, resulting in more elective surgeries, fewer emergent surgeries, decreased aneurysm-associated mortality and the detection of small aneurysms, allowing clinicians to track and assess the natural evolution of AAAs.3–6
In countries where large screening programs have not been implemented, 7 samples of patients with aneurysms are studied starting from patients referred to tertiary services, with symptomatic and asymptomatic aneurysms. Classically, this type of analysis incurs a selection bias and may underestimate the prevalence in low-risk populations, especially women and younger patients.8.9
Therefore, the aim of this study was to analyze the characteristics of aneurysms and patients referred to a tertiary university hospital, including patients who underwent elective or emergent surgery, outpatients (i.e. without undergoing surgery) and of individuals (in the same geographical region as the tertiary university hospital) in which ruptured or intact aneurysms were found at necropsy.
Methods
Patients and necropsy individuals
We retrospectively analyzed the medical records of 556 patients with a nonspecific infrarenal AAA who were referred to the Vascular and Endovascular Surgery Division Clinics Hospital, Faculty of Medicine, University of São Paulo, between 2001 and 2009. These patients were divided into three groups according to whether the AAA was identified in an inpatient setting (n = 352), outpatient setting (n = 88) or during emergent treatment (n = 116). We also included 102 cases of ruptured (n = 47) or intact (n = 55) AAA that were found at necropsy. This study was approved by the Ethical Committee of University of São Paulo Medical School by the numbers: 849/99 and 373/04.
The inpatient group included patients who were hospitalized for elective repair of asymptomatic infrarenal AAA because the maximum transverse diameter was ≥5.0 cm on ultrasound and/or computed tomography (CT). Patients with an AAA of <5.0 cm in diameter and aneurysms of the iliac arteries, indicating correction, were also included in this group. Patients with an AAA of <5.0 cm who were not indicated for surgery, or who were at high operative risk or refused to undergo surgery were included in the outpatient group. The emergent group consisted of patients with symptomatic AAA, which included pain caused by the AAA and/or AAA rupture, and who underwent urgent or emergent surgery.
The Coroner Service of the University of São Paulo, which is located in the same region as the Vascular and Endovascular Surgery Division, is responsible for performing autopsies of nonviolent deaths in São Paulo. The two groups corresponding to necropsy findings (ruptured and intact) were derived from a series already analyzed and published.10,11
The medical records of patients treated at the Division of Vascular and Endovascular Surgery were reviewed to retrieve the following information: aneurysm status (ruptured or intact), maximum transverse diameter (measured by ultrasound/CT), symptomatic/asymptomatic status of the patient, smoking status (active or former smoker) and histories of hypertension, diabetes mellitus or coronary disease.
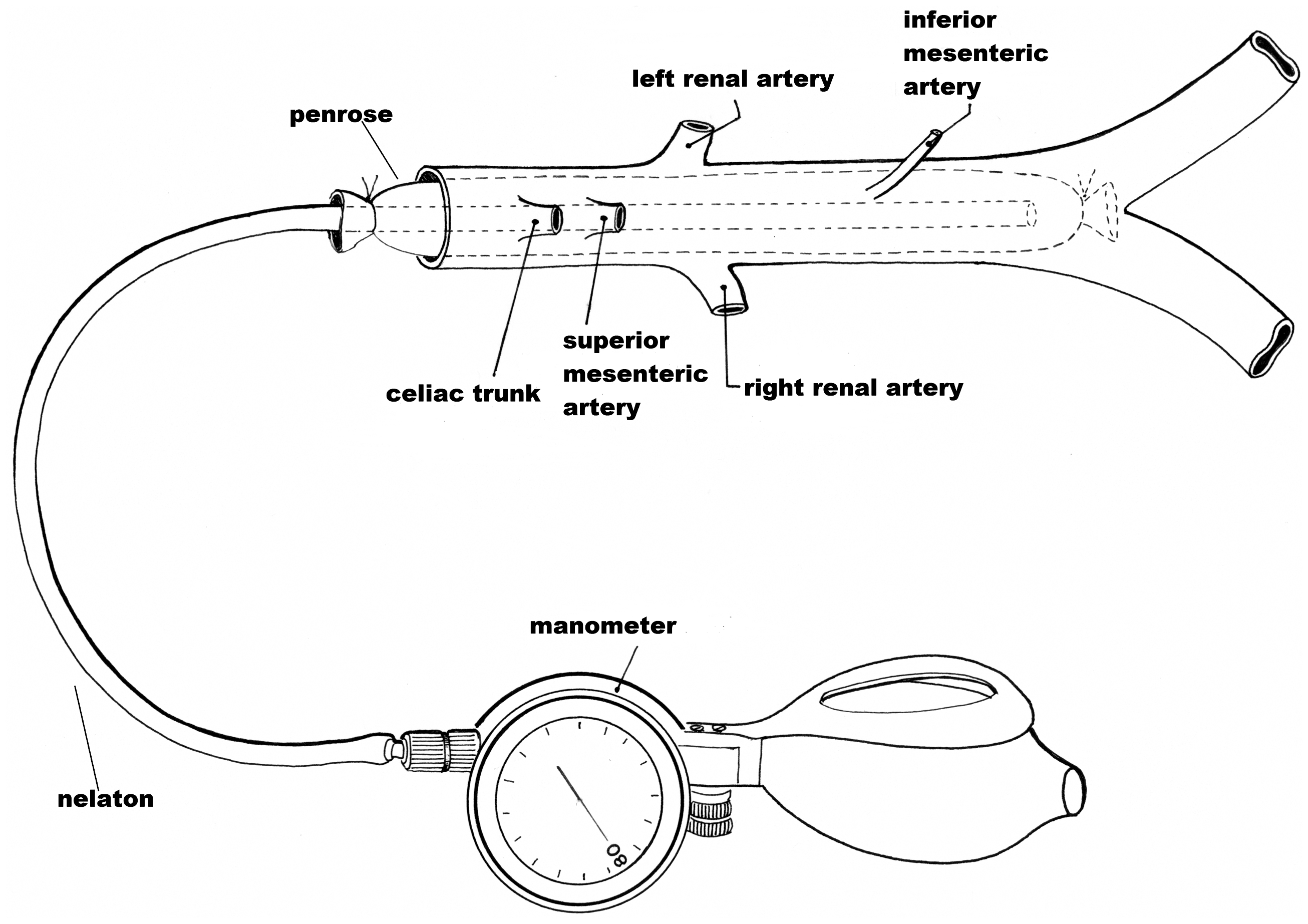
For autopsied cases, information was obtained from the necropsy report and from family members. The diameter of the AAA in autopsied cases was measured using a standardized procedure, as previously described.10,11 Briefly, after removing and carefully dissecting the specimen, the morphology of the AAA was restored as shown in Figure 1. To re-establish AAA diameter and morphology, a device was designed. This device is introduced into the artery and inflated to 80 mmHg, and the largest external diameter of the AAA is then measured with a pachymeter calibrated in mm. (Figure 2).
Abdominal aortic aneurysm specimen found at necropsy after dissection and with device inserted into aortic lumen to re-establish the morphology. Drawing of the distension device inside the aorta.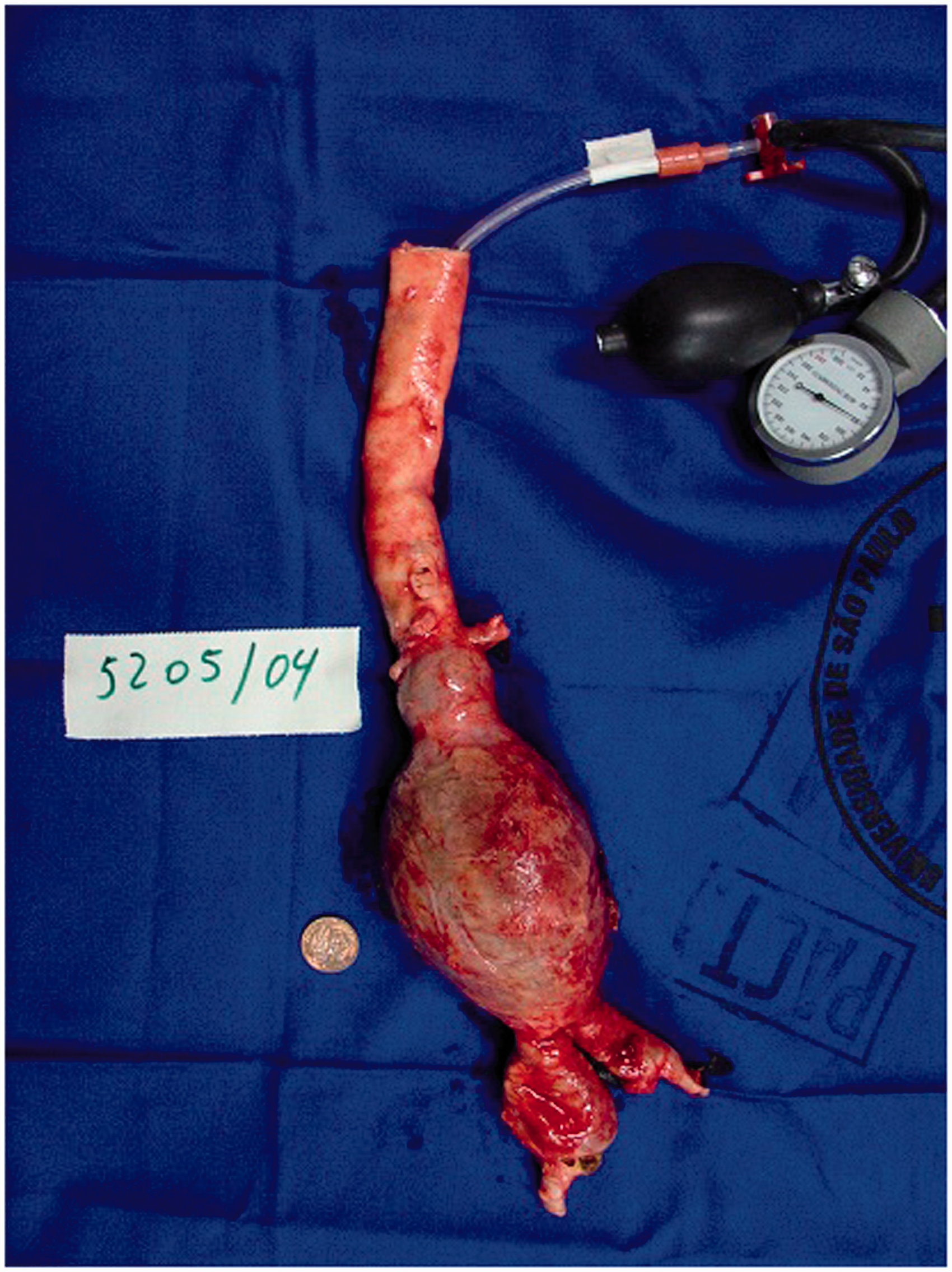
We excluded patients/necropsy cases for whom reliable information could not be obtained for any of the variables, or if there was any doubt about the etiology of the AAA.
Statistical analyses were conducted to compare groups of patients divided by sex, aneurysm status (ruptured vs. intact), symptomatic status (symptomatic vs. asymptomatic), AAA diameter (≥4.0 to <5.5 cm, ≥5.5 to <7.0 cm and ≥7.0 cm) and the clinical setting (i.e. outpatient, inpatient, emergency and necropsy). The rationale for these comparisons was to characterize individuals from different point of view and try to demonstrate if there are differences mainly on necropsy findings.
Statistical analysis
Variables are reported as percentages or as means ± standard deviation or range. Continuous variables were compared between groups using Student’s t test or analysis of variance, while categorical variables were compared using the χ2 test or Fisher’s test. Binomial logistic regression was performed for multivariate analyses, analyzing rupture and acute prerupture pain as outcomes. Values of p < .05 were considered statistically significant.
Results
General characteristics of the total study sample and of males and females separately.
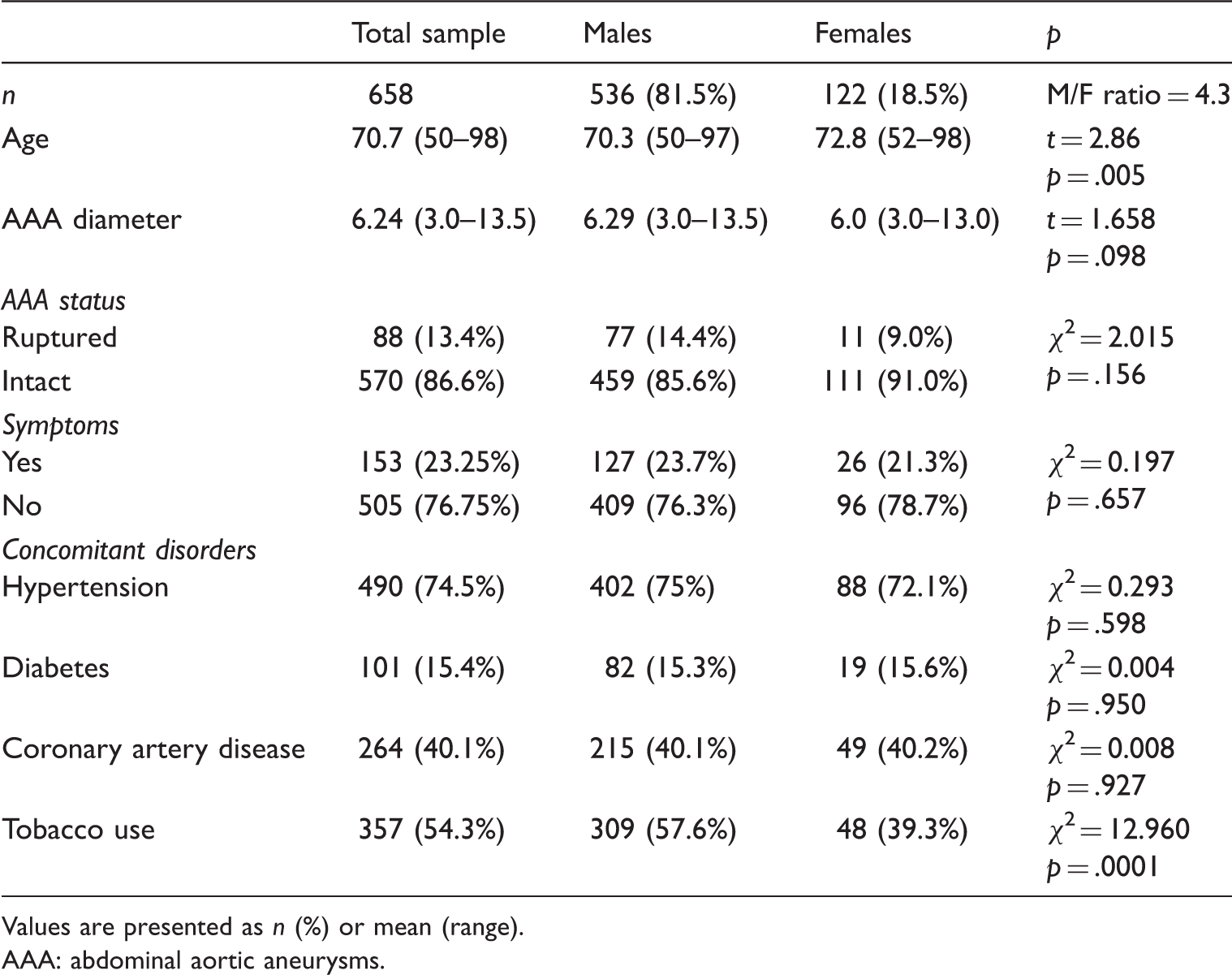
Values are presented as n (%) or mean (range).
AAA: abdominal aortic aneurysms.
Characteristics of the patients according to aneurysm status or symptom status.
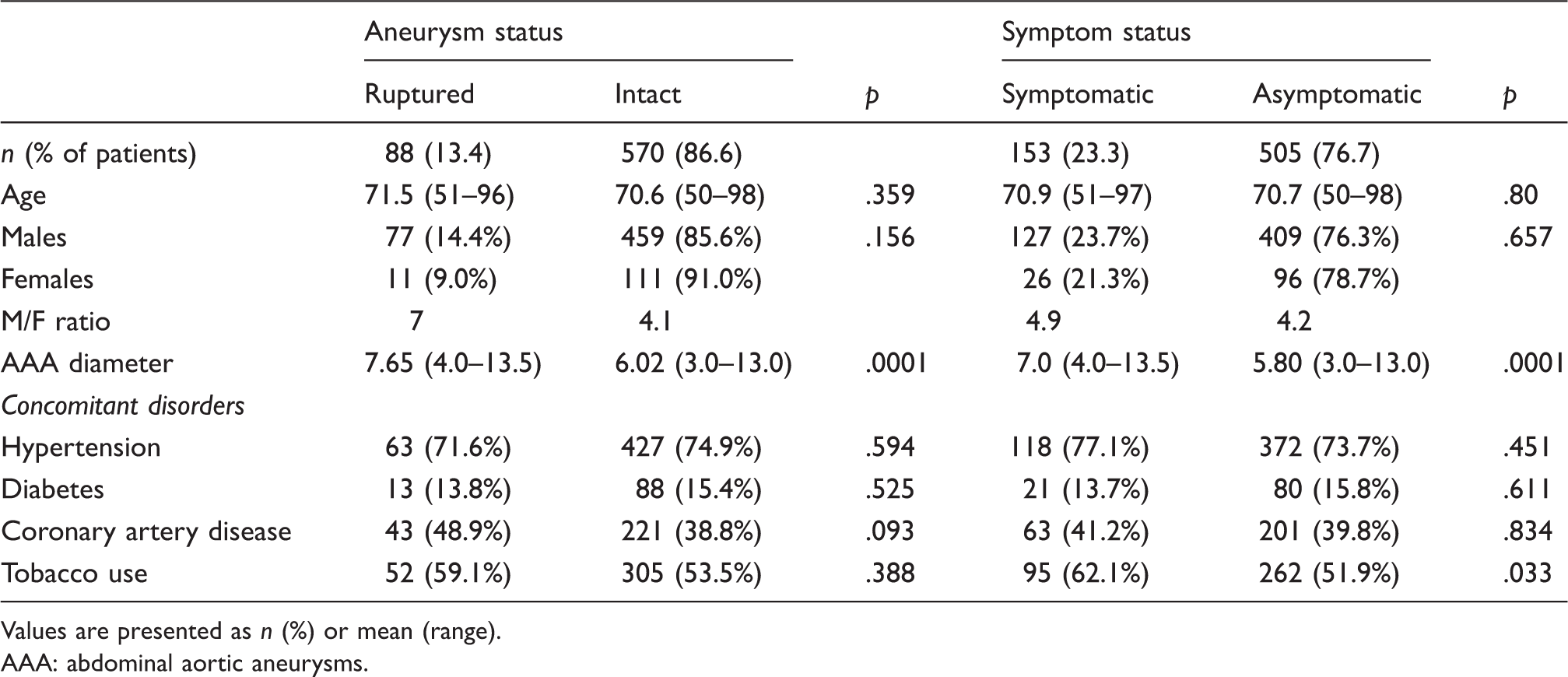
Values are presented as n (%) or mean (range).
AAA: abdominal aortic aneurysms.
The maximum transverse diameter was significantly higher in ruptured and symptomatic AAAs (average: 7.65 cm and 7.0 cm) than in intact and asymptomatic AAAs (average: 6.02 cm × 5.80 cm, p = 0.0001). The prevalence of smoking was higher and significant in symptomatic AAAs. The proportion of males was greater than that of females in all four groups, and the male to female ratio was greatest in patients with a ruptured AAA (7:1).
Logistic regression analysis was performed to determine whether any of the variables assessed in this study (i.e. age, sex, AAA diameter or history of hypertension, diabetes, smoking or coronary artery disease) were significantly associated with AAA rupture. Of all the variables assessed, only the largest transverse diameter was significantly associated with AAA rupture (p < .0001, odds ratio (OR) 1.7, 95% confidence interval (CI) 1.481–1.951). We then assessed whether these variables were associated with the development of symptoms (pain without rupture or with rupture). In this analysis, again, AAA diameter (p < 0.001, OR 1.650, 95% CI 1.458–1.867) was significantly associated with the presence of AAA symptoms.
Analysis of the sample according to place of presentation.
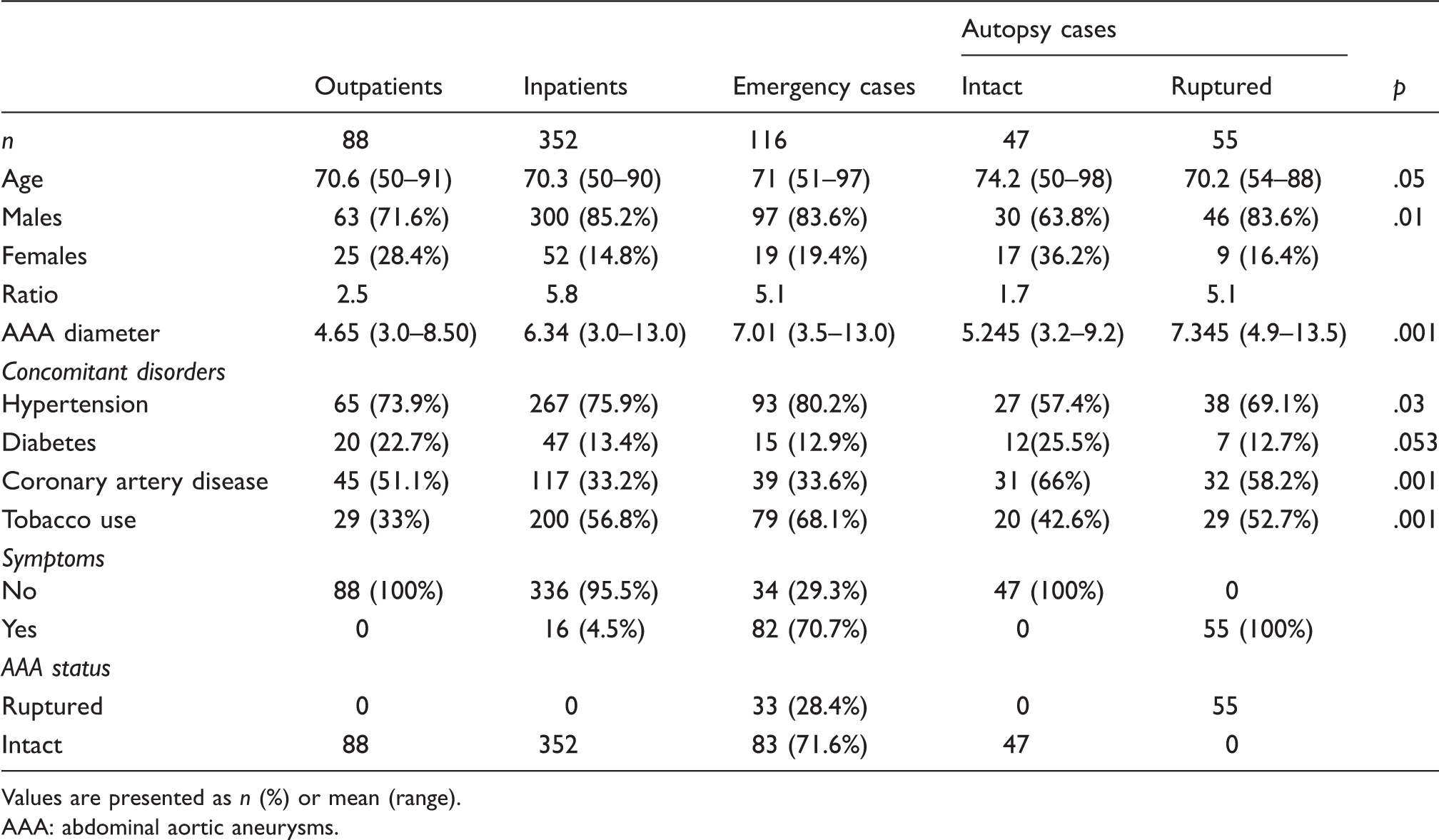
Values are presented as n (%) or mean (range).
AAA: abdominal aortic aneurysms.
The prevalence of hypertension was lowest in cases of intact aneurysm found at necropsy. The prevalence of diabetes was low in all groups, but tended to be higher in the outpatients and in cases of intact aneurysm found at necropsy (22.7% and 25.5%, respectively). The lowest proportions of smokers also characterized these two groups. The prevalence of coronary artery disease was highest in both necropsy groups.
Characteristics of ruptured aneurysms according to maximum transverse diameter of the aneurysm.

Values are presented as n (%) or mean (range).
AAA: abdominal aortic aneurysms; SD: standard deviation.
Finally, we compared the characteristics of patients according to AAA diameter, in which we included all patients with symptomatic aneurysms (i.e. ruptured aneurysms and aneurysms associated with pain). As in the analysis of ruptured aneurysms, most of the cases in Group I were males (14, 77.8%), but this group also included some women (4, 22.2%). Group II consisted of 54 patients with symptomatic AAA. Their characteristics were similar to those of Group III (81 patients). As in the analysis of ruptured aneurysms, the age increased progressively with increasing AAA diameter.
Discussion
The characteristics of patients with AAA have been analyzed in populations subjected to screening,4–6,12 in the medical records of patients with AAA in specific countries or regions,8,9,13–15 in randomized studies comparing outcomes of surgical treatment versus observational follow-up,1,2 series of surgical cases, 9 patients followed because of unfavorable clinical conditions, 16 and in necropsy series. 17
An important feature of necropsy studies is that cases of intact AAA represent a group of individuals that should not have submitted to an intervention, because the cause of death was unrelated to AAA. By contrast, cases of ruptured AAA represent a group of individuals that should have received an intervention. However, a limitation of necropsy studies is the difficulty in accurately measuring the diameter of the aneurysm. To overcome this limitation, the morphology of the AAA was restored by artificially increasing local aortic pressure.10,11
In this study, we confirmed some well-established findings, including the lower prevalence of AAA in women, that women develop AAAs at an older age than men, that relatively few patients with AAA have diabetes, and that a large proportion of patients are smokers, especially among individuals with symptomatic AAA. Table 4 shows that patients with a ruptured AAA with a diameter <5.5 cm are generally younger men with a low prevalence of diabetes and high prevalence rates of smoking and hypertension as compared with patients with larger ruptured AAA. These differences were statistically significant.
Characteristics of symptomatic aneurysms according to maximum transverse diameter of the aneurysm.

Values are presented as n (%) or mean (range).
AAA: abdominal aortic aneurysms.
Another interesting finding is that the prevalence of AAA in women (18.5%) in our study is similar to that in surgical series.8,25 However, the prevalence of AAA in women increased to 28.4% of patients who did not undergo surgery and to 36.2% of cases with an intact AAA found at necropsy. Similar prevalence rates were reported in other necropsy series.17,26–28 These results reinforce the hypothesis that correction is less frequently offered to women, because high surgical risk (for open repair) 15 or on unfavorable anatomy (for endovascular aneurysm repair)9,13,15 or low incidence and lower concern for detection. 29
Our study highlights that the widely reported male to female ratio of 4:1 is inaccurate because the ratio was 2.5:1 in patients who did not undergo surgery and was 1.7:1 in cases of intact AAAs found at autopsy.
When we analyzed patients who were followed in outpatient settings, who did not undergo surgery, or who were found to have an intact AAA at necropsy, we noted some associations between AAA diameter and other risk factors in these groups. Of note, the results of autopsy cases provide support for the observation of patients with small AAAs because the cause of death was not associated with AAA.
Screening studies and randomized trials that are designed to examine the need for surgical treatment and to monitor patients with AAA are particularly valuable in terms of elucidating the natural evolution of AAA and detecting the associated risk factors and associated diseases. However, many screening studies exclude women and limit the age range of subjects.12,13 Furthermore, in randomized trials, AAAs with a diameter ≥5.5 cm are usually surgically treated, which limits the ability to determine the natural expansion of these AAAs.1,2 Meanwhile, mortality data are based on death certificates, and there may be diagnostic errors regarding the status of AAAs.30,31
The present study was conducted in a developing country with some limitations to the healthcare system that preclude the possibility of screening large populations. 7 For this reason, we combined patients from a variety of clinical settings (i.e. outpatients, inpatients, emergency cases and necropsy cases) to better understand the characteristics of AAAs. Nevertheless, it is essential that we acknowledge the possibility of selection bias. Tertiary services and university hospitals tend to receive a large number of complex patients with multiple comorbidities. Meanwhile, coroner services responsible for investigating nonviolent deaths tend to receive people who die because of cardiovascular disease, including heart attack and stroke, which are the main causes of death in large cities, and men are mostly affected by these disorders.
Conclusions
The transverse diameter was main risk factor for AAA rupture or the presence of symptoms in this study population. It was not possible to reveal a higher frequency of rupture in females, nor were there any ruptures of smaller aneurysms in females at the time of initial diagnosis, in spite of small number of ruptures in the group of AAA diameter inferior to 5.5 cm in this sample. Smoking was associated with the presence of symptoms, whereas the presence of diabetes tended to be associated with smaller AAA and the absence of symptoms. The characteristics of outpatient and necropsy cases with intact aneurysms were similar, including higher proportions of women and individuals with diabetes, fewer smokers and smaller diameter AAAs.
Footnotes
Acknowledgements
We are grateful to the team members of the Vascular and Endovascular Division of Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, Department of Surgery, specially Karina Domingos Rosa, MD and Cristina Kobata, MD.
Conflict of interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.